Cultural Differences in Diet and Determinants of Diet Quality in Switzerland: Results from the National Nutrition Survey menuCH

 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Dietary Assessment
2.3. Diet Quality Scores
2.4. Sociodemographic and Lifestyle Variables
2.5. Weighting Strategy
2.6. Statistical Analysis
3. Results
3.1. Characteristics of the Participants
3.2. Determinants of Diet Quality
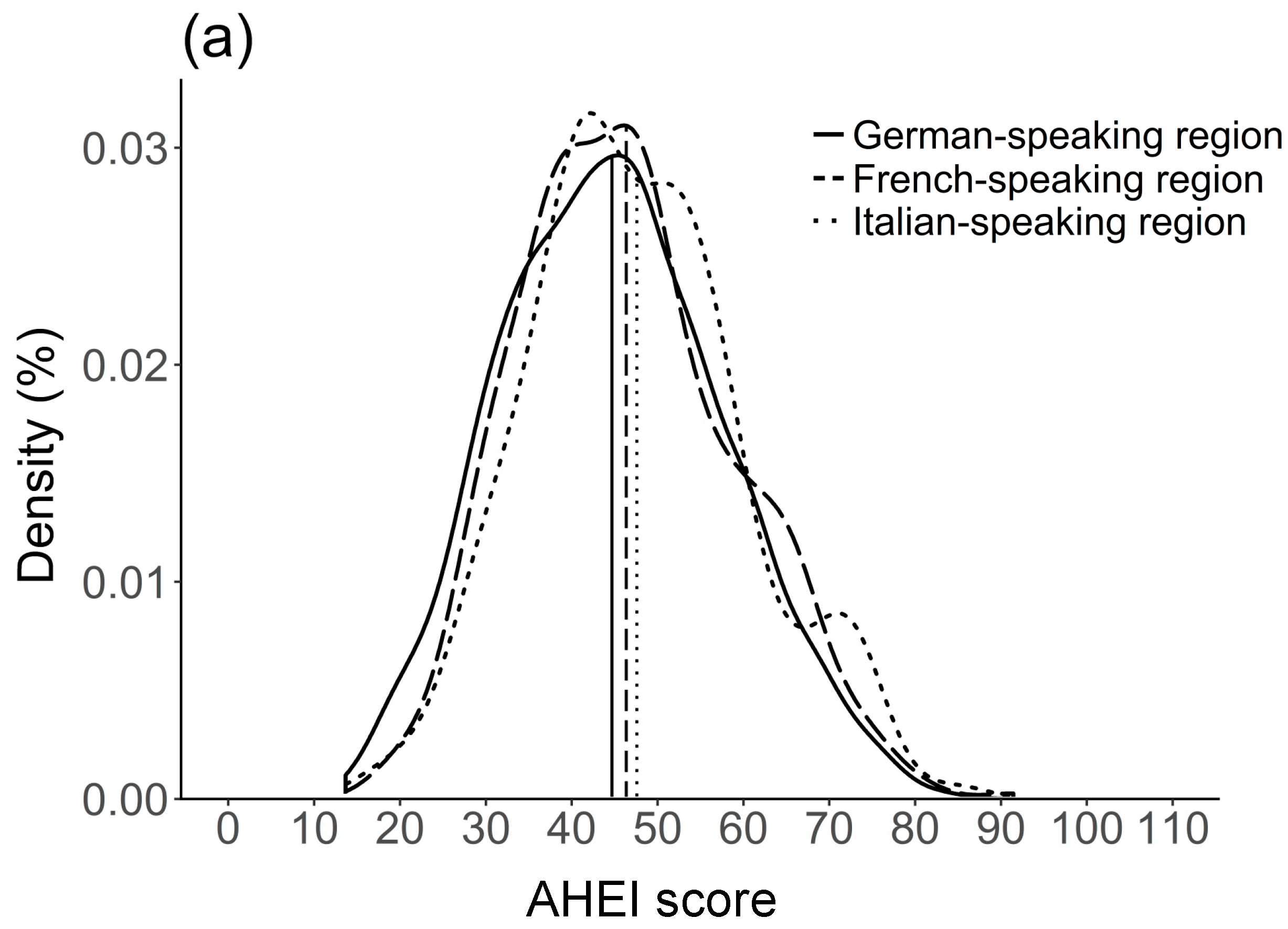
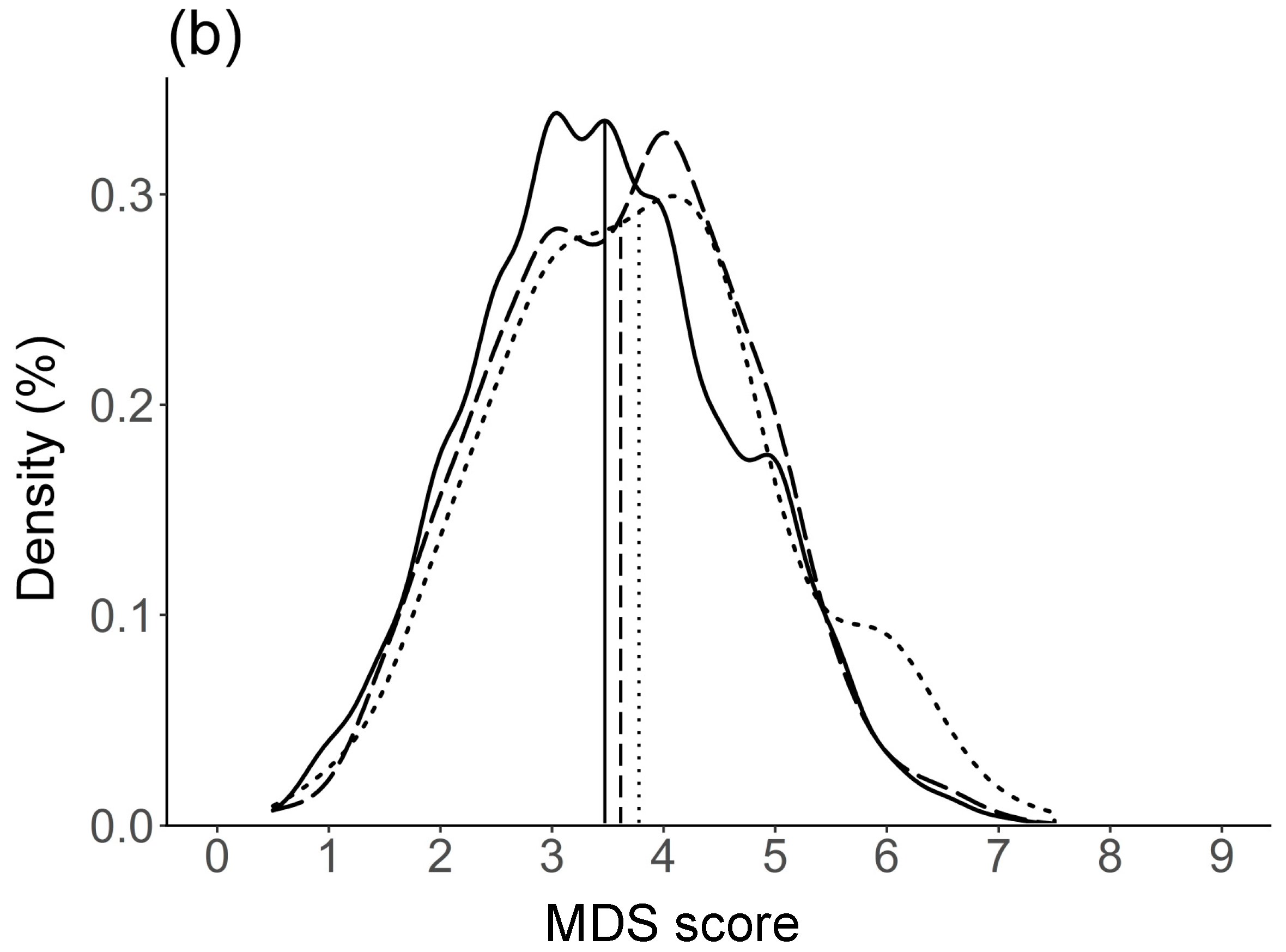
3.3. Differences in Single Components of Diet Quality Scores by Language Region
3.4. Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Global Action Plan for the Prevention and Control of Noncommunicable Diseases 2013–2020; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- World Health Organization (WHO). Diet, Nutrition and the Prevention of Chronic Diseases: Report of a Joint WHO/FAO Expert Consultation; WHO: Geneva, Switzerland, 2002. [Google Scholar]
- Schwingshackl, L.; Bogensberger, B.; Hoffmann, G. Diet Quality as Assessed by the Healthy Eating Index, Alternate Healthy Eating Index, Dietary Approaches to Stop Hypertension Score, and Health Outcomes: An Updated Systematic Review and Meta-Analysis of Cohort Studies. J. Acad. Nutr. Diet. 2018, 118, 74–100. [Google Scholar] [CrossRef] [PubMed]
- Waijers, P.M.C.M.; Feskens, E.J.M.; Ocké, M.C. A critical review of predefined diet quality scores. Br. J. Nutr. 2007, 97, 219–231. [Google Scholar] [CrossRef] [PubMed]
- Arvaniti, F.; Panagiotakos, D.B. Healthy indexes in public health practice and research: A review. Crit. Rev. Food Sci. Nutr. 2008, 48, 317–327. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef]
- Wirt, A.; Collins, C.E. Diet quality—What is it and does it matter? Public Health Nutr. 2009, 12, 2473–2492. [Google Scholar] [CrossRef] [PubMed]
- Chiuve, S.E.; Fung, T.T.; Rimm, E.B.; Hu, F.B.; McCullough, M.L.; Wang, M.; Stampfer, M.J.; Willett, W.C. Alternative dietary indices both strongly predict risk of chronic disease. J. Nutr. 2012, 142, 1009–1018. [Google Scholar] [CrossRef]
