Narrative Review of Hydration and Selected Health Outcomes in the General Population

 ,
,
Abstract
1. Introduction
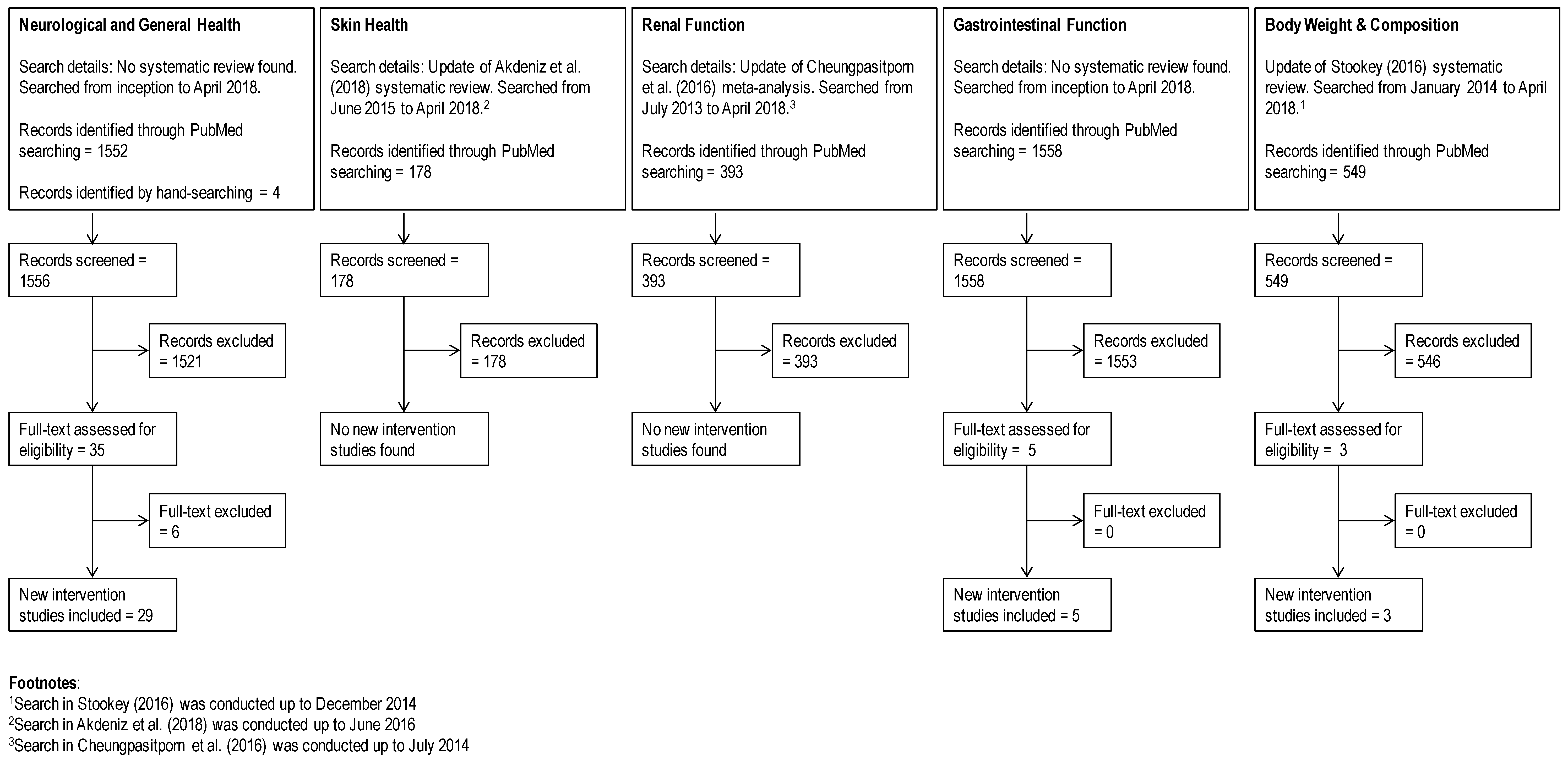
2. Materials and Methods
3. Hydration and Health Outcomes
3.1. Skin Health
3.2. Neurological Function
3.2.1. Cognition, Mood, and Fatigue in Adults
3.2.2. Cognition and Mood in Children
3.2.3. Headache
3.3. Renal Function
3.4. Gastrointestinal Function
3.5. Body Weight and Body Composition
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- European Food Safety Authority (EFSA) Panel on Dietetic Products Nutrition and Allergies (NDA). Scientific Opinion on Dietary Reference Values for water. EFSA J. 2010, 8, 1459–1507. [Google Scholar]
- Food and Nutrition Board, Institute of Medicine (IOM) Panel on Dietary Reference Intakes for Electrolytes and Water. Dietary Reference Intakes for Water, Potassium, Sodium, Chloride, and Sulfate; National Academy of Sciences Press: Washington, DC, USA, 2005.
- Cheuvront, S.N.; Kenefick, R.W. Dehydration: Physiology, assessment, and performance effects. Compr. Physiol. 2014, 4, 257–285. [Google Scholar] [PubMed]
- Thomas, D.R.; Cote, T.R.; Lawhorne, L.; Levenson, S.A.; Rubenstein, L.Z.; Smith, D.A.; Stefanacci, R.G.; Tangalos, E.G.; Morley, J.E.; Dehydration Council. Understanding clinical dehydration and its treatment. J. Am. Med. Dir. Assoc. 2008, 9, 292–301. [Google Scholar] [CrossRef]
- Sawka, M.N.; Cheuvront, S.N.; Kenefick, R.W. Hypohydration and Human Performance: Impact of Environment and Physiological Mechanisms. Sports Med. 2015, 45 (Suppl. 1), S51–S60. [Google Scholar] [CrossRef]
- Bak, A.; Tsiami, A.; Greene, C. Methods of Assessment of Hydration Status and their Usefulness in Detecting Dehydration in the Elderly. Curr. Res. Nutr. Food Sci. 2017, 5, 43–54. [Google Scholar] [CrossRef]
- Cheuvront, S.N.; Ely, B.R.; Kenefick, R.W.; Sawka, M.N. Biological variation and diagnostic accuracy of dehydration assessment markers. Am. J. Clin. Nutr. 2010, 92, 565–573. [Google Scholar] [CrossRef]
- Cheuvront, S.N.; Kenefick, R.W.; Zambraski, E.J. Spot Urine Concentrations Should Not be Used for Hydration Assessment: A Methodology Review. Int. J. Sport Nutr. Exerc. Metab. 2015, 25, 293–297. [Google Scholar] [CrossRef]
- Armstrong, L.E. Hydration assessment techniques. Nutr. Rev. 2005, 63, S40–S54. [Google Scholar] [CrossRef]
- Armstrong, L.E. Assessing hydration status: The elusive gold standard. J. Am. Coll. Nutr. 2007, 26, 575S–584S. [Google Scholar] [CrossRef]
- Cheuvront, S.N. Urinalysis for hydration assessment: An age-old problem. Am. J. Clin. Nutr. 2016, 104, 3–4. [Google Scholar] [CrossRef] [PubMed]
- Fortes, M.B.; Owen, J.A.; Raymond-Barker, P.; Bishop, C.; Elghenzai, S.; Oliver, S.J.; Walsh, N.P. Is this elderly patient dehydrated? Diagnostic accuracy of hydration assessment using physical signs, urine, and saliva markers. J. Am. Med. Dir. Assoc. 2015, 16, 221–228. [Google Scholar] [CrossRef]
- Heavens, K.R.; Charkoudian, N.; O’Brien, C.; Kenefick, R.W.; Cheuvront, S.N. Noninvasive assessment of extracellular and intracellular dehydration in healthy humans using the resistance-reactance-score graph method. Am. J. Clin. Nutr. 2016, 103, 724–729. [Google Scholar] [CrossRef]
- Hooper, L.; Bunn, D.; Jimoh, F.O.; Fairweather-Tait, S.J. Water-loss dehydration and aging. Mech. Ageing Dev. 2014, 136–137, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Hooper, L.; Bunn, D.K.; Abdelhamid, A.; Gillings, R.; Jennings, A.; Maas, K.; Millar, S.; Twomlow, E.; Hunter, P.R.; Shepstone, L.; et al. Water-loss (intracellular) dehydration assessed using urinary tests: How well do they work? Diagnostic accuracy in older people. Am. J. Clin. Nutr. 2016, 104, 121–131. [Google Scholar] [CrossRef] [PubMed]
- Volkert, D.; Beck, A.M.; Cederholm, T.; Cruz-Jentoft, A.; Goisser, S.; Hooper, L.; Kiesswetter, E.; Maggio, M.; Raynaud-Simon, A.; Sieber, C.C.; et al. ESPEN guideline on clinical nutrition and hydration in geriatrics. Clin. Nutr. 2018. [Google Scholar] [CrossRef]
- Warren, J.; Guelinckx, I.; Livingstone, B.; Potischman, N.; Nelson, M.; Foster, E.; Holmes, B. Challenges in the assessment of total fluid intake in children and adolescents: A discussion paper. Eur. J. Nutr. 2018, 57, 43–51. [Google Scholar] [CrossRef]
- Gandy, J. Water intake: Validity of population assessment and recommendations. Eur. J. Nutr. 2015, 54 (Suppl. 2), 11–16. [Google Scholar] [CrossRef]
- El-Sharkawy, A.M.; Sahota, O.; Lobo, D.N. Acute and chronic effects of hydration status on health. Nutr. Rev. 2015, 73 (Suppl. 2), 97–109. [Google Scholar] [CrossRef]
- Kenefick, R.W.; Cheuvront, S.N. Hydration for recreational sport and physical activity. Nutr. Rev. 2012, 70 (Suppl. 2), S137–S142. [Google Scholar] [CrossRef]
- Manz, F. Hydration and disease. J. Am. Coll. Nutr. 2013, 26, 535S–541S. [Google Scholar] [CrossRef]
- Maughan, R.J.; Shirreffs, S.M. Dehydration and rehydration in competitive sport. Scand. J. Med. Sci. Sports 2010, 20 (Suppl. 3), 40–47. [Google Scholar] [CrossRef] [PubMed]
- Maughan, R.J.; Shirreffs, S.M. Development of hydration strategies to optimize performance for athletes in high-intensity sports and in sports with repeated intense efforts. Scand. J. Med. Sci. Sports 2010, 20 (Suppl. 2), 59–69. [Google Scholar] [CrossRef] [PubMed]
- Akdeniz, M.; Tomova-Simitchieva, T.; Dobos, G.; Blume-Peytavi, U.; Kottner, J. Does dietary fluid intake affect skin hydration in healthy humans? A systematic literature review. Skin Res. Technol. 2018, 24, 459–465. [Google Scholar] [CrossRef] [PubMed]
- Benton, D.; Young, H.A. Do small differences in hydration status affect mood and mental performance? Nutr. Rev. 2015, 73 (Suppl. 2), 83–96. [Google Scholar] [CrossRef] [PubMed]
- Masento, N.A.; Golightly, M.; Field, D.T.; Butler, L.T.; van Reekum, C.M. Effects of hydration status on cognitive performance and mood. Br. J. Nutr. 2014, 111, 1841–1852. [Google Scholar] [CrossRef] [PubMed]
- Cheungpasitporn, W.; Rossetti, S.; Friend, K.; Erickson, S.B.; Lieske, J.C. Treatment effect, adherence, and safety of high fluid intake for the prevention of incident and recurrent kidney stones: A systematic review and meta-analysis. J. Nephrol. 2016, 29, 211–219. [Google Scholar] [CrossRef]
- Boilesen, S.N.; Tahan, S.; Dias, F.C.; Melli, L.; de Morais, M.B. Water and fluid intake in the prevention and treatment of functional constipation in children and adolescents: Is there evidence? J. Pediatr. 2017, 93, 320–327. [Google Scholar] [CrossRef]
- Stookey, J.J. Negative, Null and Beneficial Effects of Drinking Water on Energy Intake, Energy Expenditure, Fat Oxidation and Weight Change in Randomized Trials: A Qualitative Review. Nutrients 2016, 8, 19. [Google Scholar] [CrossRef]
- Dabrowska, A.K.; Spano, F.; Derler, S.; Adlhart, C.; Spencer, N.D.; Rossi, R.M. The relationship between skin function, barrier properties, and body-dependent factors. Skin Res. Technol. 2018, 24, 165–174. [Google Scholar] [CrossRef]
- Kolarsick, P.A.J.; Kolarsick, M.A.; Goodwin, C. Anatomy and Physiology of the Skin. J. Dermatol. Nurse Assoc. 2011, 3, 203–213. [Google Scholar] [CrossRef]
