Improving Cardiovascular Health through Nudging Healthier Food Choices: A Systematic Review

Abstract
1. Introduction
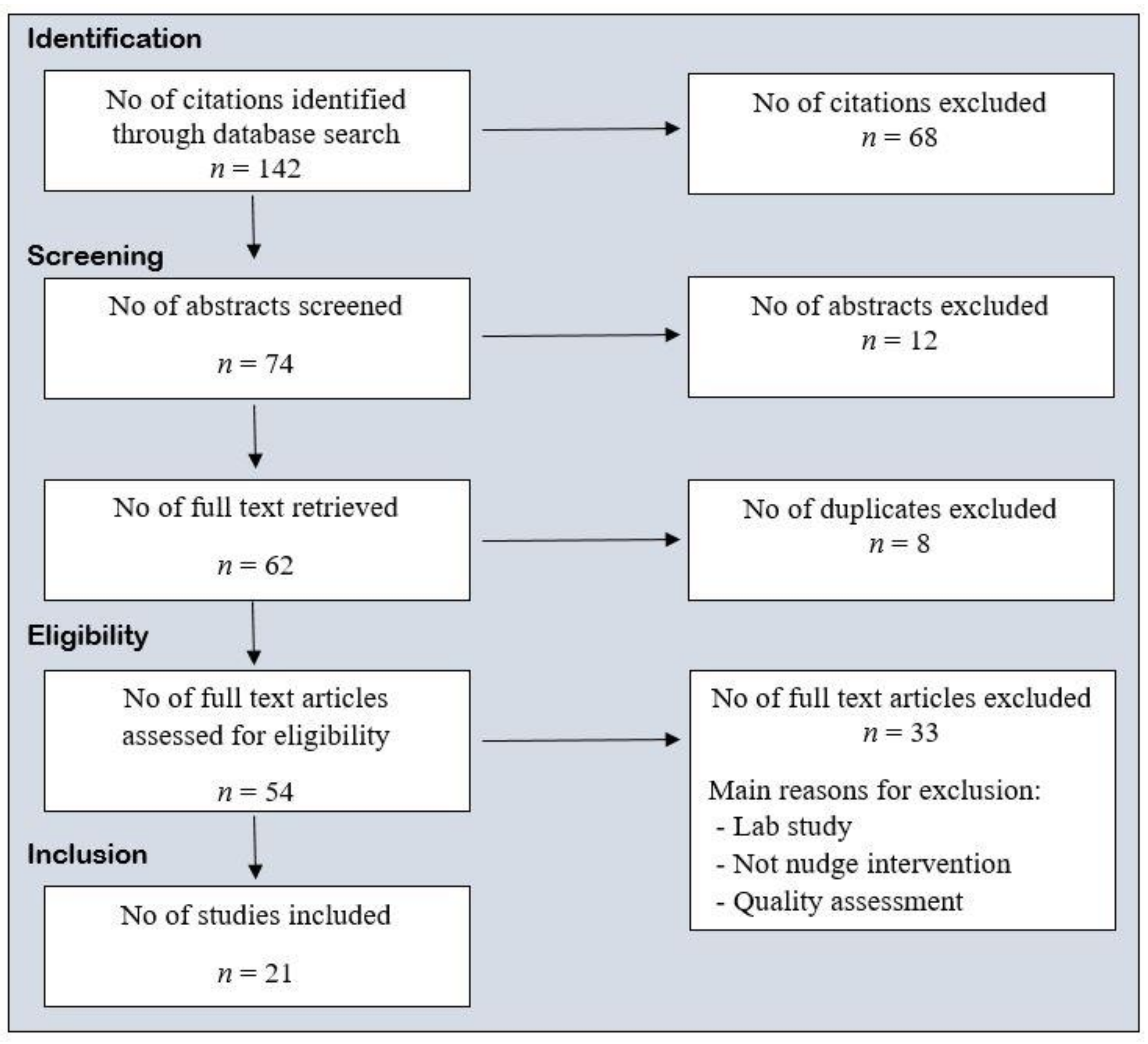
2. Materials and Methods
3. Results
3.1. Randomized Control Trials
3.2. Nonrandomized Control Trials
3.3. Mapping of the Nudges in the Included Studies
4. Discussion
4.1. Primarily Alter Properties of Objects or Stimuli
4.2. Primarily Alter Placement of Objects or Stimuli
4.3. Alter Both Properties and Placement of Objects or Stimuli
4.4. Implications for Research and Practice
4.5. Strengths and Limitations of This Study
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cornier, M.A.; Dabelea, D.; Hernandez, T.L.; Lindstrom, R.C.; Steig, A.J.; Stob, N.R.; Van Pelt, R.E.; Wang, H.; Eckel, R.H. The metabolic syndrome. Endocr. Rev. 2008, 29, 777–822. [Google Scholar] [PubMed]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [PubMed]
- Grundy, S.M. Metabolic syndrome pandemic. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 629–636. [Google Scholar] [CrossRef] [PubMed]
- Potenza, M.V.; Mechanick, J.I. The metabolic syndrome: Definition, global impact, and pathophysiology. Nutr. Clin. Pract. 2009, 24, 560–577. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.; Pieper, C.F.; Brown, A.J.; Bastian, L.A. Number of children and risk of metabolic syndrome in women. J. Womens Health 2006, 15, 763–773. [Google Scholar] [CrossRef]
- Laclaustra, M.; Corella, D.; Ordovas, J.M. Metabolic syndrome pathophysiology: The role of adipose tissue. Nutr. Metab. Cardiovasc. Dis. 2007, 17, 125–139. [Google Scholar] [CrossRef]
- Rask-Madsen, C.; Kahn, C.R. Tissue-specific insulin signaling, metabolic syndrome, and cardiovascular disease. Arterioscler. Thromb. Vasc. Biol. 2012, 32, 2052–2059. [Google Scholar]
- Thaler, R.H. Misbehaving: The Making of Behavioral Economics; Ringgold Inc.: Beaverton, OR, USA, 2015; Volume 2. [Google Scholar]
- Marteau, T.M.; Hollands, G.J.; Fletcher, P.C. Changing human behavior to prevent disease: The importance of targeting automatic processes (Report). Science 2012, 337, 1492. [Google Scholar] [CrossRef]
- Rachlin, H. Choice architecture: A review of why nudge: The politics of libertarian paternalism. J. Exp. Anal. Behav. 2015, 104, 198–203. [Google Scholar] [CrossRef]
- Vecchio, R.; Cavallo, C. Increasing healthy food choices through nudges: A systematic review. Food Qual. Prefer. 2019, 78, 103714. [Google Scholar] [CrossRef]
- Rick, S.; Loewenstein, G. Intangibility in intertemporal choice. Philos. Trans. R. Soc. Lond. Ser. B Biol. Sci. 2008, 363, 3813. [Google Scholar] [CrossRef] [PubMed]
- Hollands, G.J.; Shemilt, I.; Marteau, T.M.; Jebb, S.A.; Kelly, M.P.; Nakamura, R.; Suhrcke, M.; Ogilvie, D. Altering micro-environments to change population health behaviour: Towards an evidence base for choice architecture interventions (Report). BMC Public Health 2013, 13, 1218. [Google Scholar] [CrossRef] [PubMed]
- Kahneman, D. Thinking, Fast and Slow; Farrar, Straus and Giroux: New York, NY, USA, 2011. [Google Scholar]
