Trends in Intake of Energy and Total Sugar from Sugar-Sweetened Beverages in the United States among Children and Adults, NHANES 2003–2016


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. NHANES Dietary Interview
2.3. Sugar-Sweetened Beverages Definition and Categories
2.4. Statistical Analysis
3. Results
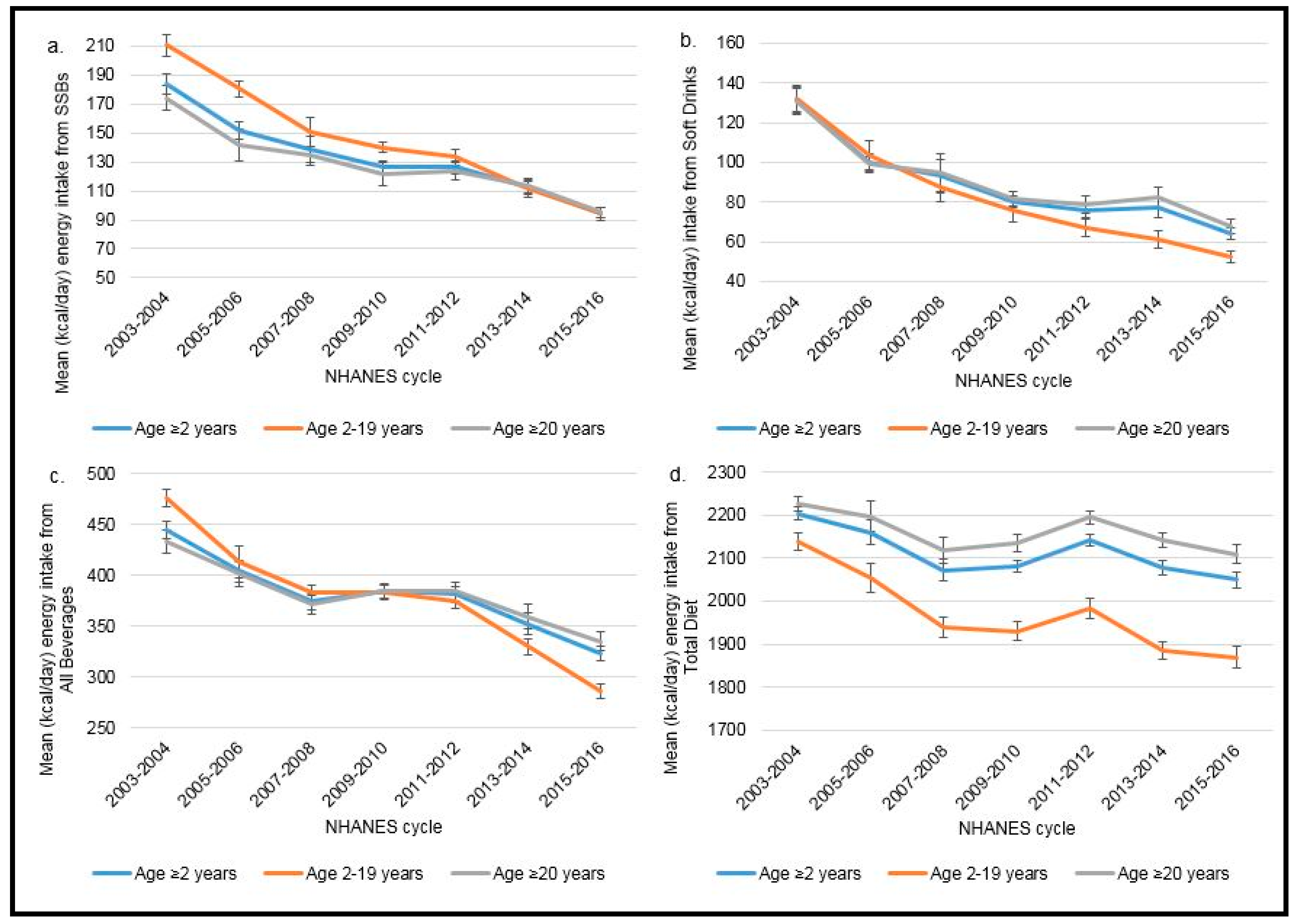
3.1. Trends in Estimated Mean Amount of Energy Intake by Age Group
3.2. Trends in Average Percentage of Estimated Daily Energy Intake by Age Group
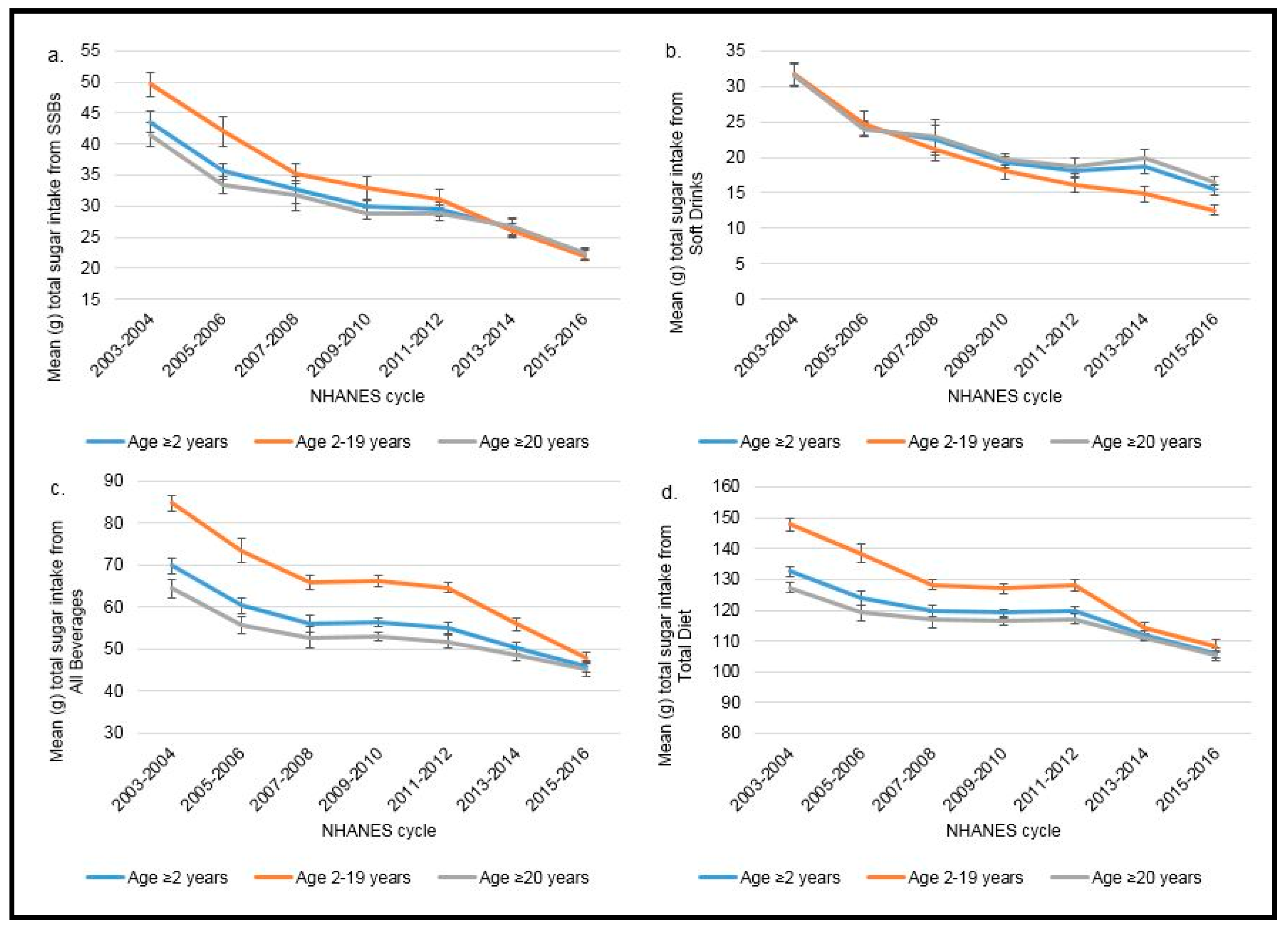
3.3. Trends in Estimated Mean Total Sugar Intake by Age Group
3.4. Trends in Average Percentage of Total Sugar Intake from Consumption of SSBs, Soft Drinks, and All Beverages by Age Group
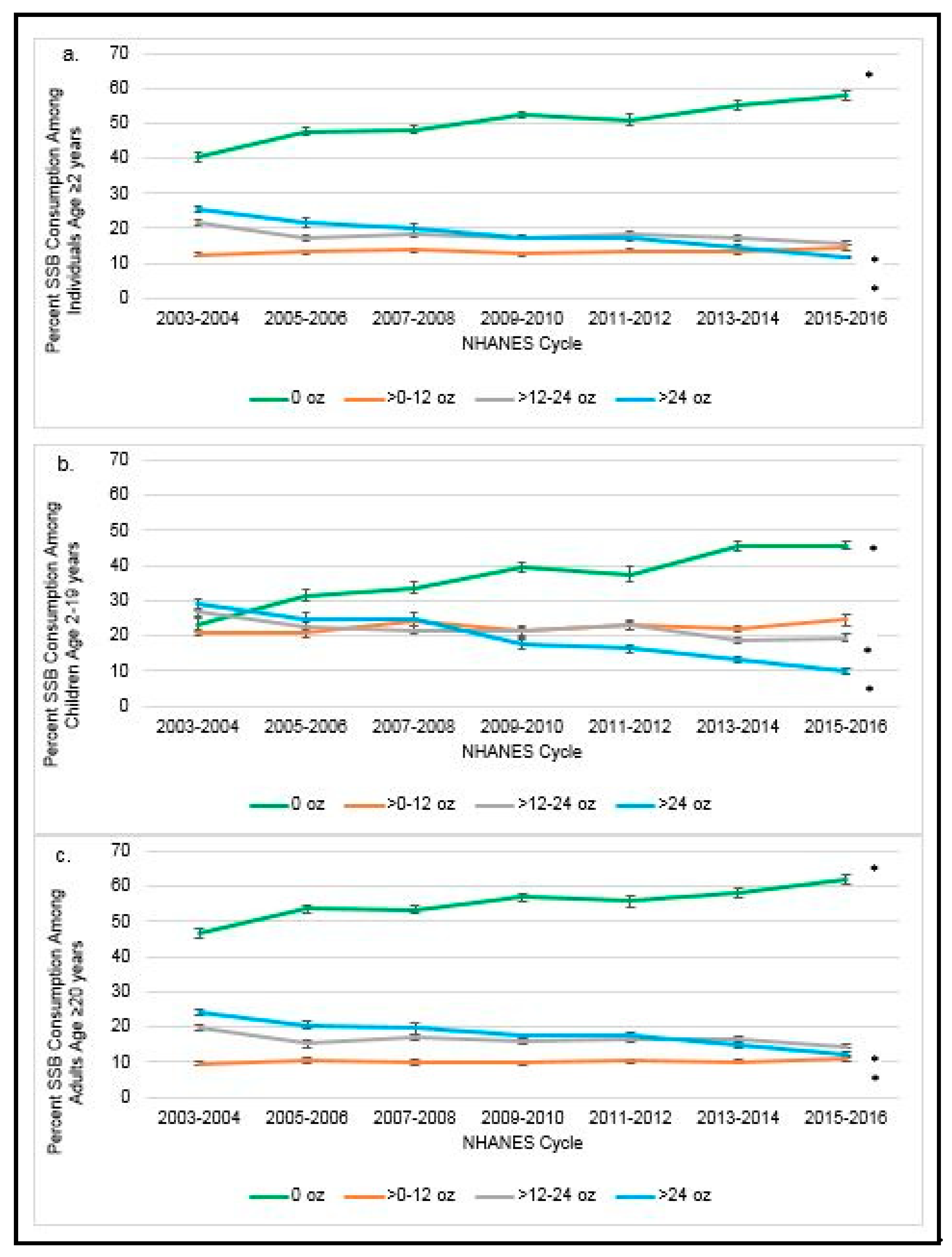
3.5. Percentage of SSB Consumers and Non-Consumers Over Time by Age Group and Tier of Consumption
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| AMPM | Automated Multiple-Pass Method |
| CDC | Center for Disease Control and Prevention |
| CVD | Cardiovascular disease |
| FNDDS | Food and Nutrient Database for Dietary Studies |
| NCHS | National Center for Health Statistics |
| NHANES | National Health and Nutrition Examination Survey |
| NHIS | National Healthy Interview Study |
| SE | Standard error |
| SSBs | Sugar-sweetened beverages |
| US | United States |
| USDA | United States Department of Agriculture |
