Different Socio-Demographic and Lifestyle Factors Can Determine the Dietary Supplement Use in Children and Adolescents in Central-Eastern Poland




Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
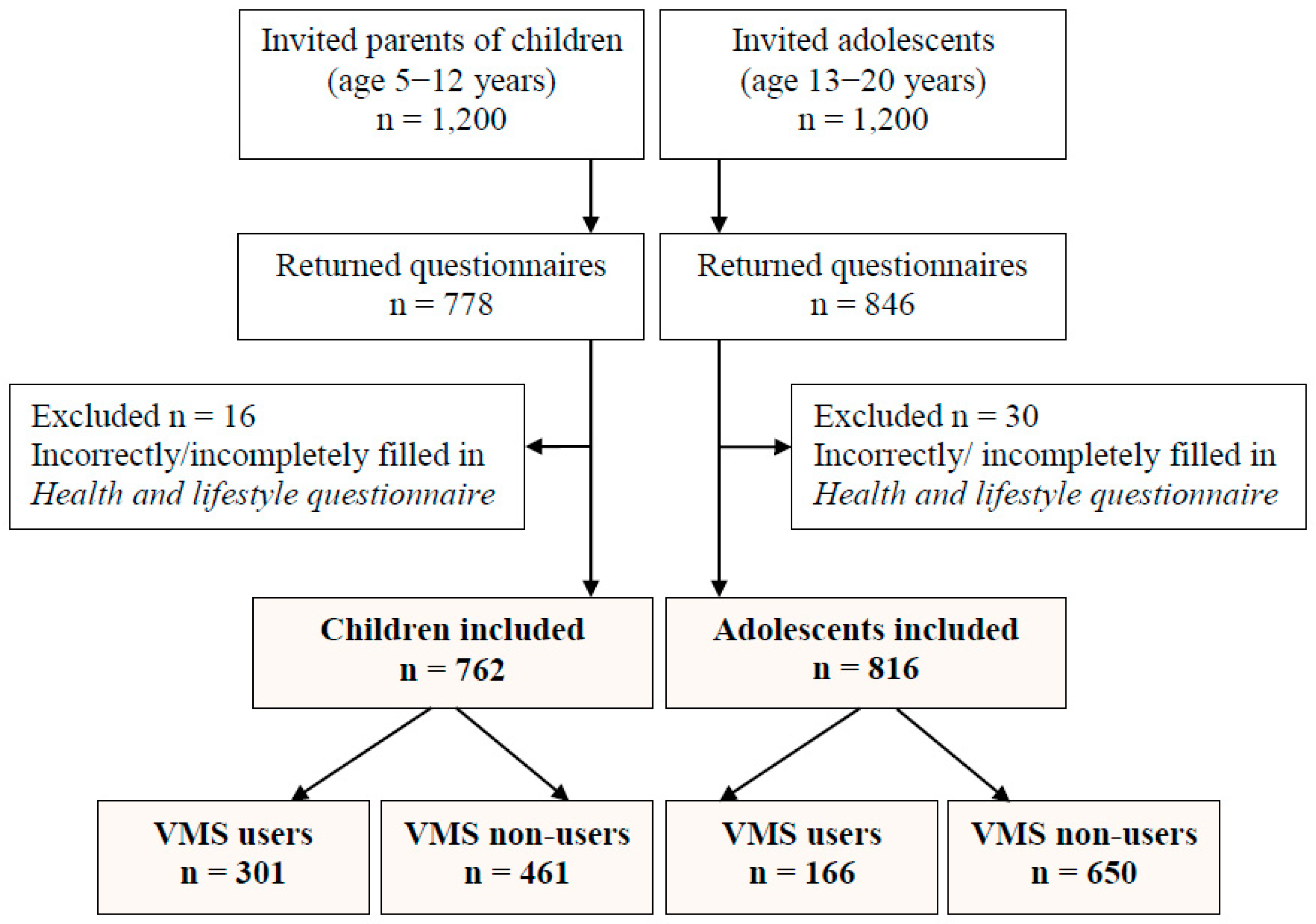
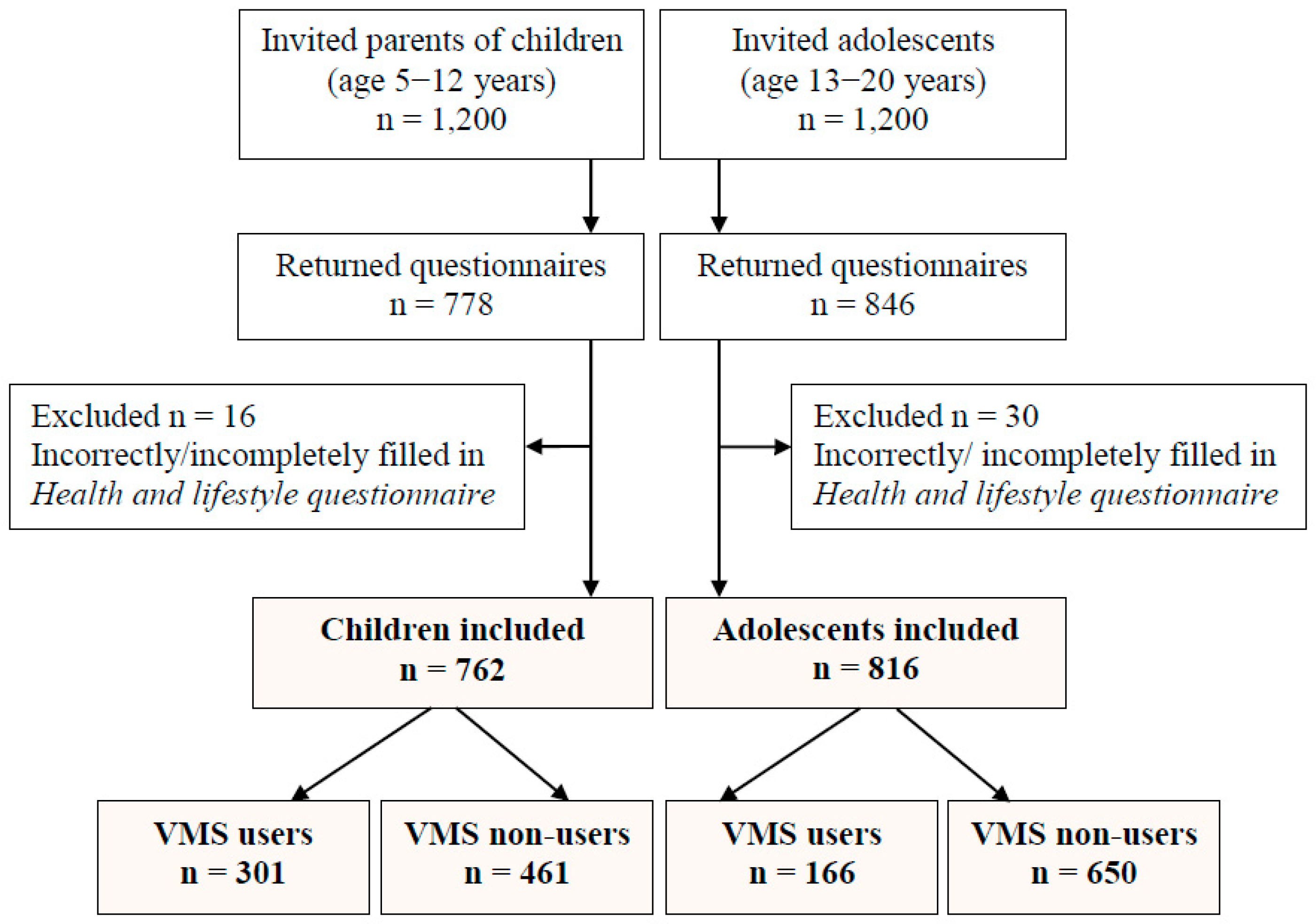
2.2. Study Population and Data Collection
2.3. Assessment of VMS Use
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. Types and Duration of VMS Use and Reason for Using/Non-Using
3.3. Determinants of VMS Use in Children and Adolescents
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bailey, R.L.; Gahche, J.J.; Lentino, C.V.; Dwyer, J.T.; Engel, J.S.; Thomas, P.R.; Betz, J.M.; Sempos, C.T.; Picciano, M.F. Dietary supplement use in the United States, 2003–2006. J. Nutr. 2011, 141, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Dwyer, J.; Nahin, R.L.; Rogers, G.T.; Barnes, P.M.; Jacques, P.M.; Sempos, C.T.; Bailey, R. Prevalence and predictors of children’s dietary supplement use: The 2007 National Health Interview Survey. Am. J. Clin. Nutr. 2013, 97, 1331–1337. [Google Scholar] [CrossRef] [PubMed]
- Skeie, G.; Braaten, T.; Hjartaker, A.; Lentjes, M.; Amiano, P.; Jakszyn, P.; Pala, V.; Palanca, A.; Niekerk, E.M.; Verhagen, H.; et al. Use of dietary supplements in the European Prospective Investigation into Cancer and Nutrition calibration study. Eur. J. Clin. Nutr. 2009, 63, S226–S238. [Google Scholar] [CrossRef] [PubMed]
- Bristow, A.; Qureshi, S.; Rona, R.J.; Chinn, S. The use of nutritional supplements by 4–12 year olds in England and Scotland. Eur. J. Clin. Nutr. 1997, 51, 366–369. [Google Scholar] [CrossRef] [PubMed]
- Mattila, V.M.; Parkkari, J.; Laakso, L.; Pihlajamaki, H.; Rimpela, A. Use of dietary supplements and anabolic-androgenic steroids among Finnish adolescents in 1991–2005. Eur. J. Public Health 2010, 20, 306–311. [Google Scholar] [CrossRef] [PubMed]
- Sterlinko Grm, H.; Stubelj Ars, M.; Besednjak-Kocijancic, L.; Golja, P. Nutritional supplement use among Slovenian adolescents. Public Health Nutr. 2012, 15, 587–593. [Google Scholar] [CrossRef]