- Rittie, L.; Fisher, G.J. Natural and sun-induced aging of human skin. Cold Spring Harb. Perspect. Med. 2015, 5, a015370. [Google Scholar] [CrossRef] [PubMed]
- Palma, L.; Marques, L.T.; Bujan, J.; Rodrigues, L.M. Dietary water affects human skin hydration and biomechanics. Clin. Cosmet. Investig. Dermatol. 2015, 8, 413–421. [Google Scholar] [PubMed]
- Palma, M.L.; Monteiro, C.; Bujan, L.T.M.J.; Rodrigues, L.M. Relationship between the dietary intake of water and skin hydration. Biomed. Biopharm. Res. 2012, 9, 173–181. [Google Scholar] [CrossRef]
- Palma, M.L.; Tavares, L.; Fluhr, J.W.; Bujan, M.J.; Rodrigues, L.M. Positive impact of dietary water on in vivo epidermal water physiology. Skin Res. Technol. 2015, 21, 413–418. [Google Scholar] [CrossRef] [PubMed]
- Mac-Mary, S.; Creidi, P.; Marsaut, D.; Courderot-Masuyer, C.; Cochet, V.; Gharbi, T.; Guidicelli-Arranz, D.; Tondu, F.; Humbert, P. Assessment of effects of an additional dietary natural mineral water uptake on skin hydration in healthy subjects by dynamic barrier function measurements and clinic scoring. Skin Res. Technol. 2006, 12, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Williams, S.; Krueger, N.; Davids, M.; Kraus, D.; Kerscher, M. Effect of fluid intake on skin physiology: Distinct differences between drinking mineral water and tap water. Int. J. Cosmet. Sci. 2007, 29, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Edmonds, C.J.; Crosbie, L.; Fatima, F.; Hussain, M.; Jacob, N.; Gardner, M. Dose-response effects of water supplementation on cognitive performance and mood in children and adults. Appetite 2017, 108, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Trinies, V.; Chard, A.N.; Mateo, T.; Freeman, M.C. Effects of Water Provision and Hydration on Cognitive Function among Primary-School Pupils in Zambia: A Randomized Trial. PLoS ONE 2016, 11, e0150071. [Google Scholar] [CrossRef] [PubMed]
- Perry, C.S., 3rd; Rapinett, G.; Glaser, N.S.; Ghetti, S. Hydration status moderates the effects of drinking water on children’s cognitive performance. Appetite 2015, 95, 520–527. [Google Scholar] [CrossRef]
- Booth, P.; Edmonds, C.J. Water supplementation improves visual attention and fine motor skills in schoolchildren. Educ. Health 2012, 30, 75–79. [Google Scholar]
- Fadda, R.; Rapinett, G.; Grathwohl, D.; Parisi, M.; Fanari, R.; Calo, C.M.; Schmitt, J. Effects of drinking supplementary water at school on cognitive performance in children. Appetite 2012, 59, 730–737. [Google Scholar] [CrossRef] [PubMed]
- Kempton, M.J.; Ettinger, U.; Foster, R.; Williams, S.C.; Calvert, G.A.; Hampshire, A.; Zelaya, F.O.; O’Gorman, R.L.; McMorris, T.; Owen, A.M.; et al. Dehydration affects brain structure and function in healthy adolescents. Hum. Brain Mapp. 2011, 32, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Edmonds, C.J.; Jeffes, B. Does having a drink help you think? 6–7-Year-old children show improvements in cognitive performance from baseline to test after having a drink of water. Appetite 2009, 53, 469–472. [Google Scholar] [CrossRef] [PubMed]
- Edmonds, C.J.; Burford, D. Should children drink more water?: The effects of drinking water on cognition in children. Appetite 2009, 52, 776–779. [Google Scholar] [CrossRef] [PubMed]
- Benton, D.; Burgess, N. The effect of the consumption of water on the memory and attention of children. Appetite 2009, 53, 143–146. [Google Scholar] [CrossRef] [PubMed]
- Stachenfeld, N.S.; Leone, C.A.; Mitchell, E.S.; Freese, E.; Harkness, L. Water intake reverses dehydration associated impaired executive function in healthy young women. Physiol. Behav. 2018, 185, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Benton, D.; Jenkins, K.T.; Watkins, H.T.; Young, H.A. Minor degree of hypohydration adversely influences cognition: A mediator analysis. Am. J. Clin. Nutr. 2016, 104, 603–612. [Google Scholar] [CrossRef]
- Pross, N.; Demazieres, A.; Girard, N.; Barnouin, R.; Metzger, D.; Klein, A.; Perrier, E.; Guelinckx, I. Effects of changes in water intake on mood of high and low drinkers. PLoS ONE 2014, 9, e94754. [Google Scholar] [CrossRef]
- Edmonds, C.J.; Crombie, R.; Ballieux, H.; Gardner, M.R.; Dawkins, L. Water consumption, not expectancies about water consumption, affects cognitive performance in adults. Appetite 2013, 60, 148–153. [Google Scholar] [CrossRef] [PubMed]
- Lindseth, P.D.; Lindseth, G.N.; Petros, T.V.; Jensen, W.C.; Caspers, J. Effects of hydration on cognitive function of pilots. Mil. Med. 2013, 178, 792–798. [Google Scholar] [CrossRef] [PubMed]
- Edmonds, C.J.; Crombie, R.; Gardner, M.R. Subjective thirst moderates changes in speed of responding associated with water consumption. Front. Hum. Neurosci. 2013, 7, 363. [Google Scholar] [CrossRef] [PubMed]
- Ely, B.R.; Sollanek, K.J.; Cheuvront, S.N.; Lieberman, H.R.; Kenefick, R.W. Hypohydration and acute thermal stress affect mood state but not cognition or dynamic postural balance. Eur. J. Appl. Physiol. 2013, 113, 1027–1034. [Google Scholar] [CrossRef] [PubMed]
- Pross, N.; Demazieres, A.; Girard, N.; Barnouin, R.; Santoro, F.; Chevillotte, E.; Klein, A.; Le Bellego, L. Influence of progressive fluid restriction on mood and physiological markers of dehydration in women. Br. J. Nutr. 2013, 109, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, L.E.; Ganio, M.S.; Casa, D.J.; Lee, E.C.; McDermott, B.P.; Klau, J.F.; Jimenez, L.; Le Bellego, L.; Chevillotte, E.; Lieberman, H.R. Mild dehydration affects mood in healthy young women. J. Nutr. 2012, 142, 382–388. [Google Scholar] [CrossRef]
- Ganio, M.S.; Armstrong, L.E.; Casa, D.J.; McDermott, B.P.; Lee, E.C.; Yamamoto, L.M.; Marzano, S.; Lopez, R.M.; Jimenez, L.; Le Bellego, L.; et al. Mild dehydration impairs cognitive performance and mood of men. Br. J. Nutr. 2011, 106, 1535–1543. [Google Scholar] [CrossRef] [PubMed]
- Kempton, M.J.; Ettinger, U.; Schmechtig, A.; Winter, E.M.; Smith, L.; McMorris, T.; Wilkinson, I.D.; Williams, S.C.; Smith, M.S. Effects of acute dehydration on brain morphology in healthy humans. Hum. Brain Mapp. 2009, 30, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Petri, N.M.; Dropulic, N.; Kardum, G. Effects of voluntary fluid intake deprivation on mental and psychomotor performance. Croat. Med. J. 2006, 47, 855–861. [Google Scholar]
- Szinnai, G.; Schachinger, H.; Arnaud, M.J.; Linder, L.; Keller, U. Effect of water deprivation on cognitive-motor performance in healthy men and women. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2005, 289, R275–R280. [Google Scholar] [CrossRef] [PubMed]
- Shirreffs, S.M.; Merson, S.J.; Fraser, S.M.; Archer, D.T. The effects of fluid restriction on hydration status and subjective feelings in man. Br. J. Nutr. 2004, 91, 951–958. [Google Scholar] [CrossRef] [PubMed]
- Neave, N.; Scholey, A.B.; Emmett, J.R.; Moss, M.; Kennedy, D.O.; Wesnes, K.A. Water ingestion improves subjective alertness, but has no effect on cognitive performance in dehydrated healthy young volunteers. Appetite 2001, 37, 255–256. [Google Scholar] [CrossRef] [PubMed]