| WWEIA | What We Eat in America |
References
- Dietary Guidelines Advisory Committee. Scientific Report of the 2015 Dietary Guidelines Advisory Committee: Advisory Report to the Secretary of Health and Human Services and the Secretary of Agriculture; U.S. Department of Agriculture; Agricultural Research Service: Washington, DC, USA, 2015.
- Malik, V.S.; Pan, A.; Willett, W.C.; Hu, F.B. Sugar-sweetened beverages and weight gain in children and adults: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2013, 98, 1084–1102. [Google Scholar] [CrossRef] [PubMed]
- United States Department of Health and Human Services; United States Department of Agriculture. Dietary Guidelines for Americans, 2015–2020, 8th ed.; Human Nutrition Information Service: Washington, DC, USA, 2015.
- Malik, V.S.; Popkin, B.M.; Bray, G.A.; Despres, J.P.; Willett, W.C.; Hu, F.B. Sugar-sweetened beverages and risk of metabolic syndrome and type 2 diabetes: A meta-analysis. Diabetes Care 2010, 33, 2477–2483. [Google Scholar] [CrossRef] [PubMed]
- Kit, B.K.; Fakhouri, T.H.; Park, S.; Nielsen, S.J.; Ogden, C.L. Trends in sugar-sweetened beverage consumption among youth and adults in the United States: 1999–2010. Am. J. Clin. Nutr. 2013, 98, 180–188. [Google Scholar] [CrossRef] [PubMed]
