Effects of a Cod Protein Hydrolysate Supplement on Symptoms, Gut Integrity Markers and Fecal Fermentation in Patients with Irritable Bowel Syndrome

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
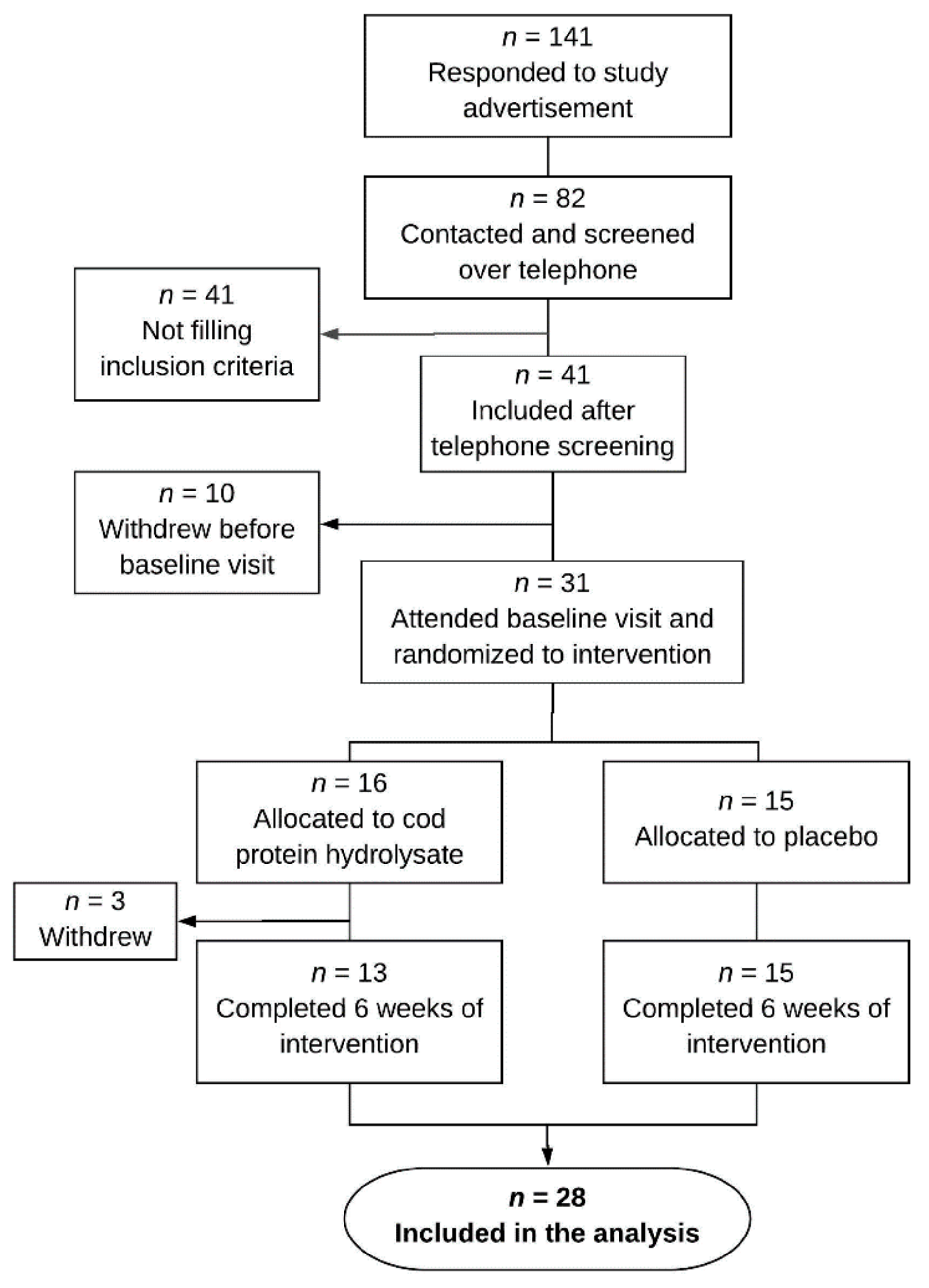
2.1. Patients
2.2. Study Design and Protocol
2.3. Test Material
2.4. Blood Samples
2.5. Fecal Samples
2.6. Symptom Questionnaires
2.7. Estimation of Nutritional Intake
2.8. Statistical Analysis
3. Results
3.1. Patient Characteristics
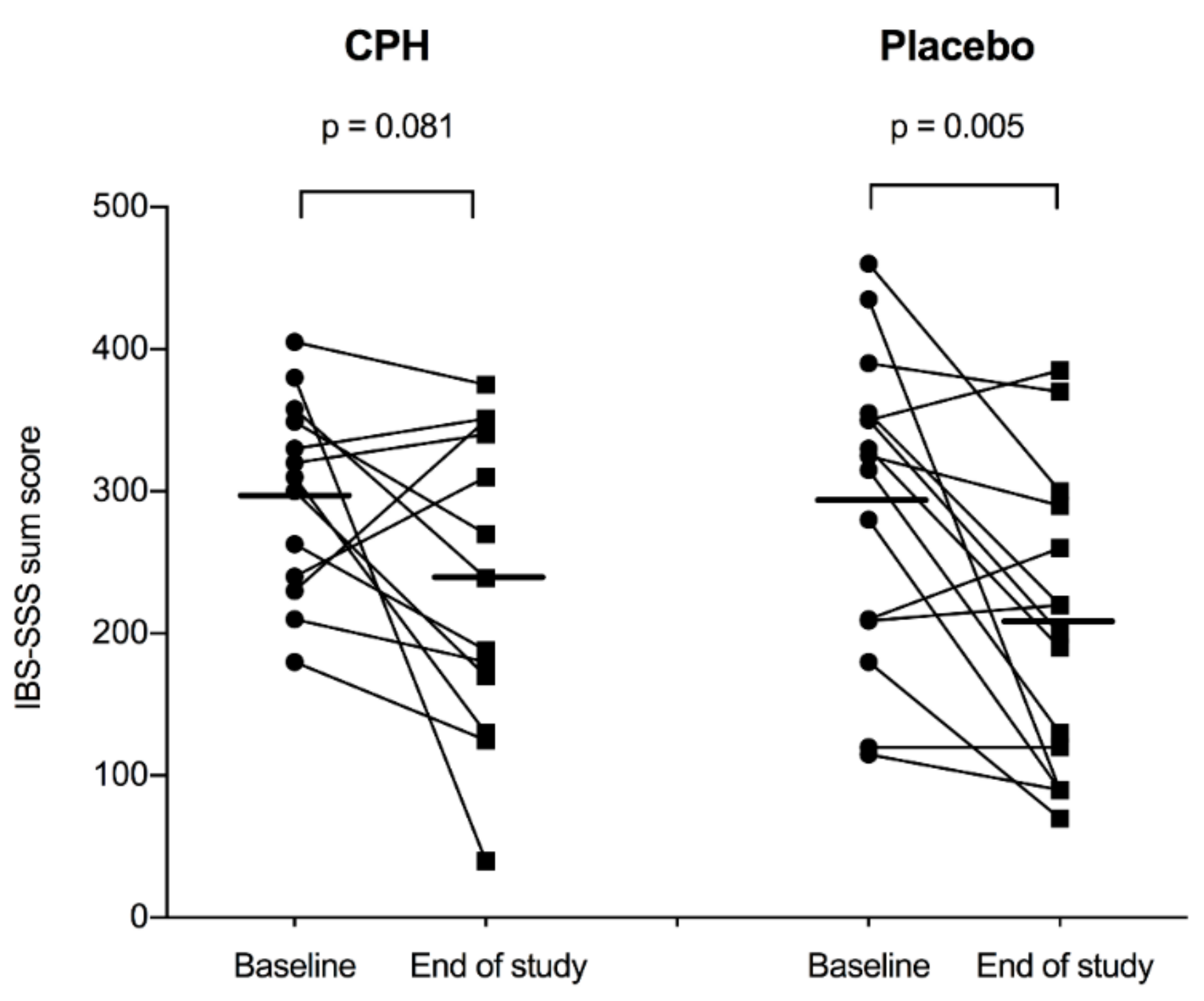
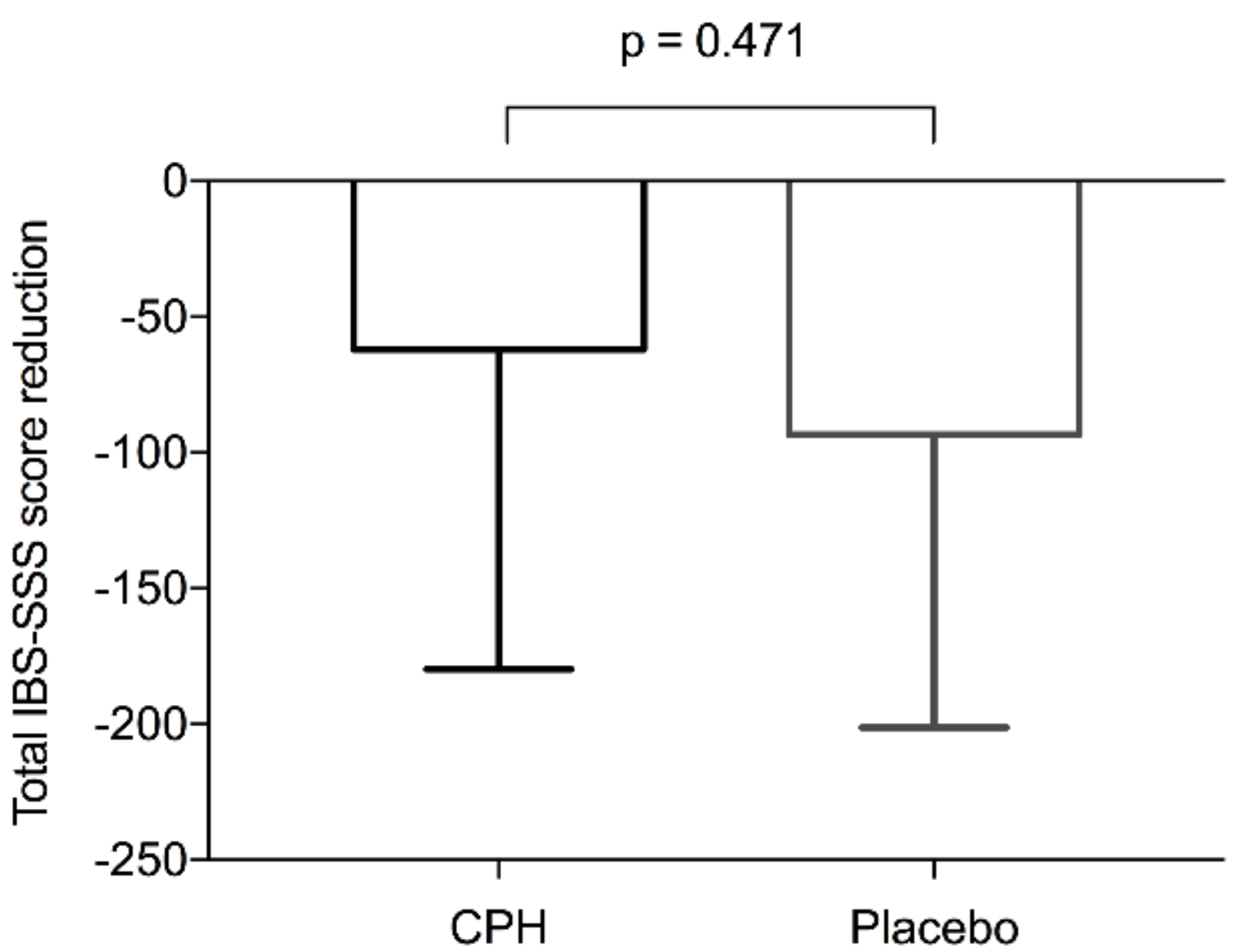
3.2. Irritable Bowel Syndrome Symptom Scores and Quality of Life
3.3. Gut Integrity Markers and Pro-Inflammatory Cytokines in Serum
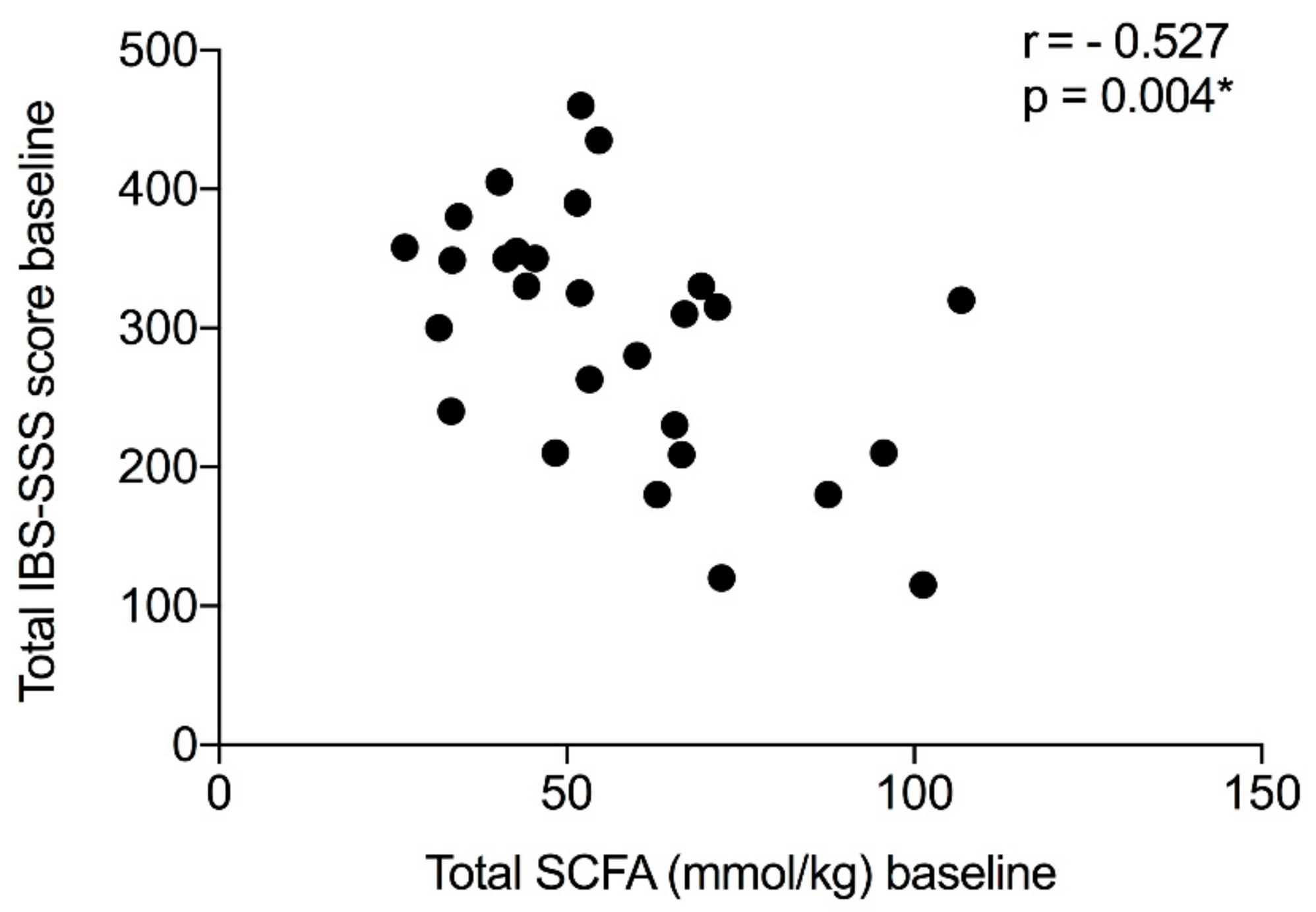
3.4. Fecal SCFAs
3.5. Fecal Calprotectin
3.6. Dietary Records
3.7. Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sperber, A.D.; Dumitrascu, D.; Fukudo, S.; Gerson, C.; Ghoshal, U.C.; Gwee, K.A.; Hungin, A.P.S.; Kang, J.Y.; Minhu, C.; Schmulson, M.; et al. The global prevalence of IBS in adults remains elusive due to the heterogeneity of studies: A Rome foundation working team literature review. Gut 2017, 66, 1075–1082. [Google Scholar] [CrossRef] [PubMed]
- Marsh, A.; Eslick, E.M.; Eslick, G.D. Does a diet low in FODMAPs reduce symptoms associated with functional gastrointestinal disorders? A comprehensive systematic review and meta-analysis. Eur. J. Nutr. 2016, 55, 897–906. [Google Scholar] [CrossRef] [PubMed]
- Andrews, E.B.; Eaton, S.C.; Hollis, K.A.; Hopkins, J.S.; Ameen, V.; Hamm, L.R.; Cook, S.F.; Tennis, P.; Mangel, A.W. Prevalence and demographics of irritable bowel syndrome: Results from a large web-based survey. Aliment. Pharmacol. Ther. 2005, 22, 935–942. [Google Scholar] [CrossRef] [PubMed]
- El-Salhy, M. Irritable bowel syndrome: Diagnosis and pathogenesis. World J. Gastroenterol. 2012, 18, 5151–5163. [Google Scholar] [PubMed]
- El-Salhy, M.; Hatlebakk, J.G.; Gilja, O.H.; Hausken, T. Irritable bowel syndrome: Recent developments in diagnosis, pathophysiology, and treatment. Expert Rev. Gastroenterol. Hepatol. 2014, 8, 435–443. [Google Scholar] [CrossRef] [PubMed]
