Association between Soft Drink Consumption and Asthma among Qatari Adults



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Sample
2.2. Outcome Variable: Asthma and Lung Function
2.3. Exposure Variable: Soft Drink Consumption
2.4. Covariates
2.5. Data Analyses
3. Results
3.1. Sample Description
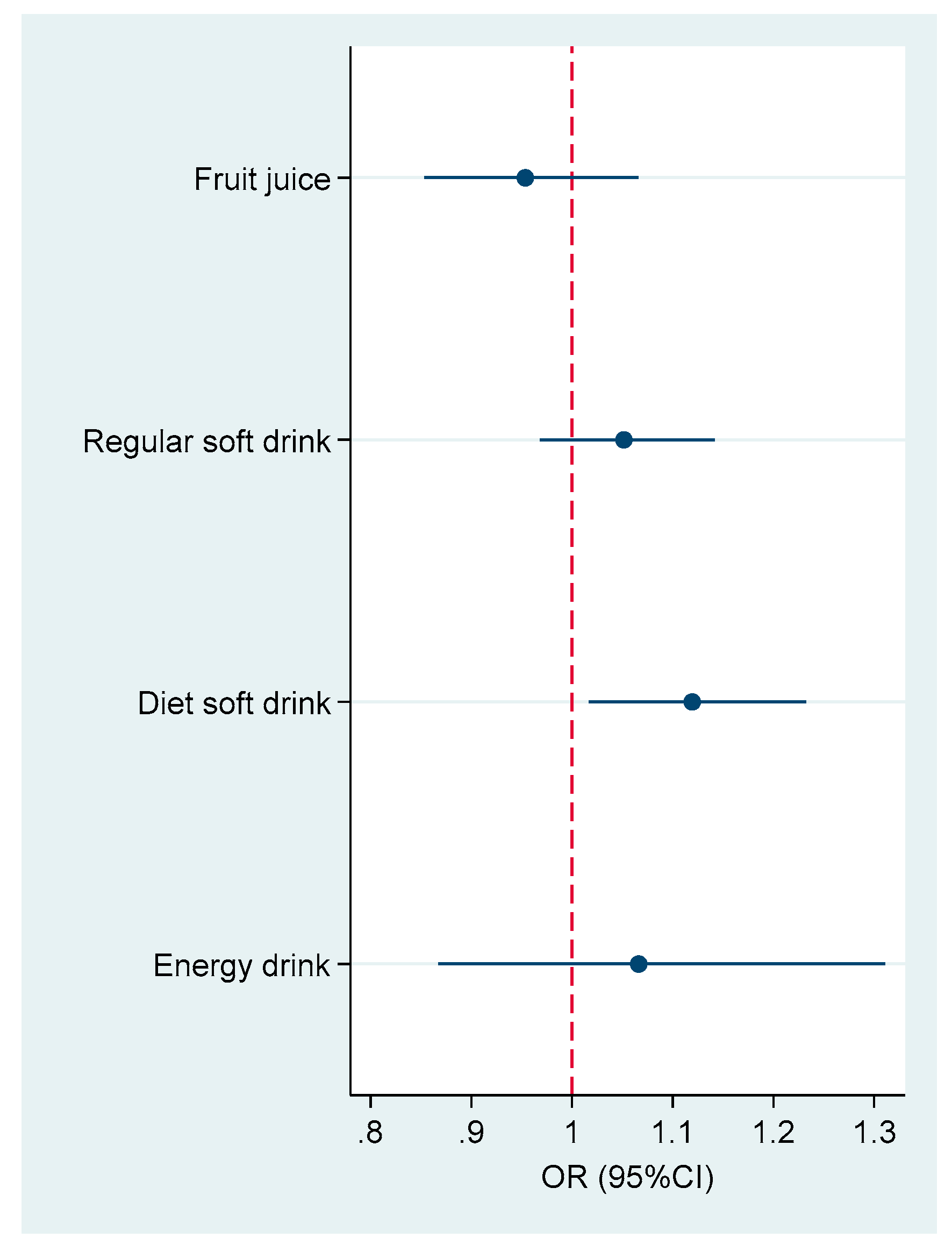
3.2. Association with Asthma
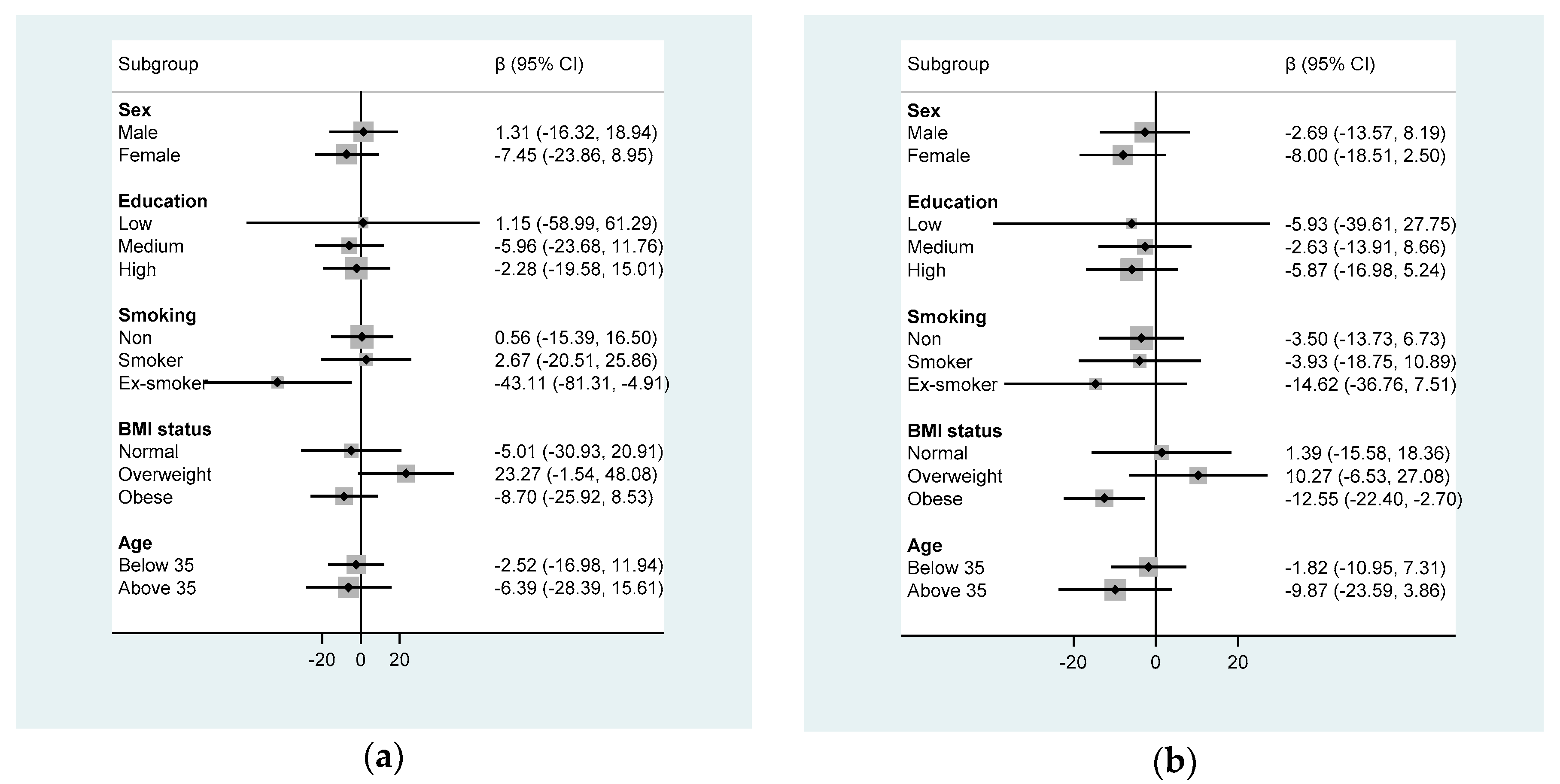
3.3. Association with FVC and FEV1
4. Discussion
4.1. Fruit Juice and Asthma
4.2. Diet Soft Drink and Asthma
4.3. Soft Drink and Lung Function
4.4. Potential Mechanisms
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Uchida, A.; Sakaue, K.; Inoue, H. Epidemiology of asthma-chronic obstructive pulmonary disease overlap (ACO). Allergol. Int. 2018, 67, 165–171. [Google Scholar] [CrossRef]
- GBD 2015 Chronic Respiratory Disease Collaborators. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet. Respir. Med. 2017, 5, 691–706. [Google Scholar] [CrossRef]
- Janahi, I.A.; Bener, A.; Bush, A. Prevalence of asthma among Qatari schoolchildren: International Study of Asthma and Allergies in Childhood, Qatar. Pediatr. Pulmonol. 2006, 41, 80–86. [Google Scholar] [CrossRef]
- Beasley, R.; Semprini, A.; Mitchell, E.A. Risk factors for asthma: Is prevention possible? Lancet 2015, 386, 1075–1085. [Google Scholar] [CrossRef]
- Colak, Y.; Afzal, S.; Lange, P.; Nordestgaard, B.G. Smoking, Systemic Inflammation, and Airflow Limitation: A Mendelian Randomization Analysis of 98 085 Individuals from the General Population. Nicotine Tob. Res. 2018. [Google Scholar] [CrossRef]
- Yiallouros, P.K.; Lamnisos, D.; Kolokotroni, O.; Moustaki, M.; Middleton, N. Associations of body fat percent and body mass index with childhood asthma by age and gender. Obesity 2013, 21, E474–E482. [Google Scholar] [CrossRef] [PubMed]
- Almqvist, C.; Pershagen, G.; Wickman, M. Low socioeconomic status as a risk factor for asthma, rhinitis and sensitization at 4 years in a birth cohort. Clin. Exp. Allergy 2005, 35, 612–618. [Google Scholar] [CrossRef] [PubMed]
- Devereux, G. Nutrition as potential determinant of asthma. Proc. Nutr. Soc. 2010, 69, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Bakolis, I.; Hooper, R.; Thompson, R.L.; Shaheen, S.O. Dietary patterns and adult asthma: Population-based case-control study. Allergy 2010, 65, 606–615. [Google Scholar] [CrossRef] [PubMed]