- Trichopoulos, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean Diet and Survival in a Greek Population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [PubMed]
- Kant, A.K. Dietary patterns and health outcomes. J. Am. Diet. Assoc. 2004, 104, 615–635. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Macchi, C.; Abbate, R.; Gensini, G.F.; Casini, A. Mediterranean diet and health status: An updated meta-analysis and a proposal for a literature-based adherence score. Public Health Nutr. 2013, 17, 2769–2782. [Google Scholar] [CrossRef] [PubMed]
- Ocké, M.C. Evaluation of methodologies for assessing the overall diet: Dietary quality scores and dietary pattern analysis. Proc. Nutr. Soc. 2013, 72, 191–199. [Google Scholar] [CrossRef]
- Hiza, H.A.B.; Casavale, K.O.; Guenther, P.M.; Davis, C.A. Diet Quality of Americans Differs by Age, Sex, Race/Ethnicity, Income, and Education Level. J. Acad. Nutr. Diet. 2013, 113, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Darmon, N.; Drewnowski, A. Does social class predict diet quality? Am. J. Clin. Nutr. 2008, 87, 1107–1117. [Google Scholar] [CrossRef] [PubMed]
- Patino-Alonso, M.C.; Recio-Rodríguez, J.I.; Magdalena Belio, J.F.; Colominas-Garrido, R.; Lema-Bartolomé, J.; Arranz, A.G.; Agudo-Conde, C.; Gomez-Marcos, M.A.; García-Ortiz, L. Factors associated with adherence to the mediterranean diet in the adult population. J. Acad. Nutr. Diet. 2014, 114, 583–589. [Google Scholar] [CrossRef]
- Federal Department of Home Affairs (FDHA). Eating Well and Staying Healthy—Swiss Nutrition Policy 2017–2024; Federal Food Safety and Veterinary Office (FSVO): Bern, Switzerland, 2017. [Google Scholar]
- Slimani, N.; Fahey, M.T.; Welch, A.A.; Wirfält, E.; Stripp, C.; Bergström, E.T.; Linseisen, J.; Schulze, M.B.; Bamia, C.; Chloptsios, Y.; et al. Diversity of dietary patterns observed in the European Prospective Investigation into Cancer and Nutrition (EPIC) project. Public Health Nutr. 2002, 5, 1311–1328. [Google Scholar] [CrossRef] [PubMed]
