Validity of an Abbreviated, Clinically Feasible Test for Postprandial Lipemia in Healthy Adults: A Randomized Cross-Over Study



Abstract
1. Introduction
2. Methods
2.1. Research Participants
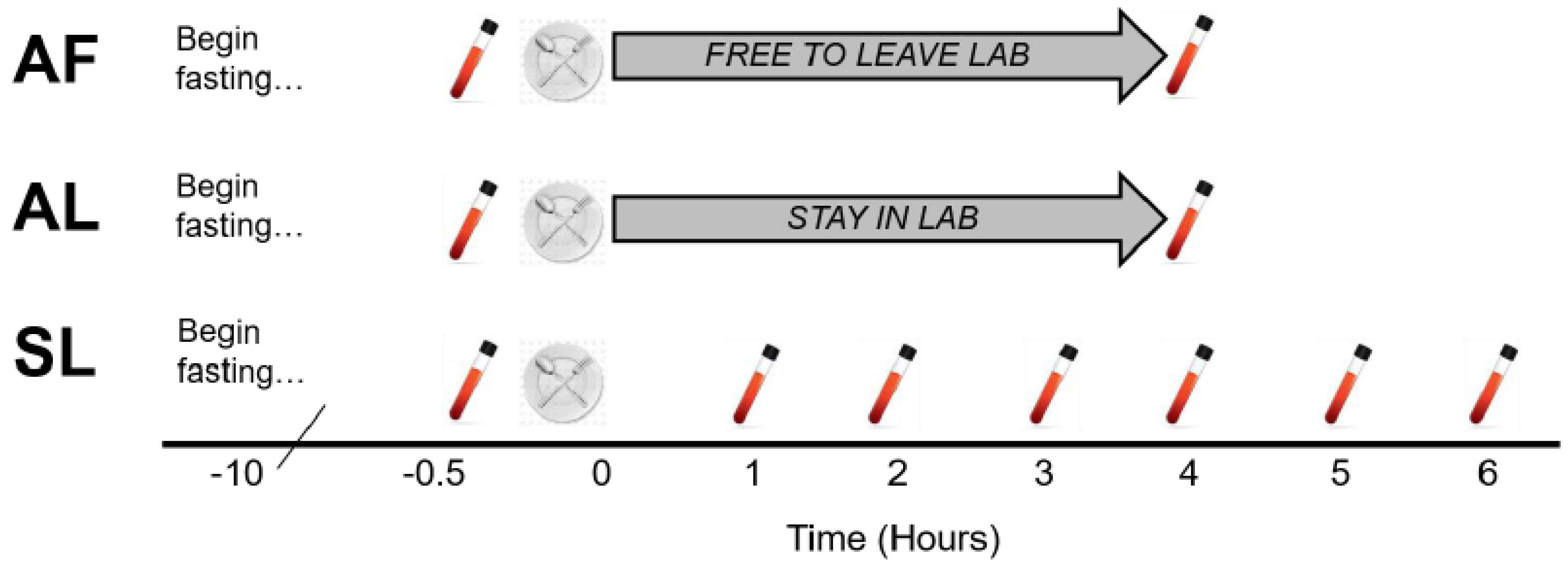
2.2. Overview of Study
2.3. Study Protocol
2.4. Statistical Analyses
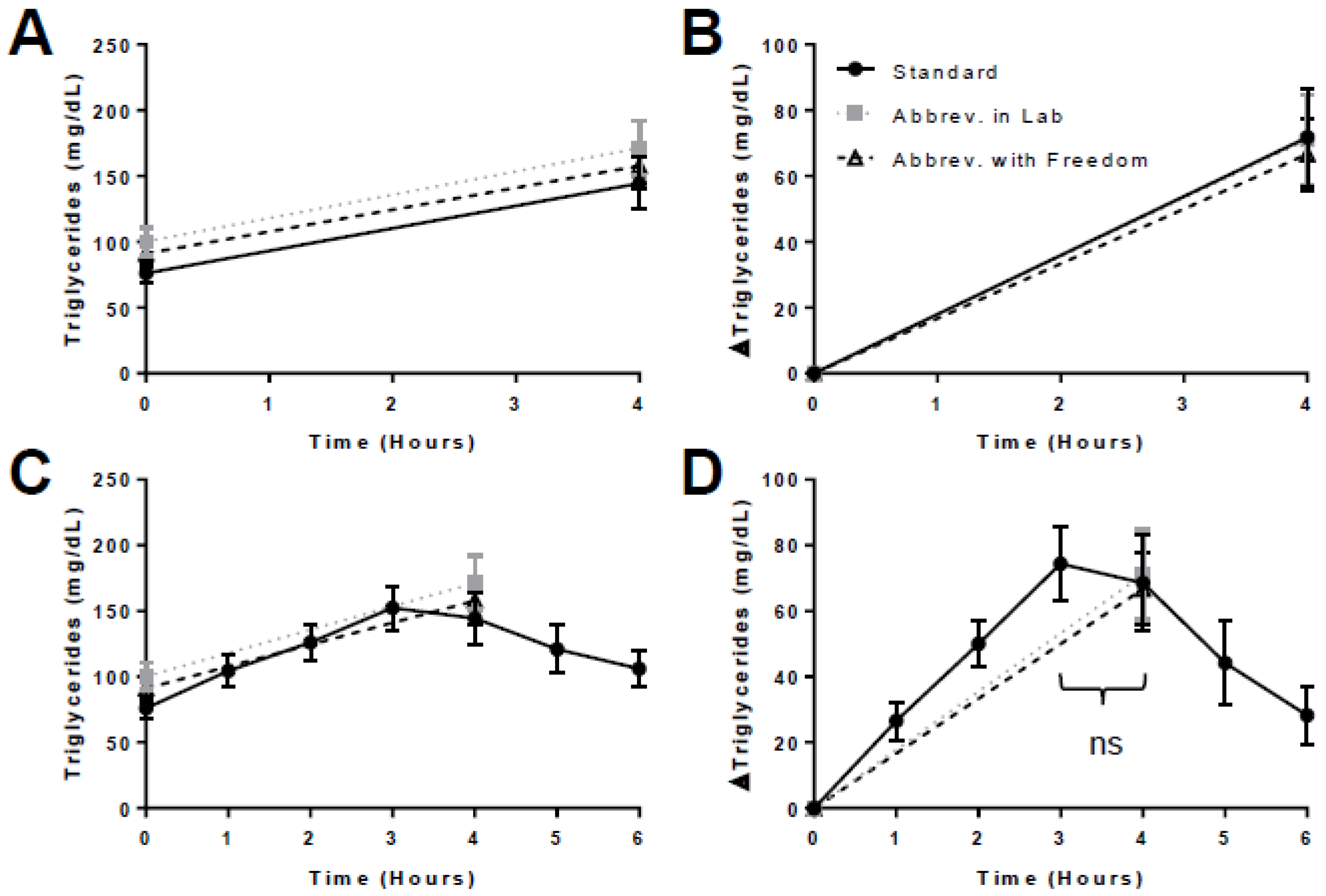
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bansal, S.; Buring, J.E.; Rifai, N.; Mora, S.; Sacks, F.M.; Ridker, P.M. Fasting compared with nonfasting triglycerides and risk of cardiovascular events in women. JAMA 2007, 298, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Hyson, D.; Rutledge, J.C.; Berglund, L. Postprandial lipemia and cardiovascular disease. Curr. Atheroscler. Rep. 2003, 5, 437–444. [Google Scholar] [CrossRef] [PubMed]
- Guerci, B.; Paul, J.; Hadjadj, S.; Durlach, V.; Vergčs, B.; Attia, N.; Girard-Globa, A.; Drouin, P. Analysis of the postprandial lipid metabolism: Use of a 3-point test. Diabetes Metab. 2008, 27, 449–457. [Google Scholar]
- Rector, S.R.; Linden, M.A.; Zhang, J.Q.; Warner, S.O.; Altena, T.S.; Smith, B.K.; Ziogas, G.G.; Liu, Y.; Thomas, T.R. Predicting Postprandial Lipemia in Healthy Adults and in At-Risk Individuals with Components of the Cardiometabolic Syndrome. J. Clin. Hypertens. 2009, 11, 663–671. [Google Scholar] [CrossRef] [PubMed]
- Maraki, M.; Aggelopoulou, N.; Christodoulou, N.; Katsarou, C.; Anapliotis, P.; Kavouras, S.A.; Panagiotakos, D.; Sidossis, L.S. Validity of abbreviated oral fat tolerance tests for assessing postprandial lipemia. Clin. Nutr. 2011, 30, 852–857. [Google Scholar] [CrossRef] [PubMed]
