Citicoline: A Superior Form of Choline?


{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Citicoline in Food Supplements: The Issue of Health Claims
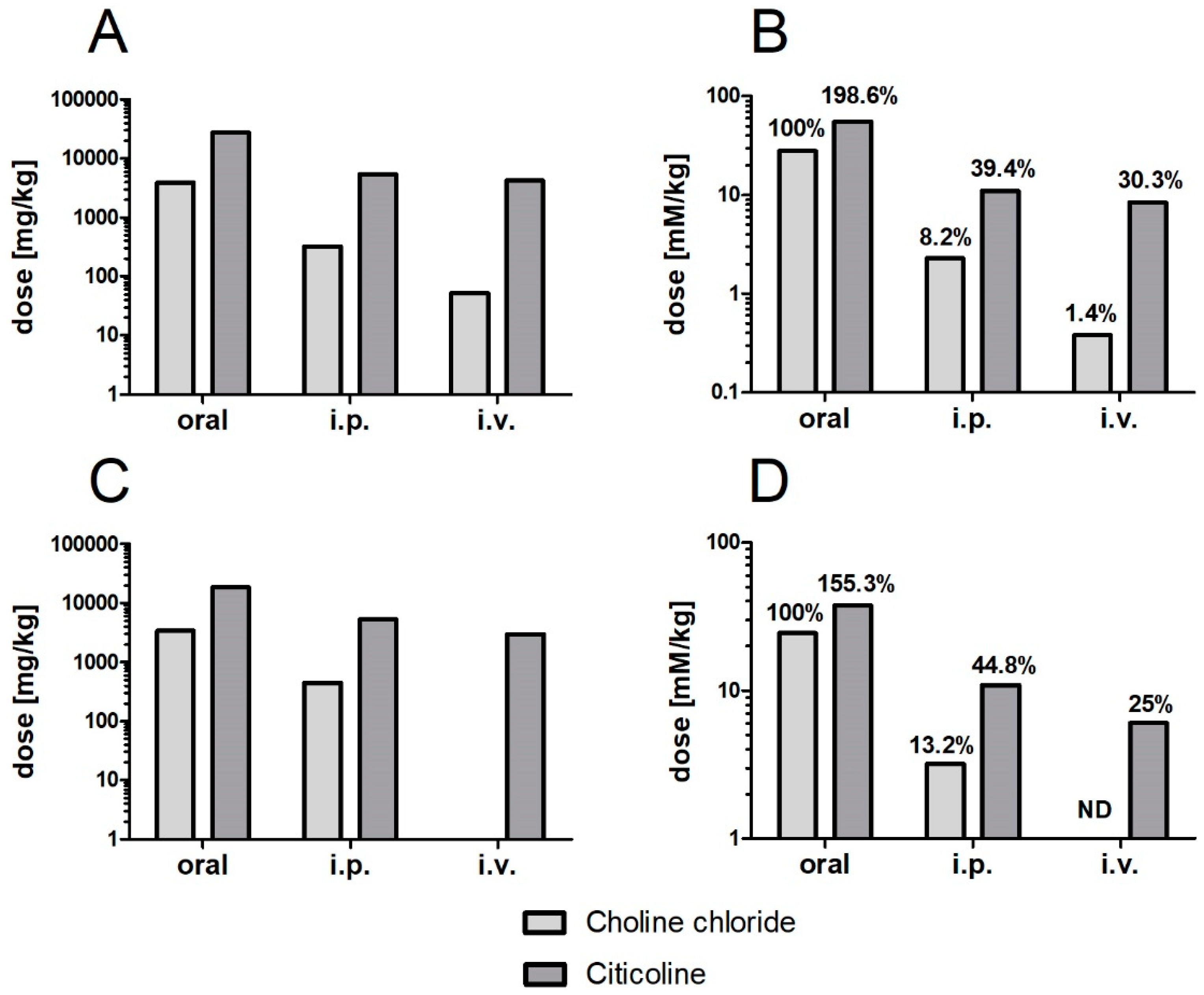