- Eswaran, S.; Tack, J.; Chey, W.D. Food: The forgotten factor in the irritable bowel syndrome. Gastroenterol. Clin. North. Am. 2011, 40, 141–162. [Google Scholar] [CrossRef] [PubMed]
- King, T.S.; Elia, M.; Hunter, J.O. Abnormal colonic fermentation in irritable bowel syndrome. Lancet 1998, 352, 1187–1189. [Google Scholar] [CrossRef]
- Tana, C.; Umesaki, Y.; Imaoka, A.; Handa, T.; Kanazawa, M.; Fukudo, S. Altered profiles of intestinal microbiota and organic acids may be the origin of symptoms in irritable bowel syndrome. Neurogastroenterol. Motil. 2010, 22, 512–519, e114-5. [Google Scholar] [CrossRef]
- Tan, J.; McKenzie, C.; Potamitis, M.; Thorburn, A.N.; Mackay, C.R.; Macia, L. The role of short-chain fatty acids in health and disease. Adv. Immunol. 2014, 121, 91–119. [Google Scholar]
- Valeur, J.; Smastuen, M.C.; Knudsen, T.; Lied, G.A.; Roseth, A.G. Exploring gut microbiota composition as an indicator of clinical response to dietary FODMAP restriction in patients with irritable bowel syndrome. Dig. Dis. Sci. 2018, 63, 429–436. [Google Scholar] [CrossRef]
- Daien, C.I.; Pinget, G.V.; Tan, J.K.; Macia, L. Detrimental impact of microbiota-accessible carbohydrate-deprived diet on gut and immune homeostasis: An overview. Front. Immunol. 2017, 8, 548. [Google Scholar] [CrossRef] [PubMed]
- Le Gouic, A.V.; Harnedy, P.A.; FitzGerald, R.J. Bioactive peptides from fish protein by-products. In Bioactive Molecules in Food; Mérillon, J.M., Ramawat, K.G., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 355–388. [Google Scholar]
- Wergedahl, H.; Liaset, B.; Gudbrandsen, O.A.; Lied, E.; Espe, M.; Muna, Z.; Mork, S.; Berge, R.K. Fish protein hydrolysate reduces plasma total cholesterol, increases the proportion of HDL cholesterol, and lowers acyl-CoA: Cholesterol acyltransferase activity in liver of Zucker rats. J. Nutr. 2004, 134, 1320–1327. [Google Scholar] [CrossRef] [PubMed]