- Rogers, P.J.; Kainth, A.; Smit, H.J. A drink of water can improve or impair mental performance depending on small differences in thirst. Appetite 2001, 36, 57–58. [Google Scholar] [CrossRef] [PubMed]
- Gopinathan, P.M.; Pichan, G.; Sharma, V.M. Role of dehydration in heat stress-induced variations in mental performance. Arch. Environ. Health 1988, 43, 15–17. [Google Scholar] [CrossRef] [PubMed]
- Sharma, V.M.; Sridharan, K.; Pichan, G.; Panwar, M.R. Influence of heat-stress induced dehydration on mental functions. Ergonomics 1986, 29, 791–799. [Google Scholar] [CrossRef] [PubMed]
- Spigt, M.; Weerkamp, N.; Troost, J.; van Schayck, C.P.; Knottnerus, J.A. A randomized trial on the effects of regular water intake in patients with recurrent headaches. Fam. Pract. 2012, 29, 370–375. [Google Scholar] [CrossRef] [PubMed]
- Spigt, M.G.; Kuijper, E.C.; Schayck, C.P.; Troost, J.; Knipschild, P.G.; Linssen, V.M.; Knottnerus, J.A. Increasing the daily water intake for the prophylactic treatment of headache: A pilot trial. Eur. J. Neurol. 2005, 12, 715–718. [Google Scholar] [CrossRef] [PubMed]
- Alelign, T.; Petros, B. Kidney Stone Disease: An Update on Current Concepts. Adv. Urol. 2018, 2018, 3068365. [Google Scholar] [CrossRef]
- Dion, M.; Ankawi, G.; Chew, B.; Paterson, R.; Sultan, N.; Hoddinott, P.; Razvi, H. CUA guideline on the evaluation and medical management of the kidney stone patient—2016 update. Can. Urol. Assoc. J. 2016, 10, E347–E358. [Google Scholar] [CrossRef]
- Pearle, M.S.; Goldfarb, D.S.; Assimos, D.G.; Curhan, G.; Denu-Ciocca, C.J.; Matlaga, B.R.; Monga, M.; Penniston, K.L.; Preminger, G.M.; Turk, T.M.; et al. Medical management of kidney stones: AUA guideline. J. Urol. 2014, 192, 316–324. [Google Scholar] [CrossRef]
- Borghi, L.; Meschi, T.; Amato, F.; Briganti, A.; Novarini, A.; Giannini, A. Urinary volume, water and recurrences in idiopathic calcium nephrolithiasis: A 5-year randomized prospective study. J. Urol. 1996, 155, 839–843. [Google Scholar] [CrossRef]
- Sarica, K.; Inal, Y.; Erturhan, S.; Yagci, F. The effect of calcium channel blockers on stone regrowth and recurrence after shock wave lithotripsy. Urol. Res. 2006, 34, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Leiper, J.B. Fate of ingested fluids: Factors affecting gastric emptying and intestinal absorption of beverages in humans. Nutr. Rev. 2015, 73 (Suppl. 2), 57–72. [Google Scholar] [CrossRef] [PubMed]
- Anti, M.; Pignataro, G.; Armuzzi, A.; Valenti, A.; Iascone, E.; Marmo, R.; Lamazza, A.; Pretaroli, A.R.; Pace, V.; Leo, P.; et al. Water supplementation enhances the effect of high-fiber diet on stool frequency and laxative consumption in adult patients with functional constipation. Hepatogastroenterology 1998, 45, 727–732. [Google Scholar] [PubMed]
- Klauser, A.G.; Beck, A.; Schindlbeck, N.E.; Muller-Lissner, S.A. Low fluid intake lowers stool output in healthy male volunteers. Z. Gastroenterol. 1990, 28, 606–609. [Google Scholar] [PubMed]
- Chung, B.D.; Parekh, U.; Sellin, J.H. Effect of increased fluid intake on stool output in normal healthy volunteers. J. Clin. Gastroenterol. 1999, 28, 29–32. [Google Scholar] [CrossRef] [PubMed]
- Ziegenhagen, D.J.; Tewinkel, G.; Kruis, W.; Herrmann, F. Adding more fluid to wheat bran has no significant effects on intestinal functions of healthy subjects. J. Clin. Gastroenterol. 1991, 13, 525–530. [Google Scholar] [CrossRef]
- van Nieuwenhoven, M.A.; Vriens, B.E.; Brummer, R.J.; Brouns, F. Effect of dehydration on gastrointestinal function at rest and during exercise in humans. Eur. J. Appl. Physiol. 2000, 83, 578–584. [Google Scholar] [CrossRef]
- Akers, J.D.; Cornett, R.A.; Savla, J.S.; Davy, K.P.; Davy, B.M. Daily self-monitoring of body weight, step count, fruit/vegetable intake, and water consumption: A feasible and effective long-term weight loss maintenance approach. J. Acad. Nutr. Diet. 2012, 112, 685–692.e2. [Google Scholar] [CrossRef]
- Dennis, E.A.; Dengo, A.L.; Comber, D.L.; Flack, K.D.; Savla, J.; Davy, K.P.; Davy, B.M. Water consumption increases weight loss during a hypocaloric diet intervention in middle-aged and older adults. Obesity 2010, 18, 300–307. [Google Scholar] [CrossRef]
- Muckelbauer, R.; Libuda, L.; Clausen, K.; Toschke, A.M.; Reinehr, T.; Kersting, M. Promotion and provision of drinking water in schools for overweight prevention: Randomized, controlled cluster trial. Pediatrics 2009, 123, e661–e667. [Google Scholar] [CrossRef]
- Stookey, J.D.; Del Toro, R.; Hamer, J.; Medina, A.; Higa, A.; Ng, V.; TinajeroDeck, L.; Juarez, L. Qualitative and/or quantitative drinking water recommendations for pediatric obesity treatment. J. Obes. Weight Loss Ther. 2014, 4, 232. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Cordero, S.; Popkin, B.M. Impact of a Water Intervention on Sugar-Sweetened Beverage Intake Substitution by Water: A Clinical Trial in Overweight and Obese Mexican Women. Ann. Nutr. Metab. 2015, 66 (Suppl. 3), 22–25. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Cordero, S.; Barquera, S.; Rodriguez-Ramirez, S.; Villanueva-Borbolla, M.A.; Gonzalez de Cossio, T.; Dommarco, J.R.; Popkin, B. Substituting water for sugar-sweetened beverages reduces circulating triglycerides and the prevalence of metabolic syndrome in obese but not in overweight Mexican women in a randomized controlled trial. J. Nutr. 2014, 144, 1742–1752. [Google Scholar] [CrossRef] [PubMed]
- Corney, R.A.; Horina, A.; Sunderland, C.; James, L.J. Effect of hydration status and fluid availability on ad-libitum energy intake of a semi-solid breakfast. Appetite 2015, 91, 399–404. [Google Scholar] [CrossRef] [PubMed]
- Parretti, H.M.; Aveyard, P.; Blannin, A.; Clifford, S.J.; Coleman, S.J.; Roalfe, A.; Daley, A.J. Efficacy of water preloading before main meals as a strategy for weight loss in primary care patients with obesity: RCT. Obesity 2015, 23, 1785–1791. [Google Scholar] [CrossRef] [PubMed]
- Wong, J.M.W.; Ebbeling, C.B.; Robinson, L.; Feldman, H.A.; Ludwig, D.S. Effects of Advice to Drink 8 Cups of Water per Day in Adolescents With Overweight or Obesity: A Randomized Clinical Trial. JAMA Pediatr. 2017, 171, e170012. [Google Scholar] [CrossRef] [PubMed]
- Chang, T.; Ravi, N.; Plegue, M.A.; Sonneville, K.R.; Davis, M.M. Inadequate Hydration, BMI, and Obesity Among US Adults: NHANES 2009–2012. Ann. Fam. Med. 2016, 14, 320–324. [Google Scholar] [CrossRef]
- Kenney, E.L.; Long, M.W.; Cradock, A.L.; Gortmaker, S.L. Prevalence of Inadequate Hydration among US Children and Disparities by Gender and Race/Ethnicity: National Health and Nutrition Examination Survey, 2009–2012. Am. J. Public Health 2015, 105, e113–e118. [Google Scholar] [CrossRef]
- Silva, C.L.; Topgaard, D.; Kocherbitov, V.; Sousa, J.J.; Pais, A.A.; Sparr, E. Stratum corneum hydration: Phase transformations and mobility in stratum corneum, extracted lipids and isolated corneocytes. Biochim. Biophys. Acta 2007, 1768, 2647–2659. [Google Scholar] [CrossRef]
