Poor Bifidobacterial Colonization Is Associated with Late Provision of Colostrum and Improved with Probiotic Supplementation in Low Birth Weight Infants

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Statement
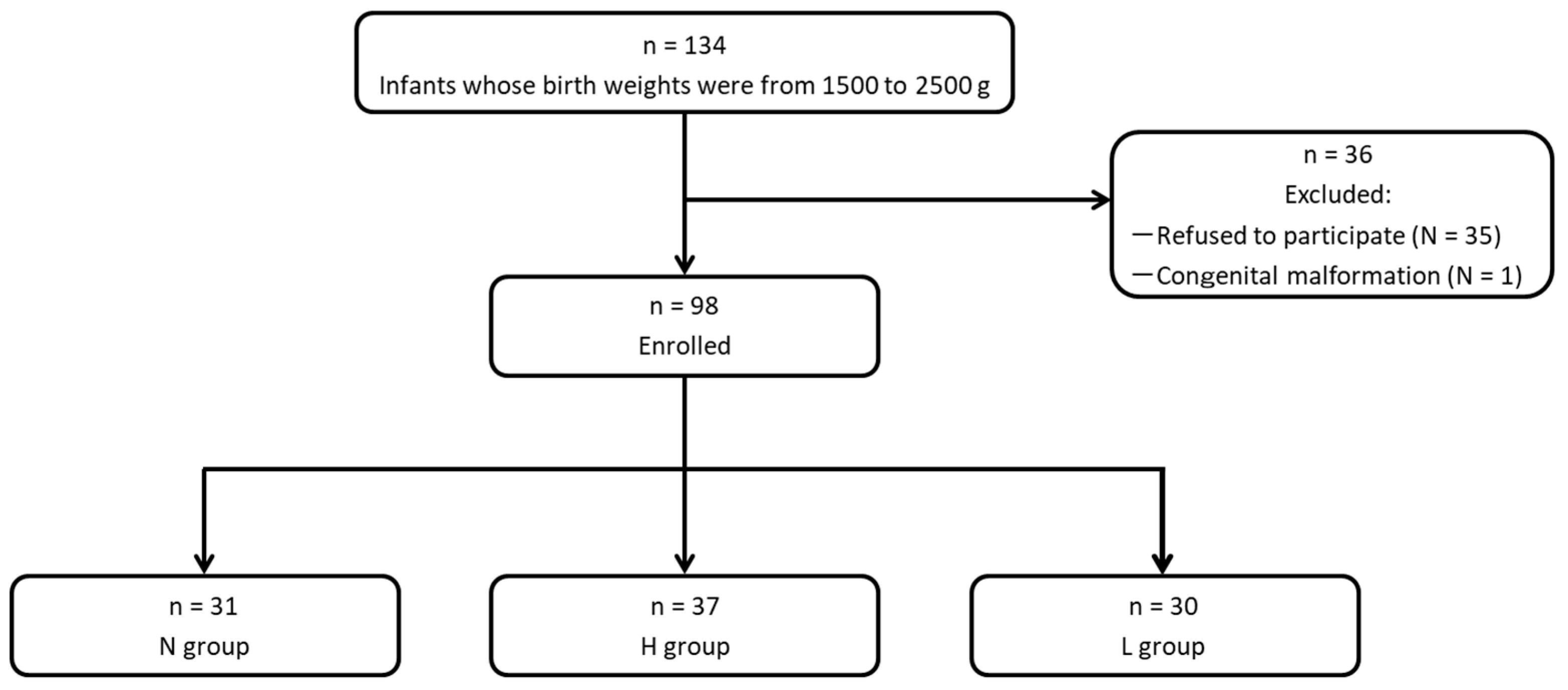
2.2. Subjects and Study Protocol
2.3. Study Intervention
2.4. Sample Collection and Bacteriological Analyses
2.5. Characteristics and Feeding Modes
2.6. Statistical Analysis
3. Results
3.1. Background Characteristics
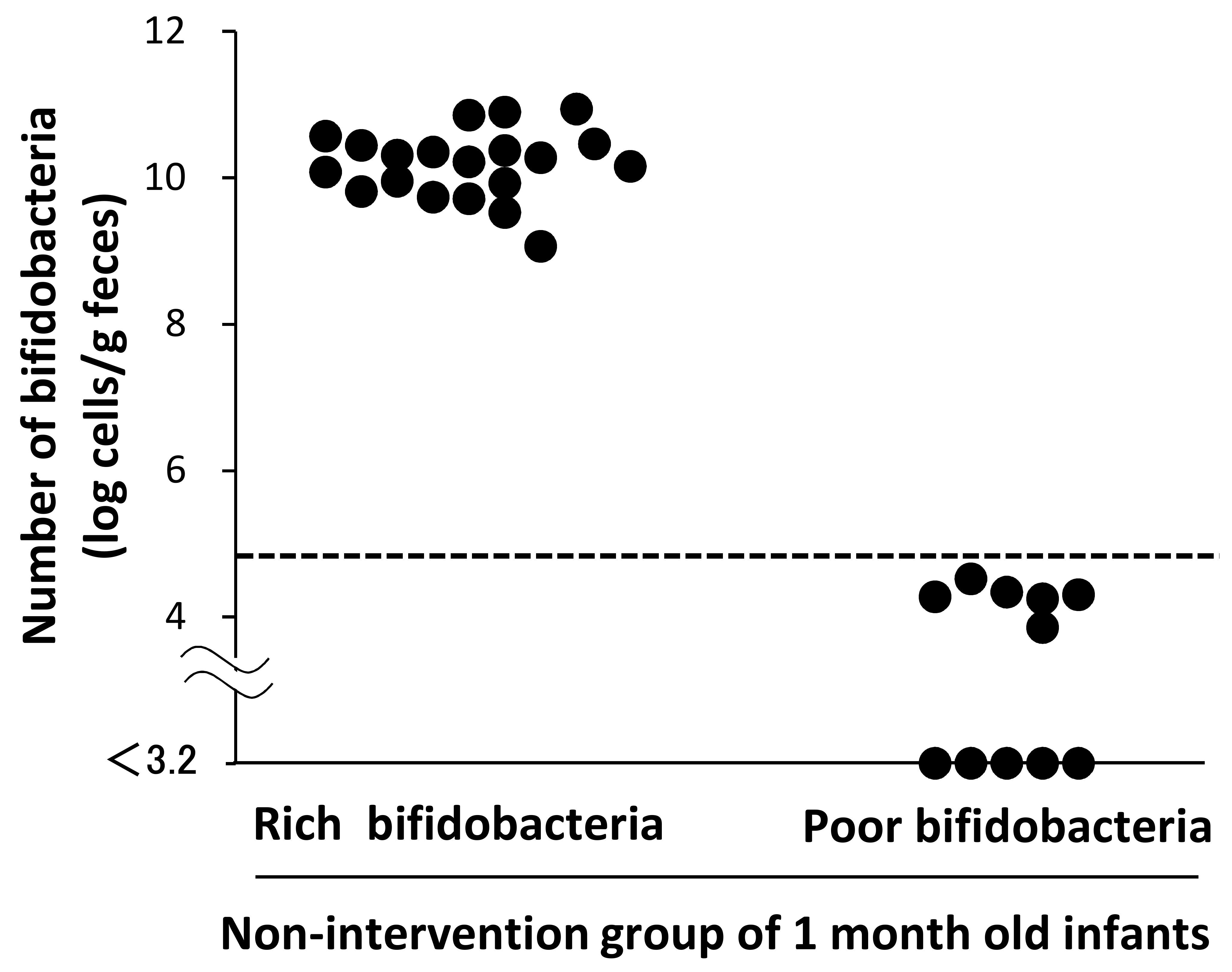
3.2. Number of Bifidobacteria in the Low Birth Weight (LBW) Infants at 1 Month of Age
3.3. Comparison of the Characteristics and Feeding History Between the Subgroups
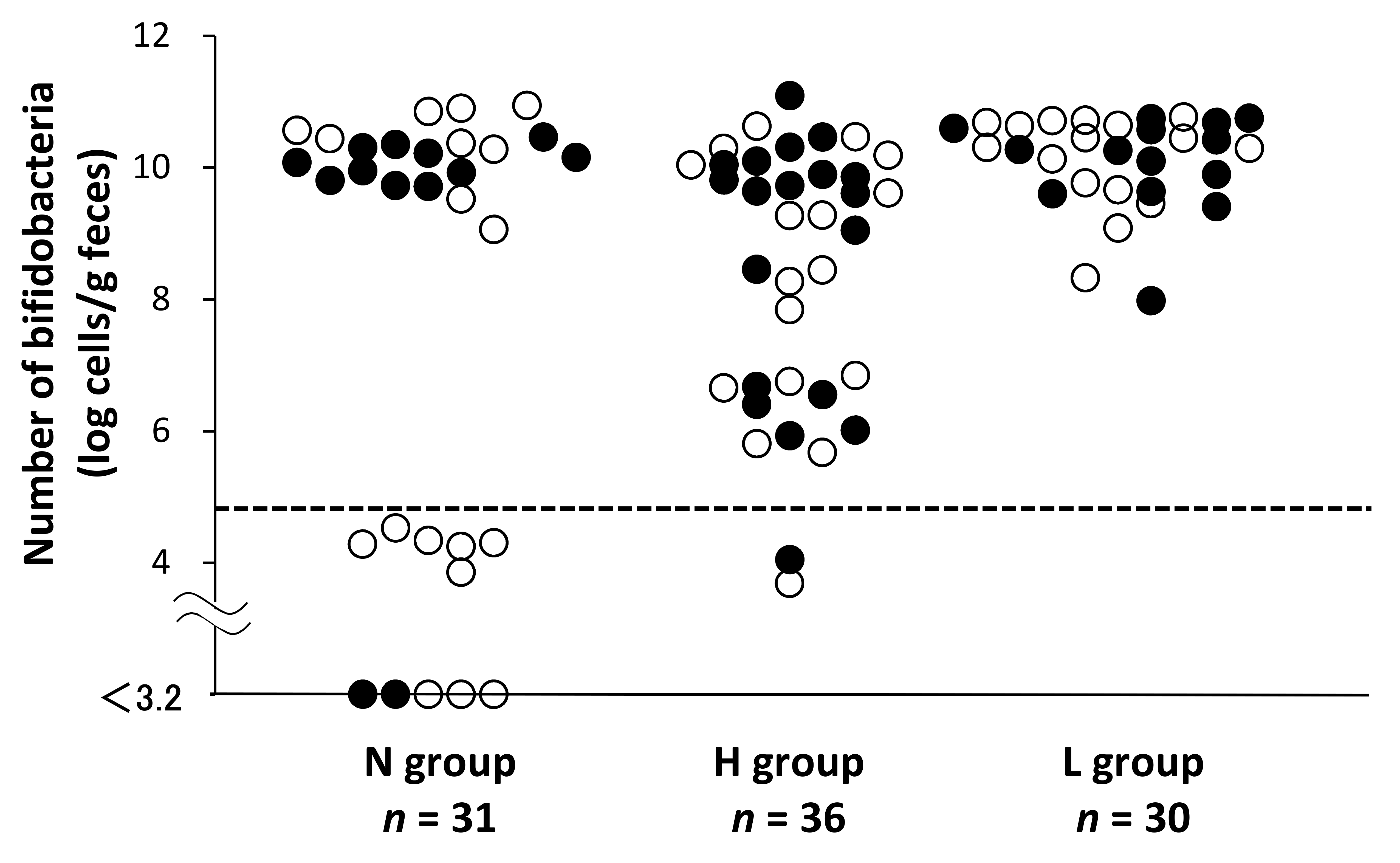
3.4. Impact of OLB6378 Administration on Fecal Bifidobacterial Counts at 1 Month of Age
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sakata, H.; Yoshioka, H.; Fujita, K. Development of the intestinal flora in very low birth weight infants compared to normal full-term newborns. Eur. J. Pediatr. 1985, 144, 186–190. [Google Scholar] [CrossRef]
- Oozeer, R.; van Limpt, K.; Ludwig, T.; Ben Amor, K.; Martin, R.; Wind, R.D.; Boehm, G.; Knol, J. Intestinal microbiology in early life: Specific prebiotics can have similar functionalities as human-milk oligosaccharides. Am. J. Clin. Nutr. 2013, 98, 561S–571S. [Google Scholar] [CrossRef] [PubMed]
- Salminen, S.; Ouwehand, A.; Benno, Y.; Lee, Y.K. Probiotics: How should they be defined? Trends Food Sci. Technol. 1999, 10, 107–110. [Google Scholar] [CrossRef]
- Collins, A.; Weitkamp, J.H.; Wynn, J.L. Why are preterm newborns at risk of infection? Arch. Dis. Child. Fetal Neonatal Ed. 2018, 103, F391–F394. [Google Scholar] [CrossRef]
