The Effects of a Whey Protein and Guar Gum-Containing Preload on Gastric Emptying, Glycaemia, Small Intestinal Absorption and Blood Pressure in Healthy Older Subjects


 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Protocol
2.3. Measurements
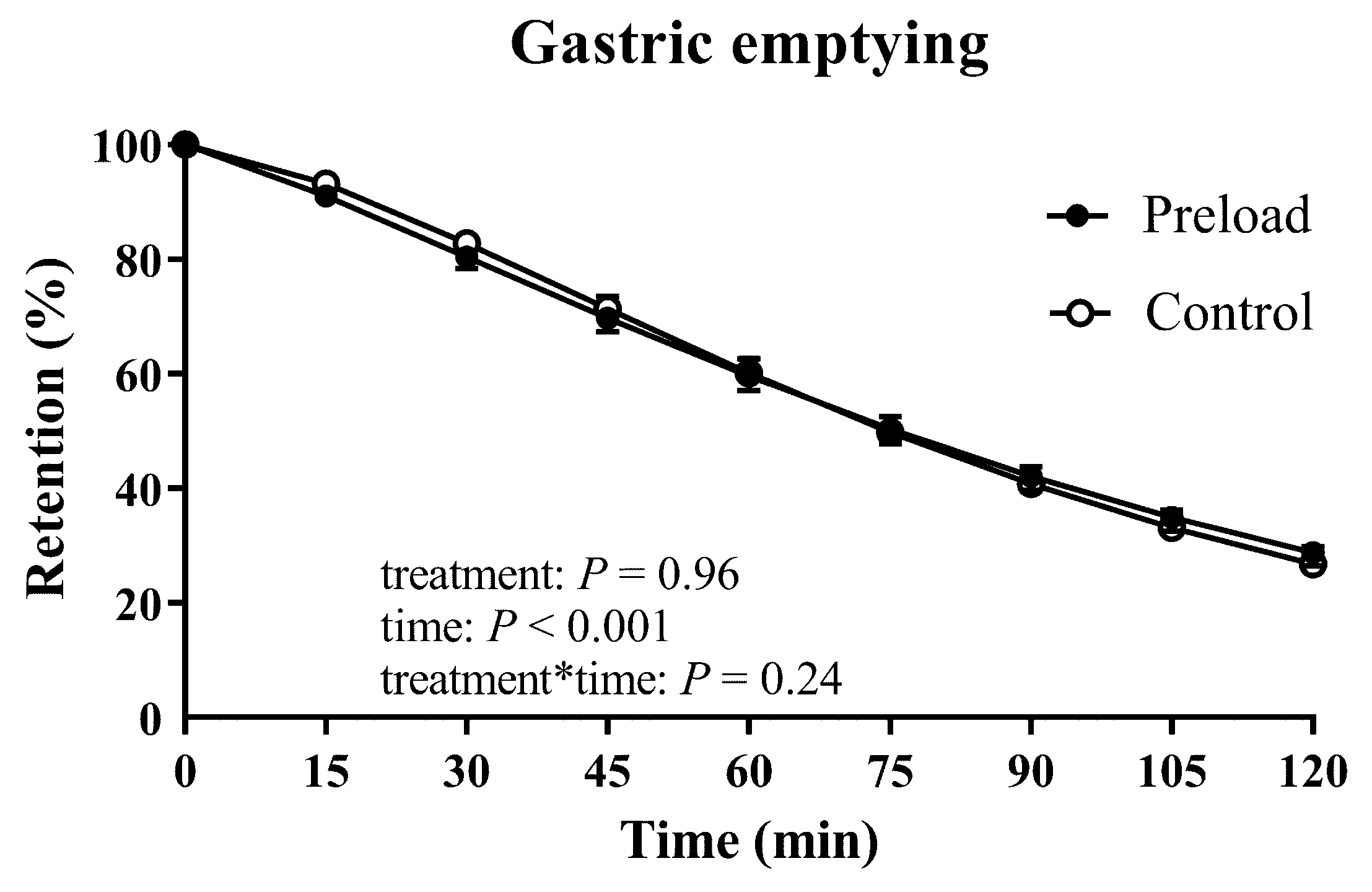
2.3.1. Gastric Emptying
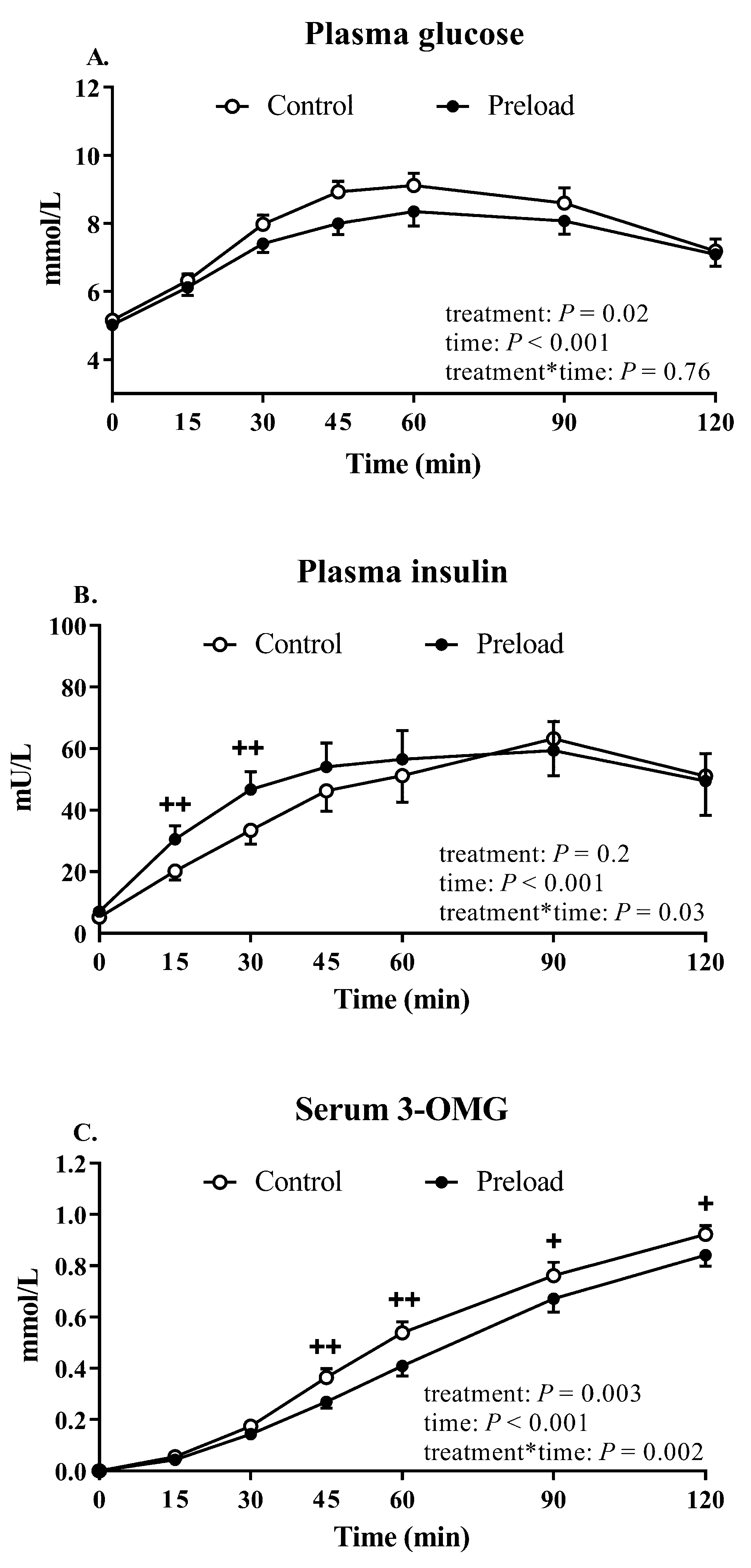
2.3.2. Plasma Glucose and Insulin
2.3.3. Oral Glucose Absorption (Serum 3-OMG)
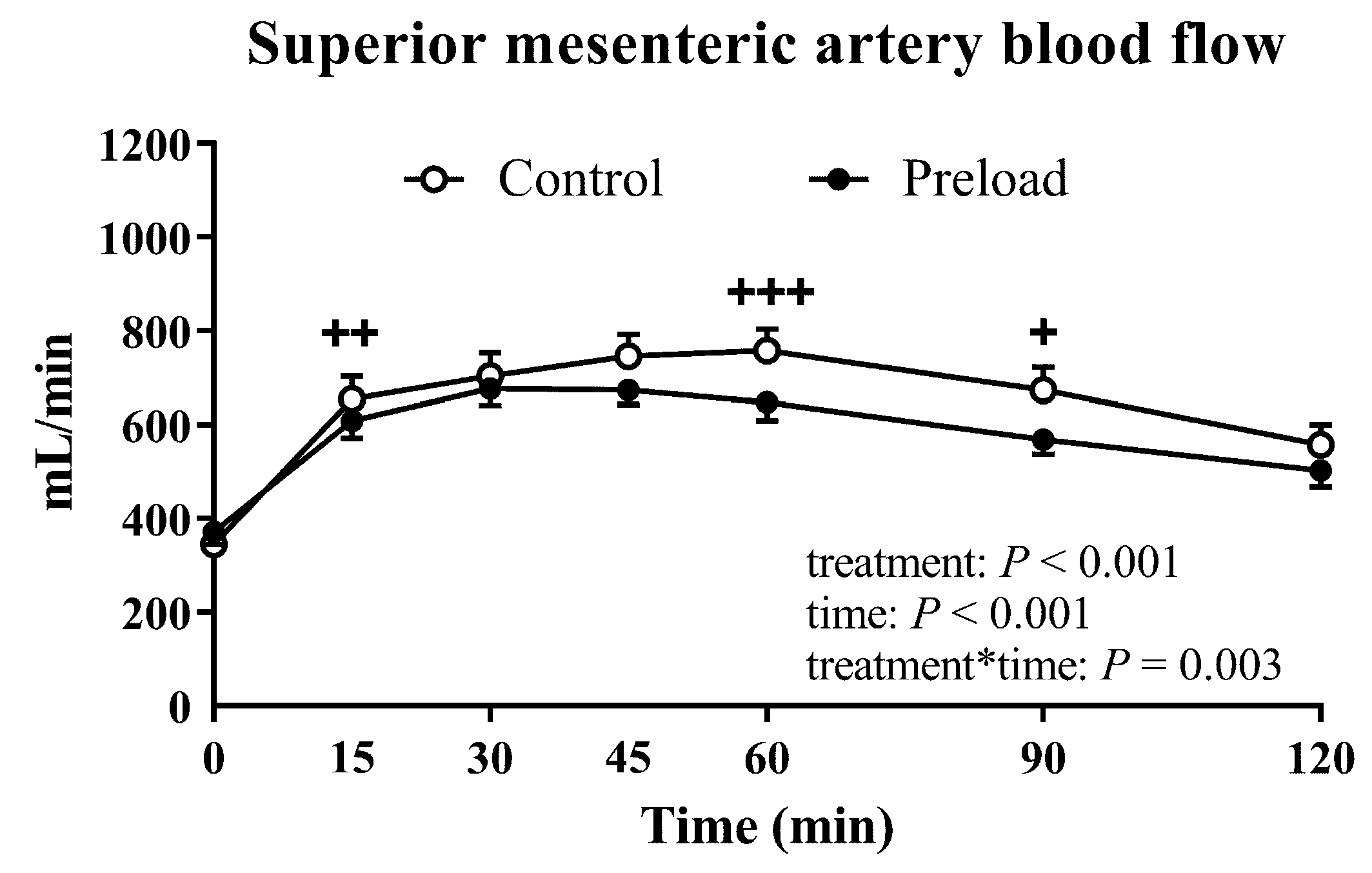
2.3.4. Superior Mesenteric Artery Blood Flow
2.3.5. Blood Pressure and Heart Rate
2.3.6. Cardiovascular Autonomic Nerve Dysfunction
2.4. Statistical Analysis
3. Results
3.1. Gastric Emptying
3.2. Plasma Glucose and Insulin
3.3. Glucose Absorption
3.4. Superior Mesenteric Artery Blood Flow
3.5. Blood Pressure and Heart Rate
3.5.1. Systolic Blood Pressure
3.5.2. Diastolic Blood Pressure
3.5.3. Heart Rate
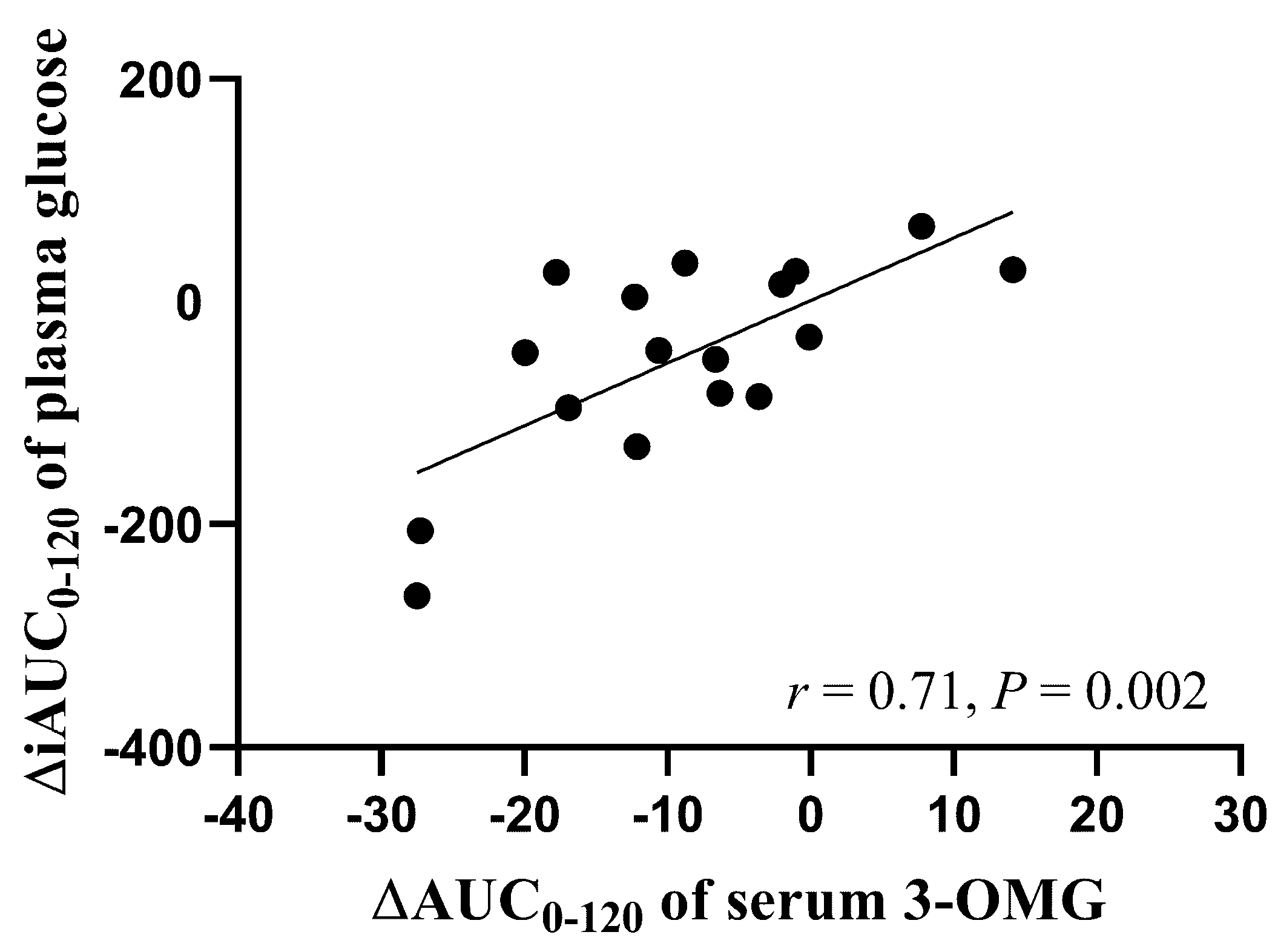
3.6. Relationships between Plasma Insulin and Serum 3-OMG between the Two Study Days
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Clifton, P.M.; Galbraith, C.; Coles, L. Effect of a low dose whey/guar preload on glycemic control in people with type 2 diabetes--A randomised controlled trial. Nutr. J. 2014, 13, 103. [Google Scholar] [CrossRef] [PubMed]
- Watson, L.E.; Phillips, L.K.; Wu, T.; Bound, M.J.; Checklin, H.L.; Grivell, J.; Jones, K.L.; Clifton, P.M.; Horowitz, M.; Rayner, C.K. A whey/guar “preload” improves postprandial glycaemia and HbA1c in type 2 diabetes-a 12-week, single-blind, randomized, placebo-controlled trial. In Diabetes, Obesity & Metabolism; Wiley Online Library: Hoboken, NJ, USA, 2018. [Google Scholar] [CrossRef]
- Li, C.-J.; Norstedt, G.; Hu, Z.-G.; Yu, P.; Li, D.-Q.; Li, J.; Yu, Q.; Sederholm, M.; Yu, D.-M. Effects of a macro-nutrient preload on type 2 diabetic patients. Front. Endocrinol. 2015, 6, 139. [Google Scholar] [CrossRef] [PubMed]