- Fortmann, S.P.; Burda, B.U.; Senger, C.A.; Lin, J.S.; Whitlock, E.P. Vitamin and mineral supplements in the primary prevention of cardiovascular disease and cancer: An updated systematic evidence review for the U.S. Preventive Services Task Force. Ann. Intern. Med. 2013, 159, 824–834. [Google Scholar] [CrossRef] [PubMed]
- Dickinson, A.; MacKay, D. Health habits and other characteristics of dietary supplement users: A review. Nutr. J. 2014, 13, 14. [Google Scholar] [CrossRef]
- Dickinson, A.; MacKay, D.; Wong, A. Consumer attitudes about the role of multivitamins and other dietary supplements: Report of a survey. Nutr. J. 2015, 14, 66. [Google Scholar] [CrossRef]
- Yu, S.M.; Kogan, M.D.; Gergen, P. Vitamin-mineral supplement use among preschool children in the United States. Pediatrics 1997, 100, E4. [Google Scholar] [CrossRef]
- George, G.C.; Hoelscher, D.M.; Nicklas, T.A.; Kelder, S.H. Diet- and body size-related attitudes and behaviors associated with vitamin supplement use in a representative sample of fourth-grade students in Texas. J. Nutr. Educ. Behav. 2009, 41, 95–102. [Google Scholar] [CrossRef]
- George, G.C.; Springer, A.E.; Forman, M.R.; Hoelscher, D.M. Associations among dietary supplement use and dietary and activity behaviors by sex and race/ethnicity in a representative multiethnic sample of 11th-grade students in Texas. J. Am. Diet. Assoc. 2011, 111, 385–393. [Google Scholar] [CrossRef]
- Gardiner, P.; Buettner, C.; Davis, R.B.; Phillips, R.S.; Kemper, K.J. Factors and common conditions associated with adolescent dietary supplement use: An analysis of the National Health and Nutrition Examination Survey (NHANES). BMC Complement. Altern. Med. 2008, 8, 9. [Google Scholar] [CrossRef] [PubMed]
- Reaves, L.; Steffen, L.M.; Dwyer, J.T.; Webber, L.S.; Lytle, L.A.; Feldman, H.A.; Hoelscher, D.M.; Zive, M.M.; Osganian, S.K. Vitamin supplement intake is related to dietary intake and physical activity: The Child and Adolescent Trial for Cardiovascular Health (CATCH). J. Am. Diet. Assoc. 2006, 106, 2018–2023. [Google Scholar] [CrossRef]
- Picciano, M.F.; Dwyer, J.T.; Radimer, K.L.; Wilson, D.H.; Fisher, K.D.; Thomas, P.R.; Yetley, E.A.; Moshfegh, A.J.; Levy, P.S.; Nielsen, S.J.; et al. Dietary supplement use among infants, children, and adolescents in the United States, 1999–2002. Arch. Pediatr. Adolesc. Med. 2007, 161, 978–985. [Google Scholar] [CrossRef]
