Timing of Food Introduction and the Risk of Food Allergy

Abstract
1. Introduction
2. Breast Milk and Cow’s Milk Protein
2.1. Exclusive Breast-Feeding Regardless the Risk of FA
2.2. Cow’s Milk Proteins Introduction Regardless the Risk of FA
2.3. High-Risk Infants
3. Hen’s Egg
4. Peanuts
5. Soy
6. Wheat and Fish
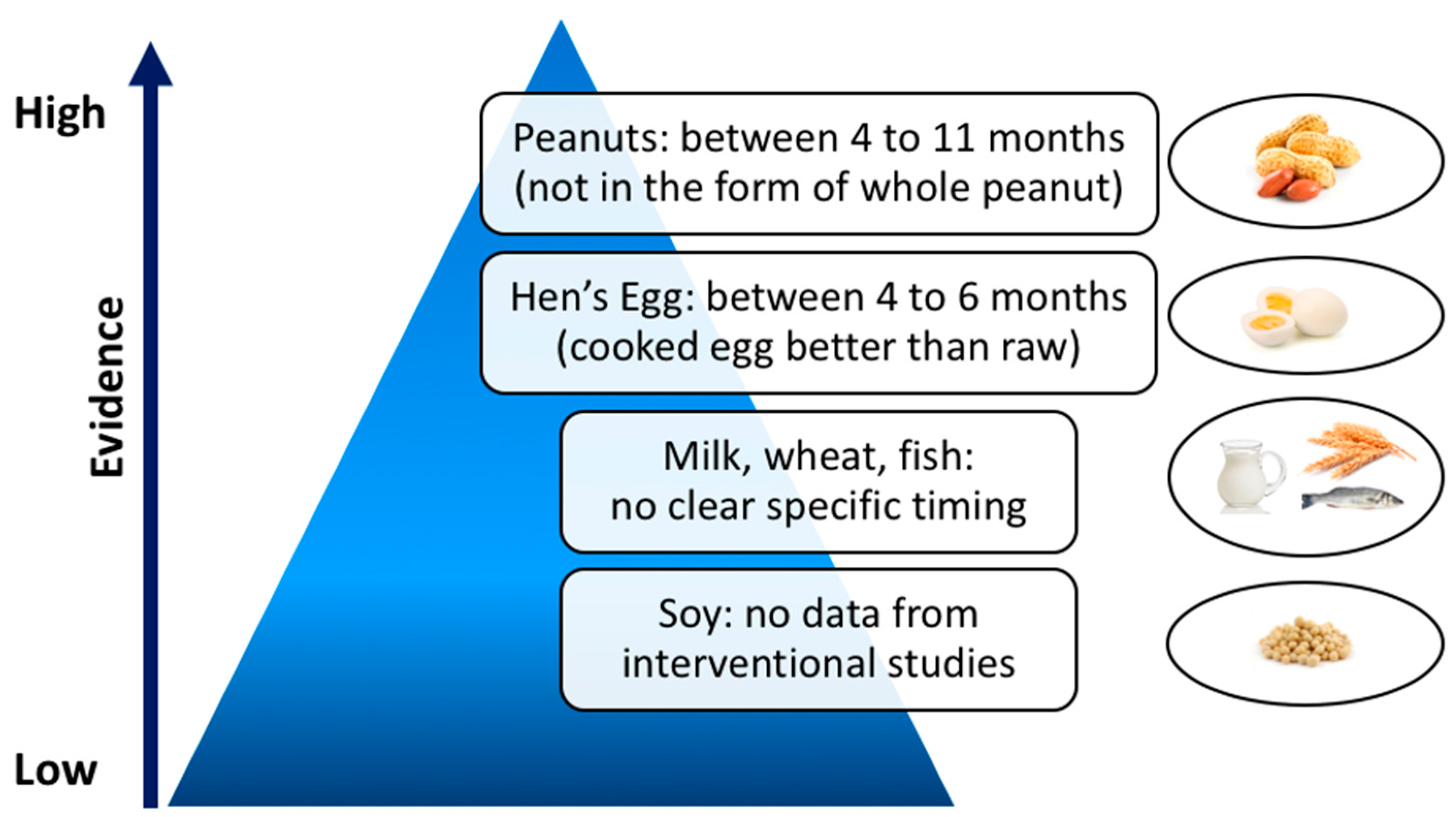
7. Recommendations
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Prescott, S.L.; Pawankar, R.; Allen, K.J.; Campbell, D.E.; Sinn, J.K.; Fiocchi, A.; Ebisawa, M.; Sampson, H.A.; Beyer, K.; Lee, B.-W. A global survey of changing patterns of food allergy burden in children. World Allergy Organ. J. 2013, 6, 21. [Google Scholar] [CrossRef]
- Winberg, A.; West, C.E.; Strinnholm, Å.; Nordström, L.; Hedman, L.; Rönmark, E. Assessment of Allergy to Milk, Egg, Cod, and Wheat in Swedish Schoolchildren: A Population Based Cohort Study. PLoS ONE 2015, 10, e0131804. [Google Scholar] [CrossRef] [PubMed]
- Nwaru, B.I.; Hickstein, L.; Panesar, S.S.; Roberts, G.; Muraro, A.; Sheikh, A.; on behalf of the EAACI Food Allergy and Anaphylaxis Guidelines Group. Prevalence of common food allergies in Europe: A systematic review and meta-analysis. Allergy 2014, 69, 992–1007. [Google Scholar] [CrossRef]
- Rona, R.J.; Keil, T.; Summers, C.; Gislason, D.; Zuidmeer, L.; Sodergren, E.; Sigurdardottir, S.T.; Lindner, T.; Goldhahn, K.; Dahlstrom, J.; et al. The prevalence of food allergy: A meta-analysis. J. Allergy Clin. Immunol. 2007, 120, 638–646. [Google Scholar] [CrossRef]
- Allen, K.J.; Koplin, J.J. The epidemiology of IgE-mediated food allergy and anaphylaxis. Immunol. Allergy Clin. N. Am. 2012, 32, 35–50. [Google Scholar] [CrossRef] [PubMed]
- Prescott, S.L.; Tang, M.L.K.; Australasian Society of Clinical Immunology and Allergy. The Australasian Society of Clinical Immunology and Allergy position statement: Summary of allergy prevention in children. Med. J. Aust. 2005, 182, 464–467. [Google Scholar]
- American Academy of Pediatrics. Committee on Nutrition. Hypoallergenic infant formulas. Pediatrics 2000, 106 (Pt 1), 346–349. [Google Scholar]
- Høst, A.; Koletzko, B.; Dreborg, S.; Muraro, A.; Wahn, U.; Aggett, P.; Bresson, J.L.; Hernell, O.; Lafeber, H.; Michaelsen, K.F.; et al. Dietary products used in infants for treatment and prevention of food allergy. Joint Statement of the European Society for Paediatric Allergology and Clinical Immunology (ESPACI) Committee on Hypoallergenic Formulas and the European Society for Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) Committee on Nutrition. Arch. Dis Child. 1999, 81, 80–84. [Google Scholar]
- Kleinman, R.E. Pediatric Nutrition Handbook, 5th ed.; American Academy of Pediatrics Commitee on Nutrition: Elk Grove Village, IL, USA, 2004; pp. 593–607. [Google Scholar]
- Fiocchi, A.; Assa’ad, A.; Bahna, S. Adverse Reactions to Foods Committee, American College of Allergy, Asthma and Immunology. Food allergy and the introduction of solid foods to infants: A consensus document. Adverse Reactions to Foods Committee, American College of Allergy, Asthma and Immunology. Ann. Allergy Asthma Immunol. Off. Publ. Am. Coll. Allergy Asthma Immunol. 2006, 97, 10–20; quiz 21, 77. [Google Scholar]