- Bjorndal, B.; Berge, C.; Ramsvik, M.S.; Svardal, A.; Bohov, P.; Skorve, J.; Berge, R.K. A fish protein hydrolysate alters fatty acid composition in liver and adipose tissue and increases plasma carnitine levels in a mouse model of chronic inflammation. Lipids Health Dis. 2013, 12, 143. [Google Scholar] [CrossRef]
- Drotningsvik, A.; Mjos, S.A.; Pampanin, D.M.; Slizyte, R.; Carvajal, A.; Remman, T.; Hogoy, I.; Gudbrandsen, O.A. Dietary fish protein hydrolysates containing bioactive motifs affect serum and adipose tissue fatty acid compositions, serum lipids, postprandial glucose regulation and growth in obese Zucker fa/fa rats. Br. J. Nutr. 2016, 116, 1336–1345. [Google Scholar] [CrossRef] [PubMed]
- Vildmyren, I.; Drotningsvik, A.; Oterhals, A.; Ween, O.; Halstensen, A.; Gudbrandsen, O.A. Cod residual protein prevented blood pressure increase in Zucker fa/fa rats, possibly by Inhibiting activities of angiotensin-converting enzyme and renin. Nutrients 2018, 10, 1820. [Google Scholar] [CrossRef]
- Dale, H.F.; Jensen, C.; Hausken, T.; Lied, E.; Hatlebakk, J.G.; Brønstad, I.; Lihaug Hoff, D.A.; Lied, G.A. Effect of a cod protein hydrolysate on postprandial glucose metabolism in healthy subjects: A double-blind cross-over trial. J. Nutr. Sci. 2018, 7, e33. [Google Scholar] [CrossRef] [PubMed]
- Nobile, V.; Duclos, E.; Michelotti, A.; Bizzaro, G.; Negro, M.; Soisson, F. Supplementation with a fish protein hydrolysate (Micromesistius poutassou): Effects on body weight, body composition, and CCK/GLP-1 secretion. Food Nutr. Res. 2016, 60, 29857. [Google Scholar] [CrossRef]
- Vikoren, L.A.; Nygard, O.K.; Lied, E.; Rostrup, E.; Gudbrandsen, O.A. A randomised study on the effects of fish protein supplement on glucose tolerance, lipids and body composition in overweight adults. Br. J. Nutr. 2013, 109, 648–657. [Google Scholar] [CrossRef]
- Vildmyren, I.; Cao, H.J.V.; Haug, L.B.; Valand, I.U.; Eng, O.; Oterhals, A.; Austgulen, M.H.; Halstensen, A.; Mellgren, G.; Gudbrandsen, O.A. Daily intake of protein from cod residual material lowers serum concentrations of nonesterified fatty acids in overweight healthy adults: A randomized double-blind pilot study. Mar. Drugs 2018, 16, 197. [Google Scholar] [CrossRef]