- Watson, L.E.; Phillips, L.K.; Wu, T.; Bound, M.J.; Checklin, H.; Grivell, J.; Jones, K.L.; Horowitz, M.; Rayner, C.K. Differentiating the effects of whey protein and guar gum preloads on postprandial glycemia in type 2 diabetes. Clin. Nutr. 2018, 38. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Stevens, J.E.; Cukier, K.; Maddox, A.F.; Wishart, J.M.; Jones, K.L.; Clifton, P.M.; Horowitz, M.; Rayner, C.K. Effects of a protein preload on gastric emptying, glycemia, and gut hormones after a carbohydrate meal in diet-controlled type 2 diabetes. Diabetes Care 2009, 32, 1600–1602. [Google Scholar] [CrossRef] [PubMed]
- Marathe, C.S.; Rayner, C.K.; Jones, K.L.; Horowitz, M. Relationships between gastric emptying, postprandial glycemia, and incretin hormones. Diabetes Care 2013, 36, 1396–1405. [Google Scholar] [CrossRef] [PubMed]
- Watson, L.E.; Xie, C.; Wang, X.; Li, Z.; Phillips, L.K.; Sun, Z.; Jones, K.L.; Horowitz, M.; Rayner, C.K.; Wu, T. Gastric emptying in patients with well-controlled type 2 diabetes compared with young and older control subjects without diabetes. J. Clin. Endocrinol. Metab. 2019, 104, 3311–3319. [Google Scholar] [CrossRef]
- Maurer, A.H.; Parkman, H.P. Update on gastrointestinal scintigraphy. Semin. Nucl. Med. 2006, 36, 110–118. [Google Scholar] [CrossRef]
- Schwartz, M.P.; Samsom, M.; Renooij, W.; Van Steenderen, L.W.; Benninga, M.A.; Van Geenen, E.-J.M.; Van Herwaarden, M.A.; De Smet, M.B.; Smout, A.J. Small bowel motility affects glucose absorption in a healthy man. Diabetes Care 2002, 25, 1857–1861. [Google Scholar] [CrossRef]
- Mathias, C.J. Postprandial hypotension. Pathophysiological mechanisms and clinical implications in different disorders. Hypertension 1991, 18, 694–704. [Google Scholar] [CrossRef]