- Hansen, P.G.; Skov, L.R.; Skov, K.L. Making Healthy Choices Easier: Regulation versus Nudging. Annu. Rev. Public Health 2016, 37, 237–251. [Google Scholar] [CrossRef] [PubMed]
- Hummel, D.; Maedche, A. How effective is nudging? A quantitative review on the effect sizes and limits of empirical nudging studies. J. Behav. Exp. Econ. 2019, 80, 47–58. [Google Scholar] [CrossRef]
- Broers, V.J.V.; De Breucker, C.; Van den Broucke, S.; Luminet, O. A systematic review and meta-analysis of the effectiveness of nudging to increase fruit and vegetable choice. Eur. J. Public Health 2017, 27, 912–920. [Google Scholar] [CrossRef] [PubMed]
- Arno, A.; Thomas, S. The efficacy of nudge theory strategies in influencing adult dietary behaviour: A systematic review and meta-analysis. BMC Public Health 2016, 16, 676. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.L.; Buckley, E.; Buckley, J.D.; Bogomolova, S. Nudging healthier food and beverage choices through salience and priming. Evidence from a systematic review. Food Qual. Prefer. 2016, 51, 47–64. [Google Scholar] [CrossRef]
- Bucher, T.; Collins, C.; Rollo, M.E.; McCaffrey, T.A.; De Vlieger, N.; Van Der Bend, D.; Truby, H.; Perez-Cueto, F.J.A. Nudging consumers towards healthier choices: A systematic review of positional influences on food choice. Br. J. Nutr. 2016, 115, 2252. [Google Scholar] [CrossRef]
- Münscher, R.; Vetter, M.; Scheuerle, T. A Review and Taxonomy of Choice Architecture Techniques. J. Behav. Decis. Mak. 2016, 29, 511–524. [Google Scholar] [CrossRef]
- Al-Khudairy, L.; Uthman, O.A.; Walmsley, R.; Johnson, S.; Oyebode, O. Choice architecture interventions to improve diet and/or dietary behaviour by healthcare staff in high-income countries: A systematic review. BMJ Open 2019, 9, e023687. [Google Scholar] [CrossRef]
- Thaler, R.H.; Sunstein, C.R. Nudge: Improving Decisions about Health, Wealth, and Happiness; Yale University Press: New Haven, CT, USA, 2008. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [PubMed]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Anzman-Frasca, S.; Braun, A.C.; Ehrenberg, S.; Epstein, L.H.; Gampp, A.; Leone, L.A.; Singh, A.; Tauriello, S. Effects of a randomized intervention promoting healthy children’s meals on children’s ordering and dietary intake in a quick-service restaurant. Physiol. Behav. 2018, 192, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.F.; Richardson, S.A.; Cluggish, S.A.; Parker, E.; Catalano, P.J.; Rimm, E.B. Effects of choice architecture and chef-enhanced meals on the selection and consumption of healthier school foods: A randomized clinical trial. JAMA Pediatr. 2015, 169, 431–437. [Google Scholar] [CrossRef] [PubMed]
- Greene, K.N.; Gabrielyan, G.; Just, D.R.; Wansink, B. Fruit-Promoting Smarter Lunchrooms Interventions: Results from a Cluster RCT. Am. J. Prev. Med. 2017, 52, 451–458. [Google Scholar] [CrossRef] [PubMed]
- Hollands, G.J.; Cartwright, E.; Pilling, M.; Pechey, R.; Vasiljevic, M.; Jebb, S.A.; Marteau, T.M. Impact of reducing portion sizes in worksite cafeterias: A stepped wedge randomised controlled pilot trial. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 78. [Google Scholar] [CrossRef]