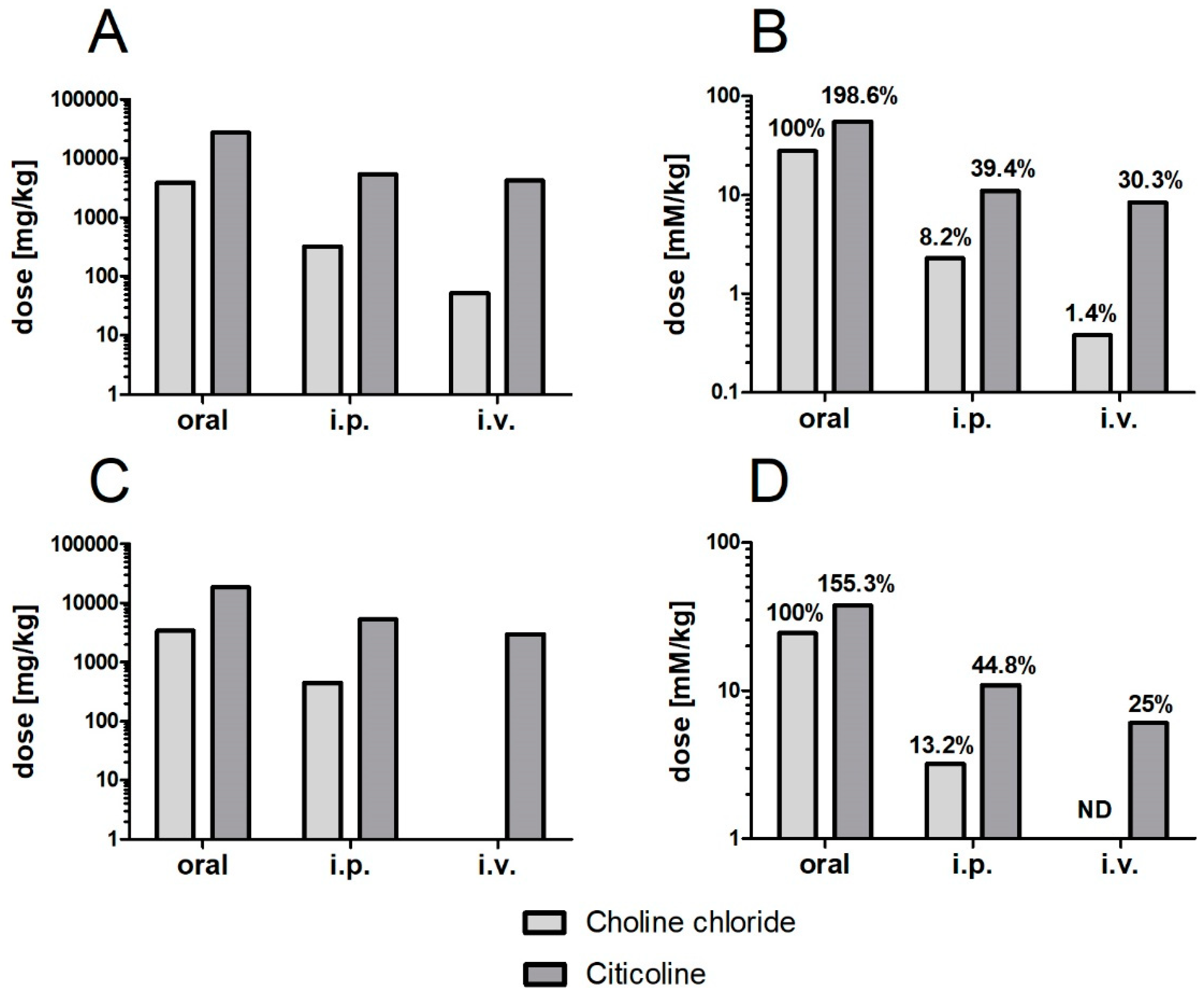
3. Citicoline as a Source of Choline: The Issue of Acute Toxicity
4. Does Resistance to Hydrolysis in the Intestine Make Citicoline