- Bernabe, E.; Vehkalahti, M.M.; Sheiham, A.; Aromaa, A.; Suominen, A.L. Sugar-sweetened beverages and dental caries in adults: A 4-year prospective study. J. Dent. 2014, 42, 952–958. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.M.; Micha, R.; Khatibzadeh, S.; Lim, S.; Ezzati, M.; Mozaffarian, D.; Global Burden of Diseases Nutrition and Chronic Diseases Expert Group. Estimated Global, Regional, and National Disease Burdens Related to Sugar-Sweetened Beverage Consumption in 2010. Circulation 2015, 132, 639–666. [Google Scholar] [CrossRef] [PubMed]
- Gamba, R.J.; Leung, C.W.; Petito, L.; Abrams, B.; Laraia, B.A. Sugar sweetened beverage consumption during pregnancy is associated with lower diet quality and greater total energy intake. PLoS ONE 2019, 14, e0215686. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.S.; Li, Y.; Pan, A.; De Koning, L.; Schernhammer, E.; Willett, W.C.; Hu, F.B. Long-Term Consumption of Sugar-Sweetened and Artificially Sweetened Beverages and Risk of Mortality in US Adults. Circulation 2019, 139, 2113–2125. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; McGuire, L.C.; Galuska, D.A. Regional Differences in Sugar-Sweetened Beverage Intake among US Adults. J. Acad. Nutr. Diet. 2015, 115, 1996–2002. [Google Scholar] [CrossRef] [PubMed]
- De Ruyter, J.C.; Olthof, M.R.; Seidell, J.C.; Katan, M.B. A trial of sugar-free or sugar-sweetened beverages and body weight in children. N. Engl. J. Med. 2012, 367, 1397–1406. [Google Scholar] [CrossRef] [PubMed]