- Vasiljevic, M.; Cartwright, E.; Pilling, M.; Lee, M.M.; Bignardi, G.; Pechey, R.; Hollands, G.J.; Jebb, S.A.; Marteau, T.M. Impact of calorie labelling in worksite cafeterias: A stepped wedge randomised controlled pilot trial. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 41. [Google Scholar] [CrossRef]
- Velema, E.; Vyth, E.L.; Hoekstra, T.; Steenhuis, I.H.M. Nudging and social marketing techniques encourage employees to make healthier food choices: A randomized controlled trial in 30 worksite cafeterias in The Netherlands. Am. J. Clin. Nutr. 2018, 107, 236–246. [Google Scholar] [CrossRef]
- Cole, R.E.; Bukhari, A.S.; Champagne, C.M.; McGraw, S.M.; Hatch, A.M.; Montain, S.J. Performance Nutrition Dining Facility Intervention Improves Special Operations Soldiers’ Diet Quality and Meal Satisfaction. J. Nutr. Educ. Behav. 2018, 50, 993–1004. [Google Scholar] [CrossRef]
- Hubbard, K.L.; Bandini, L.G.; Folta, S.C.; Wansink, B.; Eliasziw, M.; Must, A. Impact of a Smarter Lunchroom intervention on food selection and consumption among adolescents and young adults with intellectual and developmental disabilities in a residential school setting. Public Health Nutr. 2015, 18, 361–371. [Google Scholar] [CrossRef]
- Kroese, F.M.; Marchiori, D.R.; de Ridder, D.T.D. Nudging healthy food choices: A field experiment at the train station. J. Public Health 2016, 38, e133–e137. [Google Scholar] [CrossRef] [PubMed]
- Levy, D.E.; Riis, J.; Sonnenberg, L.M.; Barraclough, S.J.; Thorndike, A.N. Food choices of minority and low-income employees: A cafeteria intervention. Am. J. Prev. Med. 2012, 43, 240–248. [Google Scholar] [CrossRef] [PubMed]
- Lowe, M.R.; Tappe, K.A.; Butryn, M.L.; Annunziato, R.A.; Coletta, M.C.; Ochner, C.N.; Rolls, B.J. An intervention study targeting energy and nutrient intake in worksite cafeterias. Eat. Behav. 2010, 11, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Nikolaou, C.K.; Hankey, C.R.; Lean, M.E. Preventing weight gain with calorie-labeling. Obesity 2014, 22, 2277–2283. [Google Scholar] [CrossRef]
- Olstad, D.L.; Goonewardene, L.A.; McCargar, L.J.; Raine, K.D. Choosing healthier foods in recreational sports settings: A mixed methods investigation of the impact of nudging and an economic incentive. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 6. [Google Scholar] [CrossRef]
- Seward, M.W.; Block, J.P.; Chatterjee, A. A Traffic-Light Label Intervention and Dietary Choices in College Cafeterias. Am. J. Public Health 2016, 106, 1808–1814. [Google Scholar] [CrossRef]
- Thorndike, A.N.; Riis, J.; Sonnenberg, L.M.; Levy, D.E. Traffic-light labels and choice architecture: Promoting healthy food choices. Am. J. Prev. Med. 2014, 46, 143–149. [Google Scholar] [CrossRef]
- Thorndike, A.N.; Sonnenberg, L.; Riis, J.; Barraclough, S.; Levy, D.E. A 2-phase labeling and choice architecture intervention to improve healthy food and beverage choices. Am. J. Public Health 2012, 102, 527–533. [Google Scholar] [CrossRef]