a Safer Choline Supplement?
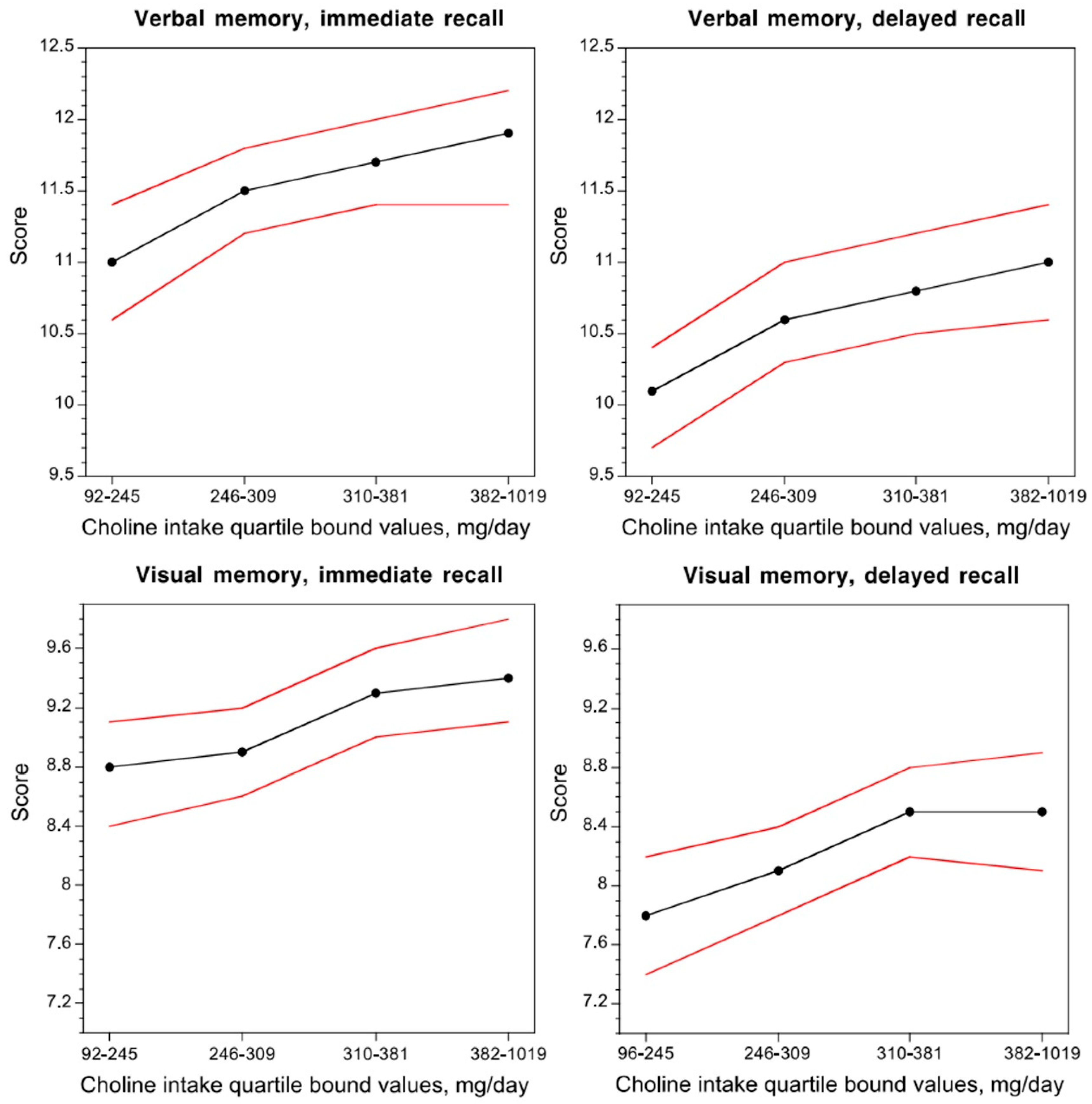
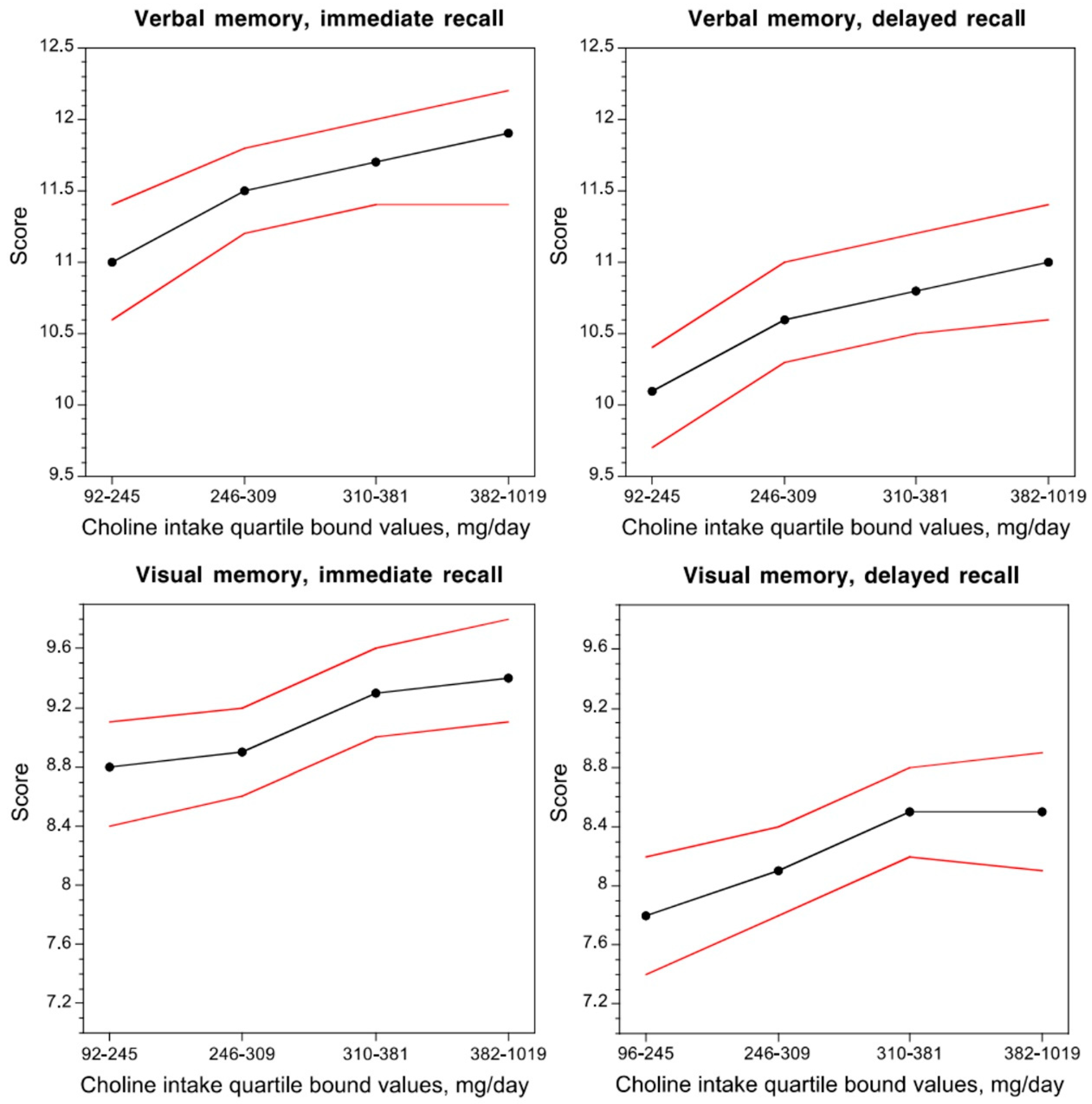
5. Citicoline: A “Procognitive” Form of Choline
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- WHO Collaborating Centre for Drug Statistics and Methodology. Available online: https://www.whocc.no/atc_ddd_index/?code=N06BX (accessed on 4 April 2019).
