Consumption of Aged White Wine under a Veil of Flor Reduces Blood Pressure-Increasing Plasma Nitric Oxide in Men at High Cardiovascular Risk



Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
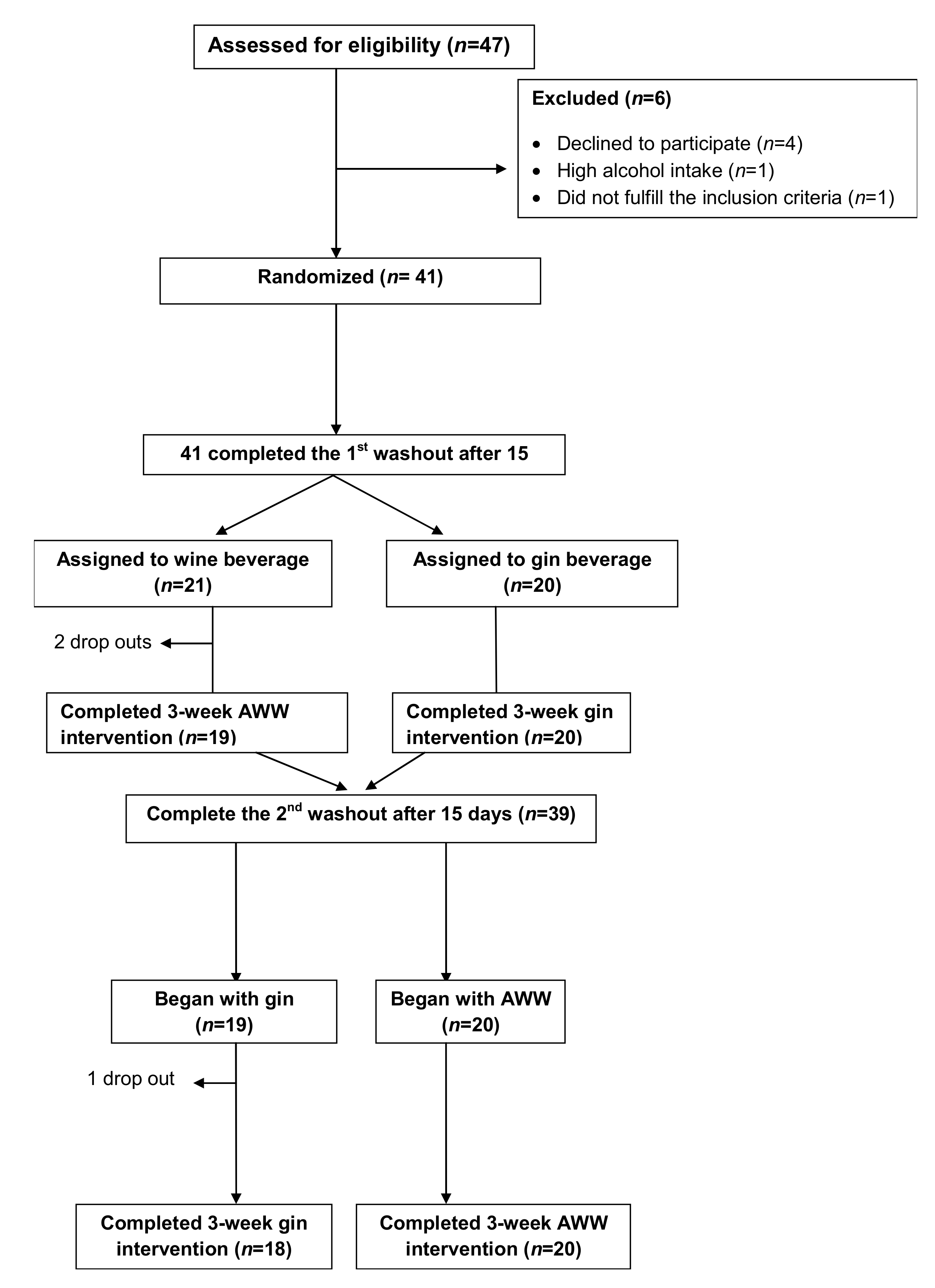
2.2. Study Design
2.3. Diet and Exercise Monitoring
2.4. Clinical and Laboratory Measurements
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Participants and Assessment of Side Effects
3.2. Intervention, Diet, and Physical Activity Monitoring
3.3. Changes in Cardiovascular Risk Factors after 3 Weeks of Intervention
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Weiner, D.E.; Tighiouart, H.; Amin, M.G.; Stark, P.C.; MacLeod, B.; Griffith, J.L.; Salem, D.N.; Levey, A.S.; Sarnak, M.J. Chronic Kidney Disease as a Risk Factor for Cardiovascular Disease and All-Cause Mortality: A Pooled Analysis of Community-Based Studies. J. Am. Soc. Nephrol. 2004, 15, 1307–1315. [Google Scholar] [CrossRef] [PubMed]
- Lackland, D.T.; Weber, M.A. Global burden of cardiovascular disease and stroke: Hypertension at the core. Can. J. Cardiol. 2015, 31, 569–571. [Google Scholar] [CrossRef]
- Huang, P.H.; Chen, Y.H.; Tsai, H.Y.; Chen, J.S.; Wu, T.C.; Lin, F.Y.; Sata, M.; Chen, J.W.; Lin, S.J. Intake of red wine increases the number and functional capacity of circulating endothelialprogenitor cells by enhancing nitric oxide bioavailability. Arterioscler. Thromb. Vasc. Biol. 2010, 30, 869–877. [Google Scholar] [CrossRef] [PubMed]
- Krenz, M.; Korthuis, R.J. Moderate ethanol ingestion and cardiovascular protection: From epidemiologic associations to cellular mechanisms. J. Mol. Cell. Cardiol. 2012, 52, 93–104. [Google Scholar] [CrossRef]
- Machha, A.; Schechter, A.N. Dietary nitrite and nitrate: A review of potential mechanisms of cardiovascular benefits. Eur. J. Nutr. 2011, 50, 293–303. [Google Scholar] [CrossRef] [PubMed]
- Bahadoran, Z.; Mirmiran, P.; Ghasemi, A.; Carlström, M.; Azizi, F.; Hadaegh, F. Association between Dietary Intakes of Nitrate and Nitrite and the Risk of Hypertension and Chronic Kidney Disease: Tehran Lipid and Glucose Study. Nutrients 2016, 8, 811. [Google Scholar] [CrossRef]
- Ramms, B.; Gordts, P.L. Dietary nitrate struggles in atherosclerosis. Atherosclerosis 2016, 245, 71–73. [Google Scholar] [CrossRef][Green Version]
- Habermeyer, M.; Roth, A.; Guth, S.; Diel, P.; Engel, K.H.; Epe, B.; Fürst, P.; Heinz, V.; Humpf, H.U.; Joost, H.G.; et al. Nitrate and nitrite in the diet: How to assess their benefit and risk for human health. Mol. Nutr. Food Res. 2015, 59, 106–128. [Google Scholar] [CrossRef]