- Van Kleef, E.; Seijdell, K.; Vingerhoeds, M.H.; de Wijk, R.A.; van Trijp, H.C.M. The effect of a default-based nudge on the choice of whole wheat bread. Appetite 2018, 121, 179–185. [Google Scholar] [CrossRef]
- Kleef, E.; Broek, O.; Trijp, H.C.M. Exploiting the Spur of the Moment to Enhance Healthy Consumption: Verbal Prompting to Increase Fruit Choices in a Self-Service Restaurant. Appl. Psychol. Health Well-Being 2015, 7, 149–166. [Google Scholar] [CrossRef]
- Van Kleef, E.; Vrijhof, M.; Polet, I.A.; Vingerhoeds, M.H.; de Wijk, R.A. Nudging children towards whole wheat bread: A field experiment on the influence of fun bread roll shape on breakfast consumption. BMC Public Health 2014, 14, 906. [Google Scholar] [CrossRef] [PubMed]
- Van Kleef, E.; Otten, K.; van Trijp, H. Healthy snacks at the checkout counter: A lab and field study on the impact of shelf arrangement and assortment structure on consumer choices. BMC Public Health 2012, 12, 1072. [Google Scholar] [CrossRef] [PubMed]
- Vermote, M.; Versele, V.; Stok, M.; Mullie, P.; D’Hondt, E.; Deforche, B.; Clarys, P.; Deliens, T. The effect of a portion size intervention on French fries consumption, plate waste, satiety and compensatory caloric intake: An on-campus restaurant experiment. Nutr. J. 2018, 17, 43. [Google Scholar] [CrossRef] [PubMed]
- Loewenstein, G.; Asch, D.A.; Friedman, J.Y.; Melichar, L.A.; Volpp, K.G. Can Behavioural Economics Make Us Healthier? BMJ Br. Med. J. 2012, 344, 23–25. [Google Scholar] [CrossRef]
- Downs, J.; Wisdom, J.; Wansink, B.; Loewenstein, G. Supplementing Menu Labeling With Calorie Recommendations to Test for Facilitation Effects. Am. J. Public Health 2013, 103, 1604–1609. [Google Scholar] [CrossRef] [PubMed]
- Geier, A.B.; Rozin, P.; Doros, G. Unit Bias: A New Heuristic That Helps Explain the Effect of Portion Size on Food Intake. Psychol. Sci. 2006, 17, 521–525. [Google Scholar] [CrossRef]
- Kallbekken, S.; Sælen, H. ‘Nudging’ hotel guests to reduce food waste as a win–win environmental measure. Econ. Lett. 2013, 119, 325–327. [Google Scholar] [CrossRef]
- Hollands, G.; Shemilt, I.; Marteau, T.; Jebb, S.; Lewis, H.; Wei, Y.; Higgins, J.; Ogilvie, D. Portion, package or tableware size for changing selection and consumption of food, alcohol and tobacco. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef]
- Cooper, J.O.; Heron, T.E.; Heward, W.L. Applied Behavior Analysis, 2nd ed.; Pearson/Merrill Prentice Hall: Upper Saddle River, NJ, USA, 2007. [Google Scholar]
- Reducing Consumption of Sugar-Sweetened Beverages to Reduce the Risk of Unhealthy Weight Gain in Adults. Available online: https://www.who.int/elena/titles/bbc/ssbs_adult_weight/en/ (accessed on 27 September 2019).
- Liu, P.J.; Wisdom, J.; Roberto, C.A.; Liu, L.J.; Ubel, P.A. Using Behavioral Economics to Design More Effective Food Policies to Address Obesity. Appl. Econ. Perspect. Policy 2014, 36, 6–24. [Google Scholar] [CrossRef]
- Vandenbroele, J.; Vermeir, I.; Geuens, M.; Slabbinck, H.; Van Kerckhove, A. Nudging to get our food choices on a sustainable track. Proc. Nutr. Soc. 2019. [Google Scholar] [CrossRef]