- Freisling, H.; Fahey, M.T.; Moskal, A.; Ocké, M.C.; Ferrari, P.; Jenab, M.; Norat, T.; Naska, A.; Welch, A.A.; Navarro, C.; et al. Region-Specific Nutrient Intake Patterns Exhibit a Geographical Gradient within and between European Countries. J. Nutr. 2010, 140, 1280–1286. [Google Scholar] [CrossRef] [PubMed]
- Naska, A.; Fouskakis, D.; Oikonomou, E.; Almeida, M.D.V.; Berg, M.A.; Gedrich, K.; Moreiras, O.; Nelson, M.; Trygg, K.; Turrini, A.; et al. Dietary patterns and their socio-demographic determinants in 10 European countries: Data from the DAFNE databank. Eur. J. Clin. Nutr. 2006, 60, 181–190. [Google Scholar] [CrossRef] [PubMed]
- Faeh, D.; Minder, C.; Gutzwiller, F.; Bopp, M. Culture, risk factors and mortality: Can Switzerland add missing pieces to the European puzzle? J. Epidemiol. Community Health 2009, 63, 639–645. [Google Scholar] [CrossRef] [PubMed]
- Vormund, K.; Braun, J.; Rohrmann, S.; Bopp, M.; Ballmer, P.; Faeh, D. Mediterranean diet and mortality in Switzerland: An alpine paradox? Eur. J. Nutr. 2015, 54, 139–148. [Google Scholar] [CrossRef]
- Richard, A.; Faeh, D.; Rohrmann, S.; Braun, J.; Tarnutzer, S.; Bopp, M. Italianity is associated with lower risk of prostate cancer mortality in Switzerland. Cancer Causes Control 2014, 25, 1523–1529. [Google Scholar] [CrossRef]
- Chammartin, F.; Probst-Hensch, N.; Utzinger, J.; Vounatsou, P. Mortality atlas of the main causes of death in Switzerland, 2008–2012. Swiss Med. Wkly. 2016, 146, w14280. [Google Scholar] [CrossRef]
- Marques-Vidal, P.; Waeber, G.; Vollenweider, P.; Bochud, M.; Stringhini, S.; Guessous, I. Sociodemographic and behavioural determinants of a healthy diet in Switzerland. Ann. Nutr. Metab. 2015, 67, 87–95. [Google Scholar] [CrossRef] [PubMed]
- De Abreu, D.; Guessous, I.; Vaucher, J.; Preisig, M.; Waeber, G.; Vollenweider, P.; Marques-Vidal, P. Low compliance with dietary recommendations for food intake among adults. Clin. Nutr. 2013, 32, 783–788. [Google Scholar] [CrossRef] [PubMed]