- Ashworth, A.; Bescos, R. Dietary nitrate and blood pressure: Evolution of a new nutrient? Nutr. Res. Rev. 2017, 17, 1–12. [Google Scholar] [CrossRef]
- Bondonno, C.P.; Yang, X.; Croft, K.D.; Considine, M.J.; Ward, N.C.; Rich, L.; Puddey, I.B.; Swinny, E.; Mubarak, A.; Hodgson, J.M. Flavonoid-rich apples and nitrate-rich spinach augment nitric oxide status and improve endothelial function in healthy men and women: A randomized controlled trial. Free Radic. Biol. Med. 2012, 52, 95–102. [Google Scholar] [CrossRef]
- Kapil, V.; Khambata, R.S.; Robertson, A.; Caulfield, M.J.; Ahluwalia, A. Dietary nitrate provides sustained blood pressure lowering in hypertensive patients: A randomized, phase 2, double-blind, placebo-controlled study. Hypertension 2015, 65, 320–327. [Google Scholar] [CrossRef]
- Kondrashov, A.; Vranková, S.; Dovinová, I.; Sevčík, R.; Parohová, J.; Barta, A.; Pecháňová, O.; Kovacsová, M. The effects of new Alibernet red wine extract on nitric oxide and reactive oxygen species production in spontaneously hypertensive rats. Oxid. Med. Cell Longev. 2012, 2012, 806285. [Google Scholar] [CrossRef] [PubMed]
- Chiva-Blanch, G.; Urpi-Sarda, M.; Ros, E.; Arranz, S.; Valderas-Martínez, P.; Casas, R.; Sacanella, E.; Llorach, R.; Lamuela-Raventos, R.M.; Andres-Lacueva, C.; et al. Dealcoholized red wine decreases systolic and diastolic blood pressure and increases plasma nitric oxide: Short communication. Circ. Res. 2012, 111, 1065–1068. [Google Scholar] [CrossRef]
- Roth, I.; Casas, R.; Medina-Remón, A.; Lamuela-Raventós, R.M.; Estruch, R. Consumption of aged white wine modulates cardiovascular risk factors via circulating endothelial progenitor cells and inflammatory biomarkers. Clin. Nutr. 2019, 38, 1036–1044. [Google Scholar] [CrossRef] [PubMed]
- Schröder, H.; Covas, M.I.; Marrugat, J.; Vila, J.; Pena, A.; Alcántara, M.; Masiá, R. Use of a three-day estimated food record, a 72-hour recall and a food-frequency questionnaire for dietary assessment in a Mediterranean Spanish population. Clin. Nutr. 2001, 20, 429–437. [Google Scholar] [CrossRef] [PubMed]
- Elosua, R.; Marrugat, J.; Molina, L.; Pons, S.; Pujol, E. Validation of the Minnesota Leisure Time Physical Activity Questionnaire in Spanish men. The MARATHOM Investigators. Am. J. Epidemiol. 1994, 139, 1197–1209. [Google Scholar] [CrossRef] [PubMed]