- Muraro, A.; Dreborg, S.; Halken, S.; Høst, A.; Niggemann, B.; Aalberse, R.; Arshad, S.H.; Berg, A.V.; Carlsen, K.H.; Duschén, K.; et al. Dietary prevention of allergic diseases in infants and small children. Part III: Critical review of published peer-reviewed observational and interventional studies and final recommendations. Pediatr. Allergy Immunol. Off. Publ. Eur. Soc. Pediatr. Allergy Immunol. 2004, 15, 291–307. [Google Scholar] [CrossRef]
- Bailey, M.; Haverson, K.; Inman, C.; Harris, C.; Jones, P.; Corfield, G.; Miller, B.; Stokes, C. The development of the mucosal immune system pre- and post-weaning: Balancing regulatory and effector function. Proc. Nutr. Soc. 2005, 64, 451–457. [Google Scholar] [CrossRef]
- Prescott, S.L.; Smith, P.; Tang, M.; Palmer, D.J.; Sinn, J.; Huntley, S.J.; Cormack, B.; Heine, R.G.; Gibson, R.A.; Makrides, M. The importance of early complementary feeding in the development of oral tolerance: Concerns and controversies. Pediatr. Allergy Immunol. Off. Publ. Eur. Soc. Pediatr. Allergy Immunol. 2008, 19, 375–380. [Google Scholar] [CrossRef]
- Tariq, S.M.; Stevens, M.; Matthews, S.; Ridout, S.; Twiselton, R.; Hide, D.W. Cohort study of peanut and tree nut sensitisation by age of 4 years. BMJ 1996, 313, 514–517. [Google Scholar] [CrossRef]
- Lack, G.; Fox, D.; Northstone, K.; Golding, J.; Avon Longitudinal Study of Parents and Children Study Team. Factors associated with the development of peanut allergy in childhood. N. Engl. J. Med. 2003, 348, 977–985. [Google Scholar] [CrossRef] [PubMed]
- Fox, A.T.; Sasieni, P.; du Toit, G.; Syed, H.; Lack, G. Household peanut consumption as a risk factor for the development of peanut allergy. J. Allergy Clin. Immunol. 2009, 123, 417–423. [Google Scholar] [CrossRef]
- Arshad, S.H.; Bateman, B.; Sadeghnejad, A.; Gant, C.; Matthews, S.M. Prevention of allergic disease during childhood by allergen avoidance: The Isle of Wight prevention study. J. Allergy Clin. Immunol. 2007, 119, 307–313. [Google Scholar] [CrossRef] [PubMed]
- Chan-Yeung, M.; Ferguson, A.; Watson, W.; Dimich-Ward, H.; Rousseau, R.; Lilley, M.; Dybuncio, A.; Becker, A. The Canadian Childhood Asthma Primary Prevention Study: Outcomes at 7 years of age. J. Allergy Clin. Immunol. 2005, 116, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Zutavern, A.; Brockow, I.; Schaaf, B.; von Berg, A.; Diez, U.; Borte, M.; Kraemer, U.; Herbath, O.; Behrendt, H.; Wichmann, H.E.; et al. Timing of solid food introduction in relation to eczema, asthma, allergic rhinitis, and food and inhalant sensitization at the age of 6 years: Results from the prospective birth cohort study LISA. Pediatrics 2008, 121, e44–e52. [Google Scholar] [CrossRef] [PubMed]
- Du Toit, G.; Katz, Y.; Sasieni, P.; Mesher, D.; Maleki, S.J.; Fisher, H.R.; Fox, A.T.; Turcanu, V.; Amir, T.; Zadik-Mnuhin, G.; et al. Early consumption of peanuts in infancy is associated with a low prevalence of peanut allergy. J. Allergy Clin. Immunol. 2008, 122, 984–991. [Google Scholar] [CrossRef]