- Kyowa Hakko USA Announces GRAS Self-Affirmation for Novel Brain Health Ingredient Cognizin Citicoline. Available online: http://www.kyowa-usa.com/news/2009/05-28.html (accessed on 20 September 2014).
- Commission Implementing Decision of 1 July 2014 Authorising the Placing on the Market of Citicoline as a Novel Food Ingredient under Regulation (EC) No 258/97 of the European Parliament and of the Council. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX%3A32014D0423 (accessed on 7 June 2019).
- Regulation, E.C. No 1924/2006 of the European Parliament and of the Council of 20 December 2006 on Nutrition and Health Claims Made on Foods. Off. J. Eur. Union 2007, 12, 3–18. [Google Scholar]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Allergies. Scientific Opinion on the substantiation of a health claim related to cytidine 5-diphosphocholine and maintenance of normal vision pursuant to Article 13 (5) of Regulation (EC) No 1924/2006. EFSA J. 2014, 12, 3575. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on the safety of “citicoline” as a Novel Food ingredient. EFSA J. 2013, 11, 3421. [Google Scholar] [CrossRef]
- Lopez, G.C.I.; Agut, J.; Von Borstel, R.; Wurtman, R.J. Metabolism of cytidine (5?)-diphosphocholine (cdp-choline) following oral and intravenous administration to the human and the rat. Neurochem. Int. 1987, 11, 293–297. [Google Scholar] [CrossRef]
- Weiss, G.B. Metabolism and Actions of Cdp-Choline as an Endogenous Compound and Administered Exogenously as Citicoline. Life Sci. 1995, 56, 637–660. [Google Scholar] [CrossRef]
- Cansev, M. Uridine and cytidine in the brain: Their transport and utilization. Brain Res. Rev. 2006, 52, 389–397. [Google Scholar] [CrossRef]
- Buchman, A.L.; Ament, M.E.; Sohel, M.; Dubin, M.; Jenden, D.J.; Roch, M.; Pownall, H.; Farley, W.; Awal, M.; Ahn, C. Choline deficiency causes reversible hepatic abnormalities in patients receiving parenteral nutrition: Proof of a human choline requirement: A placebo-controlled trial. JPEN J. Parenter. Enter. Nutr. 2001, 25, 260–268. [Google Scholar] [CrossRef]
- Buchman, A.L.; Dubin, M.D.; Moukarzel, A.A.; Jenden, D.J.; Roch, M.; Rice, K.M.; Gornbein, J.; Ament, M.E. Choline deficiency: A cause of hepatic steatosis during parenteral nutrition that can be reversed with intravenous choline supplementation. Hepatology 1995, 22, 1399–1403. [Google Scholar]
- Da Costa, K.A.; Gaffney, C.E.; Fischer, L.M.; Zeisel, S.H. Choline deficiency in mice and humans is associated with increased plasma homocysteine concentration after a methionine load. Am. J. Clin. Nutr. 2005, 81, 440–444. [Google Scholar] [CrossRef] [Green Version]
- Cho, E.; Zeisel, S.H.; Jacques, P.; Selhub, J.; Dougherty, L.; Colditz, G.A.; Willett, W.C. Dietary choline and betaine assessed by food-frequency questionnaire in relation to plasma total homocysteine concentration in the Framingham Offspring Study. Am. J. Clin. Nutr. 2006, 83, 905–911. [Google Scholar] [CrossRef] [Green Version]
