The Willingness to Modify Portion Sizes or Eat New Protein Foods Largely Depends on the Dietary Pattern of Protein Intake


 , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Population and Questionnaire
2.2. Food Intake Data
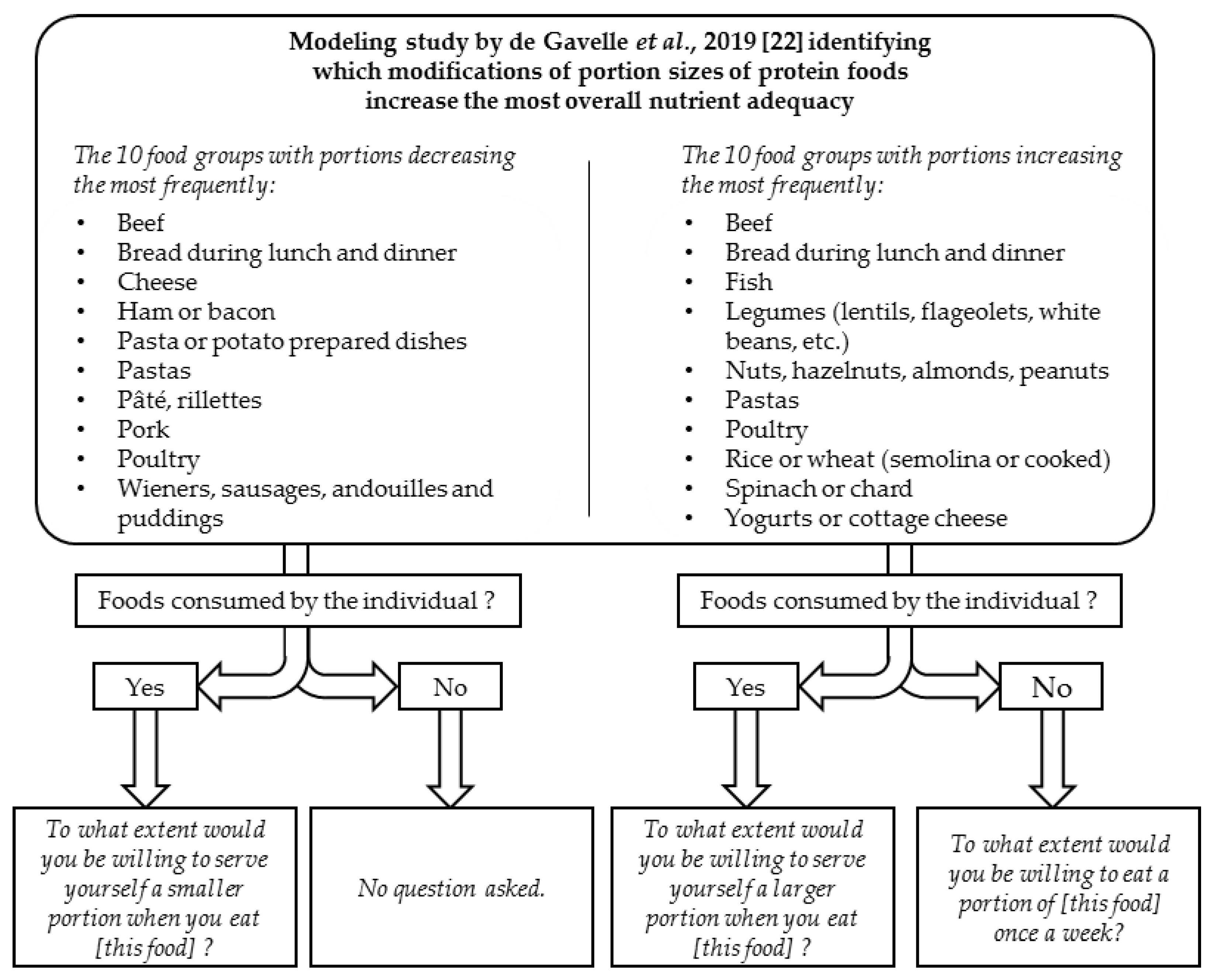
2.3. Willingness to Modify Food Behavior
2.4. Identification of Misreports
2.5. Statistical Analyses
3. Results