- Sausenthaler, S.; Heinrich, J.; Koletzko, S.; GINIplus and LISAplus Study Groups. Early diet and the risk of allergy: What can we learn from the prospective birth cohort studies GINIplus and LISAplus? Am. J. Clin. Nutr. 2011, 94 (Suppl. 6), 2012S–2017S. [Google Scholar]
- WHO. Breastfeeding. Available online: http://www.who.int/nutrition/topics/exclusive_breastfeeding/en/ (accessed on 18 February 2019).
- Greer, F.R.; Sicherer, S.H.; Burks, A.W.; American Academy of Pediatrics Committee on Nutrition, American Academy of Pediatrics Section on Allergy and Immunology. Effects of early nutritional interventions on the development of atopic disease in infants and children: The role of maternal dietary restriction, breastfeeding, timing of introduction of complementary foods, and hydrolyzed formulas. Pediatrics 2008, 121, 183–191. [Google Scholar] [CrossRef]
- Greer, F.R.; Sicherer, S.H.; Burks, A.W.; Committee on Nutrition, Section on Allergy and Immunology. The Effects of Early Nutritional Interventions on the Development of Atopic Disease in Infants and Children: The Role of Maternal Dietary Restriction, Breastfeeding, Hydrolyzed Formulas, and Timing of Introduction of Allergenic Complementary Foods. Pediatrics 2019, 143, e20190281. [Google Scholar] [CrossRef]
- Muraro, A.; Halken, S.; Arshad, S.H.; Beyer, K.; Dubois, A.E.J.; Du Toit, G.; Eigenmann, P.A.; Grimshaw, K.E.; Hoest, A.; Lack, G.; et al. EAACI food allergy and anaphylaxis guidelines. Primary prevention of food allergy. Allergy 2014, 69, 590–601. [Google Scholar] [CrossRef]
- Fewtrell, M.; Bronsky, J.; Campoy, C.; Domellöf, M.; Embleton, N.; Fidler Mis, N.; Hojsak, I.; Hulst, J.M.; Indrio, F.; Lapillonne, A.; et al. Complementary Feeding: A Position Paper by the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 119–132. [Google Scholar] [CrossRef]
- Scientific Opinion on the appropriate age for introduction of complementary feeding of infants. EFSA J. 2009, 7, 1423. [CrossRef]
- Nwaru, B.I.; Hickstein, L.; Panesar, S.S.; Muraro, A.; Werfel, T.; Cardona, V.; Dubois, A.E.J.; Halken, S.; Hoffmann-Sommergruber, K.; Poulsen, L.K.; et al. The epidemiology of food allergy in Europe: A systematic review and meta-analysis. Allergy 2014, 69, 62–75. [Google Scholar] [CrossRef]
- Grimshaw, K.E.C.; Maskell, J.; Oliver, E.M.; Morris, R.C.G.; Foote, K.D.; Mills, E.N.C.; Roberts, G.; Margetts, B.M. Introduction of complementary foods and the relationship to food allergy. Pediatrics 2013, 132, e1529–e1538. [Google Scholar] [CrossRef]
- Burgess, J.A.; Dharmage, S.C.; Allen, K.; Koplin, J.; Garcia-Larsen, V.; Boyle, R.; Waidyatillake, N.; Lodge, C.J. Age at introduction to complementary solid food and food allergy and sensitization: A systematic review and meta-analysis. Clin. Exp. Allergy J. Br. Soc. Allergy Clin. Immunol. 2019. [Google Scholar] [CrossRef]
- Eidelman, A.I. Breastfeeding and the use of human milk: An analysis of the American Academy of Pediatrics 2012 Breastfeeding Policy Statement. Breastfeed. Med. Off. J. Acad. Breastfeed. Med. 2012, 7, 323–324. [Google Scholar] [CrossRef]
- World Health Organization (WHO). 55th World Health Assembly. Infant and Young Child Nutrition. (WHA55.25). 2002. Available online: https://www.who.int/nutrition/topics/WHA55.25_iycn_en.pdf?ua=1 (accessed on 21 March 2019).