- Zaïr, Y.; Duclos, E.; Housez, B.; Vergara, C.; Cazaubiel, M.; Soisson, F. Evaluation of the satiating properties of a fish protein hydrolysate among overweight women: A pilot study. Nutr. Food Sci. 2014, 44, 389–399. [Google Scholar] [CrossRef]
- Marchbank, T.; Limdi, J.K.; Mahmood, A.; Elia, G.; Playford, R.J. Clinical trial: Protective effect of a commercial fish protein hydrolysate against indomethacin (NSAID)-induced small intestinal injury. Aliment. Pharmacol. Ther. 2008, 28, 799–804. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, A.J.; Rai, P.S.; Marchbank, T.; Taylor, G.W.; Ghosh, S.; Ritz, B.W.; Playford, R.J. Reparative properties of a commercial fish protein hydrolysate preparation. Gut 2005, 54, 775–781. [Google Scholar] [CrossRef] [PubMed]
- Barbaro, M.R.; Cremon, C.; Caio, G.; Bellacosa, L.; De Giorgio, R.; Volta, U.; Stanghellini, V.; Barbara, G. The role of zonulin in non-celiac gluten sensitivity and irritable bowel syndrome. In Proceedings of the 23rd United European Gastroenterology Week (UEG Week 2015), Barcelona, Spain, 24–27 October 2015. [Google Scholar]
- Dhillon, A.K.; Kummen, M.; Troseid, M.; Akra, S.; Liaskou, E.; Moum, B.; Vesterhus, M.; Karlsen, T.H.; Seljeflot, I.; Hov, J.R. Circulating markers of gut barrier function associated with disease severity in primary sclerosing cholangitis. Liver Int. 2019, 39, 371–381. [Google Scholar] [CrossRef] [PubMed]
- Undseth, R.; Berstad, A.; Valeur, J. Systemic symptoms in irritable bowel syndrome: An investigative study on the role of enterocyte disintegrity, endotoxemia and inflammation. Mol. Med. Rep. 2016, 14, 5072–5076. [Google Scholar] [CrossRef] [PubMed]
- Kabeerdoss, J.; Devi, R.S.; Mary, R.R.; Ramakrishna, B.S. Faecal microbiota composition in vegetarians: Comparison with omnivores in a cohort of young women in southern India. Br. J. Nutr. 2012, 108, 953–957. [Google Scholar] [CrossRef] [PubMed]