- Shaikh, U.; Byrd, R.S.; Auinger, P. Vitamin and mineral supplement use by children and adolescents in the 1999–2004 National Health and Nutrition Examination Survey: Relationship with nutrition, food security, physical activity, and health care access. Arch. Pediatr. Adolesc. Med. 2009, 163, 150–157. [Google Scholar] [CrossRef]
- Yoon, J.Y.; Park, H.A.; Kang, J.H.; Kim, K.W.; Hur, Y.I.; Park, J.J.; Lee, R.; Lee, H.H. Prevalence of dietary supplement use in Korean children and adolescents: Insights from Korea National Health and Nutrition Examination Survey 2007–2009. J. Korean Med. Sci. 2012, 27, 512–517. [Google Scholar] [CrossRef]
- Jun, S.; Cowan, A.E.; Tooze, J.A.; Gahche, J.J.; Dwyer, J.T.; Eicher-Miller, H.A.; Bhadra, A.; Guenther, P.M.; Potischman, N.; Dodd, K.W.; et al. Dietary Supplement Use among U.S. Children by Family Income, Food Security Level, and Nutrition Assistance Program Participation Status in 2011–2014. Nutrients 2018, 10, 1212. [Google Scholar] [CrossRef]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240–1243. [Google Scholar] [CrossRef]
- Cole, T.J.; Flegal, K.M.; Nicholls, D.; Jackson, A.A. Body mass index cut offs to define thinness in children and adolescents: International survey. BMJ 2007, 335, 194. [Google Scholar] [CrossRef]
- Sicińska, E.; Kałuża, J.; Januszko, O.; Pietruszka, B. Comparison of factors determining voluntarily fortified food consumption between children and adolescents in Central-Eastern Poland. J. Food Nutr. Res. 2018, 57, 284–294. [Google Scholar]
- Pietruszka, B.; Brzozowska, A. Homocysteine Serum Level in Relation to Intake of Folate, Vitamins B12, B1, B2, and B6 and MTHFR c.665C→T Polymorphism among Young Women. Austin J. Nutr. Food Sci. 2014, 2, 1052–1059. [Google Scholar]
- Pietruszka, B. The Effectiveness of Diet Supplementation with Folates Relative to Risk Factors for Folate Deficiencies in Young Women; Warsaw University of Life Sciences: Warsaw, Poland, 2007; pp. 1–182. [Google Scholar]