- Mihatsch, W.A.; Braegger, C.; Bronsky, J.; Campoy, C.; Domellöf, M.; Fewtrell, M.; Mis, N.F.; Hojsak, I.; Hulst, J.; Indrio, F.; et al. Prevention of Vitamin K Deficiency Bleeding in Newborn Infants: A Position Paper by the ESPGHAN Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2016, 63, 123–129. [Google Scholar] [CrossRef]
- Braegger, C.; Campoy, C.; Colomb, V.; Decsi, T.; Domellof, M.; Fewtrell, M.; Hojsak, I.; Mihatsch, W.; Molgaard, C.; Shamir, R.; et al. Vitamin D in the healthy European paediatric population. J. Pediatr. Gastroenterol. Nutr. 2013, 56, 692–701. [Google Scholar] [CrossRef]
- Kramer, M.S.; Kakuma, R. Optimal duration of exclusive breastfeeding. Cochrane Database Syst. Rev. 2012, CD003517. [Google Scholar] [CrossRef]
- Dewey, K.G.; Cohen, R.J.; Rivera, L.L.; Brown, K.H. Effects of age of introduction of complementary foods on iron status of breast-fed infants in Honduras. Am. J. Clin. Nutr. 1998, 67, 878–884. [Google Scholar] [CrossRef]
- Jonsdottir, O.H.; Thorsdottir, I.; Hibberd, P.L.; Fewtrell, M.S.; Wells, J.C.; Palsson, G.I.; Lucas, A.; Gunnlaugsson, G.; Kleinman, R.E. Timing of the introduction of complementary foods in infancy: A randomized controlled trial. Pediatrics 2012, 130, 1038–1045. [Google Scholar] [CrossRef]
- Dube, K.; Schwartz, J.; Mueller, M.J.; Kalhoff, H.; Kersting, M. Iron intake and iron status in breastfed infants during the first year of life. Clin. Nutr. Edinb. Scotl. 2010, 29, 773–778. [Google Scholar] [CrossRef]
- Dube, K.; Schwartz, J.; Mueller, M.J.; Kalhoff, H.; Kersting, M. Complementary food with low (8%) or high (12%) meat content as source of dietary iron: A double-blinded randomized controlled trial. Eur. J. Nutr. 2010, 49, 11–18. [Google Scholar] [CrossRef]
- Chantry, C.J.; Howard, C.R.; Auinger, P. Full breastfeeding duration and risk for iron deficiency in U.S. infants. Breastfeed. Med. Off. J. Acad. Breastfeed. Med. 2007, 2, 63–73. [Google Scholar] [CrossRef]
- Agostoni, C.; Decsi, T.; Fewtrell, M.; Goulet, O.; Kolacek, S.; Koletzko, B.; Michaelsen, K.F.; Moreno, L.; Puntis, J.; Rigo, J.; et al. Complementary feeding: A commentary by the ESPGHAN Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2008, 46, 99–110. [Google Scholar] [CrossRef]
- Güngör, D.; Nadaud, P.; LaPergola, C.C.; Dreibelbis, C.; Wong, Y.P.; Terry, N.; Abrams, S.A.; Beker, L.; Jacobovits, T.; Järvinen, K.M.; et al. Infant milk-feeding practices and food allergies, allergic rhinitis, atopic dermatitis, and asthma throughout the life span: A systematic review. Am. J. Clin. Nutr. 2019, 109 (Suppl. 7), 772S–799S. [Google Scholar]
- Institute of Medicine (US) Committee on the Evaluation of the Addition of Ingredients New to Infant Formula. Comparing Infant Formulas with Human Milk. National Academies Press (US), 2004. Available online: https://www.ncbi.nlm.nih.gov/books/NBK215837/ (accessed on 6 February 2019).