3.1. Dietary Pattern of Protein Intake Clusters
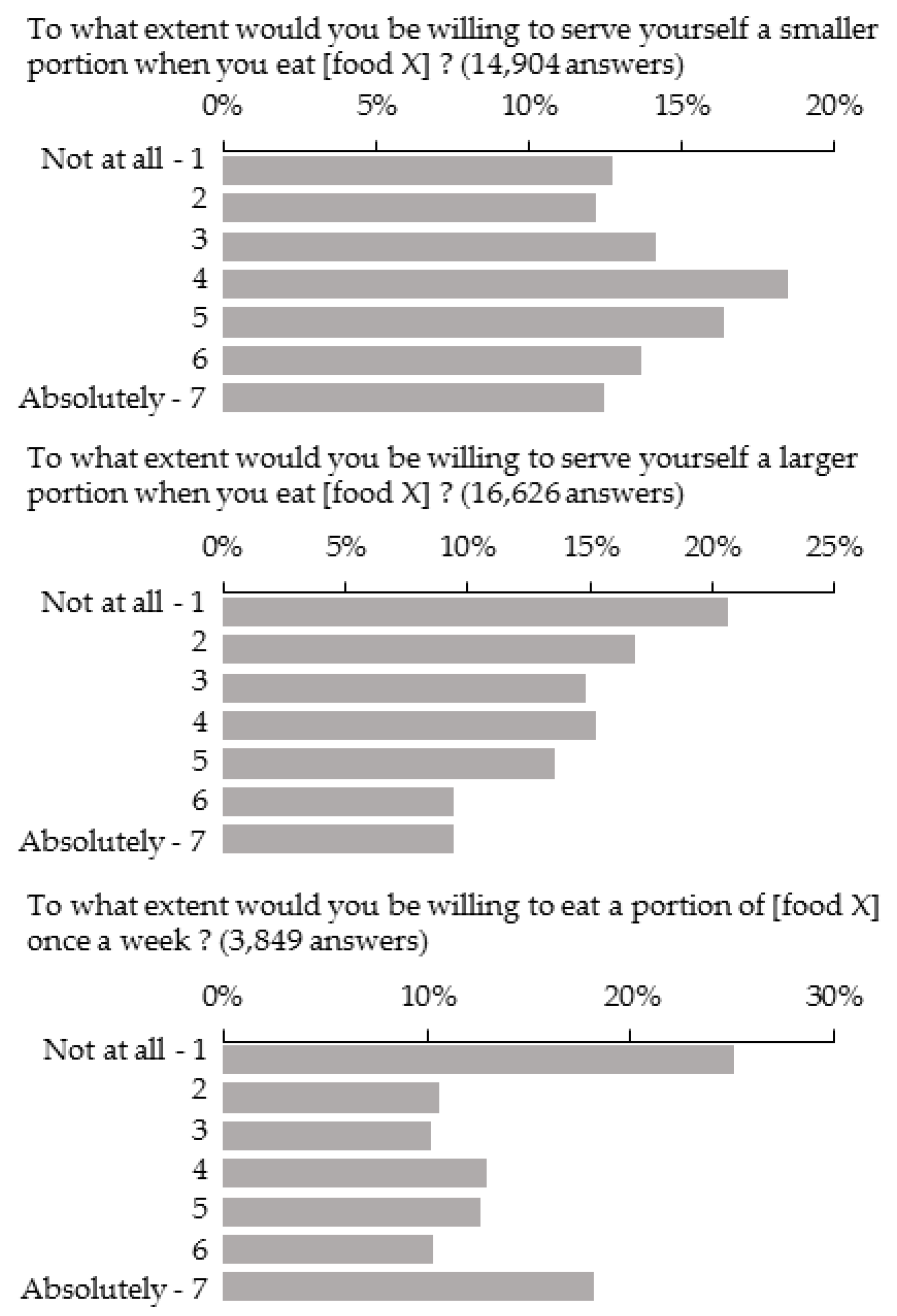
3.2. Distribution of Scores of Willingness to Modify Portion Sizes
3.3. Food Groups
3.4. Individual Patterns of Protein Intake
3.5. Sociodemographic and Other Characteristics
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- FAO. Faostat. Available online: http://www.Fao.Org/faostat/en/#data/cl (accessed on 12 December 2018).