- Forsgren, M.; Isolauri, E.; Salminen, S.; Rautava, S. Late preterm birth has direct and indirect effects on infant gut microbiota development during the first six months of life. Acta Paediatr. 2017, 106, 1103–1109. [Google Scholar] [CrossRef] [PubMed]
- Magne, F.; Suau, A.; Pochart, P.; Desjeux, J.F. Fecal microbial community in preterm infants. J. Pediatr. Gastroenterol. Nutr. 2005, 41, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Moles, L.; Gomez, M.; Heilig, H.; Bustos, G.; Fuentes, S.; de Vos, W.; Fernández, L.; Rodríguez, J.M.; Jiménez, E. Bacterial diversity in meconium of preterm neonates and evolution of their fecal microbiota during the first month of life. PLoS ONE 2013, 8, e66986. [Google Scholar] [CrossRef]
- Korpela, K.; Blakstad, E.W.; Moltu, S.J.; Strømmen, K.; Nakstad, B.; Rønnestad, A.E.; Brække, K.; Iversen, P.O.; Drevon, C.A.; de Vos, W. Intestinal microbiota development and gestational age in preterm neonates. Sci. Rep. 2018, 8, 2453. [Google Scholar] [CrossRef] [PubMed]
- Battersby, C.; Santhalingam, T.; Costeloe, K.; Modi, N. Incidence of neonatal necrotizing enterocolitis in high-income countries: A systematic review. Arch. Dis. Child. Fetal Neonatal Ed. 2018, 103, F182–F189. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Speer, C.P. Late-onset neonatal sepsis: Recent developments. Arch. Dis. Child. Fetal Neonatal Ed. 2015, 100, F257–F263. [Google Scholar] [CrossRef] [PubMed]
- Mai, V.; Torrazza, R.M.; Ukhanova, M.; Wang, X.; Sun, Y.; Li, N.; Shuster, J.; Sharma, R.; Hudak, M.L.; Neu, J. Distortions in development of intestinal microbiota associated with late onset sepsis in preterm infants. PLoS ONE 2013, 8, e52876. [Google Scholar] [CrossRef] [PubMed]
- Mai, V.; Young, C.M.; Ukhanova, M.; Wang, X.; Sun, Y.; Casella, G.; Theriaque, D.; Li, N.; Sharma, R.; Hudak, M.; et al. Fecal microbiota in premature infants prior to necrotizing enterocolitis. PLoS ONE 2011, 6, e20647. [Google Scholar] [CrossRef] [PubMed]