- Saarinen, K.M.; Juntunen-Backman, K.; Järvenpää, A.L.; Kuitunen, P.; Lope, L.; Renlund, M.; Siivola, M.; Savilahti, E. Supplementary feeding in maternity hospitals and the risk of cow’s milk allergy: A prospective study of 6209 infants. J. Allergy Clin. Immunol. 1999, 104 (Pt 1), 457–461. [Google Scholar] [CrossRef]
- Høst, A.; Husby, S.; Osterballe, O. A prospective study of cow’s milk allergy in exclusively breast-fed infants. Incidence, pathogenetic role of early inadvertent exposure to cow’s milk formula, and characterization of bovine milk protein in human milk. Acta Paediatr. Scand. 1988, 77, 663–670. [Google Scholar]
- Katz, Y.; Rajuan, N.; Goldberg, M.R.; Eisenberg, E.; Heyman, E.; Cohen, A.; Leshno, M. Early exposure to cow’s milk protein is protective against IgE-mediated cow’s milk protein allergy. J. Allergy Clin. Immunol. 2010, 126, 77–82.e1. [Google Scholar] [CrossRef] [PubMed]
- Alvisi, P.; Brusa, S.; Alboresi, S.; Amarri, S.; Bottau, P.; Cavagni, G.; Corradini, B.; Landi, L.; Loroni, L.; Marani, M.; et al. Recommendations on complementary feeding for healthy, full-term infants. Ital. J. Pediatr. 2015, 41, 36. [Google Scholar] [CrossRef]
- Koletzko, B.; von Kries, R.; Closa, R.; Monasterolo, R.C.; Escribano, J.; Subías, J.E.; Scaglioni, S.; Giovannini, M.; Beyer, J.; Demmelmair, H.; et al. Can infant feeding choices modulate later obesity risk? Am. J. Clin. Nutr. 2009, 89, 1502S–1508S. [Google Scholar] [CrossRef] [PubMed]
- Van Odijk, J.; Kull, I.; Borres, M.P.; Brandtzaeg, P.; Edberg, U.; Hanson, L.A.; Høst, A.; Kuitunen, M.; Olsen, S.F.; Skerfving, S.; et al. Breastfeeding and allergic disease: A multidisciplinary review of the literature (1966–2001) on the mode of early feeding in infancy and its impact on later atopic manifestations. Allergy 2003, 58, 833–843. [Google Scholar] [CrossRef]
- Boyle, R.J.; Ierodiakonou, D.; Khan, T.; Chivinge, J.; Robinson, Z.; Geoghegan, N.; Jarrold, K.; Afxentiou, T.; Reeves, T.; Cunha, S.; et al. Hydrolysed formula and risk of allergic or autoimmune disease: Systematic review and meta-analysis. BMJ 2016, 352, i974. [Google Scholar] [CrossRef]
- Onizawa, Y.; Noguchi, E.; Okada, M.; Sumazaki, R.; Hayashi, D. The Association of the Delayed Introduction of Cow’s Milk with IgE-Mediated Cow’s Milk Allergies. J. Allergy Clin. Immunol. Pract. 2016, 4, 481–488.e2. [Google Scholar] [CrossRef]
- Sicherer, S.H.; Sampson, H.A. Food allergy: A review and update on epidemiology, pathogenesis, diagnosis, prevention, and management. J. Allergy Clin. Immunol. 2018, 141, 41–58. [Google Scholar] [CrossRef]
- Osborn, D.A.; Sinn, J.K.; Jones, L.J. Infant formulas containing hydrolysed protein for prevention of allergic disease. Cochrane Database Syst. Rev. 2018, 10, CD003664. [Google Scholar] [CrossRef]
- Koplin, J.J.; Osborne, N.J.; Wake, M.; Martin, P.E.; Gurrin, L.C.; Robinson, M.N.; Tey, D.; Slaa, M.; Thiele, L.; Miles, L.; et al. Can early introduction of egg prevent egg allergy in infants? A population-based study. J. Allergy Clin. Immunol. 2010, 126, 807–813. [Google Scholar] [CrossRef] [PubMed]
- Bellach, J.; Schwarz, V.; Ahrens, B.; Trendelenburg, V.; Aksünger, Ö.; Kalb, B.; Niggemann, B.; Keil, T.; Beyer, K. Randomized placebo-controlled trial of hen’s egg consumption for primary prevention in infants. J. Allergy Clin. Immunol. 2017, 139, 1591–1599.e2. [Google Scholar] [CrossRef]
- Natsume, O.; Kabashima, S.; Nakazato, J.; Yamamoto-Hanada, K.; Narita, M.; Kondo, M.; Saito, M.; Kishino, A.; Takimoto, T.; Inoue, E.; et al. Two-step egg introduction for prevention of egg allergy in high-risk infants with eczema (PETIT): A randomised, double-blind, placebo-controlled trial. Lancet Lond. Engl. 2017, 389, 276–286. [Google Scholar] [CrossRef]
- Palmer, D.J.; Metcalfe, J.; Makrides, M.; Gold, M.S.; Quinn, P.; West, C.E.; Loh, R.; Prescott, S.L. Early regular egg exposure in infants with eczema: A randomized controlled trial. J. Allergy Clin. Immunol. 2013, 132, 387–392.e1. [Google Scholar] [CrossRef]