- Schmedes, M.; Brejnrod, A.D.; Aadland, E.K.; Kiilerich, P.; Kristiansen, K.; Jacques, H.; Lavigne, C.; Graff, I.E.; Eng, O.; Holthe, A.; et al. The effect of lean-seafood and non-seafood diets on fecal metabolites and gut microbiome: Results from a randomized crossover intervention study. Mol. Nutr. Food Res. 2019, 63, e1700976. [Google Scholar] [CrossRef] [PubMed]
- Mearin, F.; Lacy, B.E.; Chang, L.; Chey, W.D.; Lembo, A.J.; Simren, M.; Spiller, R. Bowel disorders. Gastroenterology 2016. [Google Scholar] [CrossRef]
- Zijlstra, J.B.; Beukema, J.; Wolthers, B.G.; Byrne, B.M.; Groen, A.; Dankert, J. Pretreatment methods prior to gaschromatographic analysis of volatile fatty acids from faecal samples. Clin. Chim. Acta 1977, 78, 243–250. [Google Scholar] [CrossRef]
- Hoverstad, T.; Fausa, O.; Bjorneklett, A.; Bohmer, T. Short-chain fatty acids in the normal human feces. Scand. J. Gastroenterol. 1984, 19, 375–381. [Google Scholar] [CrossRef]
- Francis, C.Y.; Morris, J.; Whorwell, P.J. The irritable bowel severity scoring system: A simple method of monitoring irritable bowel syndrome and its progress. Aliment. Parmacol. Ther. 1997, 11, 395–402. [Google Scholar] [CrossRef]
- Arslan, G.; Lind, R.; Olafsson, S.; Florvaag, E.; Berstad, A. Quality of life in patients with subjective food hypersensitivity: Applicability of the 10-item short form of the Nepean Dyspepsia Index. Dig. Dis. Sci. 2004, 49, 680–687. [Google Scholar] [CrossRef] [PubMed]
- Elsenbruch, S.; Enck, P. Placebo effects and their determinants in gastrointestinal disorders. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 472–485. [Google Scholar] [CrossRef]
- Sun, Q.; Jia, Q.; Song, L.; Duan, L. Alterations in fecal short-chain fatty acids in patients with irritable bowel syndrome: A systematic review and meta-analysis. Medicine 2019, 98, e14513. [Google Scholar] [CrossRef]
- Hustoft, T.N.; Hausken, T.; Ystad, S.O.; Valeur, J.; Brokstad, K.; Hatlebakk, J.G.; Lied, G.A. Effects of varying dietary content of fermentable short-chain carbohydrates on symptoms, fecal microenvironment, and cytokine profiles in patients with irritable bowel syndrome. Neurogastroenterol. Motil. 2017, 29. [Google Scholar] [CrossRef] [PubMed]