- Marques-Vidal, P.; Waeber, G.; Vollenweider, P.; Guessous, I. Socio-demographic and lifestyle determinants of dietary patterns in French-speaking Switzerland, 2009–2012. BMC Public Health 2018, 18, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Chatelan, A.; Beer-Borst, S.; Randriamiharisoa, A.; Pasquier, J.; Blanco, J.M.; Siegenthaler, S.; Paccaud, F.; Slimani, N.; Nicolas, G.; Camenzind-Frey, E.; et al. Major differences in diet across three linguistic regions of Switzerland: Results from the first national nutrition survey menuCH. Nutrients 2017, 9, 1163. [Google Scholar] [CrossRef] [PubMed]
- Krieger, J.P.; Cabaset, S.; Pestoni, G.; Rohrmann, S.; Faeh, D.; Egger, M.; Spoerri, A.; Zwahlen, M.; Puhan, M.; Bopp, M.; et al. Dietary patterns are associated with cardiovascular and cancer mortality among Swiss adults in a census-linked cohort. Nutrients 2018, 10, 313. [Google Scholar] [CrossRef] [PubMed]
- Marques-Vidal, P.; Gaspoz, J.M.; Theler, J.M.; Guessous, I. Twenty-year trends in dietary patterns in French-speaking Switzerland: Toward healthier eating. Am. J. Clin. Nutr. 2017, 106, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Schneid Schuh, D.; Campos Pellanda, L.; Guessous, I.; Marques-Vidal, P. Trends and determinants of change in compliance to dietary guidelines in a Swiss community-dwelling sample. Prev. Med. 2018, 111, 198–203. [Google Scholar] [CrossRef] [PubMed]
- Chatelan, A.; Marques-Vidal, P.; Bucher, S.; Siegenthaler, S.; Metzger, N.; Zuberbühler, C.A.; Camenzind-Frey, E.; Reggli, A.; Bochud, M.; Beer-Borst, S. Lessons Learnt About Conducting a Multilingual Nutrition Survey in Switzerland: Results from menuCH Pilot Survey. Int. J. Vitam. Nutr. Res. 2018, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Lachat, C.; Hawwash, D.; Ocké, M.C.; Berg, C.; Forsum, E.; Hörnell, A.; Larsson, C.; Sonestedt, E.; Wirfält, E.; Åkesson, A.; et al. Strengthening the Reporting of Observational Studies in Epidemiology—Nutritional Epidemiology (STROBE-nut): An Extension of the STROBE Statement. PLoS Med. 2016, 13, 1–15. [Google Scholar] [CrossRef] [PubMed]
- ISRCTN registry. Available online: https://doi.org/10.1186/ISRCTN16778734 (accessed on 24 July 2018).