- Jansen, R.W.; Lipsitz, L.A. Postprandial hypotension: Epidemiology, pathophysiology, and clinical management. Ann. Intern. Med. 1995, 122, 286–295. [Google Scholar] [CrossRef]
- Fisher, A.A.; Davis, M.W.; Srikusalanukul, W.; Budge, M.M. Postprandial hypotension predicts all-cause mortality in older, low-level care residents. J. Am. Geriatr. Soc. 2005, 53, 1313–1320. [Google Scholar] [CrossRef] [PubMed]
- Trahair, L.G.; Horowitz, M.; Jones, K.L. Postprandial hypotension: A systematic review. J. Am. Med. Dir. Assoc. 2014, 15, 394–409. [Google Scholar] [CrossRef]
- Trahair, L.G.; Horowitz, M.; Jones, K.L. Postprandial hypotension is associated with more rapid gastric emptying in healthy older individuals. J. Am. Med. Dir. Assoc. 2015, 16, 521–523. [Google Scholar] [CrossRef] [PubMed]
- Pham, H.; Phillips, L.; Trahair, L.; Hatzinikolas, S.; Horowitz, M.; Jones, K.L. Longitudinal changes in the blood pressure responses to, and gastric emptying of, an oral glucose load in healthy older subjects. J. Gerontol. A Biol. Sci. Med. Sci. 2019. [Google Scholar] [CrossRef]
- Jones, K.L.; Tonkin, A.; Horowitz, M.; Wishart, J.M.; Carney, B.I.; Guha, S.; Green, L. Rate of gastric emptying is a determinant of postprandial hypotension in non-insulin-dependent diabetes mellitus. Clin. Sci. 1998, 94, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Jones, K.L.; MacIntosh, C.; Su, Y.C.; Wells, F.; Chapman, I.M.; Tonkin, A.; Horowitz, M. Guar gum reduces postprandial hypotension in older people. J. Am. Geriatr. Soc. 2001, 49, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Russo, A.; Stevens, J.E.; Wilson, T.; Wells, F.; Tonkin, A.; Horowitz, M.; Jones, K.L. Guar attenuates fall in postprandial blood pressure and slows gastric emptying of oral glucose in type 2 diabetes. Dig. Dis. Sci. 2003, 48, 1221–1229. [Google Scholar] [CrossRef] [PubMed]