- Dalmeijer, G.W.; Olthof, M.R.; Verhoef, P.; Bots, M.L.; van der Schouw, Y.T. Prospective study on dietary intakes of folate, betaine, and choline and cardiovascular disease risk in women. Eur. J. Clin. Nutr. 2008, 62, 386–394. [Google Scholar] [CrossRef] [PubMed]
- Olthof, M.R.; Brink, E.J.; Katan, M.B.; Verhoef, P. Choline supplemented as phosphatidylcholine decreases fasting and postmethionine-loading plasma homocysteine concentrations in healthy men. Am. J. Clin. Nutr. 2005, 82, 111–117. [Google Scholar] [CrossRef] [PubMed]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on the substantiation of health claims related to choline and contribution to normal lipid metabolism (ID 3186), maintenance of normal liver function (ID 1501), contribution to normal homocysteine metabolism (ID 3090), maintenance of normal neurological function (ID 1502), contribution to normal cognitive function (ID 1502), and brain and neurological development (ID 1503) pursuant to Article 13(1) of Regulation (EC) No 1924/2006. EFSA J. 2011, 9, 2056. [Google Scholar] [CrossRef]
- Gimenez, R.; Aguilar, J. Effects of cytidine 5’-diphosphocholine on plasma homocysteine levels in rat. Comp. Biochem. Phys. B 2003, 134, 271–276. [Google Scholar] [CrossRef]
- Leoni, S.; Tovoli, F.; Napoli, L.; Serio, I.; Ferri, S.; Bolondi, L. Current guidelines for the management of non-alcoholic fatty liver disease: A systematic review with comparative analysis. World J. Gastroenterol. 2018, 24, 3361–3373. [Google Scholar] [CrossRef] [PubMed]
- Tinelli, C.; Di Pino, A.; Ficulle, E.; Marcelli, S.; Feligioni, M. Hyperhomocysteinemia as a Risk Factor and Potential Nutraceutical Target for Certain Pathologies. Front. Nutr. 2019, 6, 49. [Google Scholar] [CrossRef] [PubMed]
- Dinsdale, J.R.; Griffiths, G.K.; Rowlands, C.; Castello, J.; Ortiz, J.A.; Maddock, J.; Aylward, M. Pharmacokinetics of 14C CDP-choline. Arzneimittelforschung 1983, 33, 1066–1070. [Google Scholar] [PubMed]
- D’Orlando, K.J.; Sandage, B.W., Jr. Citicoline (CDP-choline): Mechanisms of action and effects in ischemic brain injury. Neurol. Res. 1995, 17, 281–284. [Google Scholar] [CrossRef]
- Galletti, P.; Derosa, M.; Cotticelli, M.G.; Morana, A.; Vaccaro, R.; Zappia, V. Biochemical Rationale for the Use of Cdpcholine in Traumatic Brain Injury-Pharmacokinetics of the Orally-Administered Drug. J. Neurol. Sci. 1991, 103, S19–S25. [Google Scholar] [CrossRef]
- Lopez-Coviella, I.; Agut, J.; Savci, V.; Ortiz, J.A.; Wurtman, R.J. Evidence that 5’-cytidinediphosphocholine can affect brain phospholipid composition by increasing choline and cytidine plasma levels. J. Neurochem. 1995, 65, 889–894. [Google Scholar] [CrossRef]
- Wurtman, R.J.; Regan, M.; Ulus, I.; Yu, L. Effect of oral CDP-choline on plasma choline and uridine levels in humans. Biochem. Pharmacol. 2000, 60, 989–992. [Google Scholar] [CrossRef]
- Sarkar, A.K.; Ghosh, D.; Haldar, D.; Sarkar, P.; Gupta, B.; Dastidar, S.G.; Pal, T.K. A rapid LC-ESI-MS/MS method for the quantitation of choline, an active metabolite of citicoline: Application to in vivo pharmacokinetic and bioequivalence study in Indian healthy male volunteers. J. Pharm. Biomed. Anal. 2012, 71, 144–147. [Google Scholar] [CrossRef] [PubMed]