- Slimani, N.; Casagrande, C.; Nicolas, G.; Freisling, H.; Huybrechts, I.; Ocké, M.C.; Niekerk, E.M.; van Rossum, C.; Bellemans, M.; De Maeyer, M.; et al. The standardized computerized 24-h dietary recall method EPIC-Soft adapted for pan-European dietary monitoring. Eur. J. Clin. Nutr. 2011, 65, S5–S15. [Google Scholar] [CrossRef]
- Crispim, S.P.; de Vries, J.H.M.; Geelen, A.; Souverein, O.W.; Hulshof, P.J.M.; Lafay, L.; Rousseau, A.S.; Lillegaard, I.T.L.; Andersen, L.F.; Huybrechts, I.; et al. Two non-consecutive 24h recalls using EPIC-Soft software are sufficiently valid for comparing protein and potassium intake between five European centres—Results from the European Food Consumption Validation (EFCOVAL) study. Br. J. Nutr. 2011, 105, 447–458. [Google Scholar] [CrossRef] [PubMed]
- Camenzind-Frey, E.; Zuberbühler, C. menuCH—Schweizerisches Fotobuch/Livre Photo Suisse/Manuale Fotografico Svizzero; Federal Office of Public Health (FOPH) and Federal Food Safety and Veterinary Office (FSVO): Bern, Switzerland, 2014. [Google Scholar]
- Federal Food Safety and Veterinary Office (FSVO). Swiss Food Composition Database. Available online: http://naehrwertdaten.ch/request?xml=MessageData&xml=MetaData&xsl=Start&lan=en&pageKey=Start (accessed on 23 July 2018).
- World Health Organization (WHO). MONICA Manual, Part III: Population survey. Section 1: Population Survey Data Components. 4.6 Height, Weight, Waist and Hip Measurement; WHO: Geneva, Switzerland, December 1997. [Google Scholar]
- Pasquier, J.; Chatelan, A.; Bochud, M. Weighting strategy. April 2017. Available online: https://menuch.iumsp.ch/index.php/catalog/4/download/17 (accessed on 24 July 2018).
- Van Buuren, S.; Groothuis-Oudshoorn, K. mice: Multivariate Imputation by Chained Equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef]
- Lumley, T. Analysis of Complex Survey Samples. J. Stat. Softw. 2004, 9, 1–19. [Google Scholar] [CrossRef]
- Wang, D.D.; Leung, C.W.; Li, Y.; Ding, E.L.; Chiuve, S.E.; Hu, F.B.; Willett, W.C. Trends in dietary quality among adults in the United States, 1999 through 2010. JAMA Intern. Med. 2014, 174, 1587–1595. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Hebert, J.R.; Kivimaki, M.; Akbaraly, T. Alternate Healthy Eating Index 2010, Dietary Inflammatory Index and risk of mortality: Results from the Whitehall II cohort study and meta-analysis of previous Dietary Inflammatory Index and mortality studies. Br. J. Nutr. 2017, 118, 210–221. [Google Scholar] [CrossRef] [PubMed]
- Neelakantan, N.; Naidoo, N.; Koh, W.-P.; Yuan, J.-M.; van Dam, R.M. The Alternative Healthy Eating Index Is Associated with a Lower Risk of Fatal and Nonfatal Acute Myocardial Infarction in a Chinese Adult Population. J. Nutr. 2016, 146, 1379–1386. [Google Scholar] [CrossRef] [PubMed]
- Imamura, F.; Micha, R.; Khatibzadeh, S.; Fahimi, S.; Shi, P.; Powles, J.; Mozaffarian, D. Dietary quality among men and women in 187 countries in 1990 and 2010: A systematic assessment. Lancet Glob. Health 2015, 3, e132–e142. [Google Scholar] [CrossRef]
- De Mestral, C.; Marques-Vidal, P.; Gaspoz, J.-M.; Theler, J.-M.; Guessous, I. Independent association between socioeconomic indicators and macro- and micro-nutrient intake in Switzerland. PLoS ONE 2017, 12, e0174578. [Google Scholar] [CrossRef]
- Rothman, R.L.; Housam, R.; Weiss, H.; Davis, D.; Gregory, R.; Gebretsadik, T.; Shintani, A.; Elasy, T.A. Patient Understanding of Food Labels—The Role of Literacy and Numeracy. Am. J. Prev. Med. 2006, 31, 391–398. [Google Scholar] [CrossRef]
- Fine, L.J.; Philogene, G.S.; Gramling, R.; Coups, E.J.; Sinha, S. Prevalence of multiple chronic disease risk factors: 2001 National Health Interview Survey. Am. J. Prev. Med. 2004, 27, 18–24. [Google Scholar] [CrossRef]
- Pronk, N.P.; Anderson, L.H.; Crain, A.L.; Martinson, B.C.; O’Connor, P.J.; Sherwood, N.E.; Whitebird, R.R. Meeting recommendations for multiple healthy lifestyle factors: Prevalence, clustering, and predictors among adolescent, adult, and senior health plan members. Am. J. Prev. Med. 2004, 27, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Tapsell, L.C.; Neale, E.P.; Satija, A.; Hu, F.B. Foods, Nutrients, and Dietary Patterns: Interconnections and Implications for Dietary Guidelines. Adv. Nutr. An Int. Rev. J. 2016, 7, 445–454. [Google Scholar] [CrossRef] [PubMed]
- Krieger, J.P.; Pestoni, G.; Cabaset, S.; Brombach, C.; Sych, J.; Schader, C.; Faeh, D.; Rohrmann, S. Dietary patterns and their sociodemographic and lifestyle determinants in Switzerland: Results from the national nutrition survey menuCH. Nutrients 2018, 11, 62. [Google Scholar] [CrossRef] [PubMed]
- Swiss Health Observatory (OBSAN) Indicators. Available online: https://www.obsan.admin.ch/de/indikatoren (accessed on 8 August 2018).