- Trahair, L.G.; Horowitz, M.; Hausken, T.; Feinle-Bisset, C.; Rayner, C.K.; Jones, K.L. Effects of exogenous glucagon-like peptide-1 on the blood pressure, heart rate, mesenteric blood flow, and glycemic responses to intraduodenal glucose in healthy older subjects. J. Clin. Endocrinol. Metab. 2014, 99, 2628–2634. [Google Scholar] [CrossRef]
- Jones, K.L.; Rigda, R.S.; Buttfield, M.D.M.; Hatzinikolas, S.; Pham, H.T.; Marathe, C.S.; Wu, T.; Lange, K.; Trahair, L.G.; Rayner, C.K.; et al. Effects of lixisenatide on postprandial blood pressure, gastric emptying and glycaemia in healthy people and people with type 2 diabetes. Diabetes Obes. Metab. 2019, 21, 1158–1167. [Google Scholar] [CrossRef]
- Gentilcore, D.; Doran, S.; Meyer, J.H.; Horowitz, M.; Jones, K.L. Effects of intraduodenal glucose concentration on blood pressure and heart rate in healthy older subjects. Dig. Dis. Sci. 2006, 51, 652–656. [Google Scholar] [CrossRef]
- Vanis, L.; Gentilcore, D.; Rayner, C.K.; Wishart, J.M.; Horowitz, M.; Feinle-Bisset, C.; Jones, K.L. Effects of small intestinal glucose load on blood pressure, splanchnic blood flow, glycemia, and GLP-1 release in healthy older subjects. Am. J. Phys. Regul. Integr. Comp. Phys. 2011, 300, 1524–1531. [Google Scholar] [CrossRef] [PubMed]
- Trahair, L.G.; Kimber, T.E.; Flabouris, K.; Horowitz, M.; Jones, K.L. Gastric emptying, postprandial blood pressure, glycaemia and splanchnic flow in Parkinson’s disease. World J. Gastroenterol. 2016, 22, 4860–4867. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Postprandial blood glucose. Diabetes Care 2001, 24, 775–778. [Google Scholar] [CrossRef] [PubMed]