- Wittbrodt, M.T.; Millard-Stafford, M. Dehydration Impairs Cognitive Performance: A Meta-analysis. Med. Sci. Sports Exerc. 2018, 50, 2360–2368. [Google Scholar] [CrossRef]
- Cunningham, P.; Noble, H.; Al-Modhefer, A.K.; Walsh, I. Kidney stones: Pathophysiology, diagnosis and management. Br. J. Nurs. 2016, 25, 1112–1116. [Google Scholar] [CrossRef] [PubMed]
- Masereeuw, R.; Russel, F.G. Mechanisms and clinical implications of renal drug excretion. Drug Metab. Rev. 2001, 33, 299–351. [Google Scholar] [CrossRef]
- Klein, A.V.; Kiat, H. Detox diets for toxin elimination and weight management: A critical review of the evidence. J. Hum. Nutr. Diet. 2015, 28, 675–686. [Google Scholar] [CrossRef]
- Khan, L. Constipation Management in Pediatric Primary Care. Pediatr. Ann. 2018, 47, e180–e184. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Rao, S. Constipation: Pathophysiology and Current Therapeutic Approaches. Handb. Exp. Pharmacol. 2017, 239, 59–74. [Google Scholar]
- Thornton, S.N. Increased Hydration Can Be Associated with Weight Loss. Front. Nutr. 2016, 3, 18. [Google Scholar] [CrossRef] [PubMed]
- Drewnowski, A.; Rehm, C.D.; Constant, F. Water and beverage consumption among adults in the United States: Cross-sectional study using data from NHANES 2005-2010. BMC Public Health 2013, 13, 1068. [Google Scholar] [CrossRef] [PubMed]
- Stachenfeld, N.S. Sex hormone effects on body fluid regulation. Exerc. Sport Sci. Rev. 2008, 36, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Stachenfeld, N.S. Hormonal changes during menopause and the impact on fluid regulation. Reprod. Sci. 2014, 21, 555–561. [Google Scholar] [CrossRef]
- Stookey, J.D. High prevalence of plasma hypertonicity among community-dwelling older adults: Results from NHANES III. J. Am. Diet. Assoc. 2005, 105, 1231–1239. [Google Scholar] [CrossRef]
- Maughan, R.J. Hydration, morbidity, and mortality in vulnerable populations. Nutr. Rev. 2012, 70 (Suppl. 2), S152–S155. [Google Scholar] [CrossRef] [PubMed]
- Stotts, N.A.; Hopf, H.W. The link between tissue oxygen and hydration in nursing home residents with pressure ulcers: Preliminary data. J. Wound Ostomy Cont. Nurs. 2003, 30, 184–190. [Google Scholar] [CrossRef]


{kind=link}
| Citation | Review Type/ Reporting Quality | Description | Key Findings/ Conclusions |
|---|---|---|---|
| Skin Health | |||
| Akdeniz et al., 2018 [24] | Systematic review Met 17 of 19 required PRISMA items for systematic review. 1 Fulfilled 4 of 13 required AMSTAR 2 items for systematic review.2 |
|
|
| Neurological Function | |||
| Benton and Young, 2015 [25] | Narrative review |
|
|
| Masento et al., 2014 [26] | Narrative review |
|
|
| Renal Function | |||
| Cheungpasitporn et al., 2016 [27] | Systematic review/Meta-analysis Met 22 of 24 required PRISMA items for meta-analysis.1 Met 10 of 16 required AMSTAR 2 items for meta-analysis. 2 |
|
|
| Gastrointestinal Function | |||
| Boilesen et al., 2017 [28] | Narrative review |
|
|
| Body Weight and Body Composition | |||
| Stookey, 2016 [29] | Qualitative review |
|
|
| Citation | Objective | Population | Design | Intervention/Control | Summary/Conclusion |
|---|---|---|---|---|---|
| Neurological Function in Children | |||||
| Edmonds et al., 2017 (Children) [38] | Examine dose–response effects of water on cognition in children | 60 children (58% F) ages 7–10 years. | Acute RCT | Children consumed the assigned water 20 min prior to cognition tasks:
| No significant time × volume interaction for visual attention (Letter cancellation task) and working memory (digit span task). Significant increase in pre- and post-water scores for visual attention for 25 mL and 300 mL with t-test analysis. No significant results on memory task. |
| Trinies et al., 2016 [39] | Assess the role of hydration on cognition in children living in hot, low income environments | 279 children in grades 3–6 in schools across Eastern Zambia. | Parallel RCT | Students in area where water was not nearby were provided:
| Afternoon hypohydration, assessed by mean urine specific gravity, was lower in children provided water (9.8%) compared to the control children (67.2%). No significant difference between groups in visual memory (indirect image difference), short-term memory (forward digit recall, and reverse digit recall), or visuomotor skills (line trace). Two visual attention tests were included, with a significant difference in one visual attention test (direct image difference; p = 0.05), but not the other (letter cancellation). When grouped by urine specific gravity (≥1.020 as cut-off for hypohydration) no significant difference was observed. |
| Perry et al., 2015 [40] | Assessed whether the benefit of drinking water on working memory and attention depends upon children’s hydration status and renal response. | 52 children (50% F) age 9–12 y. | Acute crossover | All subjects performed a baseline cognition test after standard breakfast (included 25 mL water and 250 mL skim milk). During the water intervention, subjects consumed 250 mL water, followed by cognition test battery (short-term effect), and another 500 mL water over the next 3 h, followed by another cognition test batter (long-term effect). During the control intervention, no additional fluid beyond breakfast was provided. | Based on osmolality, 65% of the population was dehydrated prior to breakfast intake, with 35% remaining dehydrated at the end of the control test period compared to 3.8% at the end of the active (water) period. Children who exhibited smaller decreases in urine osmolality following water intake (i.e., had underlying hypohydration) performed significantly better on the water day compared to the control day on the digit-span task (verbal memory) and pair-cancellation task (sustained attention). Children who exhibited larger decreases in urine osmolality following water intake performed better on the control day compared to the water day. No significant effects on working memory (tested using delayed match-to-sample task). |
| Booth et al., 2012 [41] | Investigate the effects of water supplementation on visual attention and motor performance in schoolchildren. | 15 students (age 8–9 y) | Acute RCT | Children were provided no water or 250 mL bottle of water and instructed to drink as much or as little 20 min prior to cognition test and mood ratings. | When offered water, children drank an average of 168 mL water. Children performed better on tasks testing visual attention and fine motor skills (Letter Cancellation Task and Wii Ravin Rabbids game) after water consumption compared to no water consumption. There were no differences for tasks testing gross motor skills (Ball Catching and Step Ups) and happiness rating. |