- Schulze, M.B.; Martínez-González, M.A.; Fung, T.T.; Lichtenstein, A.H.; Forouhi, N.G. Food based dietary patterns and chronic disease prevention. Br. Med. J. 2018, 361, k2396. [Google Scholar] [CrossRef] [PubMed]
- Moeller, S.M.; Reedy, J.; Millen, A.E.; Dixon, L.B.; Newby, P.K.; Tucker, K.L.; Krebs-Smith, S.M.; Guenther, P.M. Dietary Patterns: Challenges and Opportunities in Dietary Patterns Research. An Experimental Biology Workshop, April 1, 2006. J. Am. Diet. Assoc. 2007, 107, 1233–1239. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Overall | German-Speaking Region e | French-Speaking Region e | Italian-Speaking Region e | |
|---|---|---|---|---|
| Number of participants | 2057 | 1341 | 502 | 214 |
| Weighted | 4,627,878 | 3,203,780 | 1,167,173 | 256,925 |
| Sex (%) | ||||
| Males | 49.8 | 51.1 | 46.5 | 48.4 |
| Females | 50.2 | 48.9 | 53.5 | 51.6 |
| Age groups c (%) | ||||
| 18–29 years | 18.8 | 18.4 | 19.6 | 19.2 |
| 30–44 years | 29.9 | 29.5 | 31.0 | 29.4 |
| 45–59 years | 29.8 | 28.9 | 32.5 | 29.5 |
| 60–75 years | 21.6 | 23.2 | 16.9 | 22.0 |
| BMI categories d (%) | ||||
| Underweight | 2.4 | 2.6 | 2.1 | 2.1 |
| Normal weight | 54.1 | 53.8 | 55.3 | 52.7 |
| Overweight | 30.6 | 30.8 | 30.2 | 29.9 |
| Obese | 12.9 | 12.8 | 12.4 | 15.4 |
| Nationality (%) | ||||
| Swiss only | 61.4 | 66.3 | 49.9 | 53.3 |
| Swiss binational | 13.8 | 12.4 | 18.0 | 11.9 |
| Non-Swiss | 24.8 | 21.3 | 32.1 | 34.7 |
| Education, highest degree (%) | ||||
| Primary/no degree | 4.7 | 3.6 | 6.4 | 10.3 |
| Secondary | 42.6 | 41.3 | 44.5 | 49.6 |
| Tertiary | 52.6 | 54.9 | 49.0 | 40.1 |
| Household type (%) | ||||
| Living alone | 18.1 | 16.3 | 22.7 | 20.0 |
| Couple without children | 31.7 | 34.4 | 24.9 | 29.0 |
| Couple with children | 32.8 | 31.4 | 36.1 | 35.1 |
| One-parent family with children | 4.4 | 3.9 | 6.0 | 3.2 |
| Adult living with parents | 7.1 | 6.7 | 7.9 | 8.9 |
| Others | 5.7 | 7.1 | 2.3 | 3.8 |
| Gross household income (%) | ||||
| <6000 (CHF/month) | 17.7 | 17.5 | 17.6 | 20.4 |
| 6000–13,000 (CHF/month) | 39.8 | 41.1 | 37.3 | 35.8 |
| >13,000 (CHF/month) | 14.9 | 16.3 | 13.2 | 4.2 |
| Did not answer | 27.6 | 25.1 | 31.9 | 39.6 |
| Self-reported physical activity (%) | ||||
| Low | 12.9 | 13.9 | 9.7 | 14.6 |
| Moderate | 22.7 | 22.5 | 22.9 | 24.0 |
| High | 40.3 | 40.3 | 41.4 | 34.8 |
| Did not answer | 24.2 | 23.3 | 26.0 | 26.5 |
| Smoking status (%) | ||||
| Never | 42.9 | 43.3 | 42.3 | 40.4 |
| Former | 33.6 | 32.6 | 36.2 | 34.4 |
| Current | 23.3 | 23.8 | 21.3 | 25.2 |
| Self-reported health (%) | ||||
| Very bad to medium | 12.7 | 10.9 | 14.0 | 29.0 |
| Good to very good | 87.1 | 88.8 | 85.9 | 71.0 |
| Currently on a weight loss diet (%) | ||||