- McKeever, T.M.; Lewis, S.A.; Cassano, P.A.; Ocke, M.; Burney, P.; Britton, J.; Smit, H.A. Patterns of dietary intake and relation to respiratory disease, forced expiratory volume in 1 s, and decline in 5-y forced expiratory volume. Am. J. Clin. Nutr. 2010, 92, 408–415. [Google Scholar] [CrossRef] [PubMed]
- Shaheen, S.O.; Jameson, K.A.; Syddall, H.E.; Sayer, A.A.; Dennison, E.M.; Cooper, C.; Robinson, S.M.; Hertfordshire Cohort Study Group. The relationship of dietary patterns with adult lung function and COPD. Eur. Respir. J. 2010, 36, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Barros, R.; Moreira, A.; Padrao, P.; Teixeira, V.H.; Carvalho, P.; Delgado, L.; Lopes, C.; Severo, M.; Moreira, P. Dietary patterns and asthma prevalence, incidence and control. Clin. Exp. Allergy 2015, 45, 1673–1680. [Google Scholar] [CrossRef]
- Varraso, R.; Kauffmann, F.; Leynaert, B.; Le Moual, N.; Boutron-Ruault, M.C.; Clavel-Chapelon, F.; Romieu, I. Dietary patterns and asthma in the E3N study. Eur. Respir. J. 2009, 33, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Varraso, R.; Fung, T.T.; Hu, F.B.; Willett, W.; Camargo, C.A. Prospective study of dietary patterns and chronic obstructive pulmonary disease among US men. Thorax 2007, 62, 786–791. [Google Scholar] [CrossRef]
- Park, S.; Akinbami, L.J.; McGuire, L.C.; Blanck, H.M. Association of sugar-sweetened beverage intake frequency and asthma among U.S. adults, 2013. Prev. Med. 2016, 91, 58–61. [Google Scholar] [CrossRef]
- Shi, Z.; Dal Grande, E.; Taylor, A.W.; Gill, T.K.; Adams, R.; Wittert, G.A. Association between soft drink consumption and asthma and chronic obstructive pulmonary disease among adults in Australia. Respirology 2012, 17, 363–369. [Google Scholar] [CrossRef]
- DeChristopher, L.R.; Tucker, K.L. Excess free fructose, high-fructose corn syrup and adult asthma: The Framingham Offspring Cohort. Br. J. Nutr. 2018, 119, 1157–1167. [Google Scholar] [CrossRef]
- DeChristopher, L.R.; Uribarri, J.; Tucker, K.L. Intakes of apple juice, fruit drinks and soda are associated with prevalent asthma in US children aged 2–9 years. Public Health Nutr. 2016, 19, 123–130. [Google Scholar] [CrossRef]