- Weiss, E.P.; Fields, D.A.; Mittendorfer, B.; Haverkort, M.D.; Klein, S. Reproducibility of postprandial lipemia tests and validity of an abbreviated 4-h test. Metab. Clin. Exp. 2008, 57, 1479–1485. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.Q.; Thomas, T.R.; Ball, S.D. Effect of exercise timing on postprandial lipemia and HDL cholesterol subfractions. J. Appl. Physiol. 1998, 85, 1516–1522. [Google Scholar] [CrossRef] [PubMed]
- Emerson, S.R.; Kurti, S.P.; Emerson, E.M.; Cull, B.J.; Casey, K.; Haub, M.D.; Rosenkranz, S.K. Postprandial Metabolic Responses Differ by Age Group and Physical Activity Level. J. Nutr. Health Aging 2018, 22, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Kolovou, G.D.; Mikhailidis, D.P.; Kovar, J.; Lairon, D.; Nordestgaard, B.G.; Ooi, T.C.; Perez-Martinez, P.; Bilianou, H.; Anagnostopoulou, K.; Panotopoulos, G. Assessment and clinical relevance of non-fasting and postprandial triglycerides: An expert panel statement. Curr. Vasc. Pharmacol. 2011, 9, 258–270. [Google Scholar] [CrossRef] [PubMed]
- O’Doherty, A.; Sathyapalan, T.; Rigby, A.; Ingle, L.; Carroll, S. The repeatability of the abbreviated (4-hour) oral fat tolerance test and influence of prior acute aerobic exercise. Eur. J. Nutr. 2018, 57, 309–318. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Participants (n) | 18 |
| Age (years) | 21.2 ± 2.5 |
| Sex (M/F) | 8 M/10 F |
| Body mass (kg) | 72.9 ± 16.9 |
| Height (cm) | 169.7 ± 2.9 |
| BMI (kg/m2) | 25.2 ± 6.1 |
| Fasting glucose (mg/dL) | 90.8 ± 7.6 |
| Fasting Total-C (mg/dL) | 165.9 ± 33.5 |
| Fasting HDL-C (mg/dL) | 53.3 ± 19.3 |
| Fasting LDL-C (mg/dL) | 95.1 ± 27.9 |
| Test meal energy (kcal) | 874.8 ± 202.7 |
| SL Trial | AL Trial | AF Trial | p | ||
|---|---|---|---|---|---|
| Fasting TG (mg/dL) | Mean ± SD | 76.1 ± 34.0 | 100.4 ± 44.6 | 91.1 ± 44.9 | 0.08 |