- Bleich, S.N.; Vercammen, K.A.; Koma, J.W.; Li, Z. Trends in Beverage Consumption Among Children and Adults, 2003–2014. Obesity 2018, 26, 432–441. [Google Scholar] [CrossRef] [PubMed]
- Mendez, M.A.; Miles, D.R.; Poti, J.M.; Sotres-Alvarez, D.; Popkin, B.M. Persistent disparities over time in the distribution of sugar-sweetened beverage intake among children in the United States. Am. J. Clin. Nutr 2019, 109, 79–89. [Google Scholar] [CrossRef] [PubMed]
- Mela, D.J.; Woolner, E.M. Perspective: Total, Added, or Free? What Kind of Sugars Should We Be Talking About? Adv. Nutr. 2018, 9, 63–69. [Google Scholar] [CrossRef] [PubMed]
- USA Department of Agriculture; Agricultural Research Service. What We Eat in America, NHANES 2009–2010, 2011–2012. Beltsville Human Nutrition Research Center. Available online: https://wwwn.cdc.gov/nchs/nhanes/default.aspx (accessed on 5 August 2018).
- National Center for Health Statistics. About the National Health and Nutrition Examination Survey. Available online: http://www.cdc.gov/nchs/nhanes/about_nhanes.htm (accessed on 18 June 2018).
- Ahuja, J.K.C.; Montvile, B.J.; Omolewa-Tomobi, G.; Heendeniya, K.Y.; Martin, C.L.; Steinfeldt, L.C.; Anand, J.; Adler, M.E.; LaComb, R.P.; Moshfegh, A.J. USDA Food and Nutrient Database for Dietary Studies. Available online: http://www.ars.usda.gov/SP2UserFiles/Place/80400530/pdf/fndds/fndds5_doc.pdf#page=64 (accessed on 1 January 2019).