- Bylinowska, J.; Januszko, O.; Rolf, K.; Sicinska, E.; Kaluza, J.; Pietruszka, B. Factors influenced vitamin or mineral supplements use in a chosen group of children aged 6–12. Rocz. Panstw. Zakl. Hig. 2012, 63, 59–66. [Google Scholar] [PubMed]
- Bailey, R.L.; Fulgoni, V.L., 3rd; Keast, D.R.; Lentino, C.V.; Dwyer, J.T. Do dietary supplements improve micronutrient sufficiency in children and adolescents? J. Pediatr. 2012, 161, 837–842. [Google Scholar] [CrossRef] [PubMed]
- Brzozowska, A.; Kaluza, J.; Knoops, K.T.; de Groot, L.C. Supplement use and mortality: The SENECA study. Eur. J. Nutr. 2008, 47, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Kaluza, J.; Januszko, O.; Trybalska, E.; Wadolowska, L.; Slowinska, M.A.; Brzozowska, A. Vitamin and mineral supplement use and mortality among group of older people. Przegl. Epidemiol. 2010, 64, 557–563. [Google Scholar] [PubMed]
- Kleinman, R.E. Current Approaches to Standards of Care for Children: How Does the Pediatric Community Currently Approach This Issue? Nutr. Today 2002, 37, 177–179. [Google Scholar] [CrossRef] [PubMed]
- Dorsch, K.D.; Bell, A. Dietary supplement use in adolescents. Curr. Opin. Pediatr. 2005, 17, 653–657. [Google Scholar] [CrossRef]
- Bailey, R.L.; Gahche, J.J.; Thomas, P.R.; Dwyer, J.T. Why US children use dietary supplements. Pediatr. Res. 2013, 74, 737–741. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Children ≤12 years | Adolescents >12 years | |
|---|---|---|
| Parameters | ||
| Users a | Users a | |
| n = 301 % | n = 166 % | |
| Type of VMS | ||
| Single vitamin | 20.2 | 25.9 |
| Single mineral b | 4.3 | 16.9 |
| Multivitamin and/or mineral(s) | 39.9 | 33.1 |
| Vitamin(s)/mineral(s) + other ingredient b | 72.1 | 42.8 |
| Usage more than one VMS | 13.3 | 12.0 |
| Reason for using VMSs c | ||
| Improve overall health | 77.4 | 76.5 |
| Diet poor in nutrients b | 45.2 | 20.5 |
| Physician recommendation b | 32.2 | 26.5 |
| Necessary when medicines are used b | 10.6 | 4.8 |
| Other | 15.0 | 9.0 |
| Non-users | Non-users | |
| n = 461 % | n = 650 % | |
| Reason for avoidance VMSs c | ||
| No need to use because of proper nutrition b | 62.3 | 44.2 |
| Lack effect on health improvement b | 24.7 | 7.8 |
| It can be harmful b | 22.3 | 7.2 |
| Too high price b | 20.8 | 13.1 |