| Fadda et al., 2012 [42] | Assessed the effect of drinking water on cognitive performance, fatigue, and vigor in school children. | 168 children age 9–11 y living in a hot climate (Southern Italy). | Parallel RCT | Control group (n = 75, 35/40 M/F) and a supplemental water group (n = 93, 47/46 M/F). The water group received 1 L of additional water for the day; the control group did not receive additional water. | Based on urine osmolality measurement, 84% of children were dehydrated (morning Uosm >800) at the start of the school day. Drinking water benefited short-term memory (auditory number span) and verbal reasoning (verbal analogies) but not selective attention (Deux de Barrage). No significant differences were found in POMS fatigue or confusion scores. Significant beneficial relationship between hydration and vigor was noted. |
| Kempton et al., 2011 [43] | Investigate the effects of dehydration on brain function | 10 healthy adolescents (50% females), average age 16.8 y | Acute RCT | Subjects consumed 500 mL of water the evening prior to test day. On test day, subjects consumed a further 500 mL of water 1 h before a 90-min thermal exercise dehydration protocol (with thick and multilayered clothing) or a 90-min non-thermal control exercise protocol. | Subjects lost an average 1.65% body mass during the thermal dehydration exercise compared to 0.53% during the non-thermal control exercise. Hypohydration resulted in increased fronto-parietal brain activations during a task of executive function, lateral ventricular volume, and mental and physical sedation, but did not affect results of the executive function task. |
| Edmonds and Jeffes, 2009 [44] | Assess the effect of water consumption on cognition in children. | 23 children (61% female) age 6–7 y from one classroom. | Acute parallel | Children were separated into water group (n = 11, 4/7 M/F) or no water (n = 12, 5/7 M/F). Children were tested for baseline function as a group, then the no water group left the room and those remaining were provided 500 mL water to drink ad libitum. The post-consumption test occurred 45 min later. | Significant positive changes were reported for children consuming water on the thirst and happiness ratings, as well as the visual attention and visual search tests. Visual memory and motor performances were not significantly different. Although there was an effect on mood, the authors caution making strong conclusions based on this finding due to the lack of significance on follow-up testing. |
| Edmonds and Burford, 2009 [45] | Assessed the effect of a drink of water on children’s cognitive function. | 58 children, age 7–9 y. | Acute RCT | Control (no water) group (n = 30, 15/15 M/F) and a water group (n = 28, 11/17 M/F). Children were tested at baseline and 20 min later. Children in the water group were provided with 250 mL of water between tests. | Children who drank additional water rated themselves as significantly less thirsty and performed better on letter cancellation task (visual attention) and spot the difference task (visual attention and memory). There were no differences between groups for story memory and visuomotor tracking tasks. |
| Benton and Burgess, 2009 [46] | Examined the influence of giving additional water to school children on measures of memory and attention. | 40 children (45% female) in a school in South Wales, average age 8 y. | Acute RCT | Children were tested in the afternoon after receiving 300 mL of water or no water at the beginning of the mid-afternoon break, with testing occurring 20–35 min after consumption. | Immediate memory (recall of objects) was significantly better from children after consumption of water. The ability to sustain attention (paradigm of Shakow) was not significantly influenced by water consumption. |
| Neurological Function in Adults | |||||
| Stachenfeld et al., 2018 [47] | Investigate whether mild dehydration would adversely impact executive function tasks, with no effects on simple tasks, and that these changes in cognitive performance are independent of changes in emotion | 12 healthy women (age 18–34 y) | Crossover RCT | Subjects performed cognitive tasks and rated mood under three difference hydration conditions:
| Water deprivation increased plasma osmolality from ~283 to 287 Uosm/kg H2O. Water deprivation increased errors for tests for visual memory or working memory (Continuous Paired Associate Learning) and executive function and spatial problem solving (Groton Maze Learning Test) when compared to control and euhydration conditions. No hydration effect on simple reaction time, choice reaction time, visual attention, motor speed, visual motor function, visual learning, working memory assessed with One and Two Back Tasks, and cognitive flexibility. There were no changes in mood outcomes. |
| Edmonds et al., 2017 (Adults) [38] | Evaluate the dose–response effect of water on cognitive performance and mood in adults | 96 adults, average age 21 y. | Acute RCT | Acute consumption of 300 mL water (n = 32, 10/22 M/F), 25 mL water (n = 32, 7/25 M/F), and 0 mL water (n = 32, 11/21 M/F) 20 min before cognition tasks. | Significant time × volume interaction for visual attention (letter cancellation task), whereby scores increased from baseline in a dose-dependent manner, with 0 mL having the lowest increase and 300 mL having the highest increase. Significant time × volume interaction for working memory (digit span task). Only the increase in the 300 mL group was significant for the memory test. |
| Benton et al., 2016 [48] | Assess whether a loss of 1% of body mass due to hypohydration adversely influenced cognition, and examined the possible underlying mechanisms | 101 healthy adults. Water group aged 18–30 y; control group age 18–31 y. | Acute RCT | Water consumption group (n = 51, 26/25 M/F) and no water consumption group (n = 50, 26/24 M/F). Subjects were exposed to 30 °C for 4 h, during which they either did or did not drink 300 mL pure water. | Subjects in the no water group had greater body mass loss (−0.22% vs. +0.05%) and increase in osmolality (−117.24, no water vs. water). At 90 and 180 min, water consumption resulted in better episodic memory (word list recall task) and focused attention (arrow flanker test). Energy and depression ratings were unaffected by water consumption. Anxiety rating decreased with water consumption at 90 min, but not 180 min. |
| Pross et al., 2014 [49] | Evaluate effects of changing water intake on mood and sensation in habitual high- and low-water consumers. | 52 subjects (79% F) average age 25 y were selected based on daily fluid consumption: Low <1.2 L/d (average 1.0 L/d) High ≥2 L/d (average 2.5 L/d) | Open label 2-d intervention | Intervention conducted in controlled setting (inpatient facility) with meals (details not provided) and sleep/wake cycles standardized. Baseline data were collected during days 1–2, and intervention conducted days 3–5. Defined drinking programs were:
| Increasing water intake decreased urine osmolality from mean of 841 to 392 mOsm/kg. Decreasing water intake increased urine osmolality from mean of 222 to 720 mOsm/kg. At baseline, POMS ratings were comparable except for thirst and some depression scores. Restricting water intake in high-consumers resulted in a significant increase in thirst and decrease in contentedness, calmness, positive emotions, and vigor/activity scores. Increasing water intake in low consumers significantly decreased fatigue/inertia, confusion/bewilderment, and thirst scores, with a non-significant decrease in sleepiness. |