- Ahuja, J.K.C.; Montvile, B.J.; Omolewa-Tomobi, G.; Heendeniya, K.Y.; Martin, C.L.; Steinfeldt, L.C.; Anand, J.; Adler, M.E.; LaComb, R.P.; Moshfegh, A.J. Appendix, C. Dietary Methods Research: Overview of What We Eat in America Food Categories: FSRG-Defined Food Groups. Available online: http://www.ars.usda.gov/SP2UserFiles/Place/80400530/pdf/fndds/fndds5_doc.pdf#page=64 (accessed on 1 January 2019).
- CDC, National Center for Health Statistics, National Health and Examination Survey. Survey Methods and Analytic Guidelines. Available online: https://wwwn.cdc.gov/nchs/nhanes/analyticguidelines.aspx (accessed on 18 July 2018).
- Johnson, C.L.; Paulose-Ram, R.; Ogden, C.L.; Carroll, M.D.; Kruszon-Moran, D.; Dohrmann, S.M.; Curtin, L.R. National Health and Nutrition Examination Survey: Analytic Guidelines 1999–2010. Division of Health and Nutrition Examination Surveys; National Center for Health Statistics: Hyattsville, MD, USA, 2013; p. 17.
- CDC. National Health and Nutrition Examination Survey: Analytic Guidelines 2011–2012. Division of Health and Nutrition Examination Surveys; National Center for Health Statistics: Hyattsville, MD, USA, 2013; p. 13.
- CDC National Center for Health Statistics. NHANES Response Rates. Available online: http://www.cdc.gov/nchs/nhanes/response_rates_CPS.htm (accessed on 20 December 2018).
