Comparison of the Clinical Implications among Five Different Nutritional Indices in Patients with Lupus Nephritis

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Inclusion
2.2. Clinical and Laboratory Data Collection
2.3. Nutritional Indices Selection and Calculation
2.4. Statistical Analysis
3. Results
3.1. Clinical Characteristics of Patients
3.2. Correlation between Variables and Nutritional Indices
3.3. Comparison of Different Nutritional Indices According to Lupus Nephritis Subclasses
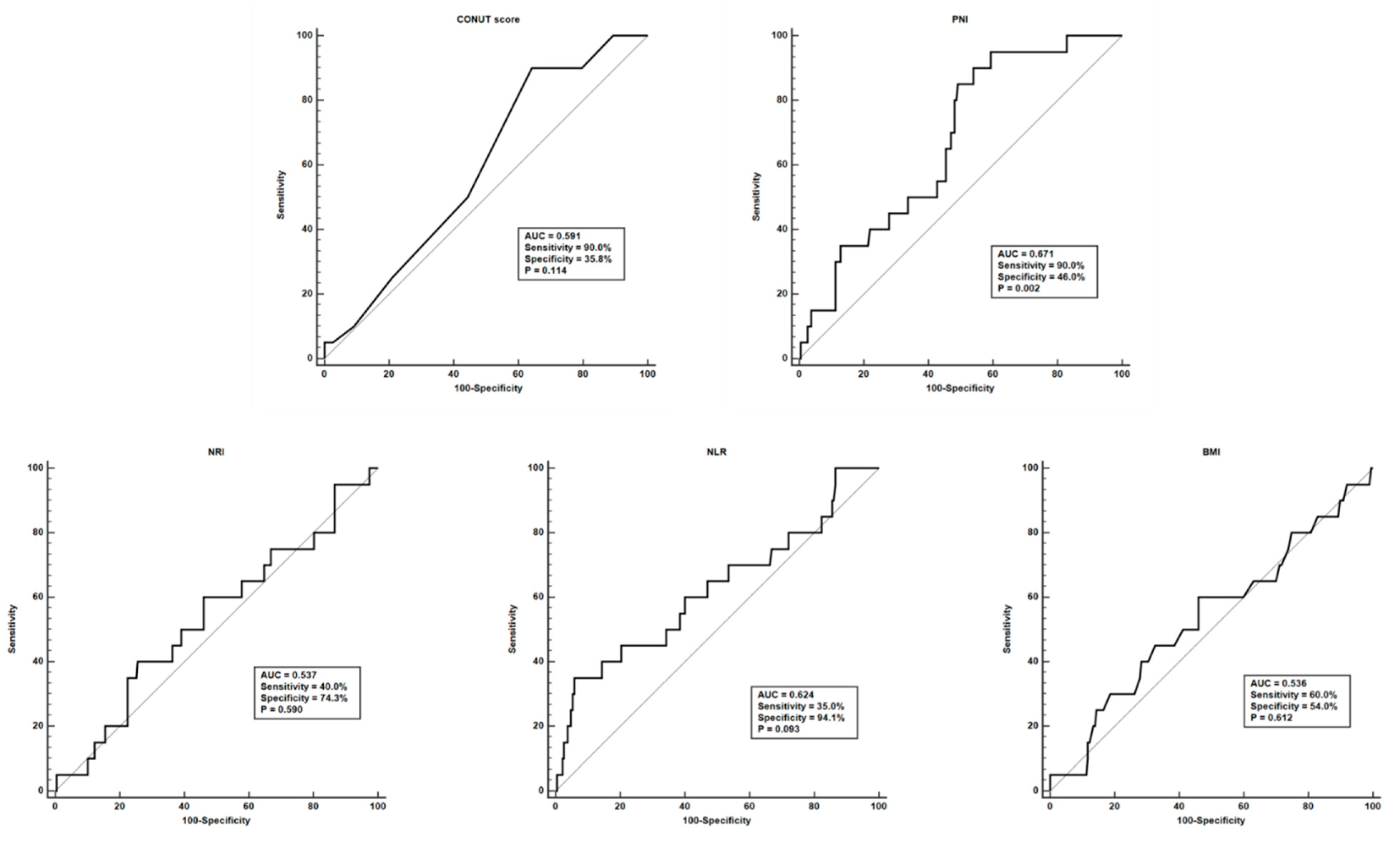
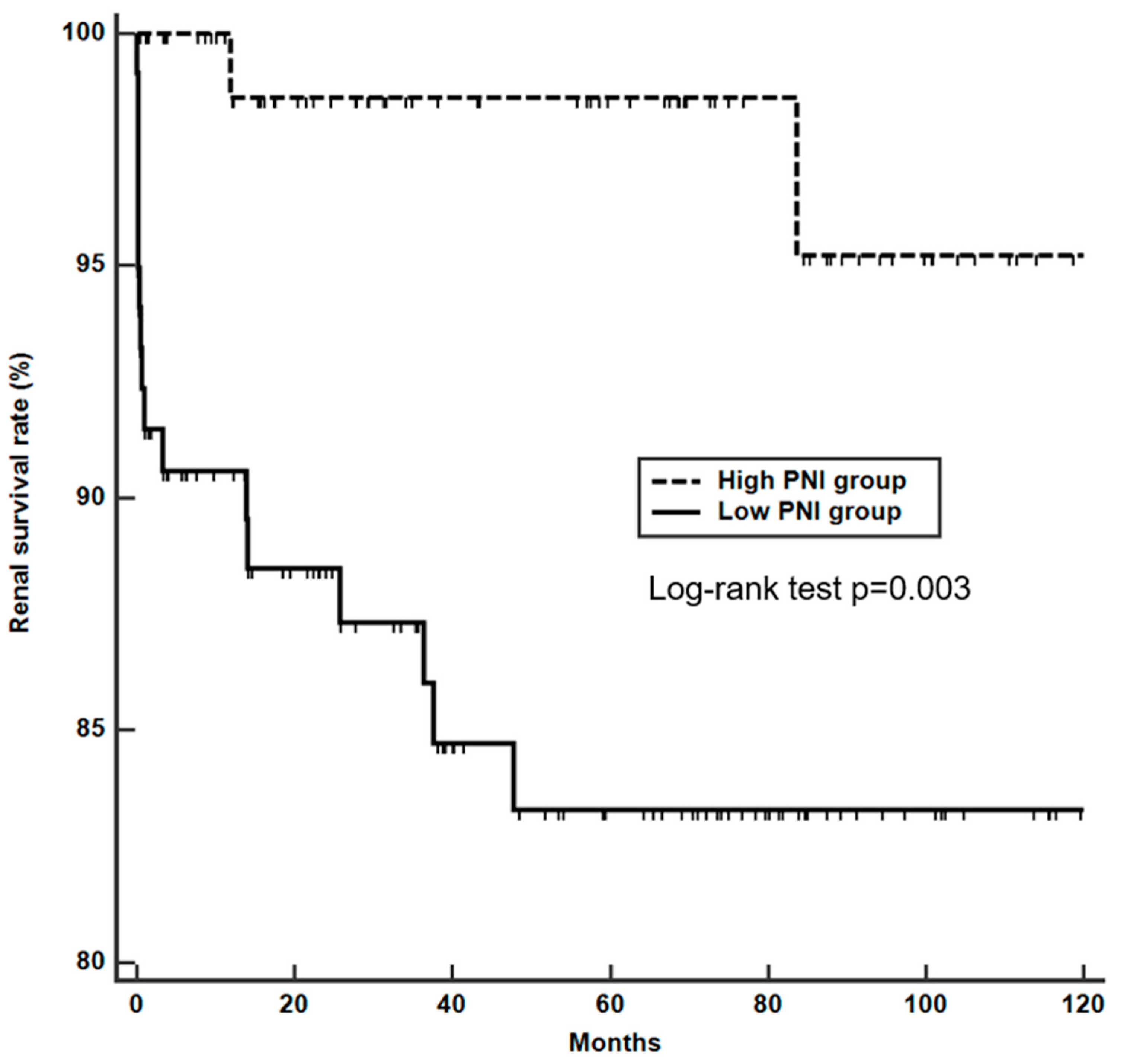
3.4. Factors Associated with End-stage Renal Failure in Patients with Lupus Nephritis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Rekvig, O.P.; Van der Vlag, J. The pathogenesis and diagnosis of systemic lupus erythematosus: Still not resolved. Semin. Immunopathol. 2014, 36, 301–311. [Google Scholar] [CrossRef] [PubMed]
- Saxena, R.; Mahajan, T.; Mohan, C. Lupus nephritis: Current update. Arthritis Res. Ther. 2011, 13, 240. [Google Scholar] [CrossRef] [PubMed]
- Maroz, N.; Segal, M.S. Lupus nephritis and end-stage kidney disease. Am. J. Med. Sci. 2013, 346, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Almaani, S.; Meara, A.; Rovin, B.H. Update on Lupus Nephritis. CJASN 2017, 12, 825–835. [Google Scholar] [CrossRef] [PubMed]
- Vandewoude, M.F.; Alish, C.J.; Sauer, A.C.; Hegazi, R.A. Malnutrition-sarcopenia syndrome: Is this the future of nutrition screening and assessment for older adults? J. Aging Res. 2012, 2012, 651570. [Google Scholar] [CrossRef] [PubMed]
- Bourke, C.D.; Berkley, J.A.; Prendergast, A.J. Immune Dysfunction as a Cause and Consequence of Malnutrition. Trends Immunol. 2016, 37, 386–398. [Google Scholar] [CrossRef] [PubMed]
- Pressoir, M.; Desne, S.; Berchery, D.; Rossignol, G.; Poiree, B.; Meslier, M.; Traversier, S.; Vittot, M.; Simon, M.; Gekiere, J.P.; et al. Prevalence, risk factors and clinical implications of malnutrition in French Comprehensive Cancer Centres. Br. J. Cancer 2010, 102, 966–971. [Google Scholar] [CrossRef]
- Fukuda, W.; Yamazaki, T.; Akaogi, T.; Hayashi, H.; Kusakabe, T.; Tsubouchi, Y.; Kawahito, Y.; Inoue, M.; Yoshikawa, T. Malnutrition and disease progression in patients with rheumatoid arthritis. Mod. Rheumatol. 2005, 15, 104–107. [Google Scholar] [CrossRef]
- Harrison, E.; Herrick, A.L.; McLaughlin, J.T.; Lal, S. Malnutrition in systemic sclerosis. Rheumatology 2012, 51, 1747–1756. [Google Scholar] [CrossRef]