- Prelec, D.; Loewenstein, G. Decision Making Over Time and Under Uncertainty: A Common Approach. Manag. Sci. 1991, 37, 770–786. [Google Scholar] [CrossRef]


{kind=link}
| PICOS | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Population | Humans | Animal studies |
| Intervention | Nudging interventions aimed at increasing healthy food choice | Lab studies Not food |
| Comparison | ||
| Outcome | Food choice/consumption | Studies that do not report food choice/intake as primary outcome |
| Study design | Randomized and nonrandomized controlled trials (quasi-experimental study) | Abstracts and protocols |
| Intervention Class | Intervention Type |
|---|---|
| Primarily alter properties of objects or stimuli | Ambience—alter aesthetic or atmospheric aspects of the surrounding environment |
| Functional design—design or adapt equipment or function of the environment | |
| Labeling—apply labeling or endorsement information to product or at point-of-choice | |
| Presentation—alter sensory qualities or visual design of the product | |
| Sizing—change size s of the product | |
| Pricing—change price of the product | |
| Primarily alter placement of objects or stimuli | Availability—add behavioral options within a given microenvironment |
| Proximity—make behavioral options easier or harder to engage with, requiring reduced or increased effort | |
| Alter both properties and placement of objects or stimuli | Priming—place incidental cues in the environment to influence a non-conscious behavioral response |
| Prompting—use nonpersonalized information to promote or raise awareness of a behavior |
| Reference | Participants/Site | Results |
|---|---|---|
| RCTs | ||
| Anzman-Frasca et al., 2018 [26] | 58 families with 4–8 year old children, quick-service restaurant | Placemats: ordered more healthy food compared to controls (B = −1.76, 95% CI −3.34, −0.19). No (overall) differences in dietary intake compared to control. |
| Cohen et al., 2015 [27] | Students 1–8 grade urban, low-income districts, school cafeteria | Fruit and vegetable selection increased in smart cafe, however smart café intervention alone had no effect on consumption. |
| Greene et al., 2017 [28] 9 week cluster | Ten middle schools (5–8 grade), cafeteria | Overall, fruit selection increased by 36% (p < 0.001), and fruit consumption increased by 23% (p < 0.017) in the fruit intervention group, compared to controls. |
| Hollands et al., 2018 [29] stepped wedge | Nine worksite cafeterias | No significant change in daily energy purchase when data from all six sites were pooled. |
| Vasiljevic et al., 2018 [30] | Six worksite cafeterias | No overall effect in energy purchase. One site 6.6% reduction (95% CI −12.9 to –0.3, p = 0.044) in energy purchased, however, the association diminished over time. |
| Velema et al., 2018 [31] | Employees | Positive effects on purchases for three of seven products |
| Non RCTs | ||
| Cole et al., 2018 [32] | US Army active duty soldiers, military installation | Intervention associated with increased diet quality and consumption of healthy food. |