- AlFaleh, K.; Anabrees, J. Probiotics for prevention of necrotizing enterocolitis in preterm infants. Cochrane Database Syst. Rev. 2014, 10, CD005496. [Google Scholar]
- Athalve-Jape, G.; Deshpande, G.; Rao, S.; Patole, S. Benefits of probiotics on enteral nutrition in preterm neonates: A systematic review. Am. J. Clin. Nutr. 2014, 100, 1508–1519. [Google Scholar] [CrossRef]
- Lau, C.S.; Chamberlain, R.S. Probiotic administration can prevent necrotizing enterocolitis in preterm infants: A meta-analysis. J. Pediatr. Surg. 2015, 50, 1405–1412. [Google Scholar] [CrossRef]
- Rao, S.C.; Athalve-Jape, G.K.; Deshpande, G.C.; Simmer, K.N.; Patole, S.K. Probiotic supplementation and late-onset sepsis in preterm infants: A meta-analysis. Pediatrics 2016, 137, e20153684. [Google Scholar] [CrossRef]
- Totsu, S.; Yamasaki, C.; Terahara, M.; Uchiyama, A.; Kusuda, S. Probiotics Study Group in Japan. Bifidobacterium and enteral feeding in preterm infants: Cluster-randomized trial. Pediatr. Int. 2014, 56, 714–719. [Google Scholar] [CrossRef]
- Mohan, R.; Koebnick, C.; Schildt, J.; Schmidt, S.; Mueller, M.; Possner, M.; Radke, M.; Blaut, M. Effect of Bifidobacterium lactis Bb12 supplementation on intestinal microbiota of preterm infants: A double-blind, placebo-controlled, randomized study. J. Clin. Microbiol. 2006, 44, 4025–4031. [Google Scholar] [CrossRef]
- Butel, M.J.; Suau, A.; Campeotto, F.; Magne, F.; Aires, J.; Ferraris, L.; Kalach, N.; Leroux, B.; Dupont, C. Conditions of bifidobacterial colonization in preterm infants: A prospective analysis. J. Pediatr. Gastroenterol. Nutr. 2007, 44, 577–582. [Google Scholar] [CrossRef] [PubMed]