- Cook, Z.; Kirk, S.; Lawrenson, S.; Sandford, S. Use of BMI in the assessment of undernutrition in older subjects: Reflecting on practice. Proc. Nutr. Soc. 2005, 64, 313–317. [Google Scholar] [CrossRef]
- Bharadwaj, S.; Ginoya, S.; Tandon, P.; Gohel, T.D.; Guirguis, J.; Vallabh, H.; Jevenn, A.; Hanouneh, I. Malnutrition: Laboratory markers vs nutritional assessment. Gastroenterol. Rep. 2016, 4, 272–280. [Google Scholar] [CrossRef] [PubMed]
- Narumi, T.; Arimoto, T.; Funayama, A.; Kadowaki, S.; Otaki, Y.; Nishiyama, S.; Takahashi, H.; Shishido, T.; Miyashita, T.; Miyamoto, T.; et al. Prognostic importance of objective nutritional indexes in patients with chronic heart failure. J. Cardiol. 2013, 62, 307–313. [Google Scholar] [CrossRef] [PubMed]
- Adejumo, O.L.; Koelling, T.M.; Hummel, S.L. Nutritional Risk Index predicts mortality in hospitalized advanced heart failure patients. J. Heart Lung Transplant. 2015, 34, 1385–1389. [Google Scholar] [CrossRef] [PubMed]
- Kaya, T.; Acikgoz, S.B.; Yildirim, M.; Nalbant, A.; Altas, A.E.; Cinemre, H. Association between neutrophil-to-lymphocyte ratio and nutritional status in geriatric patients. J. Clin. Lab. Anal. 2019, 33, e22636. [Google Scholar] [CrossRef] [PubMed]
- Hochberg, M.C. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1997, 40, 1725. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.K.; Choe, J.Y.; Lee, S.S. Self-Reported Physical Activity Is Associated with Lupus Nephritis in Systemic Lupus Erythematosus: Data from KORean Lupus Network (KORNET) Registry. Yonsei Med. J. 2018, 59, 857–864. [Google Scholar] [CrossRef] [PubMed]
- Weening, J.J.; D’Agati, V.D.; Schwartz, M.M.; Seshan, S.V.; Alpers, C.E.; Appel, G.B.; Balow, J.E.; Bruijn, J.A.; Cook, T.; Ferrario, F.; et al. The classification of glomerulonephritis in systemic lupus erythematosus revisited. JASN 2004, 15, 241–250. [Google Scholar] [CrossRef] [PubMed]
- Weening, J.J.; D’Agati, V.D.; Schwartz, M.M.; Seshan, S.V.; Alpers, C.E.; Appel, G.B.; Balow, J.E.; Bruijn, J.A.; Cook, T.; Ferrario, F.; et al. The classification of glomerulonephritis in systemic lupus erythematosus revisited. Kidney Int. 2004, 65, 521–530. [Google Scholar] [CrossRef] [PubMed]
- Gladman, D.D.; Ibanez, D.; Urowitz, M.B. Systemic lupus erythematosus disease activity index 2000. J. Rheumatol. 2002, 29, 288–291. [Google Scholar] [PubMed]
- Soares, A.A.; Eyff, T.F.; Campani, R.B.; Ritter, L.; Camargo, J.L.; Silveiro, S.P. Glomerular filtration rate measurement and prediction equations. Clin. Chem. Lab. Med. 2009, 47, 1023–1032. [Google Scholar] [CrossRef] [PubMed]