| Edmonds et al., 2013 [50] | Explore the effects of water and knowledge of aims of study on cognitive performance | 44 adults age 18–57 y. | Acute RCT |
| There were no differences in the amount of water consumed (out of 200 mL) between the water + expectancy vs. the water + no expectancy groups. Visual attention (letter cancellation task) improved with water consumption, regardless of expectancy condition. Working memory (backwards digit span task) was better in the no water groups vs. water groups. There was no effect of expectancy condition. Water and expectancy condition did not affect scores for simple reaction time or mood assessed using VAS. Water consumption effects on visual attention are due to the physiological effects of water, rather than expectancies about the effects of drinking water. |
| Lindseth et al., 2013 [51] | Examine the effect of fluid intake and possible dehydration on cognitive flight performance of pilots | 40 healthy pilots (average age 20.3 y) enrolled during the third term of the commercial phase of their collegiate aviation program at a Midwestern university | Crossover RCT | High- or low-fluid controlled diets (≥80 oz/d vs. ≤40 oz/d or ≥2.4 L/d vs. ≤1.2 L/d) for 2 weeks, with 2 week washout. | No difference between high and low fluid diets for flight performance (General Aviation Trainer full-motion flight simulator), spatial cognition (Vandenberg Mental Rotation Test), and memory (Sternberg Item Recognition Test). Scores for flight performance and spatial cognition were poorer for pilots who were dehydrated (1–3% body mass loss). Hypohydration did not affect memory. |
| Edmonds et al., 2013 [52] | Investigate the effect of water supplementation on cognitive performance and mood in adults, and whether subjective thirst moderates the relation between water supplementation and cognitive performance and mood | 34 healthy adults (74% F), age 20–53 y. | Acute RCT | Water group consumed 0.5–1 L water prior to cognitive and mood testing. The no water group was not provided water prior to testing. | Water supplementation had a positive effect on simple reaction time, whereby those who were thirsty and did not have water performed more poorly compared to those who were not thirsty. However, the poorer performance of thirsty subjects was “normalized” when they were provided water. No significant results for visual memory, visual learning, immediate and delayed memory, comprehension, learning, acquisition and reversal, sustained attention, forced choice recognition, and choice reaction time. Participants rated themselves as more tired and tense if they were thirsty, and consumption of water did not affect mood ratings. |
| Ely et al., 2013 [53] | Determine the impact of acute exposure to a range of ambient temperatures (10–40 °C) in euhydration and hypohydration states on cognition, mood and dynamic balance | 32 men (average age 22 y) | Acute RCT | 4 groups (n = 8/group) matched for aerobic fitness. Each group went through euhydration and hypohydration conditions in a crossover fashion, separated by 1 week. All subjects went through a dehydration exercise regimen. For the euhydration condition, subjects were provided water to restore body weight to their pre-dehydration body weight. For the hypohydration condition, water was only provided to ensure that body mass loss did not exceed −4.5%. Following the exercise + water consumption (if needed), subjects rested in preassigned temperatures and performed cognition tasks. | Sustained attention, choice reaction time, short-term spatial memory, and grammar-based logical reasoning were unaffected by hypohydration (4.0–4.2%body mass loss) or ambient temperature during cognition testing. Hypohydration (4.0–4.2%body mass loss) led to increased total mood disturbance, with increased ratings of anger/hostility, confusion/bewilderment, depression/dejection, and fatigue, without affecting vigor/activity and tension/anxiety. Temperature did not affect mood. |
| Pross et al., 2013 [54] | Assess no drink allowed for 23–24 h | 20 healthy women, average age 20 y | Crossover RCT | Subjects completed the following:
| Urine specific gravity significantly increased and color significantly darkened at 9 h and remained so throughout 24 h, but plasma osmolality was unchanged. Generally higher sleepiness and lower alertness scores throughout, but significant at 14–16 h with no fluids. Significantly greater fatigue and lower vigor ratings with no fluids. No significant differences on sleep parameters. |
| Armstrong et al., 2012 [55] | Investigate if mild dehydration would primarily affect mood and symptoms of dehydration and have modest effects on cognitive function. | 25 women, average age 23 y. | Acute RCT |
| While in the dehydration arms, subjects lost ≥1% body mass (mean loss of 1.36%) Overall, sustained attention, choice reaction time, working memory, short-term memory, and logical reasoning were unaffected by dehydration. Subjects reported increased anger-hostility, increased fatigue-inertia, and decreased vigor-activity when dehydrated. Total mood disturbance score was worse with dehydration. Subjects also reported greater perceived task difficulty, lower concentration, and increased headache with dehydration. |
| Ganio et al., 2011 [56] | Assess the effects of mild dehydration on cognitive performance and mood of young males | 26 men, average age 20 y | Acute RCT |
| While in the dehydration arms, subjects lost ≥1% body mass (mean loss 1.59% body mass). Dehydration resulted in lower scores for attention (scanning visual vigilance task) and working memory (matching to sample task) and increased tension/anxiety and fatigue/inertia. No significant results for visual reaction time, choice reaction time, short-term memory, and logical reasoning. |
| Kempton et al., 2009 [57] | Investigate whether acute dehydration would lead to a reduction in brain volume and subtle regional changes in brain morphology such as ventricular expansion | 7 healthy men (mean age 23.8 y) | Single arm | Subjects went through a thermal-exercise dehydration protocol to decrease body mass by 2–3%. Subjects received brain MRI scan before and after the dehydration protocol. | Average body mass loss due to dehydration protocol was 2%. Dehydration led to expansion of the ventricular system with the largest change occurring in the left lateral ventricle, without changes in total brain volume. |
| Petri et al., 2006 [58] | Measure the deterioration in mental and physical performance and dynamics of its onset during voluntary 24-h fluid intake deprivation. | 10 healthy men, age 21–30 y. | Open label 24 h | Testing occurred over 2 d, every 3 h throughout the days for a total of 7 time points a day. During the first 24 h, subjects were allowed to drink freely. From 25–48 h, subjects were not allowed to drink. Daily water intake in food was 500 g. The environmental conditions and diet were controlled. | Speed, accuracy, and mental endurance decreased after 3 h of fluid deprivation. Stability decreased after 9 h of fluid deprivation Energy decreased after 15 h of fluid deprivation. No other effect on mood. |