| Yes | 5.4 | 5.7 | 4.3 | 6.6 |
| No | 94.4 | 94.0 | 95.6 | 93.4 |
| AHEI (0–110 Points) | MDS (0–9 Points) | |||
|---|---|---|---|---|
| Coefficient | 95% CI | Coefficient | 95% CI | |
| Sex | ||||
| Males | 0 | 0 | ||
| Females | 1.57 | [0.38; 2.76] | −0.12 | [−0.23; 0.00] |
| Age group d | ||||
| 18–29 years | −1.31 | [−3.07; 0.46] | −0.09 | [−0.26; 0.08] |
| 30–44 years | 0 | 0 | ||
| 45–59 years | 3.00 | [1.64; 4.35] | 0.22 | [0.08; 0.35] |
| 60–75 years | 4.81 | [3.13; 6.49] | 0.34 | [0.17; 0.50] |
| Language region e | ||||
| German-speaking | 0 | 0 | ||
| French-speaking | 2.03 | [0.82; 3.24] | 0.20 | [0.09; 0.32] |
| Italian-speaking | 1.99 | [−0.27; 4.24] | 0.31 | [0.09; 0.53] |
| BMI categories f | ||||
| Underweight | 2.01 | [−1.33; 5.35] | 0.36 | [0.03; 0.68] |
| Normal weight | 0 | 0 | ||
| Overweight | −2.56 | [−3.77; −1.35] | −0.27 | [−0.39; −0.15] |
| Obese | −4.60 | [−6.28; −2.92] | −0.33 | [−0.49; −0.17] |
| Nationality | ||||
| Swiss only | 0 | 0 | ||
| Swiss binational | 1.06 | [−0.47; 2.59] | 0.09 | [−0.06; 0.24] |
| Non-Swiss | 2.08 | [0.78; 3.37] | 0.22 | [0.09; 0.34] |
| Education, highest degree | ||||
| Primary/no degree | −1.23 | [−3.75; 1.28] | −0.08 | [−0.33; 0.16] |
| Secondary | 0 | 0 | ||
| Tertiary | 2.47 | [1.35; 3.59] | 0.16 | [0.05; 0.27] |
| Household type | ||||
| Living alone | 0.32 | [−1.34; 1.99] | 0.08 | [−0.08; 0.24] |
| Couple without children | 0 | 0 | ||
| Couple with children | −0.67 | [−2.04; 0.69] | 0.08 | [−0.05; 0.21] |
| One-parent family with children | −2.89 | [−5.57; −0.20] | −0.01 | [−0.27; 0.25] |
| Adult living with parents | −2.44 | [−4.83; −0.05] | −0.13 | [−0.36; 0.11] |
| Others | −3.11 | [−5.56; −0.65] | 0.09 | [−0.15; 0.33] |
| Gross household income | ||||
| <6000 (CHF/month) | −0.58 | [−2.26; 1.09] | −0.10 | [−0.25; 0.06] |
| 6000–13,000 (CHF/month) | 0 | 0 | ||
| >13,000 (CHF/month) | −0.26 | [−1.88; 1.36] | −0.03 | [−0.18; 0.13] |
| Self-reported physical activity | ||||
| Low | 0 | 0 | ||
| Moderate | 2.45 | [0.53; 4.37] | 0.27 | [0.09; 0.45] |
| High | 1.60 | [−0.09; 3.29] | 0.22 | [0.06; 0.38] |
| Smoking status | ||||
| Never | 0 | 0 | ||
| Former | −1.15 | [−2.33; 0.03] | 0.12 | [0.00; 0.23] |
| Current | −3.38 | [−4.72; −2.04] | −0.04 | [−0.17; 0.09] |
| Self-reported health | ||||
| Good to very good | 0 | 0 | ||
| Very bad to medium | −1.89 | [−3.49; −0.29] | −0.05 | [−0.20; 0.11] |
| Currently on a weight loss diet | ||||
| No | 0 | 0 | ||
| Yes | 4.64 | [2.35; 6.92] | 0.29 | [0.06; 0.51] |
| German-Speaking Region e | French-Speaking Region e | Italian-Speaking Region e | Overall | German vs. French | French vs. Italian | German vs. Italian | |
|---|---|---|---|---|---|---|---|