- Ignacio de Ulibarri, J.; Gonzalez-Madrono, A.; de Villar, N.G.; Gonzalez, P.; Gonzalez, B.; Mancha, A.; Rodriguez, F.; Fernandez, G. CONUT: A tool for controlling nutritional status. First validation in a hospital population. Nutr. Hosp. 2005, 20, 38–45. [Google Scholar] [PubMed]
- Onodera, T.; Goseki, N.; Kosaki, G. Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients. Nihon Geka Gakkai Zasshi 1984, 85, 1001–1005. [Google Scholar] [PubMed]
- Walsh, S.R.; Cook, E.J.; Goulder, F.; Justin, T.A.; Keeling, N.J. Neutrophil-lymphocyte ratio as a prognostic factor in colorectal cancer. J. Surg. Oncol. 2005, 91, 181–184. [Google Scholar] [CrossRef] [PubMed]
- Pan, W.H.; Yeh, W.T. How to define obesity? Evidence-based multiple action points for public awareness, screening, and treatment: An extension of Asian-Pacific recommendations. Asia Pac. J. Clin. Nutr. 2008, 17, 370–374. [Google Scholar] [PubMed]
- Ureshino, H.; Kusaba, K.; Kidoguchi, K.; Sano, H.; Nishioka, A.; Itamura, H.; Yoshimura, M.; Yokoo, M.; Shindo, T.; Kubota, Y.; et al. Clinical impact of the CONUT score and mogamulizumab in adult T cell leukemia/lymphoma. Ann. Hematol. 2019, 98, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Miyashita, E.; Konuma, T.; Kataoka, J.; Oiwa-Monna, M.; Mizusawa, M.; Isobe, M.; Kato, S.; Sato, T.; Takahashi, S.; Tojo, A. The Prognostic Impact of Pretransplantation Inflammatory and Nutritional Status in Adult Patients after Myeloablative Single Cord Blood Transplantation. Biol. Blood Marrow Transplant. 2019, 25, 981–988. [Google Scholar] [CrossRef] [PubMed]
- Agra Bermejo, R.M.; Gonzalez Ferreiro, R.; Varela Roman, A.; Gomez Otero, I.; Kreidieh, O.; Conde Sabaris, P.; Rodriguez-Manero, M.; Moure Gonzalez, M.; Seoane Blanco, A.; Virgos Lamela, A.; et al. Nutritional status is related to heart failure severity and hospital readmissions in acute heart failure. Int. J. Cardiol. 2017, 230, 108–114. [Google Scholar] [CrossRef]
- Takaoka, A.; Sasaki, M.; Nakanishi, N.; Kurihara, M.; Ohi, A.; Bamba, S.; Andoh, A. Nutritional Screening and Clinical Outcome in Hospitalized Patients with Crohn’s Disease. Ann. Nutr. Metab. 2017, 71, 266–272. [Google Scholar] [CrossRef]
- Jain, S.; Gautam, V.; Naseem, S. Acute-phase proteins: As diagnostic tool. J. Pharm. Bioallied Sci. 2011, 3, 118–127. [Google Scholar] [CrossRef]
- Petri, M.; Orbai, A.M.; Alarcon, G.S.; Gordon, C.; Merrill, J.T.; Fortin, P.R.; Bruce, I.N.; Isenberg, D.; Wallace, D.J.; Nived, O.; et al. Derivation and validation of the Systemic Lupus International Collaborating Clinics classification criteria for systemic lupus erythematosus. Arthritis Rheum. 2012, 64, 2677–2686. [Google Scholar] [CrossRef]