- Trahair, L.G.; Horowitz, M.; Stevens, J.E.; Feinle-Bisset, C.; Standfield, S.; Piscitelli, D.; Rayner, C.K.; Deane, A.M.; Jones, K.L. Effects of exogenous glucagon-like peptide-1 on blood pressure, heart rate, gastric emptying, mesenteric blood flow and glycaemic responses to oral glucose in older individuals with normal glucose tolerance or type 2 diabetes. Diabetologia 2015, 58, 1769–1778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horowitz, M.; Edelbroek, M.A.; Wishart, J.M.; Straathof, J.W. Relationship between oral glucose tolerance and gastric emptying in normal healthy subjects. Diabetologia 1993, 36, 857–862. [Google Scholar] [CrossRef]
- Wu, T.; Zhang, X.; Trahair, L.G.; Bound, M.J.; Little, T.J.; Deacon, C.F.; Horowitz, M.; Jones, K.L.; Rayner, C.K. Small intestinal glucose delivery affects the lowering of blood glucose by acute vildagliptin in type 2 diabetes. J. Clin. Endocrinol. Metab. 2016, 101, 4769–4778. [Google Scholar] [CrossRef]
- Aono, D.; Oka, R.; Kometani, M.; Takeda, Y.; Karashima, S.; Yoshimura, K.; Takeda, Y.; Yoneda, T. Insulin secretion and risk for future diabetes in subjects with a nonpositive insulinogenic index. J. Diabetes Res. 2018, 2018, 5107589. [Google Scholar] [CrossRef]
- Wu, T.; Xie, C.; Wu, H.; Jones, K.L.; Horowitz, M.; Rayner, C.K. Metformin reduces the rate of small intestinal glucose absorption in type 2 diabetes. Diabetes Obes. Metab. 2017, 19, 290–293. [Google Scholar] [CrossRef]
- Pham, H.T.; Stevens, J.E.; Rigda, R.S.; Phillips, L.K.; Wu, T.; Hausken, T.; Soenen, S.; Visvanathan, R.; Rayner, C.K.; Horowitz, M.; et al. Effects of intraduodenal administration of the artificial sweetener sucralose on blood pressure and superior mesenteric artery blood flow in healthy older subjects. Am. J. Clin. Nutr. 2018, 108, 156–162. [Google Scholar] [CrossRef]
- Arora, R.R.; Bulgarelli, R.J.; Ghosh-Dastidar, S.; Colombo, J. Autonomie mechanisms and therapeutic implications of postural diabetic cardiovascular abnormalities. J. Diabetes Sci. Technol. 2008, 2, 645–657. [Google Scholar] [CrossRef]