- Marteau, T.M.; Hollands, G.J.; Shemilt, I.; Jebb, S.A. Downsizing: Policy options to reduce portion sizes to help tackle obesity. BMJ 2015, 351, h5863. [Google Scholar] [CrossRef] [PubMed]
- Young, L.; Nestle, M. Portion sizes and obesity: Responses of fast-food companies. J. Public Health Policy 2007, 28, 238–248. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, M.B.; Schneider, G.E.; Choi, Y.Y.; Li, X.; Harris, J.; Andreyeva, T.; Hyary, M.; Highsmith Vernick, N.; Appel, L.J. Association of a Community Campaign for Better Beverage Choices With Beverage Purchases From Supermarkets. JAMA Intern. Med. 2017, 177, 666–674. [Google Scholar] [CrossRef] [PubMed]
- Hardy, L.L.; Bell, J.B.; Bauman, A.; Mihrshahi, S. Association between adolescents’ consumption of total and different types of sugar-sweetened beverages and oral health impacts and weight status. Aust. N. Z. J. Public Health 2018, 42, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.S.; Schulze, M.B.; Hu, F.B. Intake of sugar-sweetened beverages and weight gain: A systematic review. Am. J. Clin. Nutr. 2006, 84, 274–288. [Google Scholar] [CrossRef] [PubMed]
- Briefel, R.R.; Sempos, C.T.; McDowell, M.A.; Chien, S.; Alaimo, K. Dietary methods research in the third National Health and Nutrition Examination Survey: Underreporting of energy intake. Am. J. Clin. Nutr. 1997, 65, 1203S–1209S. [Google Scholar] [CrossRef] [PubMed]
- Moshfegh, A.J.; Rhodes, D.G.; Baer, D.J.; Murayi, T.; Clemens, J.C.; Rumpler, W.V.; Paul, D.R.; Sebastian, R.S.; Kuczynski, K.J.; Ingwersen, L.A.; et al. The US Department of Agriculture Automated Multiple-Pass Method reduces bias in the collection of energy intakes. Am. J. Clin. Nutr. 2008, 88, 324–332. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Guideline: Sugars Intake for Adults and Children; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Lichtenstein, A.H. Last Nail in the Coffin for Sugar-Sweetened Beverages. Circulation 2019, 139, 2126–2128. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| 2003–2004 | 2005–2006 | 2007–2008 | 2009–2010 | 2011–2012 | 2013–2014 | 2015–2016 | p-Value 4 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % | SE | % | SE | % | SE | % | SE | % | SE | % | SE | % | SE | ||
| % Energy Intake from SSBs (kcal/day) 5 | |||||||||||||||
| ≥2 years old | 8.1 | 0.3 | 6.8 | 0.2 | 6.5 | 0.4 | 5.8 | 0.2 | 5.8 | 0.2 | 5.3 | 0.2 | 4.5 | 0.1 | <0.0001 |
| 2–19 years old | 9.8 | 0.5 | 8.5 | 0.4 | 7.6 | 0.4 | 6.9 | 0.4 | 6.6 | 0.2 | 5.8 | 0.4 | 5.0 | 0.2 | <0.0001 |
