Effectiveness of A Multifactorial Intervention in Increasing Adherence to the Mediterranean Diet among Patients with Diabetes Mellitus Type 2: A Controlled and Randomized Study (EMID Study)

 , ,
, , 
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Common Advice
2.4. Randomization and Masking
2.5. Intervention
2.5.1. Food Workshop
2.5.2. Smartphone Application (EVIDENT II)
2.5.3. Heart-Healthy Walks
2.6. Outcome Measures and Follow-Up
2.6.1. Adherence to the Mediterranean Diet
2.6.2. Diet Quality Index
2.6.3. Clinically Relevant Measures
2.7. Sample Size Calculation
2.8. Ethical Considerations
2.9. Statistical Analysis
3. Results
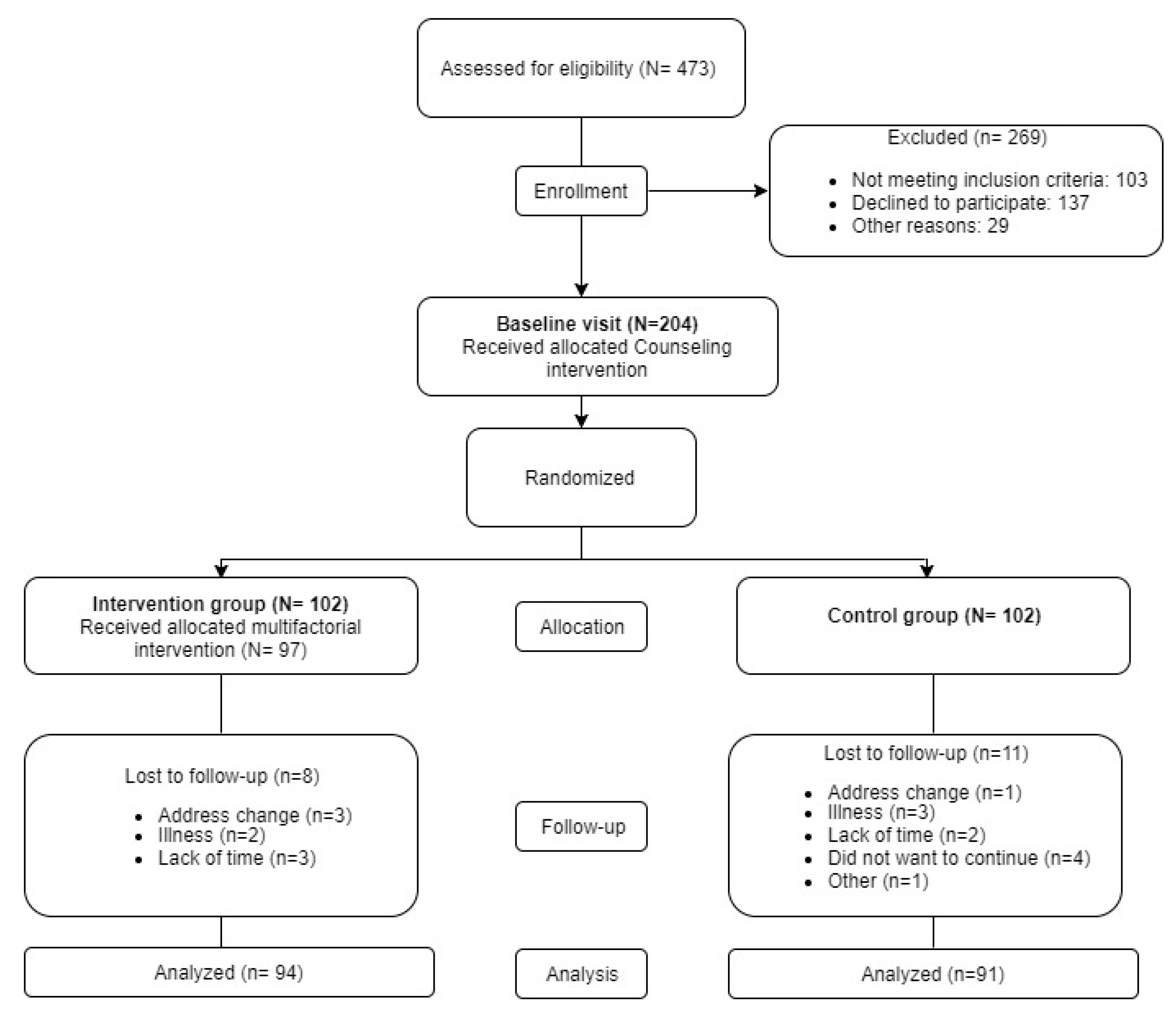
3.1. Sample Selection
3.2. Demographic and Clinical Characteristics of the Included Subjects
3.3. Adherence to the Intervention
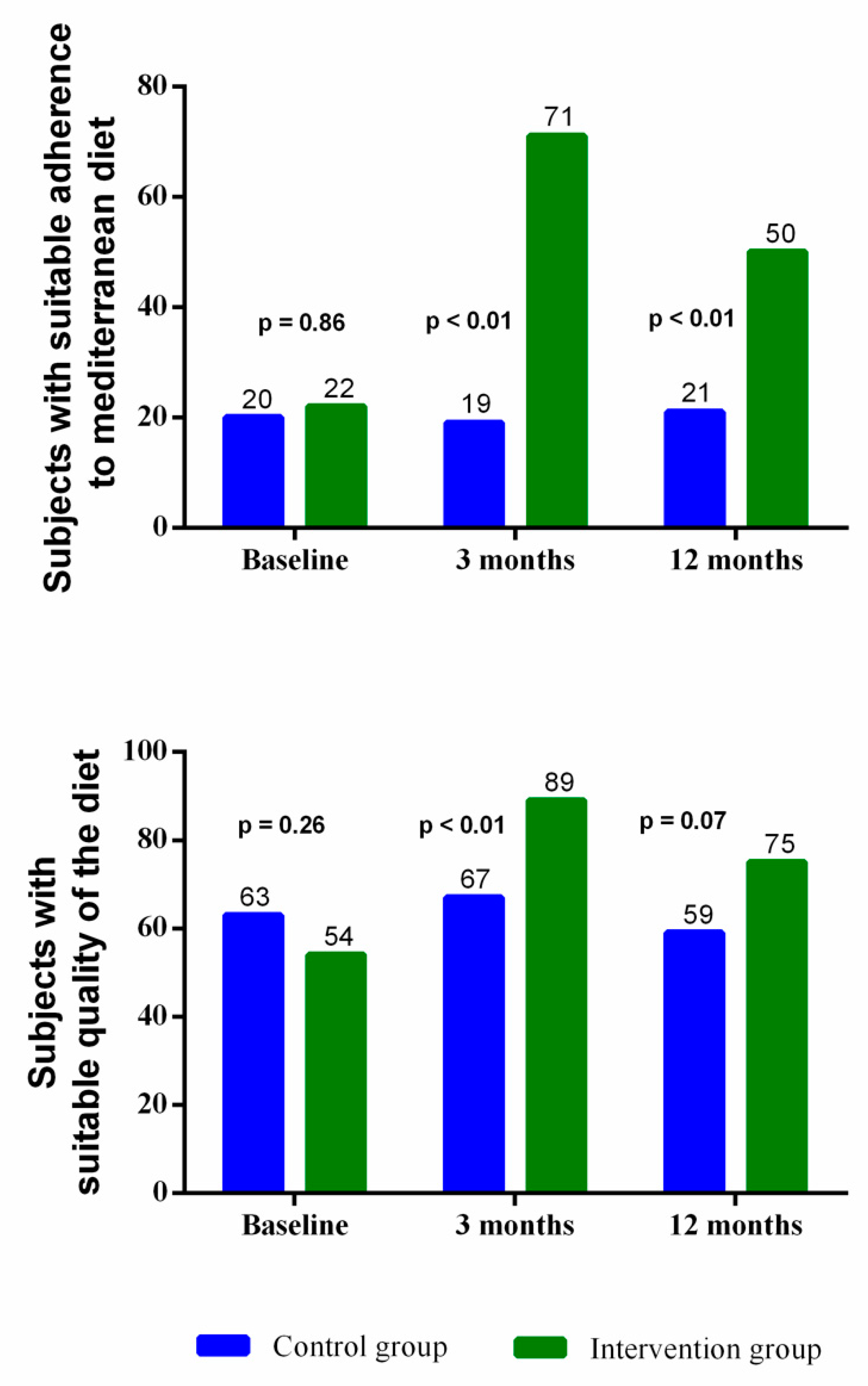
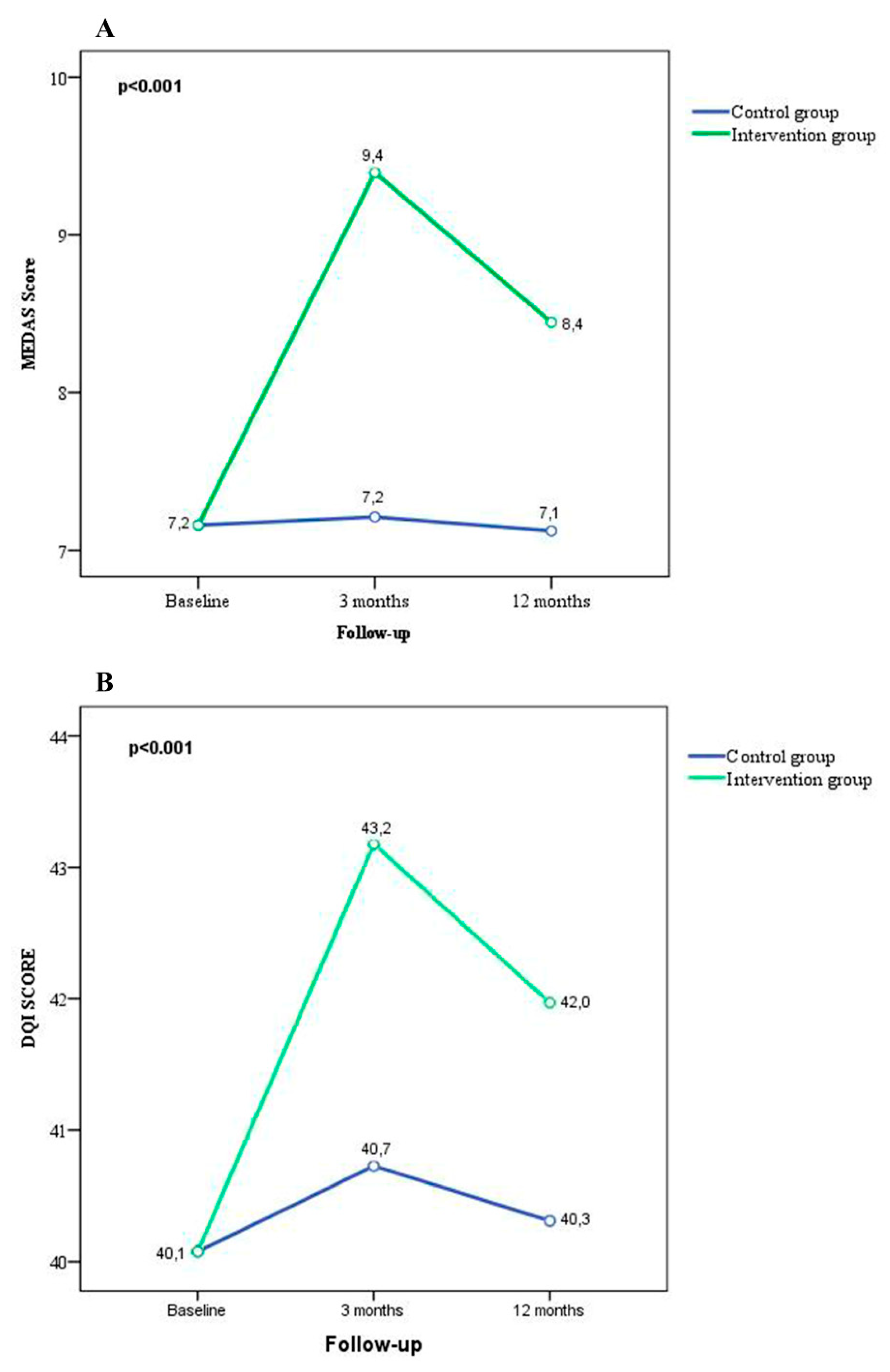
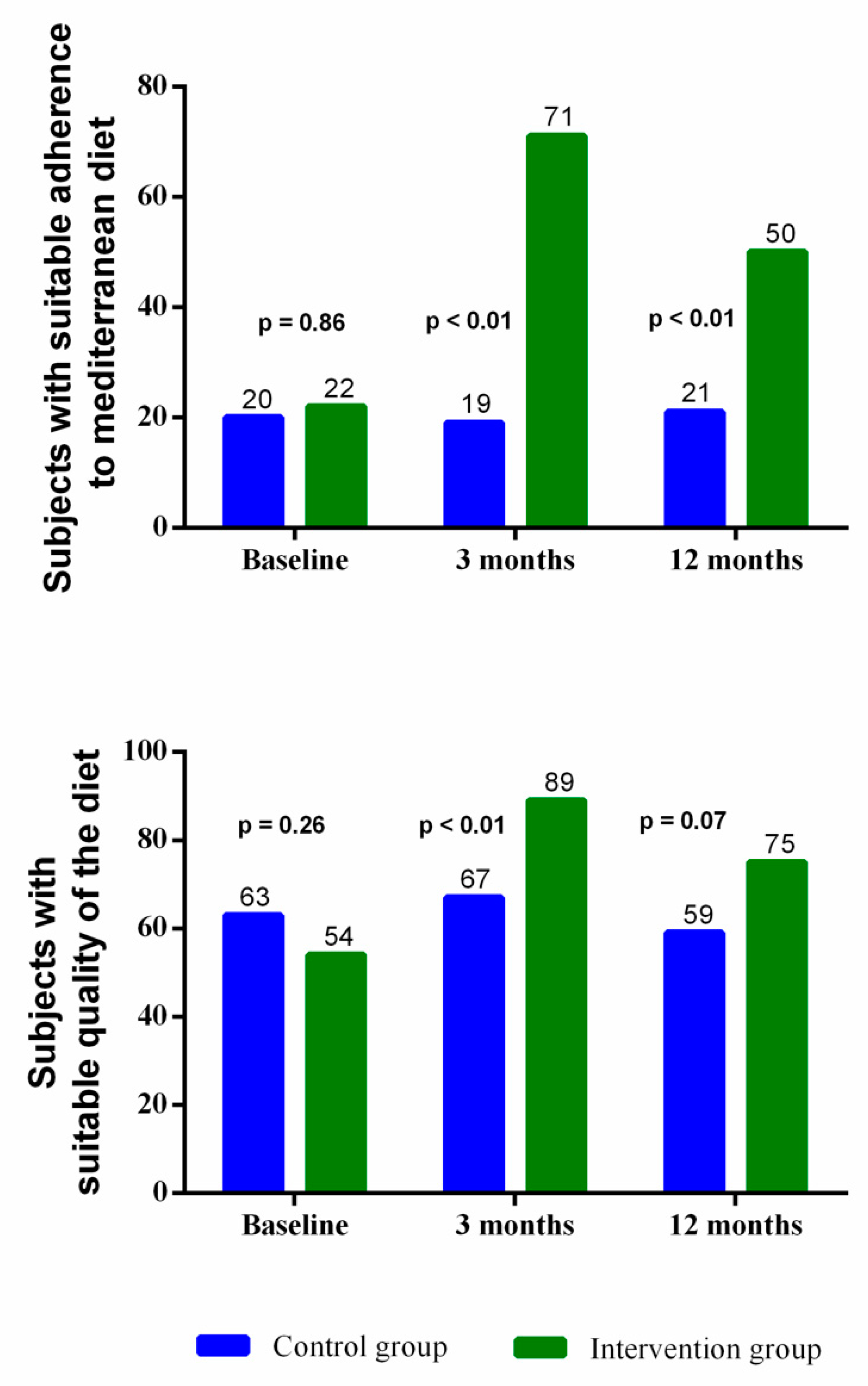
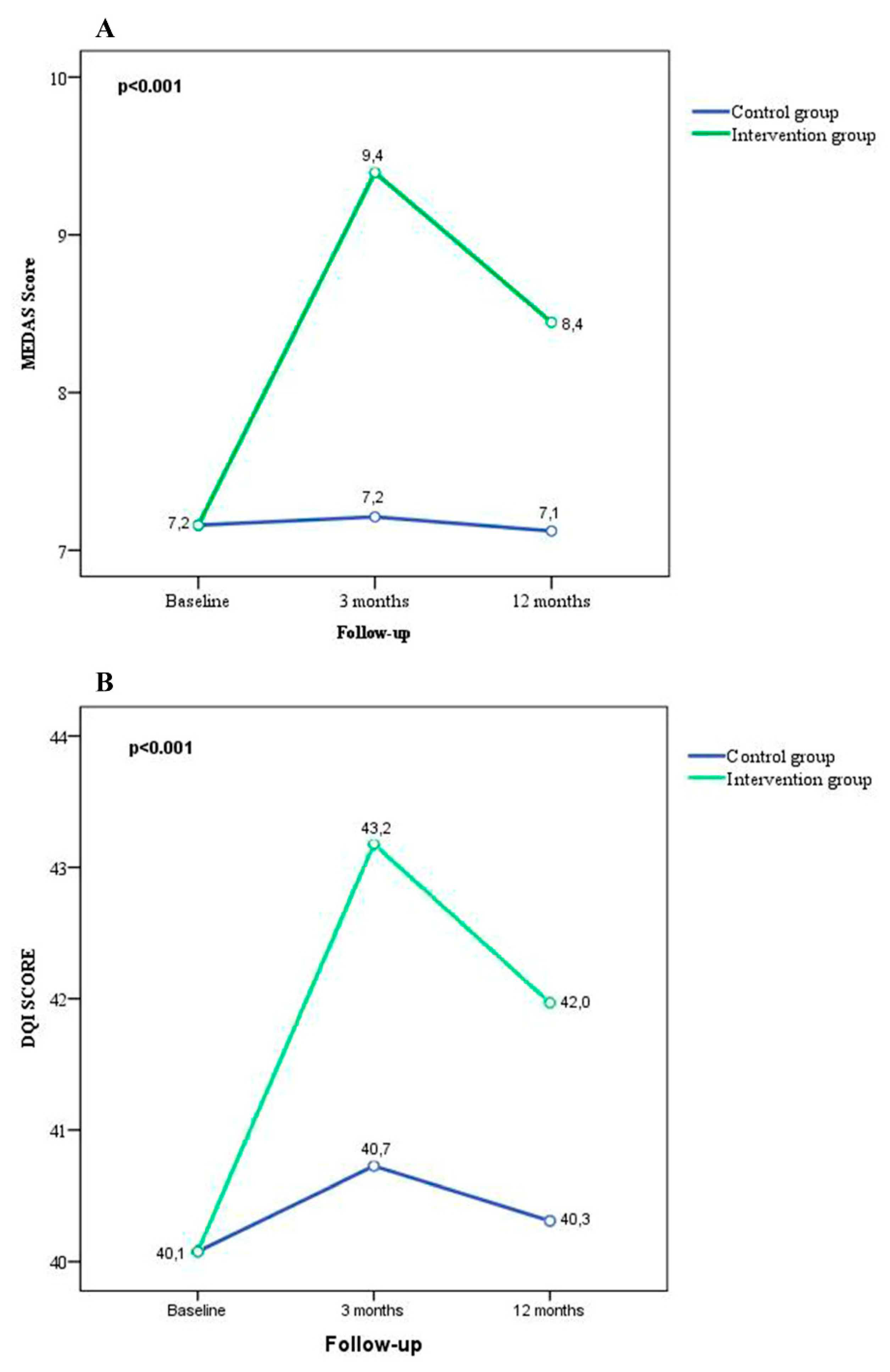
3.4. Effect of the Intervention
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Keys, A.; Menotti, A.; Karvonen, M.J.; Aravanis, C.; Blackburn, H.; Buzina, R.; Djordjevic, B.S.; Dontas, A.S.; Fidanza, F.; Keys, M.H.; et al. The diet and 15-year death rate in the seven countries study. Am. J. Epidemiol. 1986, 124, 903–915. [Google Scholar] [CrossRef] [PubMed]
- Kastorini, C.M.; Milionis, H.J.; Esposito, K.; Giugliano, D.; Goudevenos, J.A.; Panagiotakos, D.B. The effect of Mediterranean diet on metabolic syndrome and its components: A meta-analysis of 50 studies and 534,906 individuals. Am. J. Cardiol. 2011, 57, 1299–1313. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulou, A.; Martinez-Gonzalez, M.A.; Tong, T.Y.; Forouhi, N.G.; Khandelwal, S.; Prabhakaran, D.; Mozaffarian, D.; de Lorgeril, M. Definitions and potential health benefits of the Mediterranean diet: Views from experts around the world. BMC Med. 2014, 12, 112. [Google Scholar] [CrossRef] [PubMed]
- Babio, N.; Toledo, E.; Estruch, R.; Ros, E.; Martinez-Gonzalez, M.A.; Castaner, O.; Bullo, M.; Corella, D.; Aros, F.; Gomez-Gracia, E.; et al. Mediterranean diets and metabolic syndrome status in the PREDIMED randomized trial. CMAJ 2014, 186, E649–E657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huo, R.; Du, T.; Xu, Y.; Xu, W.; Chen, X.; Sun, K.; Yu, X. Effects of Mediterranean-style diet on glycemic control, weight loss and cardiovascular risk factors among type 2 diabetes individuals: A meta-analysis. Eur. J. Clin. Nutr. 2015, 69, 1200–1208. [Google Scholar] [CrossRef] [PubMed]