- Piha, S.J. Cardiovascular autonomic reflex tests: Normal responses and age-related reference values. Clin. Phys. Func. Imaging 1991, 11, 277–290. [Google Scholar]
- Ewing, D.J.; Clarke, B.F. Diagnosis and management of diabetic autonomic neuropathy. Br. Med. J. (Clin. Res. Ed.) 1982, 285, 916–918. [Google Scholar] [CrossRef] [PubMed]
- Drucker, D.J. The role of gut hormones in glucose homeostasis. J. Clin. Investig. 2007, 117, 24–32. [Google Scholar] [CrossRef]
- Holst, J.J.; Gribble, F.; Horowitz, M.; Rayner, C.K. Roles of the gut in glucose homeostasis. Diabetes Care 2016, 39, 884–892. [Google Scholar] [CrossRef] [PubMed]
- Horowitz, M.; Wishart, J.M.; Jones, K.L.; Hebbard, G.S. Gastric emptying in diabetes: An overview. Diabet. Med. J. Br. Diabet. Assoc. 1996, 13, 16–22. [Google Scholar]
- Schmitz, O.; Brock, B.; Rungby, J. Amylin agonists: A novel approach in the treatment of diabetes. Diabetes 2004, 53, 233–238. [Google Scholar] [CrossRef]
- Gentilella, R.; Pechtner, V.; Corcos, A.; Consoli, A. Glucagon-like peptide-1 receptor agonists in type 2 diabetes treatment: Are they all the same. Diabetes Metab. Res. Rev. 2019, 35, 3070. [Google Scholar] [CrossRef]
- Brener, W.; Hendrix, T.R.; McHugh, P.R. Regulation of the gastric emptying of glucose. Gastroenterology 1983, 85, 76–82. [Google Scholar]
- Lin, H.C.; Doty, J.E.; Reedy, T.J.; Meyer, J.H. Inhibition of gastric emptying by glucose depends on length of intestine exposed to nutrient. Am. J. Physiol. 1989, 256, 404–411. [Google Scholar] [CrossRef]
- O’Donovan, D.; Feinle-Bisset, C.; Chong, C.; Cameron, A.; Tonkin, A.; Wishart, J.; Horowitz, M.; Jones, K.L. Intraduodenal guar attenuates the fall in blood pressure induced by glucose in healthy older adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2005, 60, 940–946. [Google Scholar] [CrossRef]