- Chiva-Blanch, G.; Condines, X.; Magraner, E.; Roth, I.; Valderas-Martínez, P.; Arranz, S.; Casas, R.; Martínez-Huélamo, M.; Vallverdú-Queralt, A.; Quifer-Rada, P.; et al. The non-alcoholic fraction of beer increases stromal cell derived factor 1 and the number of circulating endothelial progenitor cells in high cardiovascular risk subjects: A randomized clinical trial. Atherosclerosis 2014, 233, 518–524. [Google Scholar] [CrossRef]
- Regueiro, J.; Vallverdú-Queralt, A.; Simal-Gándara, J.; Estruch, R.; Lamuela-Raventós, R. Development of a LC-ESI-MS/MS approach for the rapid quantification of main wine organic acids in human urine. J. Agric. Food Chem. 2013, 61, 6763–6768. [Google Scholar] [CrossRef]
- Liu, A.H.; Bondonno, C.P.; Croft, K.D.; Puddeym, I.B.; Woodman, R.J.; Rich, L.; Ward, N.C.; Vita, J.A.; Hodgson, J.M. Effects of a nitrate-rich meal on arterial stiffness and blood pressure in healthy volunteers. Nitric Oxide 2013, 35, 123–130. [Google Scholar] [CrossRef]
- Sindler, A.L.; Devan, A.E.; Fleenor, B.S.; Seals, D.R. Inorganic nitrite supplementation for healthy arterial aging. J. Appl. Physiol. 2014, 116, 463–477. [Google Scholar] [CrossRef]
- Tang, Y.; Jiang, H.; Bryan, N.S. Nitrite and nitrate: Cardiovascular risk-benefit and metabolic effect. Curr. Opin. Lipidol. 2011, 22, 11–15. [Google Scholar] [CrossRef] [PubMed]
- Carlstrom, M.; Persson, A.E.; Larsson, E.; Hezel, M.; Scheffer, P.G.; Teerlink, T.; Weitzberg, E.; Lundberg, J.O. Dietary nitrate attenuates oxidative stress, prevents cardiac and renal injuries, and reduces blood pressure in salt-induced hypertension. Cardiovasc. Res. 2011, 89, 574–585. [Google Scholar] [CrossRef] [PubMed]
- Hezel, M.; Peleli, M.; Liu, M.; Zollbrecht, C.; Jensen, B.L.; Checa, A.; Giulietti, A.; Wheelock, C.E.; Lundberg, J.O.; Weitzberg, E.; et al. Dietary nitrate improves age-related hypertension and metabolic abnormalities in rats via modulation of angiotensin II receptor signaling and inhibition of superoxide generation. Free Radic. Biol. Med. 2016, 99, 87–98. [Google Scholar] [CrossRef] [PubMed]
- Lundberg, J.O.; Carlstrom, M.; Larsen, F.J.; Weitzberg, E. Roles of dietary inorganic nitrate in cardiovascular health and disease. Cardiovasc. Res. 2011, 89, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Brunelli, E.; La Russa, D.; Pellegrino, D. Impaired Oxidative Status Is Strongly Associated with Cardiovascular Risk Factors. Oxid. Med. Cell Longev. 2017, 2017, 6480145. [Google Scholar] [CrossRef] [PubMed]