- Grieb, P. Neuroprotective properties of citicoline: facts, doubts and unresolved issues. CNS Drugs 2014, 28, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Neuman, M.W.; Hodge, H.C. Acute Toxicity of Choline Chloride Administered Orally to Rats. Proc. Soc. Exp. Biol. Med. 1945, 58, 87–88. [Google Scholar] [CrossRef]
- Kanabayashi, T.; Shiota, K.; Mizuno, M.; Isaka, H.; Hoshino, K. Toxicological studies on citicoline. acute and subacute toxicity study in mice and rats. Oyo Yakuri Pharmacomet. 1980, 20, 109–126. [Google Scholar]
- Sahu, A.P.; Saxena, A.K.; Singh, K.P.; Shanker, R. Effect of chronic choline administration in rats. Indian J. Exp. Biol. 1986, 24, 91–96. [Google Scholar]
- Agut, J.; Font, E.; Sacristan, A.; Ortiz, J.A. Dissimilar effects in acute toxicity studies of CDP-choline and choline. Arzneimittelforschung 1983, 33, 1016–1018. [Google Scholar]
- Hodge, H.C.; Goldstein, M.R. The Acute Toxicity of Choline Hydrochloride in Mice and Rats. Proc. Soc. Exp. Biol. Med. 1942, 51, 281–282. [Google Scholar] [CrossRef]
- Paroni, R.; Cighetti, G.; Del Puppo, M.; Kienle, M.G. Evidence for a different metabolic behaviour of cytidine diphosphate choline after oral and intravenous administration to rats. Pharmacol. Res. Commun. 1985, 17, 805–829. [Google Scholar] [CrossRef]
- Ufnal, M.; Zadlo, A.; Ostaszewski, R. TMAO: A small molecule of great expectations. Nutrition 2015, 31, 1317–1323. [Google Scholar] [CrossRef]
- Tang, W.H.; Wang, Z.; Levison, B.S.; Koeth, R.A.; Britt, E.B.; Fu, X.; Wu, Y.; Hazen, S.L. Intestinal microbial metabolism of phosphatidylcholine and cardiovascular risk. N. Engl. J. Med. 2013, 368, 1575–1584. [Google Scholar] [CrossRef] [PubMed]
- Qi, J.; You, T.; Li, J.; Pan, T.; Xiang, L.; Han, Y.; Zhu, L. Circulating trimethylamine N-oxide and the risk of cardiovascular diseases: A systematic review and meta-analysis of 11 prospective cohort studies. J. Cell. Mol. Med. 2018, 22, 185–194. [Google Scholar] [CrossRef] [PubMed]
- Rexidamu, M.; Li, H.; Jin, H.; Huang, J. Serum levels of Trimethylamine-N-oxide in patients with ischemic stroke. Biosci. Rep. 2019. [Google Scholar] [CrossRef] [PubMed]
- Liang, Z.G.; Dong, Z.X.; Guo, M.H.; Shen, Z.Q.; Yin, D.C.; Hu, S.; Hai, X. Trimethylamine N-oxide as a risk marker for ischemic stroke in patients with atrial fibrillation. J. Biochem. Mol. Toxicol. 2019, 33. [Google Scholar] [CrossRef]
- Vogt, N.M.; Romano, K.A.; Darst, B.F.; Engelman, C.D.; Johnson, S.C.; Carlsson, C.M.; Asthana, S.; Blennow, K.; Zetterberg, H.; Bendlin, B.B.; et al. The gut microbiota-derived metabolite trimethylamine N-oxide is elevated in Alzheimer’s disease. Alzheimer’s Res. Ther. 2018, 10, 124. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.E.; Rouchotas, P.; Fritz, H. Lecithin (Phosphatidylcholine): Healthy Dietary Supplement or Dangerous Toxin? Nat. Prod. J. 2016, 6, 242–249. [Google Scholar] [CrossRef]
- DiNicolantonio, J.J.; McCarty, M.; OKeefe, J. Association of moderately elevated trimethylamine N-oxide with cardiovascular risk: Is TMAO serving as a marker for hepatic insulin resistance. Open Heart 2019, 6, e000890. [Google Scholar] [CrossRef] [PubMed]