- Jenkins, D.J.; Goff, D.V.; Leeds, A.R.; Alberti, K.G.; Wolever, T.M.; Gassull, M.A.; Hockaday, T.D. Unabsorbable carbohydrates and diabetes: Decreased post-prandial hyperglycaemia. Lancet 1976, 2, 172–174. [Google Scholar] [CrossRef]
- Gentilcore, D.; Chaikomin, R.; Jones, K.L.; Russo, A.; Feinle-Bisset, C.; Wishart, J.M.; Rayner, C.K.; Horowitz, M. Effects of fat on gastric emptying of and the glycemic, insulin, and incretin responses to a carbohydrate meal in type 2 diabetes. J. Clin. Endocrinol. Metab. 2006, 91, 2062–2067. [Google Scholar] [CrossRef] [PubMed]
- Willms, B.; Werner, J.; Holst, J.J.; Orskov, C.; Creutzfeldt, W.; Nauck, M.A. Gastric emptying, glucose responses, and insulin secretion after a liquid test meal: Effects of exogenous glucagon-like peptide-1 (GLP-1)-(7–36) amide in type 2 (noninsulin-dependent) diabetic patients. J.Clin. Endocrinol. Metabo. 1996, 81, 327–332. [Google Scholar]
- Nauck, M.A.; Niedereichholz, U.; Ettler, R.; Holst, J.J.; Ørskov, C.; Ritzel, R.; Schmiegel, W.H. Glucagon-like peptide 1 inhibition of gastric emptying outweighs its insulinotropic effects in healthy humans. Am. J. Phys. Endocrinol. Metab. 1997, 273, 981–988. [Google Scholar] [CrossRef] [PubMed]
- Festa, A.; D’Agostino, R., Jr.; Hales, C.N.; Mykkanen, L.; Haffner, S.M. Heart rate in relation to insulin sensitivity and insulin secretion in nondiabetic subjects. Diabetes Care 2000, 23, 624–628. [Google Scholar] [CrossRef] [PubMed]
- Mogensen, C.E.; Christensen, N.J.; Gundersen, H.J. The acute effect of insulin on heart rate, blood pressure, plasma noradrenaline and urinary albumin excretion. The role of changes in blood glucose. Diabetologia 1980, 18, 453–457. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control (t = −3) | Preload (t = −18) | p Value | |
|---|---|---|---|
| SBP (mmHg) | 122.1 ± 3.2 | 120.0 ± 3.1 | 0.10 |