- La Russa, D.; Brunelli, E.; Pellegrino, D. Oxidative imbalance and kidney damage in spontaneously hypertensive rats: Activation of extrinsic apoptotic pathways. Clin. Sci. 2017, 131, 1419–1428. [Google Scholar] [CrossRef]
- Ahmad, A.; Singhal, U.; Hossain, M.M.; Islam, N.; Rizvi, I. The role of the endogenous antioxidant enzymes and malondialdehyde in essential hypertension. J. Clin. Diagn. Res. 2013, 7, 987–990. [Google Scholar] [CrossRef]
- Ward, N.C.; Hodgson, J.M.; Puddey, I.B.; Mori, T.A.; Beilin, L.J.; Croft, K.D. Oxidative stress in human hypertension: Association with antihypertensive treatment, gender, nutrition, and lifestyle. Free Radic. Biol. Med. 2004, 36, 226–232. [Google Scholar] [CrossRef]
- Andersen, U.O.; Jensen, G.B. Population blood pressure and low moderate alcohol intake in untreated population followed over 20 years. Copenhagen City Heart Study. Eur. Heart J. 2011, 32, 3081–3087. [Google Scholar] [CrossRef]
- Chiva-Blanch, G.; Arranz, S.; Lamuela-Raventós, R.M.; Estruch, R. Effects of wine, alcohol and polyphenols on cardiovascular disease risk factors: Evidences from human studies. Alcohol Alcohol. 2013, 48, 270–277. [Google Scholar] [CrossRef]
- Briasoulis, A.; Agarwal, V.; Messerli, F.H. Alcohol consumption and the risk of hypertension in men and women: A systematic review and meta-analysis. J. Clin. Hypertens. 2012, 14, 792–798. [Google Scholar] [CrossRef] [PubMed]
- Roerecke, M.; Tobe, S.W.; Kaczorowski, J.; Bacon, S.L.; Vafaei, A.; Hasan, O.S.M.; Krishnan, R.J.; Raifu, A.O.; Rehm, J. Sex-Specific Associations Between AlcoholConsumption and Incidence of Hypertension: A Systematic Review and Meta-Analysis of Cohort Studies. J. Am. Heart Assoc. 2018, 7, e008202. [Google Scholar] [CrossRef] [PubMed]
- Taylor, B.; Irving, H.M.; Baliunas, D.; Roerecke, M.; Patra, J.; Mohapatra, S.; Rehm, J. Alcohol and hypertension: Gender differences in dose-response relationships determined through systematic review and meta-analysis. Addiction 2009, 104, 1981–1990. [Google Scholar] [CrossRef]
- Roerecke, M.; Kaczorowski, J.; Tobe, S.W.; Gmel, G.; Hasan, O.S.M.; Rehm, J. The effect of a reduction in alcohol consumption on blood pressure: A systematic review and meta-analysis. Lancet Public Health 2017, 2, 108–120. [Google Scholar] [CrossRef]
- Santangelo, C.; Vari, R.; Scazzocchio, B.; di Benedetto, R.; Filesi, C.; Masella, R. Polyphenols, intracellular signalling and inflammation. Ann. Ist. Super. Sanita 2007, 43, 394–405. [Google Scholar]