- Ajala, O.; English, P.; Pinkney, J. Systematic review and meta-analysis of different dietary approaches to the management of type 2 diabetes. Am. J. Clin. Nutr. 2013, 97, 505–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Estruch, R.; Ros, E.; Martinez-Gonzalez, M.A. Mediterranean diet for primary prevention of cardiovascular disease. N. Eng. J. Med. 2013, 369, 676–677. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Macchi, C.; Abbate, R.; Gensini, G.F.; Casini, A. Mediterranean diet and health status: An updated meta-analysis and a proposal for a literature-based adherence score. Public Health Nutr. 2014, 17, 2769–2782. [Google Scholar] [CrossRef]
- Salas-Salvado, J.; Guasch-Ferre, M.; Lee, C.H.; Estruch, R.; Clish, C.B.; Ros, E. Protective Effects of the Mediterranean Diet on Type 2 Diabetes and Metabolic Syndrome. J. Nutr. 2016, 146, 920S–927S. [Google Scholar] [CrossRef]
- Salas-Salvado, J.; Fernandez-Ballart, J.; Ros, E.; Martinez-Gonzalez, M.A.; Fito, M.; Estruch, R.; Corella, D.; Fiol, M.; Gomez-Gracia, E.; Aros, F.; et al. Effect of a Mediterranean diet supplemented with nuts on metabolic syndrome status: one-year results of the PREDIMED randomized trial. Arch. Intern. Med. 2008, 168, 2449–2458. [Google Scholar] [CrossRef]
- Sotos-Prieto, M.; Cash, S.B.; Christophi, C.A.; Folta, S.; Moffatt, S.; Muegge, C.; Korre, M.; Mozaffarian, D.; Kales, S.N. Rationale and design of feeding America’s bravest: Mediterranean diet-based intervention to change firefighters’ eating habits and improve cardiovascular risk profiles. Contemp. Clin. Trial. 2017, 61, 101–107. [Google Scholar] [CrossRef]
- Maderuelo-Fernandez, J.A.; Recio-Rodriguez, J.I.; Patino-Alonso, M.C.; Perez-Arechaederra, D.; Rodriguez-Sanchez, E.; Gomez-Marcos, M.A.; Garcia-Ortiz, L. Effectiveness of interventions applicable to primary health care settings to promote Mediterranean diet or healthy eating adherence in adults: A systematic review. Prev. Med. 2015, 76, S39–S55. [Google Scholar] [CrossRef] [PubMed]
- Cubillos, L.; Estrada Del Campo, Y.; Harbi, K.; Keyserling, T.; Samuel-Hodge, C.; Reuland, D.S. Feasibility and Acceptability of a Clinic-based Mediterranean-style Diet Intervention to Reduce Cardiovascular Risk for Hispanic Americans With Type 2 Diabetes. Diabetes Educ. 2017, 43, 286–296. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Huelgas, R.; Jansen-Chaparro, S.; Baca-Osorio, A.J.; Mancera-Romero, J.; Tinahones, F.J.; Bernal-Lopez, M.R. Effects of a long-term lifestyle intervention program with Mediterranean diet and exercise for the management of patients with metabolic syndrome in a primary care setting. Eur. J. Intern. Med. 2015, 26, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Bueno, C.; Cavero-Redondo, I.; Martinez-Andres, M.; Arias-Palencia, N.; Ramos-Blanes, R.; Salcedo-Aguilar, F. Effectiveness of multifactorial interventions in primary health care settings for primary prevention of cardiovascular disease: A systematic review of systematic reviews. Prev. Med. 2015, 76, S68–S75. [Google Scholar] [CrossRef] [PubMed]