| 6–11 years old | 8.6 | 0.6 | 6.7 | 0.4 | 6.9 | 0.4 | 5.9 | 0.3 | 6.0 | 0.3 | 5.1 | 0.4 | 4.9 | 0.3 | <0.0001 |
| 12–19 years old | 12.2 | 0.6 | 11.2 | 0.5 | 9.5 | 0.6 | 8.9 | 0.7 | 8.2 | 0.4 | 7.4 | 0.5 | 6.0 | 0.3 | <0.0001 |
| ≥20 years old | 7.5 | 0.3 | 6.2 | 0.2 | 6.1 | 0.4 | 5.4 | 0.2 | 5.5 | 0.2 | 5.1 | 0.2 | 4.3 | 0.2 | <0.0001 |
| % Energy Intake from Soft Drinks (kcal/ day) 5 | |||||||||||||||
| ≥2 years old | 5.7 | 0.3 | 4.4 | 0.2 | 4.3 | 0.4 | 3.6 | 0.2 | 3.5 | 0.2 | 3.5 | 0.2 | 3.0 | 0.1 | <0.0001 |
| 2–19 years old | 6.1 | 0.4 | 4.6 | 0.3 | 4.3 | 0.4 | 3.6 | 0.3 | 3.4 | 0.2 | 3.0 | 0.2 | 2.7 | 0.1 | <0.0001 |
| 6–11 years old | 5.3 | 0.5 | 3.1 | 0.2 | 3.6 | 0.3 | 2.7 | 0.2 | 2.7 | 0.3 | 2.4 | 0.3 | 2.4 | 0.2 | <0.0001 |
| 12–19 years old | 8.6 | 0.6 | 7.2 | 0.4 | 6.2 | 0.6 | 5.6 | 0.6 | 4.8 | 0.3 | 4.5 | 0.3 | 3.9 | 0.2 | <0.0001 |
| ≥20 years old | 5.5 | 0.3 | 4.3 | 0.2 | 4.3 | 0.4 | 3.6 | 0.2 | 3.6 | 0.2 | 3.7 | 0.2 | 3.1 | 0.1 | <0.0001 |
| % Energy Intake from All Beverages (kcal/ day) | |||||||||||||||
| ≥2 years old | 19.6 | 0.4 | 18.3 | 0.4 | 17.8 | 0.3 | 18.0 | 0.3 | 17.6 | 0.3 | 16.6 | 0.4 | 15.4 | 0.3 | <0.0001 |
| 2–19 years old | 22.6 | 0.4 | 20.3 | 0.5 | 20.4 | 0.4 | 20.1 | 0.3 | 19.6 | 0.4 | 18.0 | 0.5 | 15.8 | 0.4 | <0.0001 |
| 6–11 years old | 21.1 | 0.7 | 18.1 | 0.7 | 19.0 | 0.4 | 18.8 | 0.4 | 18.1 | 0.5 | 16.8 | 0.4 | 15.2 | 0.5 | <0.0001 |
| 12–19 years old | 22.1 | 0.5 | 19.9 | 0.5 | 19.5 | 0.6 | 19.3 | 0.5 | 19.0 | 0.5 | 18.0 | 0.7 | 15.1 | 0.6 | <0.0001 |
| ≥20 years old | 18.5 | 0.4 | 17.5 | 0.5 | 16.9 | 0.4 | 17.3 | 0.3 | 17.0 | 0.3 | 16.1 | 0.4 | 15.3 | 0.4 | <0.0001 |
| 2003–2004 | 2005–2006 | 2007–2008 | 2009–2010 | 2011–2012 | 2013–2014 | 2015–2016 | p-Value 4 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| % | SE | % | SE | % | SE | % | SE | % | SE | % | SE | % | SE | ||
| % Total Sugar Intake from SSBs 5 | |||||||||||||||
| ≥2 years old | 29.9 | 0.9 | 23.0 | 0.8 | 21.8 | 1.0 | 19.9 | 0.5 | 20.2 | 0.7 | 18.6 | 0.8 | 16.5 | 0.6 | <0.0001 |
| 2–19 years old | 30.7 | 1.2 | 27.2 | 1.1 | 24.7 | 1.1 | 22.4 | 1.0 | 22.4 | 1.0 | 19.9 | 1.0 | 18.5 | 0.6 | <0.0001 |
| 6–11 years old | 27.3 | 1.4 | 21.4 | 1.1 | 22.6 | 1.1 | 19.7 | 1.2 | 20.3 | 1.1 | 17.8 | 1.2 | 18.1 | 1.1 | <0.0001 |
| 12–19 years old | 38.7 | 1.8 | 36.7 | 1.5 | 30.9 | 1.6 | 29.0 | 1.6 | 28.4 | 1.5 | 25.2 | 1.2 | 22.9 | 0.9 | <0.0001 |
| ≥20 years old | 25.6 | 0.9 | 21.6 | 0.9 | 20.8 | 1.0 | 19.1 | 0.6 | 19.4 | 0.8 | 18.2 | 0.9 | 15.8 | 0.6 | <0.0001 |