- Cisneros, R.; Gonzalez, M.; Brown, P.; Schweizer, D. Soda consumption and hospital admissions among Californian adults with asthma. J. Asthma 2017, 54, 371–375. [Google Scholar] [CrossRef]
- Park, S.; Blanck, H.M.; Sherry, B.; Jones, S.E.; Pan, L. Regular-soda intake independent of weight status is associated with asthma among US high school students. J. Acad. Nutr. Diet. 2013, 113, 106–111. [Google Scholar] [CrossRef]
- Sørensen, L.B.; Raben, A.; Stender, S.; Astrup, A. Effect of sucrose on inflammatory markers in overweight humans. Am. J. Clin. Nutr. 2005, 82, 421–427. [Google Scholar] [CrossRef]
- Schulze, M.B.; Hoffmann, K.; Manson, J.E.; Willett, W.C.; Meigs, J.B.; Weikert, C.; Heidemann, C.; Colditz, G.A.; Hu, F.B. Dietary pattern, inflammation, and incidence of type 2 diabetes in women. Am. J. Clin. Nutr. 2005, 82, 675–684. [Google Scholar] [CrossRef]
- Aeberli, I.; Gerber, P.A.; Hochuli, M.; Kohler, S.; Haile, S.R.; Gouni-Berthold, I.; Berthold, H.K.; Spinas, G.A.; Berneis, K. Low to moderate sugar-sweetened beverage consumption impairs glucose and lipid metabolism and promotes inflammation in healthy young men: A randomized controlled trial. Am. J. Clin. Nutr. 2011, 94, 479–485. [Google Scholar] [CrossRef]
- Buckley, S.T.; Ehrhardt, C. The receptor for advanced glycation end products (RAGE) and the lung. J. Biomed. Biotechnol. 2010, 2010, 917108. [Google Scholar] [CrossRef]
- Sayegh, A.; Dini, E.L.; Holt, R.D.; Bedi, R. Food and drink consumption, sociodemographic factors and dental caries in 4-5-year-old children in Amman, Jordan. Br. Dent. J. 2002, 193, 37–42. [Google Scholar] [CrossRef]
- Rasheed, P. Perception of body weight and self-reported eating and exercise behaviour among obese and non-obese women in Saudi Arabia. Public Health 1998, 112, 409–414. [Google Scholar] [CrossRef]
- Yang, L.; Bovet, P.; Liu, Y.; Zhao, M.; Ma, C.; Liang, Y.; Xi, B. Consumption of Carbonated Soft Drinks Among Young Adolescents Aged 12 to 15 Years in 53 Low- and Middle-Income Countries. Am. J. Public Health 2017, 107, 1095–1100. [Google Scholar] [CrossRef]
- Al Kuwari, H.; Al Thani, A.; Al Marri, A.; Al Kaabi, A.; Abderrahim, H.; Afifi, N.; Qafoud, F.; Chan, Q.; Tzoulaki, I.; Downey, P.; et al. The Qatar Biobank: Background and methods. BMC Public Health 2015, 15, 1208. [Google Scholar] [CrossRef]