- Ried-Larsen, M.; Christensen, R. Head-to-head comparison of intensive lifestyle intervention (U-TURN) versus conventional multifactorial care in patients with type 2 diabetes: Protocol and rationale for an assessor-blinded, parallel group and randomised trial. BMJ 2015, 5, e009764. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Cho, Y.; Park, Y.; Sohn, C.; Rha, M.; Lee, M.K.; Jang, H.C. Association of dietary quality indices with glycemic status in korean patients with type 2 diabetes. Clin. Nutr. Res. 2013, 2, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Murray, A.E.; McMorrow, A.M.; O’Connor, E.; Kiely, C.; Mac Ananey, O.; O’Shea, D.; Egana, M.; Lithander, F.E. Dietary quality in a sample of adults with type 2 diabetes mellitus in Ireland; a cross-sectional case control study. Nutr. J. 2013, 12, 110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muller, A.M.; Alley, S.; Schoeppe, S.; Vandelanotte, C. The effectiveness of e-& mHealth interventions to promote physical activity and healthy diets in developing countries: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 109. [Google Scholar] [PubMed]
- Pal, K.; Eastwood, S.V.; Michie, S.; Farmer, A.; Barnard, M.L.; Peacock, R.; Wood, B.; Edwards, P.; Murray, E. Computer-based interventions to improve self-management in adults with type 2 diabetes: A systematic review and meta-analysis. Diabetes Care 2014, 37, 1759–1766. [Google Scholar] [CrossRef]
- Holmen, H.; Torbjornsen, A.; Wahl, A.K.; Jenum, A.K.; Småstuen, M.C.; Årsand, E.; Ribu, L. A Mobile Health Intervention for Self-Management and Lifestyle Change for Persons With Type 2 Diabetes, Part 2: One-Year Results From the Norwegian Randomized Controlled Trial RENEWING HEALTH. JMIR mHealth uHealth 2014, 2, e57. [Google Scholar] [CrossRef] [PubMed]
- Alonso-Dominguez, R.; Gomez-Marcos, M.A.; Patino-Alonso, M.C.; Sanchez-Aguadero, N.; Agudo-Conde, C.; Castano-Sanchez, C.; Garcia-Ortiz, L.; Recio-Rodriguez, J.I. Effectiveness of a multifactorial intervention based on an application for smartphones, heart-healthy walks and a nutritional workshop in patients with type 2 diabetes mellitus in primary care (EMID): Study protocol for a randomised controlled trial. BMJ Open 2017, 7, e016191. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2018. Diabetes Care 2018, 41, S13–S27. [Google Scholar] [CrossRef] [PubMed]
- Recio-Rodriguez, J.I.; Agudo-Conde, C. Short-Term Effectiveness of a Mobile Phone App for Increasing Physical Activity and Adherence to the Mediterranean Diet in Primary Care: A Randomized Controlled Trial (EVIDENT II Study). J. Med. Int. Res. 2016, 18, e331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Recio-Rodriguez, J.I.; Martin-Cantera, C.; Gonzalez-Viejo, N.; Gomez-Arranz, A.; Arietaleanizbeascoa, M.S.; Schmolling-Guinovart, Y.; Maderuelo-Fernandez, J.A.; Perez-Arechaederra, D.; Rodriguez-Sanchez, E.; Gomez-Marcos, M.A.; et al. Effectiveness of a smartphone application for improving healthy lifestyles, a randomized clinical trial (EVIDENT II): Study protocol. BMC Public Health 2014, 14, 254. [Google Scholar] [CrossRef]