- Rouge, C.; Goldenberg, O.; Ferraris, L.; Berger, B.; Rochat, F.; Legrand, A.; Göbel, U.B.; Vodovar, M.; Voyer, M.; Rozé, J.C.; et al. Investigation of the intestinal microbiota in preterm infants using different methods. Anaerobe 2010, 16, 362–370. [Google Scholar] [CrossRef]
- Patel, K.; Konduru, K.; Patra, A.K.; Chandel, D.S.; Panigrahi, P. Trends and determinants of gastric bacterial colonization of preterm neonates in a NICU setting. PLoS ONE 2015, 10, e0114664. [Google Scholar] [CrossRef]
- Itani, T.; Ayoub Moubareck, C.; Melki, I.; Rousseau, C.; Mangin, I.; Butel, M.J.; Karam Sarkis, D. Establishment and development of the intestinal microbiota of preterm infants in a Lebanese tertiary hospital. Anaerobe 2017, 43, 4–14. [Google Scholar] [CrossRef]
- Cacho, N.T.; Lawrence, R.M. Innate immunity and breast milk. Front. Immunol. 2017, 8, 584. [Google Scholar] [CrossRef]
- Lee, J.; Kim, H.S.; Jung, Y.H.; Choi, K.Y.; Shin, S.H.; Kim, E.K.; Choi, J.H. Oropharyngeal colostrum administration in extremely premature infants: An RCT. Pediatrics 2015, 135, e357–e366. [Google Scholar] [CrossRef]
- Tanaka, K.; Tsukahara, T.; Yanagi, T.; Nakahara, S.; Furukawa, O.; Tsutsui, H.; Koshida, S. Bifidobacterium bifidum OLB6378 simultaneously enhances systemic and mucosal humoral immunity in low birth weight infants: A non-randomized study. Nutrients 2017, 9, 195. [Google Scholar] [CrossRef]
- Gengaimuthu, K. The cross contamination (cross colonization) phenomenon of probiotic use in neonatal intensive care units: Putative mechanisms and clinical and research implications. Cureus 2018, 10, e2691. [Google Scholar] [CrossRef]
- Tsukahara, T.; Inoue, R.; Nakayama, K.; Inatomi, T. Inclusion of Bacillus amyloliquefaciens strain TOA5001 in the diet of broilers suppresses the symptoms of coccidiosis by modulating intestinal microbiota. Anim. Sci. J. 2018, 89, 679–687. [Google Scholar] [CrossRef]