- Liistro, G.; Vanwelde, C.; Vincken, W.; Vandevoorde, J.; Verleden, G.; Buffels, J.; Board, C.A. Technical and functional assessment of 10 office spirometers: A multicenter comparative study. Chest 2006, 130, 657–665. [Google Scholar] [CrossRef]
- Broekhuizen, R.; Wouters, E.F.; Creutzberg, E.C.; Schols, A.M. Raised CRP levels mark metabolic and functional impairment in advanced COPD. Thorax 2006, 61, 17–22. [Google Scholar] [CrossRef]
- DeChristopher, L.R.; Uribarri, J.; Tucker, K.L. Intake of high fructose corn syrup sweetened soft drinks is associated with prevalent chronic bronchitis in U.S. Adults, ages 20–55 years. Nutr. J. 2015, 14, 107. [Google Scholar] [CrossRef]
- Maslova, E.; Strom, M.; Olsen, S.F.; Halldorsson, T.I. Consumption of artificially-sweetened soft drinks in pregnancy and risk of child asthma and allergic rhinitis. PLoS ONE 2013, 8, e57261. [Google Scholar] [CrossRef]
- Berentzen, N.E.; van Stokkom, V.L.; Gehring, U.; Koppelman, G.H.; Schaap, L.A.; Smit, H.A.; Wijga, A.H. Associations of sugar-containing beverages with asthma prevalence in 11-year-old children: The PIAMA birth cohort. Eur. J. Clin. Nutr. 2015, 69, 303–308. [Google Scholar] [CrossRef]
- DeChristopher, L.R.; Uribarri, J.; Tucker, K.L. The link between soda intake and asthma: Science points to the high-fructose corn syrup, not the preservatives: A commentary. Nutr. Diabetes 2016, 6, e234. [Google Scholar] [CrossRef]
- Genton, C.; Frei, P.C.; Pecoud, A. Value of oral provocation tests to aspirin and food additives in the routine investigation of asthma and chronic urticaria. J. Allergy Clin. Immunol. 1985, 76, 40–45. [Google Scholar] [CrossRef]
- Freedman, B.J. Sulphur dioxide in foods and beverages: Its use as a preservative and its effect on asthma. Br. J. Dis. Chest 1980, 74, 128–134. [Google Scholar] [CrossRef]
- Steinman, H.A.; Weinberg, E.G. The effects of soft-drink preservatives on asthmatic children. S. Afr. Med. J. 1986, 70, 404–406. [Google Scholar]
- Shi, W.; Lin, Z.; Liao, C.; Zhang, J.; Liu, W.; Wang, X.; Cai, J.; Zou, Z.; Wang, H.; Norback, D.; et al. Urinary phthalate metabolites in relation to childhood asthmatic and allergic symptoms in Shanghai. Environ. Int. 2018, 121, 276–286. [Google Scholar] [CrossRef]
- Sin, D.D.; Sutherland, E.R. Obesity and the lung: 4. Obesity and asthma. Thorax 2008, 63, 1018–1023. [Google Scholar] [CrossRef]