- Krader, C.G. American Diabetes Association. Diabetes clinical practice recommendations focus attention on individualization of care. Med. Econ. 2014, 91, 22. [Google Scholar] [PubMed]
- Fernandez-Ballart, J.D.; Pinol, J.L.; Zazpe, I.; Corella, D.; Carrasco, P.; Toledo, E.; Perez-Bauer, M.; Martinez-Gonzalez, M.A.; Salas-Salvado, J.; Martin-Moreno, J.M. Relative validity of a semi-quantitative food-frequency questionnaire in an elderly Mediterranean population of Spain. Br. J. Nutr. 2010, 103, 1808–1816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schroder, H.; Benitez Arciniega, A.; Soler, C.; Covas, M.I.; Baena-Diez, J.M.; Marrugat, J. Validity of two short screeners for diet quality in time-limited settings. Public Health Nutr. 2012, 15, 618–626. [Google Scholar] [CrossRef]
- World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [CrossRef] [PubMed]
- Zazpe, I.; Sanchez-Tainta, A.; Estruch, R.; Lamuela-Raventos, R.M.; Schroder, H.; Salas-Salvado, J.; Corella, D.; Fiol, M.; Gomez-Gracia, E.; Aros, F.; et al. A large randomized individual and group intervention conducted by registered dietitians increased adherence to Mediterranean-type diets: The PREDIMED study. J. Am. Diet. Assoc. 2008, 108, 1134–1144. [Google Scholar] [CrossRef] [PubMed]
- Esposito, K.; Maiorino, M.I.; Ceriello, A.; Giugliano, D. Prevention and control of type 2 diabetes by Mediterranean diet: A systematic review. Diabetes Res. Clin. Pract. 2010, 89, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Riccardi, G.; Giacco, R.; Rivellese, A.A. Dietary fat, insulin sensitivity and the metabolic syndrome. Clin. Nutr. 2004, 23, 447–456. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C.; Ahluwalia, N.; Brouns, F.; Buetler, T.; Clement, K.; Cunningham, K.; Esposito, K.; Jonsson, L.S.; Kolb, H.; Lansink, M.; et al. Dietary factors and low-grade inflammation in relation to overweight and obesity. Br. J. Nutr. 2011, 106, S75–S78. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Ros, E.; Salas-Salvado, J.; Covas, M.I.; Corella, D.; Aros, F.; Gomez-Gracia, E.; Ruiz-Gutierrez, V.; Fiol, M.; Lapetra, J.; et al. Primary prevention of cardiovascular disease with a Mediterranean diet. N. Eng. J. Med. 2013, 368, 1279–1290. [Google Scholar] [CrossRef] [PubMed]
- Guasch-Ferre, M.; Hu, F.B.; Martinez-Gonzalez, M.A.; Fito, M.; Bullo, M.; Estruch, R.; Ros, E.; Corella, D.; Recondo, J.; Gomez-Gracia, E.; et al. Olive oil intake and risk of cardiovascular disease and mortality in the PREDIMED Study. BMC Med. 2014, 12, 78. [Google Scholar] [CrossRef]