| Szinnai et al., 2005 [59] | Determine the effect of slowly progressive dehydration on mental performance | 8 healthy women (age 21–34 y) and 8 healthy men (age 20–34 y) | Crossover RCT | During the dehydration arm, subjects abstained from fluid intake for 28 h. During the control arm, subjects were allowed fluid ad libitum. | Urine osmolality increased during dehydration (2.45% body mass loss). Stroop test word naming (verbal response time) revealed significant dehydration-gender interactions, with slower response time in females, but faster response time in males with dehydration. No significant effect of dehydration or sex on visual attention, cognitive-motor speed, sustained attention, and divided attention). No difference with auditory event-related potentials P300. Subjective rating was greater for tiredness and lower for alertness with dehydration. |
| Shirreffs et al., 2004 [60] | Investigate the physiological responses and subjective feelings resulting from fluid restriction over 37 h compared to euhydration | 15 subjects (40% F) average age 30 y | Crossover RCT | Subjects randomized to different hydration conditions for up to 37 h:
| Fluid restriction: water from food, 487 ± 335 mL; urinary loss, 1.37 ± 0.39 L; body mass decrease, 2.7 ± 0.6% at 37 h. Subjects reported decreased ability to concentrate, and decreased alertness, and more headaches. Euhydration: water intake, 3168 ± 1167 mL; urinary loss, 2.76 ± 1.11 L. |
| Neave et al., 2001 [61] | Assess dehydration within normal physiological levels on mood and cognition. | 24 generally healthy adults (50% F) average age 20.1 y | Crossover | Subjects did not eat or drink anything from midnight until testing the next morning. Compared 300 mL water vs. no intake (9–11 h no water intake). | Fasting was ~9 h with testing over 2 h. Sustained attention and working memory were not affected by water intake. No water intake negatively affected calmness and alertness, measured using Bond–Lader. |
| Rogers et al., 2001 [62] | Assessing no drinking vs. 120 mL or 330 mL of water intake | 60 adults (50% F), average age 26 y | Parallel RCT | Subjects performed cognition task after acute consumption of the following:
| Improved attention with acute fluid intake Increased alertness at 2 min, but not after 25 min. No effect on ratings for revitalization. |
| Gopinathan et al., 1988 [63] | Determine the effects of various degrees of dehydration on mental performance | 11 healthy soldiers (age 20–25 y) | Crossover RCT | Subjects performed moderate work for 2 h under hot and humid conditions (30% relative humidity, 45 °C). Water was restricted during work to induce four different dehydration states: −1, −2, −3, and −4% body mass. | Short-term memory, arithmetic efficiency, and motor speed and attention deteriorated with increased dehydration, starting at 2% body mass loss. |
| Sharma et al., 1986 [64] | Investigate the effect of primary dehydration of various levels (1, 2 and 3% body-weight deficits) on mental functions in heat acclimatized subjects drawn from tropical regions of India | 8 healthy men (age 21–24 y) | Crossover RCT | Subjects performed moderate work under hot and dry conditions (60% relative humidity, 45 °C) or hot and humid conditions (30% relative humidity, 45 °C) until they reached their target dehydration states: 0 (water replenished), −1, −2, and −3% body weight. Cognition tests were performed after 90 min rest in neutral conditions (27 °C, 50% relative humidity). | Symbol classification was not affected by dehydration. Concentration, memory, and perceptual motor coordination decreased at 2% and 3% body mass loss, compared to 0% dehydration. |
| Headache | |||||
| Spigt et al., 2012 [65] | Investigate the effects of increased water intake on headache | 102 adults who had at least two episodes of moderately intense headache or at least five mildly intense episodes per month and a total fluid intake of less than 2.5 L/day. Control group: average age 45 y; water group: average age 47 y. | Parallel RCT | Both groups received written instructions about stress reduction and sleep improvement strategies. Group 1: Also instructed to consume an additional 1.5 L water/d (n = 52, 16/36 M/F). Group 2: No additional intervention (n = 50, 13/37 M/F). 3 month intervention. | Subjects who drank more water reported better migraine specific quality of life. 47% in the intervention (water) group self-reported improvement against 25% in controls. Drinking more water did not result in relevant changes in objective effect parameters, such as days with at least moderate headache or days with medication use |
| Spigt et al., 2005 [66] | Explore whether there could be a positive effect of increased water intake in headache patients | 15 adults who frequently (once a week or more) suffered from migraine or tension-type headache, mean age 44 y | Parallel RCT | Group 1: Instructed to consume an additional 1.5 L water/d (n = 8). Group 2: Received placebo tablet (n = 7). 3 month intervention. | Additional water consumption decreased total number of hours of headache and headache intensity, but effects were not statistically significant. |
| Citation | Study Objective | Population | Design | Intervention | Summary/Conclusion |
|---|---|---|---|---|---|
| Anti et al., 1998 [73] | Determine the effects of a high-fiber diet and fluid supplementation in patients with functional chronic constipation | 117 adults with chronic functional constipation (age 18–50 y). Baseline fluid intake: Group 1: 1.0 L (SD 0.2) and Group 2: 1.0 L (SD 0.4) | Parallel RCT | Group 1 (n = 58, 20/38 M/F) consumed standard diet providing 25 g fiber with ad libitum fluid intake. Group 2 (n = 59, 23/36 M/F) consumed standard diet providing 25 g fiber with 2 L/d fluid for 2 months | Fluid intake was greater in Group 2 (average 2.1 L/d) vs. Group 1 (average 1.1 L/d). Group 2 had greater increases in stool frequency and decreases in laxative use compared to Group 1. |
| Chung et al., 1999 [75] | Examine the effect of excess fluid (isotonic and hypotonic) on the actual stool output as measured by stool weight while simultaneously monitoring the urine output in 15 healthy volunteers | 15 adults age 23 to 46 y. Baseline fluid intake: Group 1: 1.38 L (SD 0.93) and Group 2:1.20 L (SD 0.29). | Parallel | Group 1 (n = 9, 4/5 M/F): Additional intake of near isotonic fluid (Gatorade); Group 2 (n = 6, 3/3 M/F): Additional intake of hypotonic solution (water). Both groups consumed additional 1 L/d of fluid for 2 days, followed by additional 2 L/d of fluid for the next 2 days. | No change in total stool weight in both groups. Stool frequency was not reported. |
