Relative Validity and Reproducibility of a Food Frequency Questionnaire to Assess Energy Intake from Minimally Processed and Ultra-Processed Foods in Young Children

 ,
,  , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. EAT5 Food Frequency Questionnaire
2.4. Weighed Diet Record (WDR)
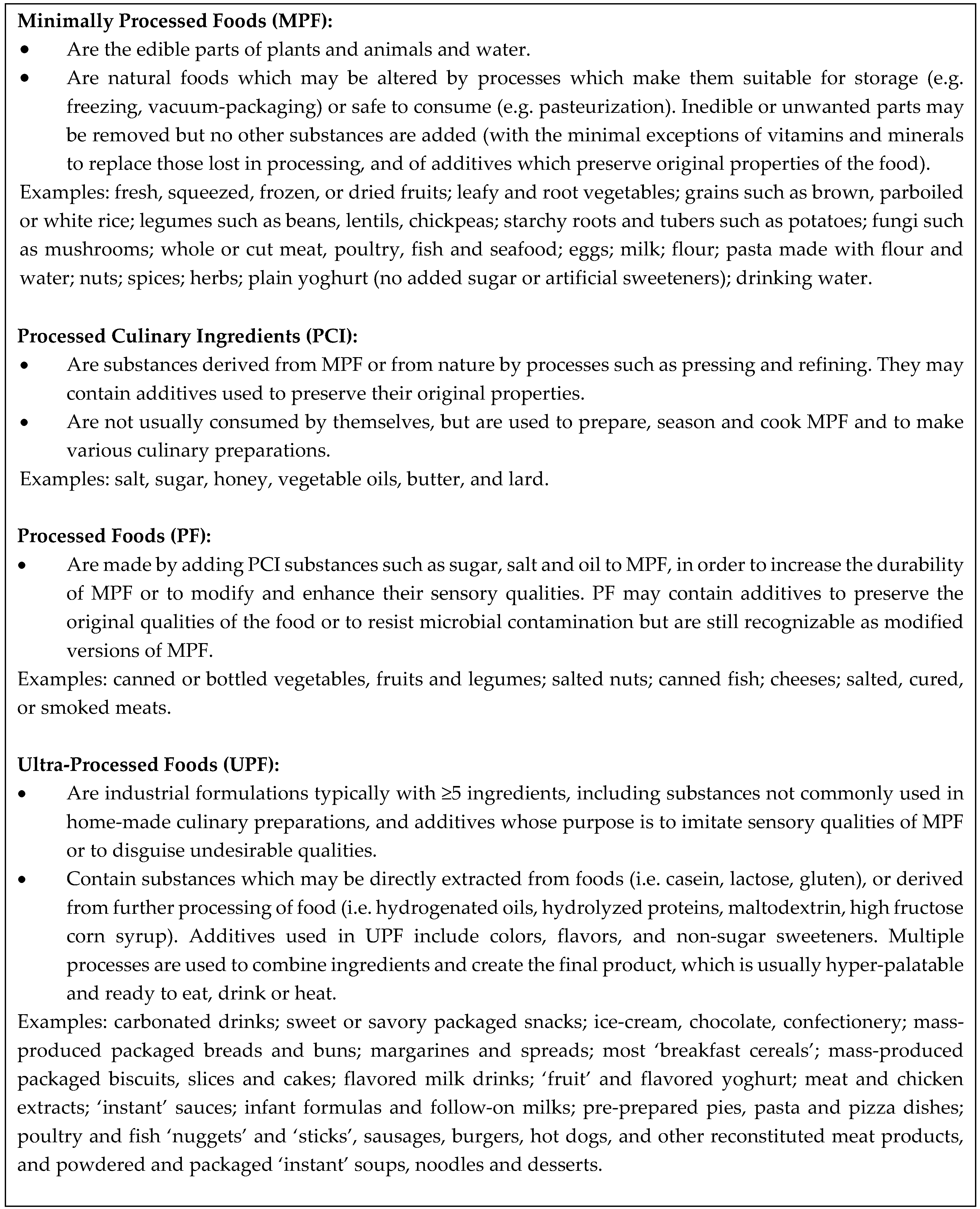
2.5. NOVA Food Processing Categories
2.6. Statistical Analysis
3. Results
3.1. Study Population
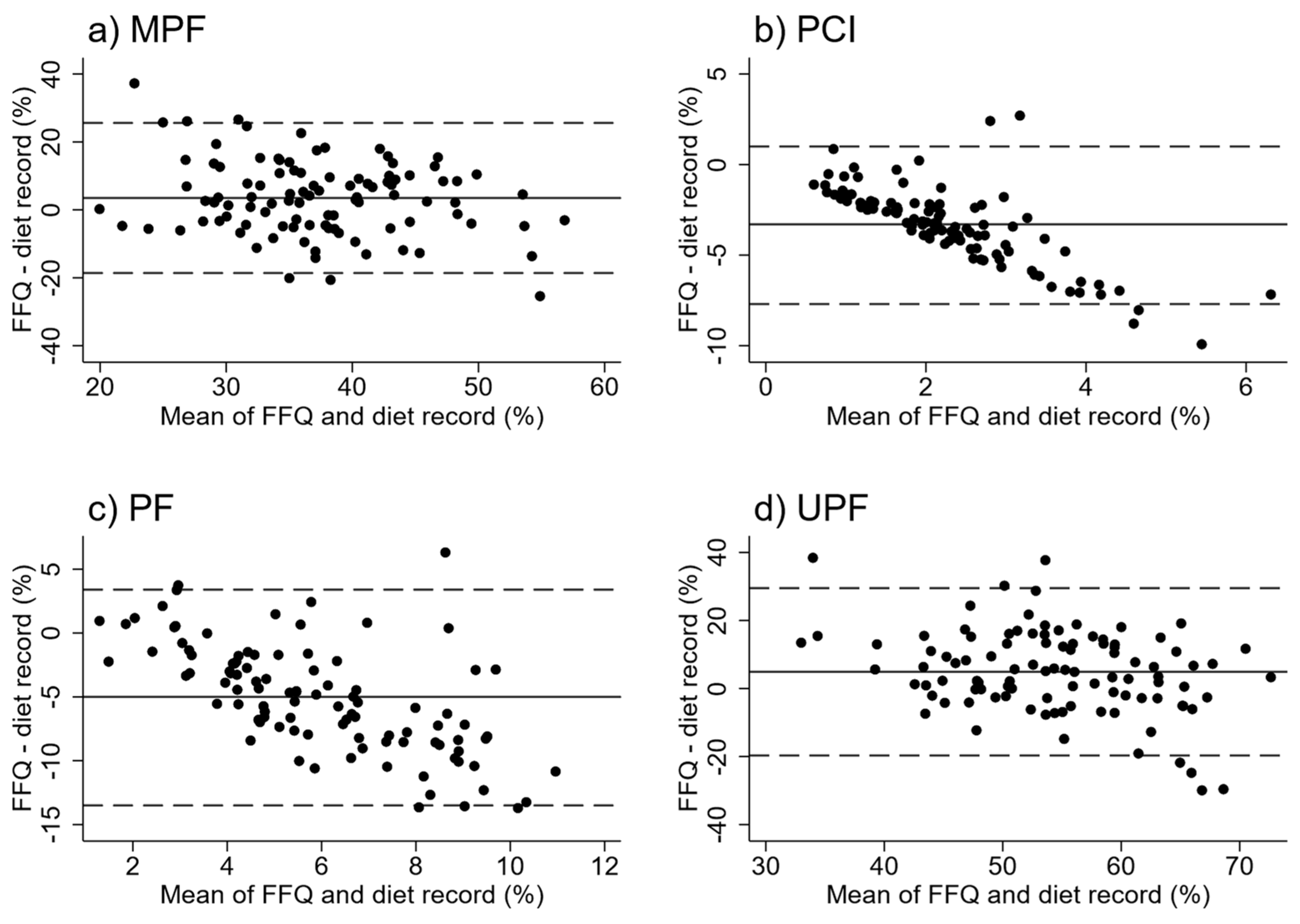
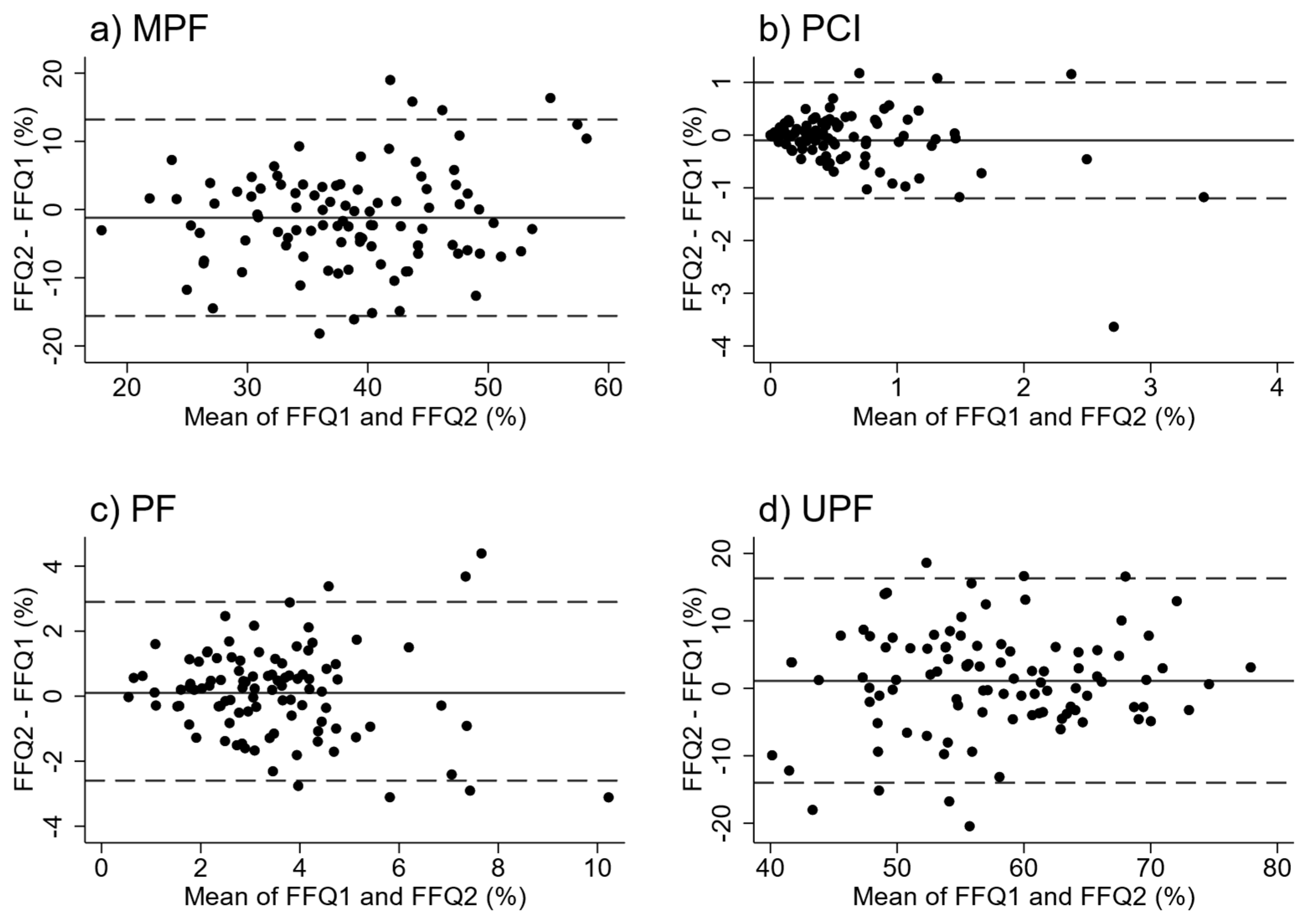
3.2. Relative Validity and Reproducibility of Energy Intakes (kJ and %) from NOVA Groups
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Processed Food Category | ||||
|---|---|---|---|---|
| Mean proportion of recipes | MPF | PCI | PF | UPF |
| By weight (g) | 60.5 | 8.6 | 13.2 | 17.7 |
| By energy content (kJ) | 52.8 | 12.5 | 12.5 | 22 |
| Mean difference between weight (g) and energy (kJ) content of recipes | 7.7 | −3.9 | 0.7 | −4.3 |
References
- Monteiro, C.A.; Cannon, G.; Levy, R.; Moubarac, J.-C.; Jaime, P.; Martins, A.P.; Canella, D.; Louzada, M.; Parra, D. NOVA. The Star Shines Bright. (Food Classification Public Health). World Nutr. 2016, 7, 28–38. [Google Scholar]
- Monteiro, C.A.; Cannon, G.; Moubarac, J.-C.; Levy, R.B.; Louzada, M.L.C.; Jaime, P.C. The UN Decade of Nutrition, the NOVA food classification and the trouble with ultra-processing. Public Health Nutr. 2017, 21, 5–17. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, C.A.; Moubarac, J.-C.; Cannon, G.; Ng, S.W.; Popkin, B. Ultra-processed products are becoming dominant in the global food system. Obes. Rev. 2013, 14 (Suppl. 2), 21–28. [Google Scholar] [CrossRef]