| Other c | 9.1 | 3.4 |
| VMS Using | n (%) * | p-value | Short-Term Users 7 days–<1 month n = 147 % ** | Medium-Term Users 1–3 months n = 214 % ** | Long-Term Users >3 months n = 106 % ** | p-value |
|---|---|---|---|---|---|---|
| Total b,c | ||||||
| children | 301 (100) | 0.012 | 29.9 | 43.9 | 26.2 | 0.048 |
| adolescents | 166 (100) | 34.3 | 49.4 | 16.3 | ||
| Vitamin A | ||||||
| children | 215 (71.4) | <0.001 | 22.3 | 48.4 | 29.3 | 0.131 |
| adolescents | 50 (30.1) | 14.0 | 64.0 | 22.0 | ||
| Vitamin E | ||||||
| children | 192 (63.8) | <0.001 | 26.0 | 47.4 | 26.6 | 0.236 |
| adolescents | 51 (30.7) | 19.6 | 60.8 | 19.6 | ||
| Vitamin D | ||||||
| children | 217 (72.1) | <0.001 | 22.6 | 47.9 | 29.5 | 0.279 |
| adolescents | 46 (27.7) | 13.0 | 58.7 | 28.3 | ||
| Vitamin C c | ||||||
| children | 252 (83.7) | <0.001 | 30.5 | 43.3 | 26.2 | 0.049 |
| adolescents | 109 (65.7) | 29.4 | 55.0 | 15.6 | ||
| Vitamin B1 a,c | ||||||
| children | 174 (57.8) | <0.001 | 24.1 | 46.0 | 29.9 | 0.010 |
| adolescents | 40 (24.1) | 12.5 | 72.5 | 15.0 | ||
| Vitamin B2 a,c | ||||||
| children | 189 (62.8) | <0.001 | 27.5 | 44.4 | 28.1 | 0.021 |
| adolescents | 41 (24.7) | 17.1 | 68.3 | 14.6 | ||
| Niacin a | ||||||
| children | 197 (65.4) | <0.001 | 25.4 | 46.7 | 27.9 | 0.041 |
| adolescents | 41 (24.7) | 14.6 | 68.3 | 17.1 | ||
| Vitamin B6 a,c | ||||||
| children | 202 (67.1) | <0.001 | 26.7 | 46.6 | 26.7 | 0.003 |
| adolescents | 55 (33.1) | 12.7 | 72.7 | 14.6 | ||
| Folic acid | ||||||
| children | 138 (45.8) | <0.001 | 19.6 | 50.0 | 30.4 | 0.064 |
| adolescents | 41 (24.7) | 12.2 | 70.7 | 17.1 | ||
| Vitamin B12 a,c | ||||||
| children | 167 (55.5) | <0.001 | 22.8 | 47.3 | 29.9 | 0.016 |
| adolescents | 40 (24.1) | 12.5 | 72.5 | 15.0 | ||
| Biotin | ||||||
| children | 127 (42.2) | <0.001 | 18.9 | 52.8 | 28.3 | 0.328 |
| adolescents | 28 (16.9) | 10.7 | 67.9 | 21.4 | ||
| Pantothenic acid | ||||||
| children | 135 (44.9) | <0.001 | 25.9 | 48.2 | 25.9 | 0.061 |
| adolescents | 39 (23.5) | 12.8 | 69.2 | 18.0 | ||
| Calcium | ||||||
| children | 76 (25.2) | 0.900 | 18.4 | 55.3 | 26.3 | 0.828 |
| adolescents | 41 (24.7) | 21.9 | 56.2 | 21.9 | ||
| Magnesium | ||||||