- Tunon, M.J.; Garcia-Mediavilla, M.V.; Sanchez-Campos, S.; Gonzalez-Gallego, J. Potential of flavonoids as anti-inflammatory agents: Modulation of pro-inflammatory gene expression and signal transduction pathways. Curr. Drug Metab. 2009, 10, 256–271. [Google Scholar] [CrossRef] [PubMed]
- Urquiaga, I.; D’Acuña, S.; Pérez, D.; Dicenta, S.; Echeverría, G.; Rigotti, A.; Leighton, F. Wine grape pomace flour improves blood pressure, fasting glucose and protein damage in humans: A randomized controlled trial. Biol. Res. 2015, 48, 49. [Google Scholar] [CrossRef]
- Diebolt, M.; Bucher, B.; Andriantsitohaina, R. Wine polyphenols decrease blood pressure, improve NO vasodilatation, and induce gene expression. Hypertension 2001, 38, 159–165. [Google Scholar] [CrossRef]
- Anselm, E.; Chataigneau, M.; Ndiaye, M.; Chataigneau, T.; Schini-Kerth, V.B. Grape juice causes endothelium-dependent relaxation via a redox-sensitive Src- and Akt-dependent activation of eNOS. Cardiovasc. Res. 2007, 73, 404–413. [Google Scholar] [CrossRef]
- Wallerath, T.; Li, H.; Godtel-Ambrust, U.; Schwarz, P.M.; Forstermann, U. A blend of polyphenolic compounds explains the stimulatory effect of red wine on human endothelial NO synthase. Nitric Oxide 2005, 12, 97–104. [Google Scholar] [CrossRef]
- Van Mierlo, L.A.; Zock, P.L.; van der Knaap, H.C.; Draijer, R. Grape polyphenols do not affect vascular function in healthy men. J. Nutr. 2010, 140, 1769–1773. [Google Scholar] [CrossRef] [PubMed]
- Dohadwala, M.M.; Hamburg, N.M.; Holbrook, M.; Kim, B.H.; Duess, M.A.; Levit, A.; Titas, M.; Chung, W.B.; Vincent, F.B.; Caiano, T.L.; et al. Effects of Concord grape juice on ambulatory blood pressure in prehypertension and stage 1 hypertension. Am. J. Clin. Nutr. 2010, 92, 1052–1059. [Google Scholar] [CrossRef] [PubMed]
- Hansen, A.S.; Marckmann, P.; Dragsted, L.O.; Nielsen, I.L.F.; Nielsen, S.E.; Grønbaek, M. Effect of red wine and red grape extract on blood lipids, haemostatic factors, and other risk factors for cardiovascular disease. Eur. J. Clin. Nutr. 2005, 59, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Botden, I.P.; Draijer, R.; Westerhof, B.E.; Rutten, J.H.; Langendonk, J.G.; Sijbrands, E.J.; Danser, A.H.; Zock, P.L.; van den Meiracker, A.H. Red wine polyphenols do not lower peripheral or central blood pressure in high normal blood pressure and hypertension. Am. J. Hypertens. 2012, 25, 718–723. [Google Scholar] [CrossRef] [PubMed]