- FranceAgriMer. Impact de la crise économique sur la consommation de viande et évolution des comportements alimentaires. Les Synthèses De Fr. 2015, 21. [Google Scholar]
- Godfray, H.C.J.; Aveyard, P.; Garnett, T.; Hall, J.W.; Key, T.J.; Lorimer, J.; Pierrehumbert, R.T.; Scarborough, P.; Springmann, M.; Jebb, S.A. Meat consumption, health, and the environment. Science 2018, 361, eaam5324. [Google Scholar] [CrossRef] [PubMed]
- Anses. Updating of the PNNS Guidelines: Revision of the Food-Based Dietary Guidelines. Anses Opin. Collect. Expert Rep. 2016. Available online: https://www.anses.fr/en/system/files/nut2012sa0103ra-1en.pdf (accessed on 12 December 2018).
- U.S. Department of Health and Human Services and U.S. Department of Agriculture. 2015–2020 Dietary Guidelines for Americans; U.S. Department of Health and Human Services and U.S. Department of Agriculture: Washington, DC, USA, 2015. Available online: http://health.Gov/dietaryguidelines/2015/guidelines/ (accessed on 1 March 2018).
- Brown, K.A.; Timotijevic, L.; Barnett, J.; Shepherd, R.; Lähteenmäki, L.; Raats, M.M. A review of consumer awareness, understanding and use of food-based dietary guidelines. Br. J. Nutr. 2011, 106, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Clonan, A.; Wilson, P.; Swift, J.A.; Leibovici, D.G.; Holdsworth, M. Red and processed meat consumption and purchasing behaviours and attitudes: Impacts for human health, animal welfare and environmental sustainability. Public Health Nutr. 2015, 18, 2446–2456. [Google Scholar] [CrossRef] [PubMed]
- De Backer, C.J.S.; Hudders, L. Meat morals: Relationship between meat consumption consumer attitudes towards human and animal welfare and moral behavior. Meat Sci. 2015, 99, 68–74. [Google Scholar] [CrossRef]
- Amiot, C.E.; El Hajj Boutros, G.; Sukhanova, K.; Karelis, A.D. Testing a novel multicomponent intervention to reduce meat consumption in young men. PLoS ONE 2018, 13, e0204590. [Google Scholar] [CrossRef]
- De Boer, J.; Aiking, H. Pursuing a low meat diet to improve both health and sustainability: How can we use the frames that shape our meals? Ecol. Econ. 2017, 142, 238–248. [Google Scholar] [CrossRef]
- Bianchi, F.; Garnett, E.; Dorsel, C.; Aveyard, P.; Jebb, S.A. Restructuring physical micro-environments to reduce the demand for meat: A systematic review and qualitative comparative analysis. Lancet Planet. Health 2018, 2, e384–e397. [Google Scholar] [CrossRef]
- De Boer, J.; Schösler, H.; Aiking, H. “Meatless days” or “less but better”? Exploring strategies to adapt western meat consumption to health and sustainability challenges. Appetite 2014, 76, 120–128. [Google Scholar] [CrossRef]
- Vandenbroele, J.; Slabbinck, H.; Van Kerckhove, A.; Vermeir, I. Curbing portion size effects by adding smaller portions at the point of purchase. Food Qual. Prefer. 2018, 64, 82–87. [Google Scholar] [CrossRef]
- Vanhonacker, F.; Van Loo, E.J.; Gellynck, X.; Verbeke, W. Flemish consumer attitudes towards more sustainable food choices. Appetite 2013, 62, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Schösler, H.; de Boer, J.; Boersema, J.J. Can we cut out the meat of the dish? Constructing consumer-oriented pathways towards meat substitution. Appetite 2012, 58, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Gazan, R.; Brouzes, C.M.C.; Vieux, F.; Maillot, M.; Lluch, A.; Darmon, N. Mathematical optimization to explore tomorrow’s sustainable diets: A narrative review. Adv. Nutr. 2018, 9, 602–616. [Google Scholar] [CrossRef] [PubMed]