| 95% CI | (59.2, 93.0) | (78.2, 122.6) | (68.7, 113.4) | ||
| 4-h TG (mg/dL) | Mean ± SD | 144.6 ± 84.2 | 171.4 ± 88.2 | 157.7 ± 76.7 | 0.49 |
| 95% CI | (102.7, 186.4) | (127.6, 215.3) | (119.6, 195.8) | ||
| 4-h TG Δ (mg/dL) | Mean ± SD | 68.5 ± 62.7 | 71.1 ± 58.0 | 66.7 ± 46.4 | 0.93 |
| 95% CI | (37.3, 99.7) | (42.2, 99.9) | (43.6, 89.7) | ||
| tAUC (mg/dL × 4 h) | Mean ± SD | 441.2 ± 224.2 | 543.7 ± 254.5 | 497.6 ± 233.5 | 0.12 |
| 95% CI | (329.7, 552.7) | (417.1, 670.2) | (381.4, 613.7) | ||
| iAUC (mg/dL × 4 h) | Mean ± SD | 138.6 ± 123.6 | 143.2 ± 114.5 | 133.3 ± 92.7 | 0.91 |
| 95% CI | (77.1, 200.0) | (86.3, 200.2) | (87.2, 179.4) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sciarrillo, C.M.; Koemel, N.A.; Kurti, S.P.; Emerson, S.R. Validity of an Abbreviated, Clinically Feasible Test for Postprandial Lipemia in Healthy Adults: A Randomized Cross-Over Study. Nutrients 2019, 11, 180. https://doi.org/10.3390/nu11010180
Sciarrillo CM, Koemel NA, Kurti SP, Emerson SR. Validity of an Abbreviated, Clinically Feasible Test for Postprandial Lipemia in Healthy Adults: A Randomized Cross-Over Study. Nutrients. 2019; 11(1):180. https://doi.org/10.3390/nu11010180
Chicago/Turabian StyleSciarrillo, Christina M., Nicholas A. Koemel, Stephanie P. Kurti, and Sam R. Emerson. 2019. "Validity of an Abbreviated, Clinically Feasible Test for Postprandial Lipemia in Healthy Adults: A Randomized Cross-Over Study" Nutrients 11, no. 1: 180. https://doi.org/10.3390/nu11010180
APA StyleSciarrillo, C. M., Koemel, N. A., Kurti, S. P., & Emerson, S. R. (2019). Validity of an Abbreviated, Clinically Feasible Test for Postprandial Lipemia in Healthy Adults: A Randomized Cross-Over Study. Nutrients, 11(1), 180. https://doi.org/10.3390/nu11010180