- Moodie, R.; Stuckler, D.; Monteiro, C.; Sheron, N.; Neal, B.; Thamarangsi, T.; Lincoln, P.; Casswell, S. On Behalf of The Lancet Ncd Action Group. Profits and Pandemics: Prevention of harmful effects of tobacco, alcohol and ultra-processed food and drink industries. Lancet 2013, 381, 670–679. [Google Scholar] [CrossRef]
- Moubarac, J.-C.; Batal, M.; Martins, A.P.B.; Claro, R.; Levy, R.B. Processed and Ultra-processed Food Products: Consumption Trends in Canada from 1938 to 2011. Can. J. Dietet. Pract. Res. 2014, 75, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Moubarac, J.-C.; Batal, M.; Louzada, M.I.; Martinez Steele, E.; Monteiro, C.A. Consumption of ultra-processed foods predicts diet quality in Canada. Appetite 2017, 108, 512–520. [Google Scholar] [CrossRef]
- Louzada, M.L.D.C.; Ricardo, C.Z.; Martinez Steele, E.; Levy, R.B.; Cannon, G.; Monteiro, C.A. The share of ultra-processed foods determines the overall nutritional quality of diets in Brazil. Public Health Nutr. 2017, 21, 94–102. [Google Scholar] [CrossRef]
- Martinez Steele, E.M.; Popkin, B.M.; Swinburn, B.; Monteiro, C.A. The share of ultra-processed foods and the overall nutritional quality of diets in the US: Evidence from a nationally representative cross-sectional study. Popul. Health Metr. 2017, 15, 6. [Google Scholar] [CrossRef]