- Botden, I.P.; Langendonk, J.G.; Meima, M.E.; Frans Boomsma, F.; Seynhaeve, A.L.; ten Hagen, T.L.M.; Jan Danser, A.H.; Sijbrands, E.J. Daily red wine consumption improves vascular function by a soluble guanylyl cyclase-dependent pathway. Am. J. Hypertens. 2011, 242, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Sivaprakasapillai, B.; Edirisinghe, I.; Randolph, J.; Steinberg, F.; Kappagoda, T. Effect of grape seed extract on blood pressure in subjects with the metabolic syndrome. Metabolism 2009, 58, 1743–1746. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Ma, W.; Zhang, P.; He, S.; Huang, D. Effect of resveratrol on blood pressure: A meta-analysis of randomized controlled trials. Clin. Nutr. 2015, 34, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Barona, J.; Aristizabal, J.C.; Blesso, C.N.; Volek, J.S.; Fernandez, M.L. Grape polyphenols reduce blood pressure and increase flow-mediated vasodilation in men with metabolic syndrome. J. Nutr. 2012, 142, 1626–1632. [Google Scholar] [CrossRef] [PubMed]
- Zamora-Ros, R.; Urpi-Sarda, M.; Lamuela-Raventós, R.M.; Martínez-González, M.Á.; Salas-Salvadó, J.; Arós, F.; Fitó, M.; Lapetra, J.; Estruch, R.; Andres-Lacueva, C. PREDIMED Study Investigators. High urinary levels of resveratrol metabolites are associated with a reduction in the prevalence of cardiovascular risk factors in high-risk patients. Pharmacol. Res. 2012, 65, 615–620. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| AWW | |
|---|---|
| Total Phenols (mEqGA/L) | 927.8 |
| Gallic acid (mg/L) | 6.0 |
| Protocatechuic acid (mg/L) | 5.6 |
| 4-Hydroxybenzoic acid (mg/L) | 0.3 |
| Vanillic acid (mg/L) | 0.7 |
| Syringic acid (mg/L) | 1.5 |
| Caffeic (mg/L) | 1.0 |
| Caffeoyl tartaric acid(mg/L) | 17.5 |
| Ferulic acid (mg/L) | 0.2 |
| p-Coumaric acid (mg/L) | 0.2 |
| p-Coumaroyl tartaric acid(mg/L) | 24.2 |
| Flavanols | |
| Catechin (mg/L) | 23.7 |
| Epicatechin (mg/L) | 12.5 |
| Procyanidin dimer B1 (mg/L) | 20.0 |
| Procyanidin dimer B2 (mg/L) | 7.2 |
| Procyanidin dimer B3 (mg/L) | 14.7 |
| Procyanidin dimer B4 (mg/L) | 3.5 |
| Flavonols | |
| Quercetin (mg/L) | 0.1 |
| Quercetin 3-O-arabinoside (mg/L) | - |
| Quercetin 3-O-rutinoside (mg/L) | - |
| Other Polyphenols | |
| Tyrosol (mg/L) | 57.3 |
| Vanillin (mg/L) | 2.2 |
| Resveratrol (mg/L) | - |
| trans-Resveratrol (mg/L) | - |
| cis-Resveratrol (mg/L) | - |
| Mean ± SD or % | |
|---|---|
| Age (years) | 68.7 ± 5.4 a |
| Height (cm) | 168.9 ± 6.2 |
| Body weight (kg) | 82 ± 11.1 |
| BMI (kg/m²) | 28.7 ± 3.2 |
| BMI ≥ 25 kg/m² [n (%)] | 35 (92) a |
| Waist circumference (cm) | 105 ± 7 |
| Hypertension [n (%)] | 27 (71) |