| children | 27 (9.0) | <0.001 | 29.6 | 48.1 | 22.3 | 0.532 |
| adolescents | 44 (26.5) | 18.2 | 56.8 | 25.0 | ||
| Iron | ||||||
| children | 35 (11.6) | 0.010 | 22.9 | 51.4 | 25.7 | 0.616 |
| adolescents | 34 (20.5) | 14.7 | 61.8 | 23.5 | ||
| Zinc a,c | ||||||
| children | 87 (28.9) | 0.210 | 23.0 | 41.4 | 35.6 | 0.015 |
| adolescents | 39 (23.5) | 12.8 | 69.2 | 18.0 |
| Study Factors | Children ≤12 years (n = 762) | Adolescents >12 years (n = 816) | ||
|---|---|---|---|---|
| Crude | Multivariate-Adjusted | Crude | Multivariate-Adjusted | |
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Age (years) | 0.96 (0.87–1.06) | 1.01 (0.90–1.14) | 0.93 (0.86–1.01) | 1.15 (0.95–1.39) |
| P for trend | 0.39 | 0.86 | 0.09 | 0.15 |
| Gender | ||||
| Female | 1.00 | 1.00 | 1.00 | 1.00 |
| Male | 0.96 (0.72–1.28) | 0.94 (0.68–1.30) | 0.75 (0.51–1.09) | 0.56 (0.37–0.87) |
| Residential area | ||||
| Urban | 1.00 | 1.00 | 1.00 | 1.00 |
| Rural | 1.04 (0.70–1.57) | 1.43 (0.88–2.35) | 0.94 (0.67–1.33) | 0.63 (0.40–0.99) |
| Mother’s education level | ||||
| Primary | 1.00 | 1.00 | 1.00 | 1.00 |
| High school | 1.87 (1.10–3.18) | 2.17 (1.17–4.01) | 2.10 (0.92–4.78) | 2.02 (0.85–4.79) |
| University | 2.05 (1.23–3.40) | 2.16 (1.14–4.07) | 6.07 (2.20–16.8) | 5.19 (1.72–15.6) |
| Socioeconomic status | ||||
| Very good or good | 1.00 | 1.00 | 1.00 | 1.00 |
| Average | 1.38 (0.99–1.91) | 1.69 (1.16–2.48) | 0.76 (0.52–1.11) | 0.75 (0.49–1.15) |
| Poor | 0.64 (0.32–1.32) | 1.12 (0.49–2.54) | 0.59 (0.33–1.04) | 0.83 (0.44–1.56) |
| Physical activity (h/week) | ||||
| <1 | 1.00 | 1.00 | 1.00 | 1.00 |
| 1–5 | 1.72 (1.26–2.36) | 1.44 (1.02–2.04) | 1.52 (1.07–2.17) | 1.26 (0.85–1.86) |
| ≥6 | 1.35 (0.76–2.41) | 1.21 (0.63–2.32) | 1.10 (0.49–2.48) | 0.87 (0.36–2.13) |
| Body Mass Index (kg/m2) | ||||
| <18.5 | 0.99 (0.64–1.52) | 1.10 (0.69–1.76) | 0.39 (0.20–0.77) | 0.35 (0.17–0.73) |
| 18.5–24.9 | 1.00 | 1.00 | 1.00 | 1.00 |
| ≥25 | 0.62 (0.44–0.88) | 0.67 (0.46–0.98) | 1.14 (0.71–1.84) | 0.99 (0.58–1.70) |
| P for trend | 0.003 | 0.008 | 0.19 | 0.22 |
| Health status | ||||
| At least good | 1.00 | 1.00 | 1.00 | 1.00 |
| Average or poor | 0.70 (0.37–1.32) | 0.56 (0.27–1.17) | 1.41 (0.89–2.24) | 1.96 (1.13–3.39) |