- Julia, C.; Martinez, L.; Alles, B.; Touvier, M.; Hercberg, S.; Mejean, C.; Kesse-Guyot, E. Contribution of ultra-processed foods in the diet of adults from the French NutriNet-Sante study. Public Health Nutr. 2017, 21, 27–37. [Google Scholar] [CrossRef]
- Rauber, F.; Da Costa, M.; Millett, C.; Monteiro, C. Ultra-Processed Food Consumption and Chronic Non-Communicable Diseases-Related Dietary Nutrient Profile in the UK (2008–2014). Nutrients 2018, 10, 587. [Google Scholar] [CrossRef]
- Louzada, M.L.D.C.; Baraldi, L.G.; Martinez Steele, E.; Martins, A.P.B.; Canella, D.S.; Moubarac, J.-C.; Levy, R.B.; Cannon, G.; Afshin, A.; Imamura, F.; et al. Consumption of ultra-processed foods and obesity in Brazilian adolescents and adults. Prev. Med. 2015, 81, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Marron-Ponce, J.A.; Sanchez-Pimienta, T.G.; Louzada, M.L.D.C.; Batis, C. Energy contribution of NOVA food groups and sociodemographic determinants of ultra-processed food consumption in the Mexican population. Public Health Nutr. 2017, 21, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Martinez Steele, E.M.; Baraldi, L.G.; Louzada, M.L.; Moubarac, J.-C.; Mozaffarian, D.; Monteiro, C.A. Ultra-processed foods and added sugars in the US diet: Evidence from a nationally representative cross-sectional study. BMJ Open 2016, 6, e009892. [Google Scholar] [CrossRef] [PubMed]