- Alhassan, A.; Young, J.; Lean, M.E.J.; Lara, J. Consumption of fish and vascular risk factors: A systematic review and meta-analysis of intervention studies. Atherosclerosis 2017, 266, 87–94. [Google Scholar] [CrossRef]
- Valderas-Martinez, P.; Chiva-Blanch, G.; Casas, R.; Arranz, S.; Martinez-Huelamo, M.; Urpi-Sarda, M.; Torrado, X.; Corella, D.; Lamuela-Raventos, R.M.; Estruch, R. Tomato Sauce Enriched with Olive Oil Exerts Greater Effects on Cardiovascular Disease Risk Factors than Raw Tomato and Tomato Sauce: A Randomized Trial. Nutrients 2016, 8, 170. [Google Scholar] [CrossRef]
- Kim, Y.; Keogh, J.B.; Clifton, P.M. Consumption of red and processed meat and refined grains for 4weeks decreases insulin sensitivity in insulin-resistant adults: A randomized crossover study. Metab. Clin. Exp. 2017, 68, 173–183. [Google Scholar] [CrossRef]
- Jiang, X.; Fan, X.; Wu, R.; Geng, F.; Hu, C. The effect of care intervention for obese patients with type II diabetes. Medicine 2017, 96, e7524. [Google Scholar] [CrossRef] [Green Version]
- Hayashino, Y.; Suzuki, H.; Yamazaki, K.; Goto, A.; Izumi, K.; Noda, M. A cluster randomized trial on the effect of a multifaceted intervention improved the technical quality of diabetes care by primary care physicians: The Japan Diabetes Outcome Intervention Trial-2 (J-DOIT2). Diabetes Med. 2016, 33, 599–608. [Google Scholar] [CrossRef]
- Johansen, M.Y.; MacDonald, C.S.; Hansen, K.B.; Karstoft, K.; Christensen, R.; Pedersen, M.; Hansen, L.S.; Zacho, M.; Wedell-Neergaard, A.S.; Nielsen, S.T.; et al. Effect of an Intensive Lifestyle Intervention on Glycemic Control in Patients with Type 2 Diabetes: A Randomized Clinical Trial. JAMA 2017, 318, 637–646. [Google Scholar] [CrossRef] [PubMed]
- Paula, T.P.; Viana, L.V.; Neto, A.T.; Leitao, C.B.; Gross, J.L.; Azevedo, M.J. Effects of the DASH Diet and Walking on Blood Pressure in Patients With Type 2 Diabetes and Uncontrolled Hypertension: A Randomized Controlled Trial. J. Clin. Hypertens. 2015, 17, 895–901. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Control Group (102) | Intervention Group (102) | p-Value | |
|---|---|---|---|
| Age (years), mean (SD) | 60.4 (8.4) | 60.8 (7.8) | 0.84 |
| Gender (female), n (%) | 41 (40.2) | 52 (51.1) | 0.08 |
| Diabetes duration (years), mean (SD) | 6.7 (4.7) | 6.4 (4.6) | 0.62 |
| BMI (kg/m2), mean (SD) | 30.3 (5.6) | 29.5 (4.2) | 0.27 |
| Obesity, n (%) | 48 (47.1) | 43 (42.2) | 0.48 |
| Work situation, n (%) | |||
| Works outside home | 41 (40.2) | 29 (28.4) | 0.91 |
| Homemaker | 18 (17.6) | 24 (23.5) | |
| Retired | 34 (33.3) | 44 (43.1) | |
| Unemployed | 7 (6.8) | 5 (4.9) | |
| Educational level, n (%) | |||
| University studies | 17 (16.7) | 17 (16.7) | 0.94 |
| Middle or high school | 33 (32.4) | 37 (36.3) | |
| Elementary school | 52 (51.0) | 48 (47.1) | |