- Bornehag, C.G.; Nanberg, E. Phthalate exposure and asthma in children. Int. J. Androl. 2010, 33, 333–345. [Google Scholar] [CrossRef]
- Bai, P.Y.; Wittert, G.A.; Taylor, A.W.; Martin, S.A.; Milne, R.W.; Shi, Z. The association of socio-demographic status, lifestyle factors and dietary patterns with total urinary phthalates in Australian men. PLoS ONE 2015, 10, e0122140. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| None | ~1 Time/Week | 1–6 Times/Week | ≥7 Times/Week | p Value | |
|---|---|---|---|---|---|
| n = 356 | n = 231 | n = 269 | n = 130 | ||
| Age | 44.6 (12.1) | 39.3 (11.1) | 36.1 (10.6) | 33.2 (8.5) | <0.001 |
| Age groups (years) | <0.001 | ||||
| <40 | 127 (35.7%) | 127 (55.0%) | 171 (63.6%) | 108 (83.1%) | |
| 40–60 | 189 (53.1%) | 95 (41.1%) | 93 (34.6%) | 21 (16.2%) | |
| >60 | 40 (11.2%) | 9 (3.9%) | 5 (1.9%) | 1 (0.8%) | |
| Sex | <0.001 | ||||
| Male | 142 (39.9%) | 125 (54.1%) | 150 (55.8%) | 81 (62.3%) | |
| Female | 214 (60.1%) | 106 (45.9%) | 119 (44.2%) | 49 (37.7%) | |
| Education | <0.001 | ||||
| Low | 62 (17.4%) | 12 (5.2%) | 20 (7.5%) | 9 (6.9%) | |
| Medium | 86 (24.2%) | 55 (23.8%) | 79 (29.5%) | 53 (40.8%) | |
| High | 208 (58.4%) | 164 (71.0%) | 169 (63.1%) | 68 (52.3%) | |
| Smoking | <0.001 | ||||
| Non | 281 (78.9%) | 146 (63.2%) | 175 (65.1%) | 68 (52.3%) | |
| Smoker | 32 (9.0%) | 48 (20.8%) | 53 (19.7%) | 47 (36.2%) | |
| Ex-smoker | 43 (12.1%) | 37 (16.0%) | 41 (15.2%) | 15 (11.5%) | |
| BMI (kg/m2) | 29.5 (5.2) | 28.2 (5.2) | 28.5 (6.1) | 29.2 (6.2) | 0.035 |
| BMI status | 0.024 | ||||
| Normal | 64 (18.0%) | 57 (24.7%) | 65 (24.2%) | 30 (23.1%) | |
| Overweight | 130 (36.5%) | 91 (39.4%) | 97 (36.1%) | 37 (28.5%) | |
| Obese | 147 (41.3%) | 71 (30.7%) | 78 (29.0%) | 51 (39.2%) | |
| Missing | 15 (4.2%) | 12 (5.2%) | 29 (10.8%) | 12 (9.2%) | |
| CRP levels (%) | 0.39 | ||||
| <6 mg/L | 245 (68.8%) | 149 (64.5%) | 178 (66.2%) | 82 (63.1%) | |
| ≥6 mg/L | 68 (19.1%) | 47 (20.3%) | 49 (18.2%) | 34 (26.2%) | |
| Missing | 43 (12.1%) | 35 (15.2%) | 42 (15.6%) | 14 (10.8%) | |
| Leisure time physical activity (MET hours/week) | 20.8 (38.4) | 18.1 (42.7) | 17.9 (40.8) | 13.4 (22.2) | 0.31 |
| FEV1 (mL) | 2745.8 (795.5) | 2977.7 (751.8) | 3156.4 (787.7) | 3191.4 (768.2) | <0.001 |
| FVC (mL) | 2946.4 (1051.4) | 3189.3 (983.5) | 3322.0 (1028.8) | 3506.8 (1032.4) | <0.001 |