- Bielemann, R.M.; Santos, L.P.; Costa, C.D.S.; Matiajasevich, A.; Santos, I.S. Early feeding practices and consumption of ultraprocessed foods at 6 y of age: Findings from the 2004 Pelotas (Brazil) Birth Cohort Study. Nutrition 2018, 47, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Rauber, F.; Campagnolo, P.D.B.; Hoffman, D.J.; Vitolo, M.R. Consumption of ultra-processed food products and its effects on children’s lipid profiles: A longitudinal study. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, P.C.A.; Ribeiro, S.A.V.; Andreoli, C.S.; de Carvalho, C.A.; Pessoa, M.C.; de Novaes, J.F.; Priore, S.E.; Franceschini, S.D.C.C. Association of exclusive breastfeeding duration with consumption of ultra-processed foods, fruit and vegetables in Brazilian children. Eur. J. Nutr. 2018. [Google Scholar] [CrossRef] [PubMed]
- Karnopp, E.V.N.; dos Santos Vaz, J.; Schafer, A.A.; Muniz, L.C.; de Leon Veleda de Souza, R.; dos Santosc, I.; Gigante, D.P.; Assuncao, M.C.F. Food consumption of children younger than 6 years according to the degree of food processing. J. Pediatr. 2017, 93, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Gibson, R.S. Principles of Nutritional Assessment; Oxford University Press: Oxford, UK, 2005. [Google Scholar]
- Cade, J.; Thompson, R.; Burley, V.; Warm, D. Development, validation and utilisation of food-frequency questionnaires—A review. Public Health Nutr. 2002, 5, 567–587. [Google Scholar] [CrossRef] [PubMed]
- Willett, W. Nutritional Epidemiology, 2nd ed.; Oxford University Press: Oxford, UK, 1998. [Google Scholar]