- Yu, H.H.; Wang, L.C.; Lee, J.H.; Lee, C.C.; Yang, Y.H.; Chiang, B.L. Lymphopenia is associated with neuropsychiatric manifestations and disease activity in paediatric systemic lupus erythematosus patients. Rheumatology 2007, 46, 1492–1494. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.S.; Jung, S.M.; Song, J.J.; Park, Y.B.; Lee, S.W. Prognostic nutritional index is correlated with disease activity in patients with systemic lupus erythematosus. Lupus 2018, 27, 1697–1705. [Google Scholar] [CrossRef] [PubMed]
- Correa-Rodriguez, M.; Pocovi-Gerardino, G.; Callejas-Rubio, J.L.; Fernandez, R.R.; Martin-Amada, M.; Cruz-Caparros, M.G.; Ortego-Centeno, N.; Rueda-Medina, B. The Prognostic Nutritional Index and Nutritional Risk Index Are Associated with Disease Activity in Patients with Systemic Lupus Erythematosus. Nutrients 2019, 11. [Google Scholar] [CrossRef] [PubMed]
- Mok, C.C. Prognostic factors in lupus nephritis. Lupus 2005, 14, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Contreras, G.; Pardo, V.; Cely, C.; Borja, E.; Hurtado, A.; De La Cuesta, C.; Iqbal, K.; Lenz, O.; Asif, A.; Nahar, N.; et al. Factors associated with poor outcomes in patients with lupus nephritis. Lupus 2005, 14, 890–895. [Google Scholar] [CrossRef]
- Singh, S.; Zhou, X.J.; Ahn, C.; Saxena, R. A retrospective analysis of clinical presentation of lupus nephritis. Am. J. Med. Sci. 2011, 342, 467–473. [Google Scholar] [CrossRef]
- Ines, L.; Duarte, C.; Silva, R.S.; Teixeira, A.S.; Fonseca, F.P.; da Silva, J.A. Identification of clinical predictors of flare in systemic lupus erythematosus patients: A 24-month prospective cohort study. Rheumatology 2014, 53, 85–89. [Google Scholar] [CrossRef]
- Reich, H.N.; Gladman, D.D.; Urowitz, M.B.; Bargman, J.M.; Hladunewich, M.A.; Lou, W.; Fan, S.C.; Su, J.; Herzenberg, A.M.; Cattran, D.C.; et al. Persistent proteinuria and dyslipidemia increase the risk of progressive chronic kidney disease in lupus erythematosus. Kidney Int. 2011, 79, 914–920. [Google Scholar] [CrossRef]
- Domingues, V.; Levinson, B.A.; Bornkamp, N.; Goldberg, J.D.; Buyon, J.; Belmont, H.M. Serum albumin at 1 year predicts long-term renal outcome in lupus nephritis. Lupus Sci. Med. 2018, 5, e000271. [Google Scholar] [CrossRef]
- Liu, G.; Wang, H.; Le, J.; Lan, L.; Xu, Y.; Yang, Y.; Chen, J.; Han, F. Early-stage predictors for treatment responses in patients with active lupus nephritis. Lupus 2019, 28, 283–289. [Google Scholar] [CrossRef]