- Gueimonde, M.; Tolkko, S.; Korpimaki, T.; Salminen, S. New real-time quantitative PCR procedure for quantification of Bifidobacteria in human fecal samples. Appl. Environ. Microbiol. 2004, 70, 4165–4169. [Google Scholar] [CrossRef]
- Ryan, T.A. Significance tests for multiple comparison of proportions, variances, and other statistics. Psychol. Bull. 1960, 57, 318–328. [Google Scholar] [CrossRef]
- Tsuji, H.; Oozeer, R.; Matsuda, K.; Matsuki, T.; Ohta, T.; Nomoto, K.; Tanaka, R.; Kawashima, M.; Kawashima, K.; Nagata, S.; et al. Molecular monitoring of the development of intestinal microbiota in Japanese infants. Benef. Microbes 2012, 3, 113–125. [Google Scholar] [CrossRef]
- Butcher, J.; Unger, S.; Li, J.; Bando, N.; Romain, G.; Francis, J.; Mottawea, W.; Mack, D.; Stintzi, A.; O’Connor, D.L. Independent of birth mode or gestational age, very-low-birth-weight infants fed their mothers’ milk rapidly develop personalized microbiotas low in bifidobacterium. J. Nutr. 2018, 148, 326–335. [Google Scholar] [CrossRef] [PubMed]
- Fanaro, S.; Chierici, R.; Guerrini, P.; Vigi, V. Intestinal microflora in early infancy: Composition and development. Acta Paediatr. Suppl. 2003, 91, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Moosavi, S.; Sepehri, S.; Robertson, B.; Bode, L.; Goruk, S.; Field, C.J.; Lix, L.M.; de Souza, R.J.; Becker, A.B.; Mandhane, P.J.; et al. Composition and variation of the human milk microbiota are influenced by maternal and early-life factors. Cell Host Microbe 2019, 25, 324–335. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Shimizu, T.; Hosaka, A.; Kaneko, N.; Ohtsuka, Y.; Yamashiro, Y. Effects of Bifidobacterium breve supplementation on intestinal flora of low birth weight infants. Pediatr. Int. 2004, 46, 509–515. [Google Scholar] [CrossRef] [PubMed]