- Horgan, G.W.; Perrin, A.; Whybrow, S.; Macdiarmid, J.I. Achieving dietary recommendations and reducing greenhouse gas emissions: Modelling diets to minimise the change from current intakes. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 46. [Google Scholar] [CrossRef]
- Maillot, M.; Vieux, F.; Amiot, M.J.; Darmon, N. Individual diet modeling translates nutrient recommendations into realistic and individual-specific food choices. Am. J. Clin. Nutr. 2009, 91, 421–430. [Google Scholar] [CrossRef] [PubMed]
- Van Dooren, C.; Tyszler, M.; Kramer, G.F.H.; Aiking, H. Combining low price, low climate impact and high nutritional value in one shopping basket through diet optimization by linear programming. Sustainability 2015, 7, 12837. [Google Scholar] [CrossRef]
- Pfeiler, T.M.; Egloff, B. Personality and meat consumption: The importance of differentiating between type of meat. Appetite 2018, 130, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Latvala, T.; Niva, M.; Mäkelä, J.; Pouta, E.; Heikkilä, J.; Kotro, J.; Forsman-Hugg, S. Diversifying meat consumption patterns: Consumers’ self-reported past behaviour and intentions for change. Meat Sci. 2012, 92, 71–77. [Google Scholar] [CrossRef] [PubMed]
- De Gavelle, E.; Huneau, J.-F.; Fouillet, H.; Mariotti, F. The initial dietary pattern should be considered when changing protein food portion sizes to increase nutrient adequacy in French adults. J. Nutr. 2019, 149, 488–496. [Google Scholar] [CrossRef]
- Sindhwani, V.; Bucak, S.; Hu, J.; Mojsilovic, A. A family of Non-Negative Matrix Factorizations for One-Class Collaborative Filtering Problems. In Proceedings of the 3rd ACM Recommender Systems Conference, (RecSys 2009), New York, NY, USA, 23–25 October 2009. [Google Scholar]
- De Vaus, D. Surveys in Social Research, 5th ed.; UCL Press: London, UK, 2002. [Google Scholar]
- Blundell, J.; de Graaf, C.; Hulshof, T.; Jebb, S.; Livingstone, B.; Lluch, A.; Mela, D.; Salah, S.; Schuring, E.; van der Knaap, H.; et al. Appetite control: Methodological aspects of the evaluation of foods. Obes. Rev. 2010, 11, 251–270. [Google Scholar] [CrossRef]
- Le Moullec, N.; Deheeger, M.; Preziosi, P.; Monteiro, P.; Valeix, P.; Rolland-Cachera, M.-F.; Potier de Courcy, G.; Christides, J.-P.; Cherouvrier, F.; Galan, P. Validation du manuel-photos utilisé pour l’enquête alimentaire de l’étude su. Vi. Max. Cah. Nutr. Diététique 1996, 31, 158–164. [Google Scholar]
- Dubuisson, C.; Lioret, S.; Touvier, M.; Dufour, A.; Calamassi-Tran, G.; Volatier, J.-L.; Lafay, L. Trends in food and nutritional intakes of French adults from 1999 to 2007: Results from the inca surveys. Br. J. Nutr. 2010, 103, 1035–1048. [Google Scholar] [CrossRef] [PubMed]
- Anses. Étude Individuelle Nationale des Consommations Alimentaires 3 (inca 3). Rapp. D’expertise Collect. 2017. Available online: https://www.anses.fr/fr/system/files/nut2014sa0234ra.pdf (accessed on 12 December 2018).
- Anses. Actualisation des Repères du PNNS: Étude des Relations Entre Consommation de Groupes D’aliments et Risque de Maladies Chroniques non Transmissibles. Rapp. D’expertise Collect. 2016. Available online: www.anses.fr/en/system/files/nut2012sa0103ra-3.pdf (accessed on 12 December 2018).