- Leong, C.; Taylor, R.W.; Haszard, J.J.; Fleming, E.A.; Tannock, G.W.; Szymlek-Gay, E.A.; Cameron, S.L.; Yu, R.; Carter, H.; Chee, L.K.; et al. Relative Validity and Reproducibility of a Food Frequency Questionnaire to Assess Nutrients and Food Groups of Relevance to the Gut Microbiota in Young Children. Nutrients 2018, 10, 1627. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, J.; Salmond, P.; Crampton, C. NZDep2013 Index of Deprivation; University of Otago: Wellington, New Zealand, 2014. [Google Scholar]
- Watson, E.O.; Heath, A.-L.M.; Taylor, R.W.; Mills, V.C.; Barris, A.C.; Skidmore, P.M.L. Relative validity and reproducibility of an FFQ to determine nutrient intakes of New Zealand toddlers aged 12–24 months. Public Health Nutr. 2015, 18, 3265–3271. [Google Scholar] [CrossRef] [PubMed]
- Mills, V.C.; Skidmore, P.M.L.; Watson, E.O.; Taylor, R.W.; Fleming, E.A.; Heath, A.-L.M. Relative Validity and Reproducibility of a Food Frequency Questionnaire for Identifying the Dietary Patterns of Toddlers in New Zealand. J. Acad. Nutr. Diet. 2015, 115, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Marriott, L.D.; Inskip, H.M.; Borland, S.E.; Godfrey, K.M.; Law, C.M.; Robinson, S.M. What do babies eat? Evaluation of a food frequency questionnaire to assess the diets of infants aged 12 months. Public Health Nutr. 2009, 12, 967–972. [Google Scholar] [CrossRef] [PubMed]
- New Zealand Institute for Plant & Food Research Limited. Ministry of Health New Zealand Food Composition Database. New Zealand FOODfiles™ 2014. Available online: http://www.foodcomposition.co.nz/foodfiles (accessed on 1 January 2018).