| Current chronic diseases | ||||
| No | 1.00 | 1.00 | 1.00 | 1.00 |
| Yes | 2.24 (1.52–3.31) | 2.32 (1.46–3.69) | 1.90 (0.99–3.68) | 1.27 (0.61–2.66) |
| Special diet | ||||
| No | 1.00 | 1.00 | 1.00 | 1.00 |
| Yes | 1.58 (0.88–2.83) | 0.82 (0.40–1.66) | 1.57 (0.96–2.58) | 1.02 (0.56–1.85) |
| Number of meals/day | ||||
| ≤3 | 1.00 | 1.00 | 1.00 | 1.00 |
| 4 | 1.38 (0.86–2.20) | 1.16 (0.69–1.96) | 1.52 (1.04–2.22) | 1.46 (0.95–2.25) |
| ≥5 | 1.82 (1.09–3.01) | 1.68 (0.96–2.95) | 1.47 (0.90–2.41) | 1.51 (0.86–2.65) |
| Fortified food consumption | ||||
| No | 1.00 | 1.00 | 1.00 | 1.00 |
| Yes | 3.39 (2.35–4.89) | 3.79 (2.54–5.63) | 3.12 (2.04–4.77) | 2.54 (1.62–4.00) |
| Diet modification | ||||
| Lack of modification | 1.00 | 1.00 | 1.00 | 1.00 |
| Excluding or including some foods | 1.76 (1.17–2.64) | 1.60 (1.01–2.53) | 2.36 (1.51–3.70) | 2.09 (1.24–3.52) |
| Simultaneously excluding and including some foods | 2.95 (1.83–4.75) | 2.22 (1.29–3.81) | 3.00 (1.85–4.87) | 3.02 (1.71–5.35) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sicińska, E.; Pietruszka, B.; Januszko, O.; Kałuża, J. Different Socio-Demographic and Lifestyle Factors Can Determine the Dietary Supplement Use in Children and Adolescents in Central-Eastern Poland. Nutrients 2019, 11, 658. https://doi.org/10.3390/nu11030658
Sicińska E, Pietruszka B, Januszko O, Kałuża J. Different Socio-Demographic and Lifestyle Factors Can Determine the Dietary Supplement Use in Children and Adolescents in Central-Eastern Poland. Nutrients. 2019; 11(3):658. https://doi.org/10.3390/nu11030658
Chicago/Turabian StyleSicińska, Ewa, Barbara Pietruszka, Olga Januszko, and Joanna Kałuża. 2019. "Different Socio-Demographic and Lifestyle Factors Can Determine the Dietary Supplement Use in Children and Adolescents in Central-Eastern Poland" Nutrients 11, no. 3: 658. https://doi.org/10.3390/nu11030658
APA StyleSicińska, E., Pietruszka, B., Januszko, O., & Kałuża, J. (2019). Different Socio-Demographic and Lifestyle Factors Can Determine the Dietary Supplement Use in Children and Adolescents in Central-Eastern Poland. Nutrients, 11(3), 658. https://doi.org/10.3390/nu11030658