| Hubbard et al., 2015 [33] | Students (n 43) 11–22 years with intellectual and developmental disabilities | Smarter lunchroom increased selection (whole grains) and consumption (whole grains, fruit) of healthy food. |
| Kroese et al., 2015 [34] | Travelers, train station snack shops | More healthy (but not fewer unhealthy) products were sold in both nudge conditions. |
| Levy et al., 2012 [35] | Employees who were regular cafeteria patrons (n = 4642) | Labeling decreased unhealthy purchases and increased healthy purchases. |
| Lowe et al., 2010 [36] | Employees, worksite cafeteria | Total energy intake: no difference. Dietary intake improved over study period. |
| Nikolaou et al., 2014 [37] | 120 students, catering | Calorie-labeling associated with a 3.5 kg less weight gain. |
| Olstad et al., 2014 [38] | Patrons, recreational swimming pool | In the full sample, sales of healthy items did not differ across periods. In the subsample, the sale of healthy items increased by 30% when signage + taste testing was implemented (p < 0.01). |
| Seward et al., 2016 [39] | 6 college cafeterias (Harvard University, Cambridge, Massachusetts) | No significant changes (items served) were revealed when intervention sites were compared with controls. |
| Thorndike et al., 2014 [40] | Cafeteria | The traffic-light and choice architecture cafeteria intervention resulted in increased sale of healthier items over 2 years (from 41% to 46%). |
| Thorndike et al., 2012 [41] | Hospital cafeteria | A color-coded labeling intervention improved sales of healthy items and was enhanced by a choice architecture intervention. |
| Van Kleef et al., 2018 [42] | Participants at a Dutch university | Regardless of the topping, when the whole wheat bun was the default option, 94% decided to stick with the default. |
| Van Kleef et al., 2015 [43] | Customers in self-service restaurant during breakfast | The sales increased significant during the verbal prompts intervention periods compared to baseline. |
| Van Kleef et al., 2014 [44] | Children (n = 1113) primary schools in the Netherlands | Consumption of fun-shaped whole wheat bread rolls almost doubled consumption of whole wheat bread (p = 0.001). |
| Van Kleef et al., 2012 [45] | Students | Assortment structure led to higher sales of healthy snacks. |
| Vermote et al., 2018 [46] | University students and employees | Total french fries intake decreased by 9.1%, and total plate waste decreased by 66.4%. No differences in satiety or caloric intake (dietary recall) between baseline and intervention week. |
| Intervention Class | Intervention Type | Anzman-Frasca et al. 2018 [26] | Cohen et al. 2015 [27] | Cole et al. 2018 [32] | Greene et al. 2017 [28] | Hollands et al. 2018 [29] | Hubbard et al. 2014 [33] | Kroese et al. 2015 [34] | Levy et al. 2012 [35] | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| A | B | C | A | B | ||||||||
| Primarily alter properties of objects or stimuli | Ambience | |||||||||||
| Functional design | ||||||||||||
| Labeling | X | X | X | X | X | X | X | |||||
| Presentation | X | X | X | X | ||||||||
| Sizing | X | X | ||||||||||
| Pricing | ||||||||||||