- Valeur, J.; Roseth, A.G.; Knudsen, T.; Malmstrom, G.H.; Fiennes, J.T.; Midtvedt, T.; Berstad, A. Fecal fermentation in irritable bowel syndrome: Influence of dietary restriction of fermentable oligosaccharides, disaccharides, monosaccharides and polyols. Digestion 2016, 94, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Ajamian, M.; Steer, D.; Rosella, G.; Gibson, P.R. Serum zonulin as a marker of intestinal mucosal barrier function: May not be what it seems. PLoS ONE 2019, 14, e0210728. [Google Scholar] [CrossRef]
- Seyedmirzaee, S.; Hayatbakhsh, M.M.; Ahmadi, B.; Baniasadi, N.; Bagheri Rafsanjani, A.M.; Nikpoor, A.R.; Mohammadi, M. Serum immune biomarkers in irritable bowel syndrome. Clin. Res. Hepatol. Gastroenterol. 2016, 40, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Linsalata, M.; Riezzo, G.; D’Attoma, B.; Clemente, C.; Orlando, A.; Russo, F. Noninvasive biomarkers of gut barrier function identify two subtypes of patients suffering from diarrhoea predominant-IBS: A case-control study. BMC Gastroenterol. 2018, 18, 167. [Google Scholar] [CrossRef]
- Choghakhori, R.; Abbasnezhad, A.; Hasanvand, A.; Amani, R. Inflammatory cytokines and oxidative stress biomarkers in irritable bowel syndrome: Association with digestive symptoms and quality of life. Cytokine 2017, 93, 34–43. [Google Scholar] [CrossRef]
- Zhou, Q.; Verne, M.L.; Fields, J.Z.; Lefante, J.J.; Basra, S.; Salameh, H.; Verne, G.N. Randomised placebo-controlled trial of dietary glutamine supplements for postinfectious irritable bowel syndrome. Gut 2019, 68, 996–1002. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | CPH (n = 13) | Placebo (n = 15) | p-Value |
|---|---|---|---|
| Age, years | 42.7 (11.9) | 45.1 (14.8) | 0.647 |
| Gender (male/female) | 1/12 | 4/11 | - |
| BMI, kg/m2 | 24.1 (2.8) | 27.2 (3.9) | 0.025 * |
| IBS-D/IBS-M | 8/5 | 11/4 | - |
| IBS severity 1 mild | 0 | 2 | - |
| moderate | 5 | 4 | - |
| severe | 8 | 9 | - |