- De Gavelle, E.; Huneau, J.-F.; Mariotti, F. Patterns of protein food intake are associated with nutrient adequacy in the general French adult population. Nutrients 2018, 10, 226. [Google Scholar] [CrossRef] [PubMed]
- Brunet, J.-P.; Tamayo, P.; Golub, T.R.; Mesirov, J.P. Metagenes and molecular pattern discovery using matrix factorization. Proc. Natl. Acad. Sci. USA 2004, 101, 4164–4169. [Google Scholar] [CrossRef] [PubMed]
- Gazan, R.; Béchaux, C.; Crépet, A.; Sirot, V.; Drouillet-Pinard, P.; Dubuisson, C.; Havard, S. Dietary patterns in the French adult population: A study from the second French national cross-sectional dietary survey (inca2) (2006–2007). Br. J. Nutr. 2016, 116, 300–315. [Google Scholar] [CrossRef] [PubMed]
- Sy, M.M.; Feinberg, M.; Verger, P.; Barré, T.; Clémençon, S.; Crépet, A. New approach for the assessment of cluster diets. Food Chem. Toxicol. 2013, 52, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Sarle, W. SAS Technical Report a-108, Cubic Clustering Criterion; SAS Institute Inc.: Cary, NC, USA, 1983; p. 56. [Google Scholar]
- Harabasz, C.T.; Karoński, M. A dendrite method for cluster analysis. Commun. Stat. 1974, 3, 1–27. [Google Scholar]
- Spence, M.; Stancu, V.; Dean, M.; Livingstone, M.B.E.; Gibney, E.R.; Lähteenmäki, L. Are food-related perceptions associated with meal portion size decisions? A cross-sectional study. Appetite 2016, 103, 377–385. [Google Scholar] [CrossRef]
- Graça, J.; Calheiros, M.M.; Oliveira, A. Attached to meat? (un)willingness and intentions to adopt a more plant-based diet. Appetite 2015, 95, 113–125. [Google Scholar] [CrossRef]
- Schneider, A.V.C. Overview of the market and consumption of puises in europe. Br. J. Nutr. 2002, 88, 243–250. [Google Scholar] [CrossRef]
- Winham, D.M.; Hutchins, A.M. Perceptions of flatulence from bean consumption among adults in 3 feeding studies. Nutr. J. 2011, 10, 128. [Google Scholar] [CrossRef] [PubMed]
- Petti, A.; Palmieri, B.; Vadalà, M.; Laurino, C. Vegetarianism and veganism: Not only benefits but also gaps. A review. Prog. Nutr. 2017, 19, 229–242. [Google Scholar]
- Nolan-Clark, D.J.; Neale, E.P.; Probst, Y.C.; Charlton, K.E.; Tapsell, L.C. Consumers’ salient beliefs regarding dairy products in the functional food era: A qualitative study using concepts from the theory of planned behaviour. BMC Public Health 2011, 11, 843. [Google Scholar] [CrossRef] [PubMed]
- Story, M.; Kaphingst, K.M.; Robinson-O’Brien, R.; Glanz, K. Creating healthy food and eating environments: Policy and environmental approaches. Annu. Rev. Public Health 2008, 29, 253–272. [Google Scholar] [CrossRef] [PubMed]
- Solomon-Krakus, S.; Sabiston, C.M. Body checking is associated with weight- and body-related shame and weight- and body-related guilt among men and women. Body Image 2017, 23, 80–84. [Google Scholar] [CrossRef] [PubMed]
- Beardsworth, A.; Bryman, A.; Keil, T.; Goode, J.; Haslam, C.; Lancashire, E. Women, men and food: The significance of gender for nutritional attitudes and choices. Br. Food J. 2002, 104, 470–491. [Google Scholar] [CrossRef]