| Smoking, n (%) | |||
| Non-smoker | 37 (36.3) | 39 (38.2) | 0.13 |
| Smoker | 26 (25.5) | 10 (9.8) | |
| Former smoker | 39 (38.2) | 53 (51.9) | |
| Medication use, n (%) | |||
| Antihypertensive drugs | 55 (53.9) | 58 (56.9) | 0.24 |
| Lipid-lowering drugs | 59 (57.8) | 58 (52.0) | 0.39 |
| Antidiabetic drugs | 89 (87.3) | 93.0 (91.2) | 0.37 |
| Insulins | 18 (17.6) | 12 (11.8) | 0.24 |
| Metformin | 81 (79.4) | 82 (80.4) | 0.86 |
| Sulphonylureas | 8 (7.8) | 6 (5.9) | 0.58 |
| Thiazolidinediones | 3 (2.9) | 3 (2.9) | 1.0 |
| SGLT2 Inhibitors | 1 (1.0) | 2 (2.0) | 0.56 |
| Meglitinides | 2 (2.0) | 4 (3.9) | 0.41 |
| DPP-4 inhibitors | 38 (37.3) | 37 (36.3) | 0.89 |
| GLP-1 receptor agonists | 1 (1.0) | 4 (3.9) | 0.18 |
| Baseline | 3-Month Follow Up | 12-Month Follow Up | ||||
|---|---|---|---|---|---|---|
| Control Group | Intervention Group | Control Group | Intervention Group | Control Group | Intervention Group | |
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | |
| Total score (points) | ||||||
| Mediterranean Diet Adherence Screener | 6.9 (1.7) | 7.2 (1.9) | 7.1 (1.7) | 9.4 (1.7) | 7.0 (1.9) | 8.5 (1.9) |
| Diet Quality Index | 40.2 (2.6) | 39.8 (2.6) | 40.8 (2.7) | 42.9 (2.5) | 40.4 (2.7) | 41.8 (2.8) |
| Mediterranean diet criteria (%) | ||||||
| Use olive oil as main culinary fat | 89.0 (31.2) | 96.0 (19.5) | 92.0 (27.8) | 99.0 (10.1) | 88.0 (32.8) | 98.0 (14.3) |
| Olive oil ≥ 4 tablespoons | 15.0 (35.6) | 17.0 (37.5) | 17.0 (37.5) | 43.0 (49.7) | 20.0 (40.1) | 48.0 (50.2) |
| Vegetables ≥ 2 servings/day | 20.0 (39.9) | 24.0 (42.6) | 23.0 (42.3) | 52.0 (50.2) | 22.0 (41.6) | 34.0 (47.6) |
| Fruits ≥ 3 servings/day | 51.0 (50.2) | 54.0 (50.1) | 59.0 (49.4) | 76.0 (43.2) | 57.0 (49.8) | 64.0 (48.3) |
| Red or processed meats < 1 serving/day | 97.0 (17.0) | 91.0 (28.5) | 96.0 (20.1) | 93.0 (25.9) | 91.0 (28.5) | 92.0 (27.7) |
| Butter, cream or margarine <1 serving/day | 92.0 (27.0) | 86.0 (34.6) | 93.0 (26.1) | 93.0 (26.7) | 95.0 (22.9) | 91.5 (26.4) |
| Sugar-sweetened beverage < 1 cup/day | 76.0 (42.6) | 88.0 (32.4) | 87.0 (33.2) | 97.0 (17.3) | 86.0 (35.2) | 93.0 (25.1) |
| Red wine ≥ 7 servings/week | 15.0 (35.6) | 19.0 (39.1) | 12.0 (33.2) | 20.0 (40.5) | 14.0 (35.2) | 15.0 (36.3) |
| Legumes ≥ 3 servings/week | 19.0 (39.1) | 21.0 (40.6) | 26.0 (44.1) | 34.0 (47.5) | 25.0 (43.7) | 26.0 (44.0) |
| Fish or seafood ≥ 3 servings/week | 42.0 (49.6) | 51.0 (50.2) | 47.0 (50.2) | 66.0 (47.5) | 44.0 (49.9) | 61.0 (49.1) |
| Commercial bakery ≤ 2 servings/week | 47.0 (50.2) | 32.0 (47.0) | 38.0 (48.7) | 46.0 (50.1) | 31.0 (46.4) | 29.0 (45.5) |
| Nuts ≥ 3 servings/week | 24.0 (42.6) | 27.0 (44.8) | 28.0 (45.2) | 51.0 (50.2) | 20.0 (40.1) | 42.0 (49.7) |
| White meats more than red meats | 58.0 (49.6) | 71.0 (45.8) | 56.0 (49.9) | 89.0 (31.7) | 66.0 (47.7) | 87.0 (34.2) |