- Perkin, M.R.; Logan, K.; Tseng, A.; Raji, B.; Ayis, S.; Peacock, J.; Brough, H.; Marrs, T.; Radulovic, S.; Craven, J.; et al. Randomized Trial of Introduction of Allergenic Foods in Breast-Fed Infants. N. Engl. J. Med. 2016, 374, 1733–1743. [Google Scholar] [CrossRef]
- Wei-Liang Tan, J.; Valerio, C.; Barnes, E.H.; Turner, P.J.; Van Asperen, P.A.; Kakakios, A.M.; Campbell, D.E.; Beating Egg Allergy Trial (BEAT) Study Group. A randomized trial of egg introduction from 4 months of age in infants at risk for egg allergy. J. Allergy Clin. Immunol. 2017, 139, 1621–1628.e8. [Google Scholar] [CrossRef]
- Ierodiakonou, D.; Garcia-Larsen, V.; Logan, A.; Groome, A.; Cunha, S.; Chivinge, J.; Robinson, Z.; Geoghegan, N.; Jarrold, K.; Reeves, T.; et al. Timing of Allergenic Food Introduction to the Infant Diet and Risk of Allergic or Autoimmune Disease: A Systematic Review and Meta-analysis. JAMA 2016, 316, 1181–1192. [Google Scholar] [CrossRef]
- Bird, J.A.; Parrish, C.; Patel, K.; Shih, J.A.; Vickery, B.P. Prevention of food allergy: Beyond peanut. J. Allergy Clin. Immunol. 2019, 143, 545–547. [Google Scholar] [CrossRef]
- Palmer, D.J.; Sullivan, T.R.; Gold, M.S.; Prescott, S.L.; Makrides, M. Randomized controlled trial of early regular egg intake to prevent egg allergy. J. Allergy Clin. Immunol. 2017, 139, 1600–1607.e2. [Google Scholar] [CrossRef]
- Du Toit, G.; Roberts, G.; Sayre, P.H.; Bahnson, H.T.; Radulovic, S.; Santos, A.F.; Brough, H.A.; Phippard, D.; Basting, M.; Feeney, M.; et al. Randomized trial of peanut consumption in infants at risk for peanut allergy. N. Engl. J. Med. 2015, 372, 803–813. [Google Scholar] [CrossRef]
- Du Toit, G.; Sayre, P.H.; Roberts, G.; Lawson, K.; Sever, M.L.; Bahnson, H.T.; Fisher, H.R.; Feeney, M.; Radulovic, S.; Basting, M.; et al. Allergen specificity of early peanut consumption and effect on development of allergic disease in the Learning Early about Peanut Allergy study cohort. J. Allergy Clin. Immunol. 2018, 141, 1343–1353. [Google Scholar] [CrossRef]
- Du Toit, G.; Sayre, P.H.; Roberts, G.; Sever, M.L.; Lawson, K.; Bahnson, H.T.; Brough, H.A.; Santos, A.F.; Harris, K.M.; Radulovic, S.; et al. Effect of Avoidance on Peanut Allergy after Early Peanut Consumption. N. Engl. J. Med. 2016, 374, 1435–1443. [Google Scholar] [CrossRef]
- Fleischer, D.M.; Sicherer, S.; Greenhawt, M.; Campbell, D.; Chan, E.; Muraro, A.; Halken, S.; Katz, Y.; Ebisawa, M.; Eichenfield, L.; et al. Consensus communication on early peanut introduction and the prevention of peanut allergy in high-risk infants. J. Allergy Clin. Immunol. 2015, 136, 258–261. [Google Scholar] [CrossRef]
- Du Toit, G.; Sampson, H.A.; Plaut, M.; Burks, A.W.; Akdis, C.A.; Lack, G. Food allergy: Update on prevention and tolerance. J. Allergy Clin. Immunol. 2018, 141, 30–40. [Google Scholar] [CrossRef]
- Togias, A.; Cooper, S.F.; Acebal, M.L.; Assa’ad, A.; Baker, J.R.; Beck, L.A.; Block, J.; Byrd-Bredbenner, C.; Chan, E.S.; Eichenfield, L.F.; et al. Addendum guidelines for the prevention of peanut allergy in the United States: Report of the National Institute of Allergy and Infectious Diseases-sponsored expert panel. J. Allergy Clin. Immunol. 2017, 139, 29–44. [Google Scholar] [CrossRef]
- Osborn, D.A.; Sinn, J. Soy formula for prevention of allergy and food intolerance in infants. Cochrane Database Syst. Rev. 2006, CD003741. [Google Scholar] [CrossRef]
- Katz, Y.; Gutierrez-Castrellon, P.; González, M.G.; Rivas, R.; Lee, B.W.; Alarcon, P. A comprehensive review of sensitization and allergy to soy-based products. Clin. Rev. Allergy Immunol. 2014, 46, 272–281. [Google Scholar] [CrossRef]
- Vandenplas, Y. Prevention and Management of Cow’s Milk Allergy in Non-Exclusively Breastfed Infants. Nutrients 2017, 9, 731. [Google Scholar] [CrossRef]
- Nowak-Węgrzyn, A. Food protein-induced enterocolitis syndrome and allergic proctocolitis. Allergy Asthma Proc. 2015, 36, 172–184. [Google Scholar] [CrossRef]
- Nowak-Węgrzyn, A.; Jarocka-Cyrta, E.; Moschione Castro, A. Food Protein-Induced Enterocolitis Syndrome. J. Investig. Allergol. Clin. Immunol. 2017, 27, 1–18. [Google Scholar] [CrossRef]