- Versini, M.; Jeandel, P.Y.; Rosenthal, E.; Shoenfeld, Y. Obesity in autoimmune diseases: Not a passive bystander. Autoimmun. Rev. 2014, 13, 981–1000. [Google Scholar] [CrossRef] [PubMed]
- Tedeschi, S.K.; Barbhaiya, M.; Malspeis, S.; Lu, B.; Sparks, J.A.; Karlson, E.W.; Willett, W.; Costenbader, K.H. Obesity and the risk of systemic lupus erythematosus among women in the Nurses’ Health Studies. Semin. Arthritis Rheum. 2017, 47, 376–383. [Google Scholar] [CrossRef] [PubMed]
- Crowson, C.S.; Matteson, E.L.; Davis, J.M., 3rd; Gabriel, S.E. Contribution of obesity to the rise in incidence of rheumatoid arthritis. Arthritis Care Res. 2013, 65, 71–77. [Google Scholar] [CrossRef]
- Love, T.J.; Zhu, Y.; Zhang, Y.; Wall-Burns, L.; Ogdie, A.; Gelfand, J.M.; Choi, H.K. Obesity and the risk of psoriatic arthritis: A population-based study. Ann. Rheum. Dis. 2012, 71, 1273–1277. [Google Scholar] [CrossRef] [PubMed]
- Schulman, E.; Bartlett, S.J.; Schieir, O.; Andersen, K.M.; Boire, G.; Pope, J.E.; Hitchon, C.; Jamal, S.; Thorne, J.C.; Tin, D.; et al. Overweight, Obesity, and the Likelihood of Achieving Sustained Remission in Early Rheumatoid Arthritis: Results from a Multicenter Prospective Cohort Study. Arthritis Care Res. 2018, 70, 1185–1191. [Google Scholar] [CrossRef] [PubMed]
- Hojgaard, P.; Glintborg, B.; Kristensen, L.E.; Gudbjornsson, B.; Love, T.J.; Dreyer, L. The influence of obesity on response to tumour necrosis factor-alpha inhibitors in psoriatic arthritis: Results from the DANBIO and ICEBIO registries. Rheumatology 2016, 55, 2191–2199. [Google Scholar] [CrossRef] [PubMed]
- McMahon, M.; Hahn, B.H.; Skaggs, B.J. Systemic lupus erythematosus and cardiovascular disease: Prediction and potential for therapeutic intervention. Expert Rev. Clin. Immunol. 2011, 7, 227–241. [Google Scholar] [CrossRef]
- Toto, R.D.; Greene, T.; Hebert, L.A.; Hiremath, L.; Lea, J.P.; Lewis, J.B.; Pogue, V.; Sika, M.; Wang, X. Relationship between body mass index and proteinuria in hypertensive nephrosclerosis: Results from the African American Study of Kidney Disease and Hypertension (AASK) cohort. Am. J. Kidney Dis. 2010, 56, 896–906. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Total (n = 207) | Patients with ESRF (n = 20) | Patients without ESRF (n = 187) | p-value |
|---|---|---|---|---|
| Demographic data | ||||
| Age, years | 36.0 (27.0–46.0) | 37.5 (32.5–51.0) | 36.0 (26.0–46.0) | 0.210 |
| Female sex, n (%) | 186 (89.9) | 19 (95.0) | 167 (89.3) | 0.700 |
| Follow-up duration, months | 57.1 (17.5–90.8) | 33.3 (9.9–82.9) | 59.2 (19.7–93.6) | 0.214 |
| SLE activity-related measures | ||||