| Use of sofrito sauce ≥ 2 servings/week | 49.0 (50.2) | 48.0 (50.0) | 39.0 (48.9) | 83.0 (38.1) | 45.0 (50.0) | 66.0 (47.6) |
| 3 Months vs. Baseline | 12 Months vs. Baseline | |||
|---|---|---|---|---|
| Mean (95% CI) | p | Mean (95% CI) | p | |
| Total score (points) | ||||
| Mediterranean Diet Adherence Screener | 2.2 (1.8–2.5) | <0.001 | 1.3 (0.8–1.8) | <0.001 |
| Diet Quality Index | 2.5 (1.9–3.0) | <0.001 | 1.7 (1.0–2.4) | <0.001 |
| Mediterranean diet criteria (%) | ||||
| Use olive oil as main culinary fat | 4.3 (−5.0–9.1) | 0.080 | 0.8 (1.4–14.5) | 0.017 |
| Olive oil ≥ 4 tablespoons | 25.9 (14.3–37.5) | <0.001 | 28.4 (15.5–41.4) | <0.001 |
| Vegetables ≥ 2 servings/day | 26.8 (16.1–37.5) | <0.001 | 10.8 (1.6–23.2) | 0.087 |
| Fruits ≥ 3 servings/day | 15.0 (4.8–25.2) | 0.004 | 4.9 (−7.6–17.3) | 0.441 |
| Red or processed meats < 1 serving/day | 3.4 (−10.0–3.2) | 0.313 | 1.1 (−7.1–9.2) | 0.793 |
| Butter, cream or margarine < 1 serving/day | 3.7 (−2.1–9.6) | 0.211 | 3.2 (−1.7–8.9) | 0.325 |
| Sugar-sweetened beverage < 1 cup/day | 5.4 (−1.2–11.9) | 0.109 | 2.2 (−6.2–10.5) | 0.608 |
| Red wine ≥ 7 servings/week | 5.3 (−2.3–12.8) | 0.169 | −0.3 (−7.6–7.1) | 0.945 |
| Legumes ≥ 3 servings/week | 6.6 (−5.7–18.8) | 0.292 | 0.6 (−11.4–12.5) | 0.926 |
| Fish or seafood ≥ 3 servings/week | 12.8 (2.3–23.4) | 0.018 | 12.9 (0.2–25.6) | 0.046 |
| Commercial bakery ≤ 2 servings/week | 18.1 (6.1–30.0) | 0.003 | 3.9 (−8.5–16.2) | 0.537 |
| Nuts ≥ 3 servings/week | 22.1 (10.1–34.1) | <0.001 | 21.9 (9.9–33.9) | <0.001 |
| White meats more than red meats | 27.3 (17.3–37.3) | <0.001 | 16.1 (5.4–26.9) | 0.004 |
| Use of sofrito sauce ≥ 2 servings/week | 44.1 (31.8–56.4) | <0.001 | 21.0 (7.0–35.0) | 0.004 |
| Baseline | 3-Month Follow Up | 12-Month Follow Up | ||||
|---|---|---|---|---|---|---|
| Control Group | Intervention Group | Control Group | Intervention Group | Control Group | Intervention Group | |
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | |
| Glycated haemoglobin (%) | 6.8 (1.2) | 6.9 (1.2) | 6.8 (1.1) | 6.8 (1.0) | 7.0 (1.3) | 6.9 (1.1) |
| Postprandial glucose (mg/dL) | 147.6 (35.5) | 149.2 (39.0) | 148.9 (37.8) | 140.0 (31.7) | 148.3 (34.1) | 143.2 (29.0) |
| Atherogenic index | 3.8 (1.1) | 3.5 (1.0) | 3.7 (1.1) | 3.4 (1.0) | 3.6 (1.1) | 3.4 (1.1) |
| Total serum cholesterol (mg/dL) | 176.4 (31.7) | 178.8 (30.3) | 173.1 (29.0) | 173.7 (30.6) | 173.0 (32.5) | 174.8 (34.0) |
| LDL-cholesterol (mg/dL) | 100.4 (28.6) | 101.8 (30.0) | 97.9 (24.9) | 97.2 (27.9) | 94.9 (25.3) | 95.6 (31.6) |
| HDL-cholesterol (mg/dL) | 50.3 (14.8) | 54.4 (14.1) | 49.8 (13.6) | 54.0 (14.6) | 51.4 (13.5) | 54.1 (14.8) |
| Waist circumference (cm) | 104.9 (13.1) | 102.2 (11.5) | 105.5 (13.0) | 100.4 (11.0) | 104.2 (16.0) | 101.2 (11.8) |