- Kitajima, H.; Sumida, Y.; Tanaka, R.; Yuki, N.; Takayama, H.; Fujimura, M. Early administration of Bifidobacterium breve to preterm infants: Randomised controlled trial. Arch. Dis. Child. Fetal Neonatal Ed. 1997, 76, F101–F107. [Google Scholar] [CrossRef] [PubMed]
- Latorre, E.; Layunta, E.; Grasa, L.; Castro, M.; Pardo, J.; Gomollón, F.; Alcalde, A.I.; Mesonero, J.E. Intestinal Serotonin Transporter Inhibition by Toll-Like Receptor 2 Activation. A Feedback Modulation. PLoS ONE 2016, 11, e0169303. [Google Scholar] [CrossRef] [PubMed]
- Cario, E.; Gerken, G.; Podolsky, D.K. Toll-like receptor 2 enhances ZO-1-associated intestinal epithelial barrier integrity via protein kinase C. Gastroenterology 2004, 127, 224–238. [Google Scholar] [CrossRef]
- Hörmann, N.; Brandão, I.; Jäckel, S.; Ens, N.; Lillich, M.; Walter, U.; Reinhardt, C. Gut microbial colonization orchestrates TLR2 expression, signaling and epithelial proliferation in the small intestinal mucosa. PLoS ONE 2014, 9, e113080. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Poor Bifidobacteria | Rich Bifidobacteria | ||
|---|---|---|---|
| n = 11 | n = 20 | P Value | |
| Characteristics | |||
| Gestational age, weeks a | 36.1 ± 1.9 | 35.1 ± 1.6 | 0.11 † |
| Body weight at birth, g a | 1930 ± 275 | 2081 ± 234 | 0.13 † |
| Body weight at 1 month, g a | 2481 ± 315 | 2808 ± 552 | 0.09 † |
| Apgar score at 1 min ≤ 3 b | 0 (0) | 0 (0) | 1.00 ‡ |
| Apgar score at 5 min ≥ 7 b | 11 (100) | 20 (100) | 1.00 ‡ |
| Male sex b | 4 (36) | 10 (50) | 0.36 ‡ |
| Cesarean section b | 9 (82) | 16 (80) | 0.65 ‡ |
| Multiple births b | 7 (64) | 7 (35) | 0.12 ‡ |
| Antibiotic administration during the first month b | 0 (0) | 3 (15) | 0.25 ‡ |
| Time of initiation of colostrum intake, day c,d | 4 (2–4) [n = 11] | 1 (1–2) [n = 19] | 0.04 § |
| Average of breast milk intake rate (breast milk intake/total milk intake) | |||