| IBS-SSS sum score (0–500) | 295 (107) | 298 (69) | 0.928 |
| Energy intake, kcal/day | 1750 (500) | 1950 (395) | 0.245 |
| Protein intake, g/kg BW/day | 1.2 (0.4) | 1.0 (0.3) | 0.185 |
| Carbohydrates, g/day | 140.0 (68.1) | 180.2 (53.6) | 0.093 |
| Fiber, g/day | 18.9 (7.6) | 17.9 (5.7) | 0.697 |
| Total FODMAP 2, g/day | 11.2 (6.6) | 13.0 (11.3) | 0.623 |
| Alcohol, g/day | 5.3 (6.8) | 6.2 (8.6) | 0.760 |
| Fat, g/day | 130.0 (190.5) | 91.7 (22.6) | 0.445 |
| CPH (n = 13) | Placebo (n = 15) | ||||||
|---|---|---|---|---|---|---|---|
| Symptom Scores | Baseline | End of Study | p-Value | Baseline | End of Study | p-Value | |
| IBS-SSS | Sum score | 298.1 (68.9) | 236.0 (105.9) | 0.081 | 294.9 (106.6) | 201.7 (103.6) | 0.005 * |
| Pain severity | 45.0 (25.1) | 39.2 (25.3) | 0.096 | 43.3 (33.3) | 25.0 (32.3) | 0.016 * | |
| Pain frequency | 45.4 (34.3) | 39.2 (25.3) | 0.446 | 47.3 (35.5) | 25.3 (28.5) | 0.018 * | |
| Bloating | 65.9 (18.5) | 46.0 (27.5) | 0.046 * | 59.3 (35.9) | 37.0 (31.1) | 0.038 * | |
| Bowel habit dissatisfaction | 77.1 (20.1) | 62.3 (30.8) | 0.059 | 73.7 (26.2) | 54.0 (30.1) | 0.034 * | |
| Life interference | 78.5 (17.1) | 57.4 (30.4) | 0.023 * | 71.3 (23.6) | 60.3 (22.2) | 0.034 * | |
| SF-NDI | Sum score | 28.0 (7.1) | 23.9 (9.1) | 0.104 | 24.1 (7.9) | 18.3 (7.9) | 0.042 * |
| CPH (n = 13) | Placebo (n = 15) | |||||
|---|---|---|---|---|---|---|
| Inflammatory Marker | Baseline | End of Study | p-Value | Baseline | End of Study | p-Value |
| iFABP (ng/mL) | 68.3 (43.2) | 58.2 (28.0) | 0.432 | 55.5 (20.1) | 56.2 (28.7) | 0.940 |
| LBP (ng/mL) | 6097 (2630) | 6446 (2043) | 0.355 | 6931 (3023) | 6884 (3274) | 0.925 |
| Zonulin (ng/mL) | 40.5 (5.6) | 42.5 (6.3) | 0.125 | 46.6 (5.9) | 45.7 (5.3) | 0.286 |
| IL-8 (pg/mL) | 8.8 (11.8) | 11.4 (10.1) | 0.185 | 7.4 (6.5) | 8.9 (9.1) | 0.413 |
| CPH (n = 13) | Placebo (n = 15) | |||||
|---|---|---|---|---|---|---|
| Parameter | Baseline | End of Study | p-Value | Baseline | End of Study | p-Value |
| Total SCFA | 51.8 (22.4) | 55.7 (24.1) | 0.591 | 62.6 (19.5) | 62.4 (23.1) | 0.997 |