| SLEDAI-2K | 9.0 (7.0–12.0) | 9.0 (5.0–11.0) | 9.0 (7.0–13.0) | 0.079 |
| WBC count (/mm3) | 4560.0 (3337.5–6805.0) | 4390.0 (2795.0–7755.0) | 4560.0 (3372.5–6650.0) | 0.767 |
| Platelet count (×1000/mm3) | 205.0 (138.3–251.8) | 183.5 (68.5–222.0) | 207.0 (145.8–254.0) | 0.036 |
| Complement 3, mg/dL | 45.6 (29.5–69.1) | 42.1 (27.5–59.5) | 45.9 (29.6–70.8) | 0.374 |
| Complement 4, mg/dL | 6.2 (3.2–13.3) | 6.8 (3.8–12.7) | 6.2 (3.1–13.3) | 0.995 |
| Anti-dsDNA (IU/mL) | 174.8 (10.3–379.0) | 25.0 (0.0–245.2) | 196.9 (20.3–379.0) | 0.042 |
| Urinary P/Cr ratio | 2.9 (1.5–6.1) | 4.2 (1.5–6.9) | 2.8 (1.5–5.9) | 0.422 |
| Clinical features, n (%) | ||||
| Skin rash | 55 (26.6) | 4 (20.0) | 51 (27.3) | 0.601 |
| Photosensitivity | 14 (6.8) | 0 (0.0) | 14 (7.5) | 0.370 |
| Oral ulcer | 22 (10.6) | 1 (5.0) | 21 (11.2) | 0.702 |
| Arthritis | 11 (5.3) | 0 (0.0) | 11 (5.9) | 0.605 |
| Serositis | 48 (23.2) | 6 (30.0) | 42 (22.5) | 0.449 |
| Neurologic disorder | 2 (1.0) | 0 (0.0) | 2 (1.1) | 0.999 |
| Hematologic disorder | 179 (86.5) | 18 (90.0) | 161 (86.1) | 0.999 |
| Immunologic disorder | 183 (88.4) | 17 (85.0) | 166 (88.8) | 0.710 |
| Laboratory data | ||||
| Lymphocyte count (/mm3) | 900.0 (602.5–1260.0) | 655.0 (330.0–1070.0) | 940.0 (610.0–1270.0) | 0.012 |
| ESR (mm/h) | 48.0 (26.0–75.0) | 46.0 (28.0–66.5) | 48.0 (26.0–75.0) | 0.867 |
| CRP (mg/L) | 2.3 (1.0–7.3) | 4.7 (1.7–15.8) | 2.3 (1.0–6.3) | 0.061 |
| Cr (mg/dL) | 0.8 (0.6–1.1) | 1.6 (0.9–3.6) | 0.8 (0.6–1.1) | <0.001 |
| GFR (CKD-EPI), mL/min/1.73 m2 | 94.0 (64.3–115.0) | 38.5 (17.0–73.5) | 100.0 (69.0–117.0) | <0.001 |
| Total cholesterol (mg/dL) | 196.0 (159.3–243.8) | 220.0 (185.0–234.5) | 195.0 (156.0–245.8) | 0.557 |
| Serum albumin (g/dL) | 2.9 (2.3–3.4) | 2.5 (2.1–3.1) | 2.9 (2.3–3.4) | 0.067 |
| AST (IU/L) | 21.0 (17.0–35.5) | 26.0 (16.5–44.5) | 21.0 (17.0–34.0) | 0.366 |
| ALT (IU/L) | 16.0 (10.0–25.0) | 15.0 (9.5–30.0) | 16.0 (10.0–25.0) | 0.684 |
| Renal biopsy data | ||||
| Lupus nephritis class, n (%) | ||||
| Class I | 3 (1.4) | 0 (0.0) | 3 (1.6) | 0.999 |
| Class II | 8 (3.9) | 0 (0.0) | 8 (4.3) | 0.999 |
| Pure class III | 49 (23.7) | 5 (25.0) | 44 (23.5) | 0.883 |
| Pure class IV | 92 (44.4) | 13 (65.0) | 79 (42.2) | 0.052 |
| Pure class V | 23 (11.1) | 1 (5.0) | 22 (11.8) | 0.706 |
| Mixed class V | 31 (105.0) | 0 (0.0) | 31 (16.6) | 0.049 |
| Class V + II | 1 (0.5) | 0 (0.0) | 1 (0.5) | |
| Class V + III | 21 (10.1) | 0 (0.0) | 21 (11.2) | |
| Class V + IV | 9 (4.3) | 0 (0.0) | 9 (4.8) | |
| Class VI | 1 (0.5) | 1 (5.0) | 0 (0.0) | 0.097 |
| Activity/Chronicity index | ||||