| Systolic blood pressure (mmHg) | 135.0 (33.2) | 133.2 (15.9) | 131.2 (16.4) | 127.1 (15.9) | 130.3 (16.4) | 126.2 (15.8) |
| Diastolic blood pressure (mmHg) | 80.5 (9.6) | 80.8 (9.0) | 79.7 (9.6) | 78.8 (9.5) | 80.6 (8.8) | 79.4 (8.5) |
| ABSI × 100 | 8.5 (0.5) | 8.5 (0.4) | 8.5 (0.6) | 8.3 (0.4) | 8.5 (0.7) | 8.4 (0.4) |
| 3 Months vs. Baseline | 12 Months vs. Baseline | |||
|---|---|---|---|---|
| Mean (95% CI) | p | Mean (95% CI) | p | |
| Glycated haemoglobin (%) | −0.1 (−0.3–0.0) | 0.145 | −0.1 (−0.4–0.1) | 0.241 |
| Postprandial glucose (mg/dL) | −9.4 (−18.0–−0.8) | 0.031 | −6.6 (−14.9–1.7) | 0.118 |
| Atherogenic index | −0.1 (−0.3–0.1) | 0.324 | 0.0 (−0.2–0.2) | 0.998 |
| Total serum cholesterol (mg/dL) | −1.8 (−8.1–4.5) | 0.567 | −0.9 (−8.5–6.8) | 0.823 |
| LDL-cholesterol (mg/dL) | −2.6 (−8.3–3.2) | 0.380 | −0.1 (−6.5–6.3) | 0.973 |
| HDL-cholesterol (mg/dL) | 0.8 (−1.5–3.1) | 0.501 | −0.1 (−2.4–2.2) | 0.927 |
| Waist circumference (cm) | −2.5 (−3.3–−1.6) | <0.001 | −0.9 (−3.1–1.2) | 0.390 |
| Systolic blood pressure (mmHg) | −3.1 (−7.1–0.8) | 0.120 | −1.5 (−8.7–5.7) | 0.678 |
| Diastolic blood pressure (mmHg) | −1.2 (−3.3–0.9) | 0.244 | −1.3 (−3.5–0.8) | 0.227 |
| ABSI × 100 | 0.1 (−0.2–−0.1) | 0.001 | 0.1 (−0.2–0.0) | 0.198 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alonso-Domínguez, R.; García-Ortiz, L.; Patino-Alonso, M.C.; Sánchez-Aguadero, N.; Gómez-Marcos, M.A.; Recio-Rodríguez, J.I. Effectiveness of A Multifactorial Intervention in Increasing Adherence to the Mediterranean Diet among Patients with Diabetes Mellitus Type 2: A Controlled and Randomized Study (EMID Study). Nutrients 2019, 11, 162. https://doi.org/10.3390/nu11010162
Alonso-Domínguez R, García-Ortiz L, Patino-Alonso MC, Sánchez-Aguadero N, Gómez-Marcos MA, Recio-Rodríguez JI. Effectiveness of A Multifactorial Intervention in Increasing Adherence to the Mediterranean Diet among Patients with Diabetes Mellitus Type 2: A Controlled and Randomized Study (EMID Study). Nutrients. 2019; 11(1):162. https://doi.org/10.3390/nu11010162
Chicago/Turabian StyleAlonso-Domínguez, Rosario, Luis García-Ortiz, Maria C. Patino-Alonso, Natalia Sánchez-Aguadero, Manuel A. Gómez-Marcos, and José I. Recio-Rodríguez. 2019. "Effectiveness of A Multifactorial Intervention in Increasing Adherence to the Mediterranean Diet among Patients with Diabetes Mellitus Type 2: A Controlled and Randomized Study (EMID Study)" Nutrients 11, no. 1: 162. https://doi.org/10.3390/nu11010162
APA StyleAlonso-Domínguez, R., García-Ortiz, L., Patino-Alonso, M. C., Sánchez-Aguadero, N., Gómez-Marcos, M. A., & Recio-Rodríguez, J. I. (2019). Effectiveness of A Multifactorial Intervention in Increasing Adherence to the Mediterranean Diet among Patients with Diabetes Mellitus Type 2: A Controlled and Randomized Study (EMID Study). Nutrients, 11(1), 162. https://doi.org/10.3390/nu11010162