- Chang, Y.; Chatterjee, S.; Kim, J. Household finance and food insecurity. J. Fam. Econ. Issues 2014, 35, 499–515. [Google Scholar] [CrossRef]
- Fávaro-Moreira, N.C.; Krausch-Hofmann, S.; Duyck, J.; Matthys, C.; Vanhauwaert, E.; Declercq, A.; Vereecken, C.; Bekkering, G.E. Risk factors for malnutrition in older adults: A systematic review of the literature based on longitudinal data. Adv. Nutr. 2016, 7, 507–522. [Google Scholar] [CrossRef] [PubMed]
- Meiselman, H.L.; King, S.C.; Gillette, M. The demographics of neophobia in a large commercial us sample. Food Qual. Prefer. 2010, 21, 893–897. [Google Scholar] [CrossRef]
- Siegrist, M.; Hartmann, C.; Keller, C. Antecedents of food neophobia and its association with eating behavior and food choices. Food Qual. Prefer. 2013, 30, 293–298. [Google Scholar] [CrossRef]
- Inelmen, E.; Toffanello, E.; Enzi, G.; Sergi, G.; Coin, A.; Busetto, L.; Manzato, E. Differences in dietary patterns between older and younger obese and overweight outpatients. J. Nutr. Health Aging 2008, 12, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Gorber, S.C.; Tremblay, M.; Moher, D.; Gorber, B. A comparison of direct vs. Self-report measures for assessing height, weight and body mass index: A systematic review. Obes. Rev. 2007, 8, 307–326. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Reference | Smaller Portion Size (M1) | Larger Portion Size (M2) | Introduction of a Small Portion of a New Food (M3) | |||
|---|---|---|---|---|---|---|---|
| OR (95%CI) | p | OR (95%CI) | p | OR (95%CI) | p | ||
| Dietary pattern of protein intake cluster | 0.0063 | 0.0041 | NS | ||||
| Pork eaters | Bread and dairy eaters | 0.96 (0.75; 1.22) | 1.15 (0.91; 1.46) | 1.12 (0.83; 1.51) | |||
| Take-away eaters | 1.16 (0.88; 1.54) | 1.52 (1.16; 2.01) | 1.15 (0.81; 1.61) | ||||
| Healthy eaters | 1.64 (1.20; 2.24) | 1.15 (0.86; 1.55) | 0.78 (0.51; 1.18) | ||||
| Poultry eaters | 1.34 (1.04; 1.74) | 1.15 (0.89; 1.48) | 0.81 (0.59; 1.11) | ||||
| Beef eaters | 1.12 (0.88; 1.43) | 0.87 (0.68; 1.11) | 1.07 (0.79; 1.46) | ||||
| Quartile of frequency of intake of the food group considered | <0.0001 | <0.0001 | N/A | ||||
| 1st | 4th | 1.42 (1.22; 1.64) | 0.59 (0.52; 0.68) | N/A | |||
| 2nd | 1.14 (1; 1.29) | 0.78 (0.69; 0.89) | N/A | ||||
| 3rd | 0.99 (0.85; 1.14) | 0.88 (0.78; 0.99) | N/A | ||||
| Quartile of portion size of the food group considered | 0.023 | <0.0001 | N/A | ||||
| 1st | 4th | 0.91 (0.80; 1.04) | 0.59 (0.52; 0.68) | N/A | |||
| 2nd | 0.83 (0.73; 0.94) | 0.90 (0.80; 1.03) | N/A | ||||
| 3rd | 0.94 (0.81; 1.08) | 1.15 (1.00; 1.33) | N/A | ||||
| Consumers of the food group considered in the individual’s cluster (%) 2 | N/A | N/A | <0.0001 | ||||
| N/A | N/A | 1.029 (1.01; 1.04) | |||||
| Appetite score (1–7) 2 | 0.032 | 0.007 | NS | ||||
| 0.94 (0.89; 0.99) | 1.08 (1.02; 1.13) | 1.05 (0.99; 1.13) | |||||
| Food group | <0.0001 | <0.0001 | <0.0001 | ||||
| Beef | Bread 3 | 0.84 (0.70; 1.02) | 0.64 (0.54; 0.74) | 0.56 (0.29; 1.05) | |||