| Activity index | 7.0 (2.0–11.0) | 8.5 (4.5–12.0) | 7.0 (2.0–11.0) | 0.126 |
| Chronicity index | 1.0 (1.0–2.0) | 2.0 (1.5–5.0) | 1.0 (1.0–2.0) | <0.001 |
| Nutritional indices | ||||
| CONUT score | 4.0 (3.0–5.0) | 4.5 (4.0–5.5) | 4.0 (3.0–5.0) | 0.173 |
| PNI | 33.9 (26.7–39.3) | 31.1 (23.7–34.1) | 34.7 (27.0–39.9) | 0.012 |
| NRI | 48.8 (44.4–53.2) | 49.8 (44.5–53.8) | 48.7 (44.4–53.0) | 0.584 |
| NLR | 3.7 (2.1–6.7) | 4.7 (2.4–12.4) | 3.6 (2.1–6.3) | 0.070 |
| BMI | 21.9 (20.0–24.0) | 22.4 (20.1–25.1) | 21.8 (19.9–23.9) | 0.595 |
| Variables | CONUT Score | PNI | NRI | NLR | BMI |
|---|---|---|---|---|---|
| SLE activity-related measures | |||||
| SLEDAI-2K | 0.467 (<0.001) | −0.356 (<0.001) | −0.183 (0.008) | −0.091 (0.192) | −0.088 (0.206) |
| WBC count (/mm3) | −0.264 (<0.001) | 0.205 (0.003) | 0.053 (0.449) | 0.548 (<0.001) | 0.089 (0.200) |
| Platelet count (×1000/mm3) | −0.329 (<0.001) | 0.260 (<0.001) | 0.063 (0.371) | 0.072 (0.302) | −0.002 (0.978) |
| Complement 3, mg/dL | −0.502 (<0.001) | 0.377 (<0.001) | 0.138 (0.047) | 0.058 (0.403) | 0.086 (0.217) |
| Complement 4, mg/dL | −0.335 (<0.001) | 0.223 (0.001) | 0.083 (0.236) | 0.052 (0.454) | 0.024 (0.737) |
| Anti-dsDNA (IU/mL) | 0.278 (<0.001) | −0.144 (0.038) | −0.046 (0.508) | −0.089 (0.201) | 0.007 (0.919) |
| Urinary P/Cr ratio | 0.221 (0.001) | −0.515 (<0.001) | 0.031 (0.655) | 0.064 (0.361) | 0.151 (0.030) |
| Laboratory data | |||||
| Lymphocyte count (/mm3) | −0.662 (<0.001) | 0.549 (<0.001) | 0.102 (0.145) | −0.400 (<0.001) | 0.057 (0.413) |
| ESR (mm/hr) | 0.101 (0.148) | −0.105 (0.134) | −0.095 (0.173) | −0.109 (0.119) | −0.090 (0.198) |
| CRP (mg/L) | 0.246 (<0.001) | −0.141 (0.043) | 0.059 (0.401) | 0.166 (0.017) | 0.137 (0.049) |
| Cr (mg/dL) | 0.109 (0.118) | −0.153 (0.028) | 0.021 (0.762) | 0.097 (0.166) | 0.100 (0.153) |
| GFR (CKD-EPI), mL/min/1.73 m2 | −0.042 (0.550) | 0.118 (0.090) | −0.130 (0.062) | −0.084 (0.228) | −0.216 (0.002) |
| Total cholesterol (mg/dL) | −0.133 (0.056) | −0.274 (<0.001) | 0.091 (0.192) | 0.144 (0.038) | 0.165 (0.018) |
| Serum albumin (g/dL) | −0.611 (<0.001) | 0.922 (<0.001) | 0.147 (0.034) | −0.135 (0.053) | −0.055 (0.433) |
| AST (IU/L) | 0.191 (0.006) | −0.097 (0.164) | −0.091 (0.190) | 0.010 (0.887) | −0.111 (0.110) |
| ALT (IU/L) | 0.037 (0.597) | 0.031 (0.658) | 0.002 (0.981) | 0.032 (0.646) | −0.034 (0.631) |
| Renal biopsy data | |||||
| Activity index | 0.188 (0.007) | −0.215 (0.002) | −0.007 (0.921) | 0.072 (0.302) | 0.053 (0.448) |
| Univariable Analysis | Multivariable Analysis | |||||
|---|---|---|---|---|---|---|