- Harttig, U.; Haubrock, J.; Knüppel, S.; Boeing, H. The MSM program: Web-based statistics package for estimating usual dietary intake using the Multiple Source Method. Eur. J. Clin. Nutr. 2011, 65, S87–S91. [Google Scholar] [CrossRef] [PubMed]
- O’Halloran, S.A.; Lacy, K.E.; Woods, J.; Grimes, C.A.; Campbell, K.J.; Nowson, C.A. The provision of ultra-processed foods and their contribution to sodium availability in Australian long day care centres. Public Health Nutr. 2017, 21, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Gibney, M.J.; Forde, C.G.; Mullally, D.; Gibney, E.R. Ultra-processed foods in human health: A critical appraisal. Am. J. Clin. Nutr. 2017, 106, 717–724. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.M. Food processing: Criteria for dietary guidance and public health? Proc. Nutr. Soc. 2019, 78, 4–18. [Google Scholar] [CrossRef] [PubMed]
- O’Halloran, S.A.; Lacy, K.E.; Grimes, C.A.; Woods, J.; Campbell, K.J.; Nowson, C.A. A novel processed food classification system applied to Australian food composition databases. J. Hum. Nutr. Diet. 2017, 30, 534–541. [Google Scholar] [CrossRef] [PubMed]



| Mean (SD) from WDR | Mean (SD) from FFQ | Mean difference (95% CI) between FFQ and WDR | p-Value | 95% Limits of Agreement | Intra-Class Correlation Coefficient between FFQ and WDR | |
|---|---|---|---|---|---|---|
| MPF | ||||||
| EI (kJ) | 2088 (705) | 2798 (967) | 710 (503, 918) | <0.001 | 0 to 2800 | 0.24 |
| EI (%) | 35.6 (10.4) | 39.1 (8.3) | 3.5 (1.3, 5.7) | 0.002 | −18.6 to 25.6 | 0.31 |
| PCI | ||||||
| EI (kJ) | 229 (116) | 44 (58) | −185 (−211, −158) | <0.001 | −452 to 82 | −0.05 |
| EI (%) | 4.0 (2.0) | 0.6 (0.7) | −3.3 (−3.8, −2.9) | <0.001 | −7.7 to 0.1 | −0.01 |
| PF | ||||||
| EI (kJ) | 499 (264) | 242 (141) | −257 (−318, −196) | <0.001 | −870 to 355 | −0.05 |
| EI (%) | 8.5 (4.0) | 3.4 (1.9) | −5.0 (−5.9, −4.2) | <0.001 | −13.5 to 3.4 | 0.07 |
| UPF | ||||||
| EI (kJ) | 3009 (820) | 4102 (1386) | 1093 (818, 1368) | <0.001 | 0 to 3864 | 0.26 |
| EI (%) | 52.0 (11.9) | 56.9 (8.6) | 4.9 (2.5, 7.3) | <0.001 | −19.7 to 29.5 | 0.30 |
| Quartiles of Daily Energy Intake from Processed Food Categories Using Food Frequency Questionnaire | p-Value For Trend | ||||
|---|---|---|---|---|---|
| Mean (SD) daily EI from NOVA categories using WDR | Quartile 1 | Quartile 2 | Quartile 3 | Quartile 4 | |
| MPF | |||||
| EI (kJ) | 1882 (427) | 2149 (535) | 2155 (732) | 2166 (992) | 0.175 |
| EI (%) | 33.3 (7.3) | 33.9 (9.3) | 33.1 (12.7) | 42.1 (9.1) | 0.006 |
| PCI | |||||
| EI (kJ) | 207 (97) | 228 (123) | 263 (114) | 217 (129) | 0.548 |
| EI (%) | 3.1 (1.4) | 4.5 (2.0) | 4.5 (2.1) | 3.7 (2.3) | 0.308 |
| PF | |||||
| EI (kJ) | 496 (285) | 423 (196) | 599 (277) | 480 (274) | 0.593 |
| EI (%) | 8.1 (3.4) | 7.0 (3.7) | 9.9 (4.3) | 8.9 (4.1) | 0.145 |
| UPF | |||||
| EI (kJ) | 2607 (682) | 2956 (760) | 3243 (822) | 3230 (883) | 0.003 |