| DBP (mmHg) | 68.2 ± 1.9 | 67.3 ± 1.9 | 0.38 |
| HR (beats/min) | 62.1 ± 1.7 | 63.9 ± 2.3 | 0.09 |
| Plasma glucose (mmol/L) | 5.2 ± 0.1 | 5.2 ± 0.1 | 0.68 |
| Plasma insulin (mU/L) | 5.2 ± 0.9 | 5.3 ± 0.8 | 0.68 |
| SMA blood flow (mL/min) | 344 ± 23.6 | 329 ± 24.8 | 0.34 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pham, H.; Holen, I.S.; Phillips, L.K.; Hatzinikolas, S.; Huynh, L.Q.; Wu, T.; Hausken, T.; Rayner, C.K.; Horowitz, M.; Jones, K.L. The Effects of a Whey Protein and Guar Gum-Containing Preload on Gastric Emptying, Glycaemia, Small Intestinal Absorption and Blood Pressure in Healthy Older Subjects. Nutrients 2019, 11, 2666. https://doi.org/10.3390/nu11112666
Pham H, Holen IS, Phillips LK, Hatzinikolas S, Huynh LQ, Wu T, Hausken T, Rayner CK, Horowitz M, Jones KL. The Effects of a Whey Protein and Guar Gum-Containing Preload on Gastric Emptying, Glycaemia, Small Intestinal Absorption and Blood Pressure in Healthy Older Subjects. Nutrients. 2019; 11(11):2666. https://doi.org/10.3390/nu11112666
Chicago/Turabian StylePham, Hung, Iselin S. Holen, Liza K. Phillips, Seva Hatzinikolas, Lian Q. Huynh, Tongzhi Wu, Trygve Hausken, Christopher K. Rayner, Michael Horowitz, and Karen L. Jones. 2019. "The Effects of a Whey Protein and Guar Gum-Containing Preload on Gastric Emptying, Glycaemia, Small Intestinal Absorption and Blood Pressure in Healthy Older Subjects" Nutrients 11, no. 11: 2666. https://doi.org/10.3390/nu11112666
APA StylePham, H., Holen, I. S., Phillips, L. K., Hatzinikolas, S., Huynh, L. Q., Wu, T., Hausken, T., Rayner, C. K., Horowitz, M., & Jones, K. L. (2019). The Effects of a Whey Protein and Guar Gum-Containing Preload on Gastric Emptying, Glycaemia, Small Intestinal Absorption and Blood Pressure in Healthy Older Subjects. Nutrients, 11(11), 2666. https://doi.org/10.3390/nu11112666