| during 0–7 day c | 0.08 (0.01–0.22) | 0.24 (0.13–0.33) | 0.04 § |
| during 8–14 day c,d | 0.63 (0.33–0.80) [n = 8] | 0.73 (0.63–0.88) [n = 16] | 0.27 § |
| during 15–21 day c,d | 0.56 (0.19–0.89) [n = 8] | 1.00 (0.63–1.00) [n = 12] | 0.04 § |
| during 22–28 day c,d | 0.30 (0.09–0.63) [n = 6] | 0.89 (0.47–1.00) [n = 8] | 0.052 § |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanaka, K.; Nakamura, Y.; Terahara, M.; Yanagi, T.; Nakahara, S.; Furukawa, O.; Tsutsui, H.; Inoue, R.; Tsukahara, T.; Koshida, S. Poor Bifidobacterial Colonization Is Associated with Late Provision of Colostrum and Improved with Probiotic Supplementation in Low Birth Weight Infants. Nutrients 2019, 11, 839. https://doi.org/10.3390/nu11040839
Tanaka K, Nakamura Y, Terahara M, Yanagi T, Nakahara S, Furukawa O, Tsutsui H, Inoue R, Tsukahara T, Koshida S. Poor Bifidobacterial Colonization Is Associated with Late Provision of Colostrum and Improved with Probiotic Supplementation in Low Birth Weight Infants. Nutrients. 2019; 11(4):839. https://doi.org/10.3390/nu11040839
Chicago/Turabian StyleTanaka, Katsunori, Yoshitaka Nakamura, Masaki Terahara, Takahide Yanagi, Sayuri Nakahara, Ouki Furukawa, Hidemi Tsutsui, Ryo Inoue, Takamitsu Tsukahara, and Shigeki Koshida. 2019. "Poor Bifidobacterial Colonization Is Associated with Late Provision of Colostrum and Improved with Probiotic Supplementation in Low Birth Weight Infants" Nutrients 11, no. 4: 839. https://doi.org/10.3390/nu11040839
APA StyleTanaka, K., Nakamura, Y., Terahara, M., Yanagi, T., Nakahara, S., Furukawa, O., Tsutsui, H., Inoue, R., Tsukahara, T., & Koshida, S. (2019). Poor Bifidobacterial Colonization Is Associated with Late Provision of Colostrum and Improved with Probiotic Supplementation in Low Birth Weight Infants. Nutrients, 11(4), 839. https://doi.org/10.3390/nu11040839