- Koletzko, S.; Niggemann, B.; Arato, A.; Dias, J.A.; Heuschkel, R.; Husby, S.; Mearin, M.L.; Papadopoulou, A.; Ruemmele, F.M.; Staiano, A.; et al. Diagnostic approach and management of cow’s-milk protein allergy in infants and children: ESPGHAN GI Committee practical guidelines. J. Pediatr. Gastroenterol. Nutr. 2012, 55, 221–229. [Google Scholar] [CrossRef]
- Kull, I.; Bergström, A.; Lilja, G.; Pershagen, G.; Wickman, M. Fish consumption during the first year of life and development of allergic diseases during childhood. Allergy 2006, 61, 1009–1015. [Google Scholar] [CrossRef]
- Nwaru, B.I.; Erkkola, M.; Ahonen, S.; Kaila, M.; Haapala, A.-M.; Kronberg-Kippilä, C.; Salmelin, R.; Veijola, R.; Ilonen, J.; Simell, O.; et al. Age at the introduction of solid foods during the first year and allergic sensitization at age 5 years. Pediatrics 2010, 125, 50–59. [Google Scholar] [CrossRef]
- Alm, B.; Goksör, E.; Thengilsdottir, H.; Pettersson, R.; Möllborg, P.; Norvenius, G.; Erdes, L.; Aberg, N.; Wennergren, G. Early protective and risk factors for allergic rhinitis at age 4½ yr. Pediatr. Allergy Immunol. Off. Publ. Eur. Soc. Pediatr. Allergy Immunol. 2011, 22, 398–404. [Google Scholar] [CrossRef]
- Fisher, H.R.; Keet, C.A.; Lack, G.; du Toit, G. Preventing Peanut Allergy: Where Are We Now? J. Allergy Clin. Immunol. Pract. 2019, 7, 367–373. [Google Scholar] [CrossRef]
- Abrams, E.M.; Hildebrand, K.; Blair, B.; Chan, E.S. Timing of introduction of allergenic solids for infants at high risk. Paediatr. Child Health 2019, 24, 56–57. [Google Scholar] [CrossRef]
- Lowe, A.J.; Hosking, C.S.; Bennett, C.M.; Allen, K.J.; Axelrad, C.; Carlin, J.B.; Abramson, M.J.; Dharmage, S.C.; Hill, D.J. Effect of a partially hydrolyzed whey infant formula at weaning on risk of allergic disease in high-risk children: A randomized controlled trial. J. Allergy Clin. Immunol. 2011, 128, 360–365.e4. [Google Scholar] [CrossRef]


{kind=link}
| Exclusive Breastfeeding | Complementary Food | |
|---|---|---|
| World Health Organization (WHO) [22] | For the first 6 months of life | All infants should start receiving foods in addition to breast milk from 6 months onwards |
| American Academy of Pediatrics (AAP) [23,24,31] | Exclusive breastfeeding for about 6 months, with continuation of breastfeeding for 1 year or longer as mutually desired by mother and infant | Although solid foods should not be introduced before 4 to 6 months of age, there is no current convincing evidence that delaying their introduction beyond this period has a significant protective effect on the development of atopic disease |
| European Academy of Allergy and Clinical Immunology (EAACI) [25] | Exclusive breastfeeding is recommended for the first 4–6 months of life | Introduction of complementary foods after the age of 4 months for all children irrespective of atopic heredity |
| European Society for Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) [26] | Exclusive or full breast-feeding should be promoted for at least 4 months (17 weeks, beginning of the 5th month of life). Exclusive or predominant breast-feeding for approximately 6 months is considered a desirable goal. | Complementary foods should not be introduced before 4 months but should not be delayed beyond 6 months |
| European Food Safety Authority (EFSA) [27] | Exclusive breast-feeding is nutritionally adequate up to 6 months for the majority of infants, while some infants may need complementary foods before 6 months (but not before the age of 4 months) in addition to breastfeeding to support optimal growth and development | The introduction of complementary food into the diet of healthy term infants between the age of 4 and 6 months is safe and does not pose a risk for adverse health effects |
| Author, Year, Trial Name | Country | Population | Intervention | Outcome | Results |
|---|---|---|---|---|---|