| Spinach/Chard | N/A | 1.47 (1.19; 1.82) | 2.02 (0.93; 4.37) | ||||
| Cheese | 0.73 (0.60; 0.89) | N/A | N/A | ||||
| Ham | 0.91 (0.75; 1.11) | N/A | N/A | ||||
| Legumes | N/A | 0.69 (0.58; 0.82) | 1.52 (0.88; 2.6) | ||||
| Nuts/Seeds | N/A | 1.30 (1.08; 1.56) | 1.68 (0.9; 3.12) | ||||
| Pâté | 2.06 (1.65; 2.57) | N/A | N/A | ||||
| Pasta | 1.68 (1.40; 2.03) | 0.37 (0.32; 0.44) | N/A | ||||
| Pasta/Potato dishes | 1.19 (0.95; 1.48) | N/A | N/A | ||||
| Fish | N/A | 1.17 (0.99; 1.37) | 2.09 (1.18; 3.7) | ||||
| Pork | 1.25 (1.02; 1.52) | N/A | N/A | ||||
| Rice/Wheat | N/A | 0.48 (0.41; 0.57) | 1.33 (0.78; 2.27) | ||||
| Sausage | 1.19 (0.96; 1.46) | N/A | N/A | ||||
| Poultry | 0.65 (0.54; 0.79) | 0.77 (0.66; 0.91) | 0.66 (0.37; 1.17) | ||||
| Yogurts | N/A | 0.91 (0.77; 1.08) | 0.29 (0.16; 0.52) | ||||
| Sex | 0.0001 | 0.014 | NS | ||||
| Male | Women | 0.73 (0.62; 0.86) | 1.22 (1.04; 1.44) | 0.84 (0.68; 1.03) | |||
| Age (years) | NS | <0.0001 | 0.024 | ||||
| 18–24 | 55–65 | 1.28 (0.95; 1.71) | 1.68 (1.26; 2.23) | 0.65 (0.45; 0.92) | |||
| 25–34 | 1.21 (0.95; 1.55) | 1.79 (1.40; 2.28) | 0.82 (0.60; 1.12) | ||||
| 35–44 | 1.33 (1.05; 1.70) | 1.76 (1.39; 2.23) | 1.06 (0.79; 1.44) | ||||
| 45–54 | 1.08 (0.85; 1.35) | 1.55 (1.24; 1.95) | 1.08 (0.81; 1.44) | ||||
| BMI (kg/m²) | 0.0005 | 0.013 | NS | ||||
| ≤18.5 | 18.5–25 | 0.76 (0.52; 1.12) | 0.68 (0.46; 0.99) | 0.67 (0.43; 1.05) | |||
| 25–30 | 1.40 (1.16; 1.68) | 1.08 (0.90; 1.29) | 0.81 (0.61; 1.08) | ||||
| >30 | 1.26 (0.99; 1.60) | 0.76 (0.6; 0.97) | 1.08 (0.86; 1.36) | ||||
| Income (€/month) | 0.037 | 0.048 | NS | ||||
| ≤1500 | >3400 | 0.83 (0.65; 1.06) | 1.30 (1.02; 1.64) | 0.95 (0.71; 1.28) | |||
| 1500–2500 | 0.75 (0.61; 0.93) | 0.98 (0.80; 1.21) | 0.93 (0.71; 1.23) | ||||
| 2500–3400 | 0.96 (0.77; 1.20) | 0.96 (0.77; 1.19) | 1.19 (0.90; 1.59) | ||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Gavelle, E.; Davidenko, O.; Fouillet, H.; Delarue, J.; Darcel, N.; Huneau, J.-F.; Mariotti, F. The Willingness to Modify Portion Sizes or Eat New Protein Foods Largely Depends on the Dietary Pattern of Protein Intake. Nutrients 2019, 11, 1556. https://doi.org/10.3390/nu11071556
de Gavelle E, Davidenko O, Fouillet H, Delarue J, Darcel N, Huneau J-F, Mariotti F. The Willingness to Modify Portion Sizes or Eat New Protein Foods Largely Depends on the Dietary Pattern of Protein Intake. Nutrients. 2019; 11(7):1556. https://doi.org/10.3390/nu11071556
Chicago/Turabian Stylede Gavelle, Erwan, Olga Davidenko, Hélène Fouillet, Julien Delarue, Nicolas Darcel, Jean-François Huneau, and François Mariotti. 2019. "The Willingness to Modify Portion Sizes or Eat New Protein Foods Largely Depends on the Dietary Pattern of Protein Intake" Nutrients 11, no. 7: 1556. https://doi.org/10.3390/nu11071556
APA Stylede Gavelle, E., Davidenko, O., Fouillet, H., Delarue, J., Darcel, N., Huneau, J.-F., & Mariotti, F. (2019). The Willingness to Modify Portion Sizes or Eat New Protein Foods Largely Depends on the Dietary Pattern of Protein Intake. Nutrients, 11(7), 1556. https://doi.org/10.3390/nu11071556