| T3 (%) | T3 (%) | T3 (%) | p-Value c | p-Value c,d | p-Value c,d | p-Value c,d | |
| Vegetables | 32.8 | 34.1 | 36.7 | 0.49 | 1 | 0.44 | 0.36 |
| Fruit | 33.1 | 31.6 | 32.3 | 0.72 | 1 | 1 | 1 |
| Whole grains | 23.8 | 19.7 | 16.3 | <0.01 | 0.50 | 0.03 | <0.01 |
| SSB/fruit juices f | 31.3 | 34.9 | 51.0 | <0.01 | 1 | 0.01 | <0.01 |
| Nuts and legumes | 34.1 | 31.4 | 32.5 | 0.07 | 0.56 | 0.71 | 0.05 |
| Red/processed meat f | 32.2 | 35.7 | 35.7 | 0.39 | 1 | 1 | 0.75 |
| Trans fat f | 83.2 | 91.8 | 95.0 | <0.01 | <0.01 | 0.97 | <0.01 |
| Fish | 4.9 | 6.6 | 9.7 | <0.01 | <0.01 | 1 | 0.01 |
| PUFA | 33.5 | 34.1 | 27.0 | 0.18 | 0.55 | 0.50 | 0.86 |
| Sodium f | 30.9 | 38.4 | 40.5 | 0.03 | 0.11 | 1 | 0.16 |
| Alcohol f | 34.7 | 27.0 | 42.8 | <0.01 | 0.02 | <0.01 | 0.08 |
| German-Speaking Region e | French-Speaking Region e | Italian-Speaking Region e | Overall | German vs. French | French vs. Italian | German vs. Italian | |
|---|---|---|---|---|---|---|---|
| 1 Point (%) | 1 Point (%) | 1 Point (%) | p-Value c | p-Value c,d | p-Value c,d | p-Value c,d | |
| Vegetables | 27.6 | 30.0 | 30.1 | 0.60 | 1 | 1 | 1 |
| Legumes | 1.1 | 0.5 | 1.5 | 0.76 | 1 | 1 | 1 |
| Fruits and nuts | 32.8 | 32.9 | 29.6 | 0.42 | 1 | 0.25 | 0.50 |
| Cereals | 32.4 | 28.8 | 24.6 | 0.31 | 1 | 1 | 0.44 |
| Fish | 5.1 | 6.6 | 9.7 | <0.01 | <0.01 | 1 | 0.01 |
| Meat f | 30.2 | 26.6 | 27.0 | 0.50 | 1 | 1 | 1 |
| Dairy products f | 30.0 | 43.0 | 40.4 | <0.01 | <0.01 | 1 | 0.03 |
| Alcohol f | 12.3 | 10.5 | 20.8 | 0.05 | 0.98 | 0.01 | 0.05 |
| Fat intake g | 28.0 | 31.4 | 44.2 | <0.01 | 1 | 0.01 | <0.01 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pestoni, G.; Krieger, J.-P.; Sych, J.M.; Faeh, D.; Rohrmann, S. Cultural Differences in Diet and Determinants of Diet Quality in Switzerland: Results from the National Nutrition Survey menuCH. Nutrients 2019, 11, 126. https://doi.org/10.3390/nu11010126
Pestoni G, Krieger J-P, Sych JM, Faeh D, Rohrmann S. Cultural Differences in Diet and Determinants of Diet Quality in Switzerland: Results from the National Nutrition Survey menuCH. Nutrients. 2019; 11(1):126. https://doi.org/10.3390/nu11010126
Chicago/Turabian StylePestoni, Giulia, Jean-Philippe Krieger, Janice Marie Sych, David Faeh, and Sabine Rohrmann. 2019. "Cultural Differences in Diet and Determinants of Diet Quality in Switzerland: Results from the National Nutrition Survey menuCH" Nutrients 11, no. 1: 126. https://doi.org/10.3390/nu11010126
APA StylePestoni, G., Krieger, J.-P., Sych, J. M., Faeh, D., & Rohrmann, S. (2019). Cultural Differences in Diet and Determinants of Diet Quality in Switzerland: Results from the National Nutrition Survey menuCH. Nutrients, 11(1), 126. https://doi.org/10.3390/nu11010126