| Type 2 diabetes mellitus [n (%)] | 8 (23) |
| Dyslipidemia [n (%)] | 20 (53) |
| Current smokers [n (%)] | 5 (13) |
| Sedentariness [n (%)] | 4 (11) |
| Family history of premature CHD [n (%)] | 4 (11) |
| Systolic blood pressure (mmHg) | 144.2 ± 16.2 |
| Diastolic blood pressure (mmHg) | 76.9 ± 9.7 |
| Heart rate (beats/min) | 65.3 ± 9.2 |
| Diuretics [n (%)] | 10 (26) |
| Statins [n (%)] | 15 (39) |
| Fibrates [n (%)] | 13 (34) |
| ACE inhibitors [n (%)] | 19 (50) |
| Oral hypoglycemic drugs [n (%)] | 14 (37) |
| Aspirin or antiplatelet drugs [n (%)] | 9 (24) |
| Others [n (%)] | 17 (45) |
| Glucose (mg/dL) | 111.3 ± 23.3 |
| Total cholesterol (mg/dL) | 170.8 ± 38.5 |
| LDL-cholesterol (mg/dL) | 103.9 ± 36.1 |
| HDL-cholesterol (mg/dL) | 44.8 ± 14.4 |
| Triglycerides (mg/dL) | 105.5 ± 54.5 |
| ALT (IU/L) | 25.5 ± 11.6 |
| AST (IU/L) | 25.3 ± 11.7 |
| GGT (IU/L) | 21.4 ± 13.8 |
| Folic acid (serum) (ng/mL) | 8.9 ± 2.9 |
| Vitamin B12 (pg/mL) | 399.5 ± 175.4 |
| Apo A1 (mg/dL) | 113.7 ± 18.9 |
| Apo B (mg/dL) | 79.3 ± 19.2 |
| Lipoprotein (a) (mg/dL) | 37.1 ± 54.1 |
| Before AWW Mean ± SD + | After AWW Mean ± SD + | Mean Differences (95% CI) ǂ | Before Gin Mean ± SD + | After Gin Mean ± SD + | Mean Differences (95% CI) ǂ | p-Value | |
|---|---|---|---|---|---|---|---|
| Physical activity (METS/week) | 6560 ± 6333 | 6686 ± 6531 | 125.94 (−733.80 to 985.70) | 5783 ± 4624 | 6477 ± 6379 | 694 (−1294to 2682) | 0.481 |
| Energy (Kcal) | 1753 ± 264 | 1965 ± 353 | 212.03 (83.95 to 340.10) * | 1730 ± 301 | 1972 ± 397 | 242.02 (−90.50 to 393.54) * | 0.003 |
| Protein (g) | 82.35 ± 15,63 | 86.07 ± 14.61 | 3.71 (−2.75 to 10.18) | 84.15 ± 16.53 | 83.61 ± 18.01 | −0.53 (−8.94 to 7.86) | 0.896 |
| Carbohydrates (g) | 187.72 ± 39.05 | 196.64 ± 50.72 | 8.92 (−6.63 to 24.48) | 187.81 ± 47.92 | 196.53 ± 54.37 | 8.71 (−14.96 to 32.39) | 0.456 |
| Dietary fiber | 17.19 ± 5.10 | 17.67 ± 6.96 | 0.48 (−1.81 to 2.78) | 17.28 ± 6.25 | 16.90 ± 7.61 | −0.38 (−3.24 to 2.47) | 0.785 |
| Total fat (g) | 78.41 ± 17.82 | 73.01 ± 16.17 | −5.41 (−12.54 to 1.72) | 76.55 ± 18.28 | 73.30 ± 18.22 | −3.25 (−11.71 to 5.20) | 0.436 |
| Cholesterol (mg) | 278.42 ± 63.70 | 281.69 ± 106.31 | 3.26 (−44.32 to 50.86) | 281.37 ± 72.40 | 272.48 ± 85.56 | −8.89 (−54.70 to 36.92) | 0.693 |
| Polyphenols (mg) | 1192 ± 374 | 1428.41 ± 641.62 | 236.30 (28.80 to 443.80) * | 1281 ± 588 | 1294 ± 608 | 12.99 (−282.69 to 308.68) | 0.929 |
| Alcohol (g) | 0.00 ± 0.00 | 26.17 ± 0.32 | 26.17 ( 26.04 to 26.30) * | 0.00 ± 0.00 | 29.26 ± 1.88 | 29.26 (28.49 to 30.02) * | <0.001 |