| Acetic acid | 30.4 (12.3) | 32.2 (14.5) | 0.705 | 36.3 (11.9) | 35.9 (11.3) | 0.921 |
| Propionic acid | 9.9 (6.3) | 10.4 (6.7) | 0.768 | 10.7 (3.8) | 10.8 (6.0) | 0.963 |
| Butyric acid | 7.4 (3.9) | 8.5 (5.0) | 0.473 | 10.3 (4.5) | 10.0 (5.1) | 0.827 |
| Iso-butyric acid | 1.1 (0.5) | 1.3 (0.6) | 0.257 | 1.3 (0.7) | 1.4 (0.8) | 0.595 |
| Valeric acid | 1.1 (0.8) | 1.2 (0.6) | 0.785 | 1.7 (0.9) | 1.8 (1.0) | 0.805 |
| Iso-valeric acid | 1.6 (0.8) | 1.9 (1.0) | 0.322 | 1.9 (1.1) | 2.0 (1.3) | 0.554 |
| Caproic acid | 0.3 (0.5) | 0.3 (0.4) | 0.992 | 0.5 (0.5) | 0.6 (0.8) | 0.425 |
| Iso-caproic acid | 0.0 (0,0) | 0.0 (0.0) | - | 0.01 (0.04) | 0.01 (0.04) | 0.670 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dale, H.F.; Jensen, C.; Hausken, T.; Hatlebakk, J.G.; Brønstad, I.; Valeur, J.; Hoff, D.A.L.; Lied, G.A. Effects of a Cod Protein Hydrolysate Supplement on Symptoms, Gut Integrity Markers and Fecal Fermentation in Patients with Irritable Bowel Syndrome. Nutrients 2019, 11, 1635. https://doi.org/10.3390/nu11071635
Dale HF, Jensen C, Hausken T, Hatlebakk JG, Brønstad I, Valeur J, Hoff DAL, Lied GA. Effects of a Cod Protein Hydrolysate Supplement on Symptoms, Gut Integrity Markers and Fecal Fermentation in Patients with Irritable Bowel Syndrome. Nutrients. 2019; 11(7):1635. https://doi.org/10.3390/nu11071635
Chicago/Turabian StyleDale, Hanna Fjeldheim, Caroline Jensen, Trygve Hausken, Jan Gunnar Hatlebakk, Ingeborg Brønstad, Jørgen Valeur, Dag Arne Lihaug Hoff, and Gülen Arslan Lied. 2019. "Effects of a Cod Protein Hydrolysate Supplement on Symptoms, Gut Integrity Markers and Fecal Fermentation in Patients with Irritable Bowel Syndrome" Nutrients 11, no. 7: 1635. https://doi.org/10.3390/nu11071635
APA StyleDale, H. F., Jensen, C., Hausken, T., Hatlebakk, J. G., Brønstad, I., Valeur, J., Hoff, D. A. L., & Lied, G. A. (2019). Effects of a Cod Protein Hydrolysate Supplement on Symptoms, Gut Integrity Markers and Fecal Fermentation in Patients with Irritable Bowel Syndrome. Nutrients, 11(7), 1635. https://doi.org/10.3390/nu11071635