| Asthma | 21 (5.9%) | 15 (6.5%) | 14 (5.2%) | 15 (11.5%) | 0.098 |
| None | ~1 Time/Week | 1–6 Times/Week | ≥7 Times/Week | p Value | |
|---|---|---|---|---|---|
| Model 1 | 1.00 | 1.23 (0.61–2.47) | 1.00 (0.48–2.08) | 2.51 (1.17–5.36) | 0.002 |
| Model 2 | 1.00 | 1.23 (0.61–2.51) | 1.00 (0.48–2.08) | 2.60 (1.20–5.63) | 0.001 |
| Model 3 | 1.00 | 1.19 (0.58–2.46) | 0.94 (0.44–1.98) | 2.33 (1.06–5.15) | 0.005 |
| Model 4 | 1.00 | 1.21 (0.53–2.75) | 1.29 (0.59–2.84) | 2.64 (1.10–6.36) | 0.010 |
| None | ~1 Time/Week | 1–6 Times/Week | ≥7 Times/Week | p Value | |
|---|---|---|---|---|---|
| FVC | |||||
| Model 1 | 0.00 | −87.1 (−219.7–45.5) | −46.9 (−177.4–83.7) | −12.6 (−178.1–153.0) | 0.811 |
| Model 2 | 0.00 | −117.3 (−250.5–15.9) | −54.8 (−185.1–75.6) | −29.1 (−195.5–137.3) | 0.813 |
| Model 3 | 0.00 | −116.3 (−249.5–16.8) | −53.1 (−183.7–77.5) | −6.7(−174.0–160.6) | 0.889 |
| Model 4 | 0.00 | −126.5 (−261.4–8.5) | −60.0 (−191.6–71.6) | −3.0 (−173.9–167.9) | 0.824 |
| FEV1 | |||||
| Model 1 | 0.00 | −79.0 (−161.9–3.8) | 6.4 (−75.2–88.0) | −100.7 (−204.1–2.8) | 0.203 |
| Model 2 | 0.00 | −88.3 (−171.9−4.7) | 7.8 (−74.0–89.6) | −97.6 (−202.0–6.9) | 0.285 |
| Model 3 | 0.00 | −81.7 (−164.9–1.6) | 9.5 (−72.2–91.1) | −90.1 (−194.6–14.5) | 0.403 |
| Model 4 | 0.00 | −94.0 (−177.7–10.3) | 1.4 (−80.2–83.1) | −96.4 (−202.4–9.6) | 0.485 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ibrahim, A.A.; Qamar, B.; Fituri, S.; Akbar, Z.A.; Al-Abdi, T.; Shi, Z. Association between Soft Drink Consumption and Asthma among Qatari Adults. Nutrients 2019, 11, 606. https://doi.org/10.3390/nu11030606
Ibrahim AA, Qamar B, Fituri S, Akbar ZA, Al-Abdi T, Shi Z. Association between Soft Drink Consumption and Asthma among Qatari Adults. Nutrients. 2019; 11(3):606. https://doi.org/10.3390/nu11030606
Chicago/Turabian StyleIbrahim, Amna Al, Bushra Qamar, Sundus Fituri, Zoha Ali Akbar, Tamara Al-Abdi, and Zumin Shi. 2019. "Association between Soft Drink Consumption and Asthma among Qatari Adults" Nutrients 11, no. 3: 606. https://doi.org/10.3390/nu11030606
APA StyleIbrahim, A. A., Qamar, B., Fituri, S., Akbar, Z. A., Al-Abdi, T., & Shi, Z. (2019). Association between Soft Drink Consumption and Asthma among Qatari Adults. Nutrients, 11(3), 606. https://doi.org/10.3390/nu11030606