| Ziegenhagen et al., 1991 [76] | Compare the long-term effects of wheat bran alone vs. wheat bran with fluid addition on gastrointestinal function in healthy subjects | 11 adults (55% F), age 19–33 y | Crossover RCT | Period 1: 15 g wheat bran twice/d. Period 2: 15 g wheat bran + 300 mL tea or water twice/d. Basal fluid intake restricted to 1–1.2 L/d. 14 d intervention, 7 d washout. | Gastric emptying was slower with bran vs. control and bran + fluid. Whole gut (oroanal) transit was shorter, while stool frequency and stool weight were greater with bran and bran + fluid vs. control. No effects due to addition of fluid were reported. |
| Klauser et al., 1990 [74] | Investigate whether fluid deprivation has an influence on colonic function | 8 healthy men (age 21–28 y) | Crossover RCT | Control week: Consume >2500 mL fluid/d. Intervention week: Consume <500 mL fluid/d. 1 week intervention, 1 week washout. | Stool weight and frequency decreased with fluid restriction. No change in oroanal transit time. |
| van Nieuwenhoven et al., 2000 | Examine the effect of dehydration on various gastrointestinal parameters during strenuous exercise. | 10 healthy men (age 18–30 y) | Crossover RCT | Euhydration/control arm: Habitual fluid consumption. Dehydration arm: 15-min periods in a dry sauna interspersed with 10-min cooling off periods until 3% body mass loss was reached | Gastric emptying was significantly slower during dehydration. Orocecal transit time, intestinal permeability, and intestinal glucose absorption were unaffected by dehydration. Hydration status during euhydration/control arm was not assessed. Habitual fluid intake was not reported. (Only results from the pre-exercise/resting stage are reported herein). |
| Citation | Study Objective | Population | Design | Intervention | Summary/Conclusion |
|---|---|---|---|---|---|
| Wong et al., 2017 [86] | Compare a standard weight-loss program with and without water | 38 overweight and obese adolescents who reported drinking ≤4 cups of water/d; Control: 6M/13F, mean age 15.7 y; Water: 5M/14F, mean age 14.1 y | 6 month parallel RCT | All participants received similar weight-reducing interventions (i.e., dietary counseling, daily text messages, and a cookbook with health guides). Control: No specific advice on water consumption. +Water: Received well-defined water messages through counseling and daily text messages, a water bottle, and a water pitcher with filters, and a target to increase habitual water intake to 8 cups/d. | Water group consumed more water [4.8 (3.8 to 5.9) cups of water/d] compared to the Control group [3.5 (2.6 to 4.4) cups/d]. Changes in BMI z-score and other anthropometric measures did not differ significantly between the two groups. |
| Parretti et al., 2015 [85] | Investigate the efficacy of water preloading before meals as a weight loss strategy for adults with obesity. | 84 obese adults; Control: 15/28 M/F, mean age 57.8 y; Water: 15/26 M/F, mean age 55.1 y | 12 week parallel RCT | All participants were given a face-to-face weight management consultation at baseline and a follow-up telephone consultation at 2 weeks. Control: Instructed to imagine their stomach was full before meals. +Water: Instructed to drink 500 mL of water 30 min before their main meals. | Water group lost 1.3 kg more than control group at 12 weeks. |
| Corney et al., 2015 [84] | Examine the effects of hydration status and/or fluid availability during eating on ad libitum energy intake | 16 healthy males, average age 25 y. | Acute RCT | Subjects provided standard foods for 24 h which were designed so subjects are euhydrated or hypohydrated. Ad libitum breakfast was provided the next day. | Hydration status prior to ad libitum breakfast did not affect energy intake. Those who were hypohydrated (~1.8% body mass loss) consumed more fluids during breakfast compared to those who were euhydrated. |
| Health Outcomes | Summary of Literature Findings |
|---|---|
| Skin Health | The effectiveness of additional water consumption on skin barrier function is unclear. A few studies suggest that increasing water consumption may improve the hydration of the stratum corneum layer of the epidermis, which plays a key role in skin barrier function. However, no changes to transepidermal water loss (measure of barrier integrity) were reported. |
| Cognition | Despite variability among study methodologies, dehydration impairs cognitive performance for tasks involving attention, executive function, and motor coordination when water deficits exceed 2% body mass loss. Cognitive domains involving lower order mental processing (e.g., simple reaction time) are less sensitive to changes in hydration status. In children, results from studies on hydration and cognition are mixed. |
| Mood and Fatigue | Hypohydration is associated with increased negative emotions such as anger, hostility, confusion, depression and tension as well as fatigue and tiredness. These findings are consistent in adults, but unclear and very limited in children. |
| Headache | The evidence is too limited to determine if hydration affects headache. |
| Kidney Stones | A significant association between high fluid intake and a lower risk of incident kidney stones has been reported, but data are limited. |
| Renal Function related to Toxin Elimination | There is not enough evidence to support commercial detox diets for toxin elimination. |
| Gastrointestinal Function and Constipation | Studies on hydration and general gastrointestinal function in healthy people are lacking. Clinical trials have been conducted on constipation, but currently do not support the use of increased fluid intake in the treatment of functional constipation. Further studies are necessary to understand the role of water and fluid consumption in the etiology and treatment of constipation. |
| Body Weight and Body Composition | Studies on fluid replacement of caloric beverages with non-caloric beverages have consistently resulted in lower energy intake. Existing data suggest that increased water consumption contributes to reductions in body fat and/or weight loss in obese adults, independent of changes in energy intake. Data in children are limited. More studies are needed to clarify the effect in both adults and children. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liska, D.; Mah, E.; Brisbois, T.; Barrios, P.L.; Baker, L.B.; Spriet, L.L. Narrative Review of Hydration and Selected Health Outcomes in the General Population. Nutrients 2019, 11, 70. https://doi.org/10.3390/nu11010070
Liska D, Mah E, Brisbois T, Barrios PL, Baker LB, Spriet LL. Narrative Review of Hydration and Selected Health Outcomes in the General Population. Nutrients. 2019; 11(1):70. https://doi.org/10.3390/nu11010070
Chicago/Turabian StyleLiska, DeAnn, Eunice Mah, Tristin Brisbois, Pamela L. Barrios, Lindsay B. Baker, and Lawrence L. Spriet. 2019. "Narrative Review of Hydration and Selected Health Outcomes in the General Population" Nutrients 11, no. 1: 70. https://doi.org/10.3390/nu11010070
APA StyleLiska, D., Mah, E., Brisbois, T., Barrios, P. L., Baker, L. B., & Spriet, L. L. (2019). Narrative Review of Hydration and Selected Health Outcomes in the General Population. Nutrients, 11(1), 70. https://doi.org/10.3390/nu11010070