| % Total Sugar Intake from Soft Drinks 5 | |||||||||||||||
| ≥2 years old | 19.5 | 0.8 | 15.4 | 0.6 | 14.8 | 1.1 | 12.7 | 0.5 | 12.7 | 0.6 | 12.7 | 0.6 | 11.1 | 0.4 | <0.0001 |
| 2–19 years old | 19.7 | 1.0 | 15.9 | 0.9 | 14.2 | 1.1 | 11.9 | 0.7 | 11.8 | 0.8 | 10.8 | 0.7 | 10.4 | 0.5 | <0.0001 |
| 6–11 years old | 17.4 | 1.3 | 10.6 | 0.8 | 12.1 | 1.0 | 9.3 | 0.8 | 9.5 | 1.0 | 8.3 | 0.9 | 9.1 | 0.8 | <0.0001 |
| 12–19 years old | 27.8 | 1.7 | 24.8 | 1.2 | 20.3 | 1.8 | 18.0 | 1.2 | 17.3 | 1.3 | 16.0 | 1.0 | 14.8 | 0.8 | <0.0001 |
| ≥20 years old | 19.4 | 0.8 | 15.2 | 0.6 | 15.0 | 1.1 | 12.9 | 0.5 | 13.0 | 0.7 | 13.3 | 0.7 | 11.4 | 0.5 | <0.0001 |
| % Total Sugar Intake from All Beverages | |||||||||||||||
| ≥2 years old | 46.4 | 0.7 | 42.6 | 1.0 | 41.5 | 0.8 | 41.4 | 0.5 | 40.6 | 0.8 | 38.7 | 0.8 | 36.9 | 0.8 | <0.0001 |
| 2–19 years old | 55.4 | 0.7 | 50.5 | 1.0 | 49.8 | 1.0 | 49.2 | 0.6 | 48.9 | 0.8 | 46.1 | 1.0 | 42.8 | 1.2 | <0.0001 |
| 6–11 years old | 51.3 | 1.1 | 44.2 | 1.7 | 46.7 | 1.3 | 46.3 | 1.1 | 45.5 | 1.0 | 43.1 | 1.0 | 41.1 | 1.6 | <0.0001 |
| 12–19 years old | 58.9 | 1.1 | 55.0 | 0.9 | 52.0 | 1.2 | 51.5 | 0.8 | 52.1 | 1.0 | 48.9 | 1.2 | 44.7 | 1.5 | <0.0001 |
| ≥20 years old | 43.1 | 0.9 | 39.8 | 1.1 | 39.0 | 0.8 | 38.7 | 0.9 | 37.8 | 0.9 | 36.4 | 0.8 | 35.0 | 0.8 | <0.0001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marriott, B.P.; Hunt, K.J.; Malek, A.M.; Newman, J.C. Trends in Intake of Energy and Total Sugar from Sugar-Sweetened Beverages in the United States among Children and Adults, NHANES 2003–2016. Nutrients 2019, 11, 2004. https://doi.org/10.3390/nu11092004
Marriott BP, Hunt KJ, Malek AM, Newman JC. Trends in Intake of Energy and Total Sugar from Sugar-Sweetened Beverages in the United States among Children and Adults, NHANES 2003–2016. Nutrients. 2019; 11(9):2004. https://doi.org/10.3390/nu11092004
Chicago/Turabian StyleMarriott, Bernadette P., Kelly J. Hunt, Angela M. Malek, and Jill C. Newman. 2019. "Trends in Intake of Energy and Total Sugar from Sugar-Sweetened Beverages in the United States among Children and Adults, NHANES 2003–2016" Nutrients 11, no. 9: 2004. https://doi.org/10.3390/nu11092004
APA StyleMarriott, B. P., Hunt, K. J., Malek, A. M., & Newman, J. C. (2019). Trends in Intake of Energy and Total Sugar from Sugar-Sweetened Beverages in the United States among Children and Adults, NHANES 2003–2016. Nutrients, 11(9), 2004. https://doi.org/10.3390/nu11092004