| Primarily alter placement of objects or stimuli | Availability | X | X | X | ||||||||
| Proximity | X | X | X | X | X | X | ||||||
| Alter both properties and placement objects and stimuli | Priming | X | ||||||||||
| Prompting | X | X | X | |||||||||
| Effect | On food choice | N | Y | Y | Y | |||||||
| On dietary consumption Short-term | N | Y | Y | N | Y | Y | Y | |||||
| On dietary consumption Long-term | N | Y | N | Y | ||||||||
| Intervention Class. | Intervention Type | Lowe et al. 2010 [36] | Nikolaou et al. 2014 [37] | Olstad et al. 2014 [38] | Seward et al. 2016 [39] | Thorndike et al. 2014 [40] | Thorndike et al. 2012 [41] | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| A | B | A | B | C | A | B | A | B | ||||
| Primarily alter properties of objects or stimuli | Ambience | |||||||||||
| Functional design | ||||||||||||
| Labeling | X | X | X | X | X | X | X | X | X | X | X | |
| Presentation | X | X | X | |||||||||
| Sizing | ||||||||||||
| Pricing | X | X | ||||||||||
| Primarily alter placement of objects or stimuli | Availability | X | X | X | ||||||||
| Proximity | X | X | ||||||||||
| Alter both properties and placement objects and stimuli | Priming | X | X | |||||||||
| Prompting | ||||||||||||
| Effect | On food choice | Y | Y | N | N | N | N | Y | Y | Y | Y | |
| On dietary consumption Short-term | ||||||||||||
| On dietary consumption Long-term | Y | |||||||||||
| Intervention Class. | Intervention Type | Van Kleef et al. 2018 [42] | Van Kleef et al. 2015 [43] | Van Kleef et al. 2014 [44] | Van Kleef et al. 2012 [45] | Vasiljevic et al. 2018 [30] | Velema et al. 2018 [31] | Vermote et al. 2018 [46] |
|---|---|---|---|---|---|---|---|---|
| Primarily alter properties of objects or stimuli | Ambience | |||||||
| Functional design | ||||||||
| Labeling | X | |||||||
| Presentation | X | X | ||||||
| Sizing | X | X | ||||||
| Pricing | X | |||||||
| Primarily alter placement of objects or stimuli | Availability | X | X | |||||
| Proximity | X | X | X | |||||
| Alter both properties and placement objects and stimuli | Priming | X | ||||||
| Prompting | X | |||||||
| Effect | On food choice | Y | Y | Y | N/Y | Y | N | |
| On dietary consumptionShort-term | Y | Y | ||||||
| On dietary consumptionLong-term |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tørris, C.; Mobekk, H. Improving Cardiovascular Health through Nudging Healthier Food Choices: A Systematic Review. Nutrients 2019, 11, 2520. https://doi.org/10.3390/nu11102520
Tørris C, Mobekk H. Improving Cardiovascular Health through Nudging Healthier Food Choices: A Systematic Review. Nutrients. 2019; 11(10):2520. https://doi.org/10.3390/nu11102520
Chicago/Turabian StyleTørris, Christine, and Hilde Mobekk. 2019. "Improving Cardiovascular Health through Nudging Healthier Food Choices: A Systematic Review" Nutrients 11, no. 10: 2520. https://doi.org/10.3390/nu11102520
APA StyleTørris, C., & Mobekk, H. (2019). Improving Cardiovascular Health through Nudging Healthier Food Choices: A Systematic Review. Nutrients, 11(10), 2520. https://doi.org/10.3390/nu11102520