| BIOMARKERS | BEFORE WINE Mean ± SD + | AFTER WINE Mean ± SD + | Mean differences (95%Cl) ǂ | p | BEFORE GIN Mean ± SD + | AFTER GIN Mean ± SD + | Mean differences (95% Cl) ǂ | p | p-Value |
|---|---|---|---|---|---|---|---|---|---|
| Systolic BP (mmHg) | 141.78 ± 14.94 | 136.87 ± 13.17 | −4.91 (−9.41 to −0.418) * | 0.033 | 137.43 ± 15.87 | 139.55 ± 17.51 | 2.12 (−2.31 to 6.56) | 0.338 | 0.039 |
| Diastolic BP (mmHg) | 76.34 ± 9.29 | 73.44 ± 10.50 | −2.90 (−5.50 to −0.295) * | 0.030 | 72.83 ± 11.87 | 73.44 ± 910.87 | 0.61 (−1.64 to 2.86) | 0.585 | 0.039 |
| Heart rate (lpm) | 65.15 ± 8.64 | 64.66 ± 9.69 | −0.49 (−3.52 to 2.53) | 0.743 | 65.76 ± 10.26 | 65.91 ± 9.45 | 0.15 (−3.26 to 3.57) | 0.928 | 0.538 |
| Weight (Kg) | 81.77 ± 10.94 | 82.06 ± 10.64 | 0.28 (−0.21 to 0.78) | 0.248 | 82.00 ± 10.86 | 82.29 ± 10.66 | 0.29 (−0.76 to 0.66) | 0.116 | 0.496 |
| Body mass index (Kg/m2) | 28.73 ± 3.12 | 28.84 ± 3.04 | 0.11 (−0.07 to 0.30) | 0.222 | 27.91 ± 5.15 | 28.73 ± 3.02 | 0.81 (−0.84 to 2.48) | 0.325 | 0.285 |
| Waist circumference (cm) | 103.37 ± 7.61 | 102.98 ± 8.30 | −0.38 (−1.70 to 0.92) | 0.551 | 102.79 ± 8.06 | 102.95 ± 7.39 | 0.16 (−0.56 to 0.90) | 0.648 | 0.484 |
| NOx serum (µmol/L) | 28.50 ± 12.62 | 56.37 ± 62.98 | 27.86 (−6.86 to 62.59) | 0.013 | 27.48 ± 16.79 | 39.31 ± 43.97 | 11.83 (−6.63 to 6.25) | 0.272 | 0.237 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roth, I.; Casas, R.; Ribó-Coll, M.; Estruch, R. Consumption of Aged White Wine under a Veil of Flor Reduces Blood Pressure-Increasing Plasma Nitric Oxide in Men at High Cardiovascular Risk. Nutrients 2019, 11, 1266. https://doi.org/10.3390/nu11061266
Roth I, Casas R, Ribó-Coll M, Estruch R. Consumption of Aged White Wine under a Veil of Flor Reduces Blood Pressure-Increasing Plasma Nitric Oxide in Men at High Cardiovascular Risk. Nutrients. 2019; 11(6):1266. https://doi.org/10.3390/nu11061266
Chicago/Turabian StyleRoth, Irene, Rosa Casas, Margarita Ribó-Coll, and Ramón Estruch. 2019. "Consumption of Aged White Wine under a Veil of Flor Reduces Blood Pressure-Increasing Plasma Nitric Oxide in Men at High Cardiovascular Risk" Nutrients 11, no. 6: 1266. https://doi.org/10.3390/nu11061266
APA StyleRoth, I., Casas, R., Ribó-Coll, M., & Estruch, R. (2019). Consumption of Aged White Wine under a Veil of Flor Reduces Blood Pressure-Increasing Plasma Nitric Oxide in Men at High Cardiovascular Risk. Nutrients, 11(6), 1266. https://doi.org/10.3390/nu11061266