| Bellach 2017, Hen’s Egg Allergy Prevention (HEAP) [55] | Germany (Berlin) | “Normal-risk” infants aged 4–6 months with specific IgE to egg < 0.35 kU/L | Pasteurized egg white powder (2.5 g protein) vs. rice powder 3 times/week from age 4–6 months to 12 months | Egg allergy diagnosed by oral food challenge at 1 year plus specific IgE to egg ≥ 0.35 kU/L | In egg group, 2.1% were confirmed to have egg allergies versus 0.6% in the placebo group (relative risk, 3.30; 95% CI, 0.35–31.32; P = 0.35) |
| Natsume 2017, Prevention of egg allergy with tiny amount intake trial (PETIT) [56] | Japan (Tokyo) | “High-risk” infants aged 4–5 months of age with atopic dermatitis | Heated egg powder, 50 mg/day, from 6–9 months; 250 mg/day from 9–12 months vs. placebo from 6–12 months | Egg allergy diagnosed by oral food challenge at 1 year | In the egg group 8% had an egg allergy compared with 38% in the placebo group (risk ratio 0.221; 95% CI, 0.090–0.543; p = 0.0001) |
| Palmer 2013, Solid Timing for Allergy Research (STAR) [57] | Australia (University of Western Australia) | “High-risk” singleton term infants with moderate or severe eczema (SCORAD ≥ 15) and no prior egg or solid food intake | One teaspoon pasteurized whole egg powder daily (0.9 g protein) vs. rice flour powder from age 4 months to 8 months | Egg allergy diagnosed by oral food challenge to pasteurized egg at 1 year plus positive skin prick test | In the egg group 33% were given a diagnosis of IgE-mediated egg allergy compared with 51% in the control group (relative risk, 0.65; 95% CI, 0.38–1.11; P = 0.11). |
| Palmer 2017, Starting Time for Egg Protein (STEP) [62] | Australia (University of Western Australia) | “High-risk” infants with an atopic mother, no prior egg ingestion, and no prior allergic disease | Pasteurized whole egg powder daily (0.9 g protein) vs. rice powder daily from age 4–6 mo to 10 mo | Egg allergy diagnosed by oral food challenge to pasteurized egg at 1 year plus positive skin prick test | In the egg group 7% were given a diagnosis of IgE-mediated egg allergy compared with 10.3% in the control group (adjusted relative risk, 0.75; 95% CI, 0.48–1.17; P = 0.20) |
| Perkin 2016, Enquiring about tolerance (EAT) [58] | United Kingdom (London) | “Normal-risk” singleton term infants exclusively breastfed for ≥3 months | Sequential introduction of 6 allergenic foods (4 g protein/week for each food, yogurt, peanut, boiled egg, sesame, fish, and wheat) from age 3 months, vs. avoidance to age ≥ 6 months | Egg allergy diagnosed by oral food challenge to egg at 1 and at 3 years | - intention-to-treat analysis: egg allergy 3.7% in the early-introduction group and 5.4% in the standard-introduction group, i.e., a nonsignificant 31% lower relative risk in the early-introduction group (P = 0.17) - In the per-protocol analysis: egg allergy 1.4% in the early-introduction group versus 5.5% in the standard-introduction group, representing a 75% lower relative risk (P = 0.009) |
| Tan 2017, Beating Egg Allergy (BEAT) [59] | Australia (Sydney) | “High-risk” infants with first-degree relative with allergic disease and egg skin prick test < 2mm at age 4mo | Pasteurized whole egg powder daily (350 mg egg protein) vs. rice powder daily from the time of solid food introduction to age 8 months | Egg allergy diagnosed by oral food challenge to lightly cooked whole egg at 1 year | Sensitization to egg white at 12 months was 20% and 11% in infants randomized to placebo and egg, respectively (odds ratio, 0.46; 95% CI, 0.22–0.95; P = 0.03) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferraro, V.; Zanconato, S.; Carraro, S. Timing of Food Introduction and the Risk of Food Allergy. Nutrients 2019, 11, 1131. https://doi.org/10.3390/nu11051131
Ferraro V, Zanconato S, Carraro S. Timing of Food Introduction and the Risk of Food Allergy. Nutrients. 2019; 11(5):1131. https://doi.org/10.3390/nu11051131
Chicago/Turabian StyleFerraro, Valentina, Stefania Zanconato, and Silvia Carraro. 2019. "Timing of Food Introduction and the Risk of Food Allergy" Nutrients 11, no. 5: 1131. https://doi.org/10.3390/nu11051131
APA StyleFerraro, V., Zanconato, S., & Carraro, S. (2019). Timing of Food Introduction and the Risk of Food Allergy. Nutrients, 11(5), 1131. https://doi.org/10.3390/nu11051131