| Variables | Odds Ratio | 95% Confidence Interval | p-Value | Odds Ratio | 95% Confidence Interval | p-Value |
| SLEDAI-2K | 0.904 | 0.803–1.016 | 0.091 | |||
| WBC count (/mm3) | 1.000 | 0.999–1.000 | 0.744 | |||
| Platelet count (×1000/mm3) | 0.993 | 0.987–0.999 | 0.015 | |||
| Complement 3, mg/dL | 0.992 | 0.974–1.010 | 0.362 | |||
| Complement 4, mg/dL | 0.995 | 0.938–1.054 | 0.853 | |||
| Anti-dsDNA (IU/mL) | 0.998 | 0.995–1.000 | 0.063 | |||
| Urinary P/Cr ratio | 1.078 | 0.964–1.206 | 0.185 | |||
| Lymphocyte count (/mm3) | 0.999 | 0.998–0.999 | 0.023 | |||
| ESR (mm/h) | 1.000 | 0.986–1.014 | 0.999 | |||
| CRP (mg/L) | 1.012 | 0.999–1.025 | 0.070 | |||
| Cr (mg/dL) | 1.827 | 1.522, 2.193 | <0.001 | 1.623 | 1.322–1.993 | <0.001 |
| GFR (CKD-EPI), mL/min/1.73 m2 | 0.959 | 0.944, 0.975 | <0.001 | |||
| Total cholesterol (mg/dL) | 0.999 | 0.994–1.006 | 0.977 | |||
| Serum albumin (g/dL) | 0.569 | 0.311–1.041 | 0.067 | |||
| AST (IU/L) | 1.002 | 0.996–1.009 | 0.491 | |||
| ALT (IU/L) | 0.999 | 0.986–1.014 | 0.979 | |||
| Pure proliferative lupus nephritis¶ | 4.300 | 0.998–18.534 | 0.050 | |||
| Activity index | 1.076 | 0.989–1.171 | 0.089 | |||
| Chronicity index | 1.493 | 1.254–1.778 | <0.001 | 1.458 | 1.203–1.767 | <0.001 |
| CONUT score | 1.230 | 0.957–1.582 | 0.106 | |||
| PNI | 0.932 | 0.880–0.987 | 0.017 | 0.925 | 0.865–0.989 | 0.022 |
| NRI | 1.007 | 0.959–1.057 | 0.789 | |||
| NLR | 1.070 | 1.020–1.122 | 0.006 | |||
| BMI | 1.029 | 0.908–1.167 | 0.651 | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahn, S.S.; Yoo, J.; Jung, S.M.; Song, J.J.; Park, Y.-B.; Lee, S.-W. Comparison of the Clinical Implications among Five Different Nutritional Indices in Patients with Lupus Nephritis. Nutrients 2019, 11, 1456. https://doi.org/10.3390/nu11071456
Ahn SS, Yoo J, Jung SM, Song JJ, Park Y-B, Lee S-W. Comparison of the Clinical Implications among Five Different Nutritional Indices in Patients with Lupus Nephritis. Nutrients. 2019; 11(7):1456. https://doi.org/10.3390/nu11071456
Chicago/Turabian StyleAhn, Sung Soo, Juyoung Yoo, Seung Min Jung, Jason Jungsik Song, Yong-Beom Park, and Sang-Won Lee. 2019. "Comparison of the Clinical Implications among Five Different Nutritional Indices in Patients with Lupus Nephritis" Nutrients 11, no. 7: 1456. https://doi.org/10.3390/nu11071456
APA StyleAhn, S. S., Yoo, J., Jung, S. M., Song, J. J., Park, Y.-B., & Lee, S.-W. (2019). Comparison of the Clinical Implications among Five Different Nutritional Indices in Patients with Lupus Nephritis. Nutrients, 11(7), 1456. https://doi.org/10.3390/nu11071456