| EI (%) | 44.9 (8.7) | 55.3 (15.9) | 52.8 (9.5) | 54.9 (9.6) | 0.009 |
| Correctly Classified 1 | Correctly or Adjacently Classified 2 | Correct Extremes 3 | Grossly Misclassified 4 | |
|---|---|---|---|---|
| Chance | 25% | 62.5% | 12.5% | 12.5% |
| MPF | ||||
| EI (kJ) | 23 | 70 | 15 | 9 |
| EI (%) | 33 | 72 | 19 | 7 |
| PCI | ||||
| EI (kJ) | 31 | 67 | 13 | 14 |
| EI (%) | 30 | 66 | 15 | 12 |
| PF | ||||
| EI (kJ) | 25 | 70 | 13 | 13 |
| EI (%) | 29 | 68 | 13 | 9 |
| UPF | ||||
| EI (kJ) | 29 | 73 | 18 | 6 |
| EI (%) | 32 | 74 | 20 | 4 |
| FFQ1 Mean (SD) | FFQ2 Mean (SD) | Mean Difference (95% CI) between both FFQ Administrations | p-Value | 95% Limits of Agreement | Intra-Class Correlation Coefficient | |
|---|---|---|---|---|---|---|
| MPF | ||||||
| EI (kJ) | 2802 (971) | 2564 (855) | −239 (−373, −104) | 0.001 | 0 to 1108 | 0.73 |
| EI (%) | 39.1 (8.4) | 37.9 (9.4) | −1.2 (−2.6, 0.2) | 0.102 | −15.6 to 13.2 | 0.67 |
| PCI | ||||||
| EI, kJ | 44.2 (58.3) | 36.9 (34.0) | −7.3 (−16.7, 2.2) | 0.129 | −102 to 87 | 0.51 |
| EI, % | 0.63 (0.74) | 0.56 (0.55) | −0.07 (−0.18, 0.04) | 0.196 | −1.1 to 1.0 | 0.64 |
| PF | ||||||
| EI, kJ | 243 (142) | 240 (119) | −3 (−25, 19) | 0.764 | −223 to 217 | 0.65 |
| EI, % | 3.4 (1.9) | 3.6 (1.7) | 0.1 (−0.1, 0.4) | 0.336 | −2.6 to 2.9 | 0.70 |
| UPF | ||||||
| EI, kJ | 4102 (1393) | 4003 (1427) | −99 (−295, 97) | 0.319 | 0 to 1868 | 0.76 |
| EI, % | 56.8 (8.6) | 58.0 (9.3) | 1.1 (−0.4, 2.6) | 0.141 | −14.0 to 16.3 | 0.64 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fangupo, L.J.; Haszard, J.J.; Leong, C.; Heath, A.-L.M.; Fleming, E.A.; Taylor, R.W. Relative Validity and Reproducibility of a Food Frequency Questionnaire to Assess Energy Intake from Minimally Processed and Ultra-Processed Foods in Young Children. Nutrients 2019, 11, 1290. https://doi.org/10.3390/nu11061290
Fangupo LJ, Haszard JJ, Leong C, Heath A-LM, Fleming EA, Taylor RW. Relative Validity and Reproducibility of a Food Frequency Questionnaire to Assess Energy Intake from Minimally Processed and Ultra-Processed Foods in Young Children. Nutrients. 2019; 11(6):1290. https://doi.org/10.3390/nu11061290
Chicago/Turabian StyleFangupo, Louise J., Jillian J. Haszard, Claudia Leong, Anne-Louise M. Heath, Elizabeth A. Fleming, and Rachael W. Taylor. 2019. "Relative Validity and Reproducibility of a Food Frequency Questionnaire to Assess Energy Intake from Minimally Processed and Ultra-Processed Foods in Young Children" Nutrients 11, no. 6: 1290. https://doi.org/10.3390/nu11061290
APA StyleFangupo, L. J., Haszard, J. J., Leong, C., Heath, A.-L. M., Fleming, E. A., & Taylor, R. W. (2019). Relative Validity and Reproducibility of a Food Frequency Questionnaire to Assess Energy Intake from Minimally Processed and Ultra-Processed Foods in Young Children. Nutrients, 11(6), 1290. https://doi.org/10.3390/nu11061290