- Nam, H.S. Gut Microbiota and Ischemic Stroke: The Role of Trimethylamine N-Oxide. J. Stroke 2019, 21, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Poly, C.; Massaro, J.M.; Seshadri, S.; Wolf, P.A.; Cho, E.Y.; Krall, E.; Jacques, P.F.; Au, R. The relation of dietary choline to cognitive performance and white-matter hyperintensity in the Framingham Offspring Cohort. Am. J. Clin. Nutr. 2011, 94, 1584–1591. [Google Scholar] [CrossRef] [Green Version]
- Nurk, E.; Refsum, H.; Bjelland, I.; Drevon, C.A.; Tell, G.S.; Ueland, P.M.; Vollset, S.E.; Engedal, K.; Nygaard, H.A.; Smith, D.A. Plasma free choline, betaine and cognitive performance: The Hordaland Health Study. Br. J. Nutr. 2013, 109, 511–519. [Google Scholar] [CrossRef]
- Blusztajn, J.K.; Slack, B.E.; Mellott, T.J. Neuroprotective Actions of Dietary Choline. Nutrients 2017, 9, 815. [Google Scholar] [CrossRef] [PubMed]
- Lippelt, D.P.; van der Kint, S.; van Herk, K.; Naber, M. No Acute Effects of Choline Bitartrate Food Supplements on Memory in Healthy, Young, Human Adults. PLoS ONE 2016, 11. [Google Scholar] [CrossRef] [PubMed]
- McGlade, E.; Agoston, A.M.; DiMuzio, J.; Kizaki, M.; Nakazaki, E.; Kamiya, T.; Yurgelun-Todd, D. The Effect of Citicoline Supplementation on Motor Speed and Attention in Adolescent Males. J. Atten. Disord. 2019, 23, 121–134. [Google Scholar] [CrossRef] [PubMed]
- Gareri, P.; Castagna, A.; Cotroneo, A.M.; Putignano, S.; De Sarro, G.; Bruni, A.C. The role of citicoline in cognitive impairment: Pharmacological characteristics, possible advantages, and doubts for an old drug with new perspectives. Clin. Interv. Aging 2015, 10, 1421–1429. [Google Scholar] [CrossRef] [PubMed]
- Fioravanti, M.; Yanagi, M. Cytidinediphosphocholine (CDP-choline) for cognitive and behavioural disturbances associated with chronic cerebral disorders in the elderly. Cochrane Database Syst. Rev. 2005. [Google Scholar] [CrossRef] [PubMed]
- Castagna, A.; Cotroneo, A.M.; Ruotolo, G.; Gareri, P. The CITIRIVAD Study: CITIcoline plus RIVAstigmine in Elderly Patients Affected with Dementia Study. Clin. Drug Investig. 2016, 36, 1059–1065. [Google Scholar] [CrossRef] [PubMed]
- Gareri, P.; Castagna, A.; Cotroneo, A.M.; Putignano, D.; Conforti, R.; Santamaria, F.; Marino, S.; Putignano, S. The Citicholinage Study: Citicoline Plus Cholinesterase Inhibitors in Aged Patients Affected with Alzheimer’s Disease Study. J. Alzheimer’s Dis. 2017, 56, 557–565. [Google Scholar] [CrossRef]
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Synoradzki, K.; Grieb, P. Citicoline: A Superior Form of Choline? Nutrients 2019, 11, 1569. https://doi.org/10.3390/nu11071569
Synoradzki K, Grieb P. Citicoline: A Superior Form of Choline? Nutrients. 2019; 11(7):1569. https://doi.org/10.3390/nu11071569
Chicago/Turabian StyleSynoradzki, Kamil, and Paweł Grieb. 2019. "Citicoline: A Superior Form of Choline?" Nutrients 11, no. 7: 1569. https://doi.org/10.3390/nu11071569
APA StyleSynoradzki, K., & Grieb, P. (2019). Citicoline: A Superior Form of Choline? Nutrients, 11(7), 1569. https://doi.org/10.3390/nu11071569