The Possibility of Applying the Vitamin D Brief Food Frequency Questionnaire as a Tool for a Country with No Vitamin D Data in Food Composition Tables

 ,
, 
 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Adjusting the VIDEO-FFQ Questionnaire to the Croatian Population (Developing Cro-VIDEO-FFQ Questionnaire)
2.2. Validation of the Cro-VIDEO-FFQ Questionnaire
2.3. Statistical Analysis of Validation of the Cro-VIDEO-FFQ Questionnaire
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Cashman, K.D.; Dowling, K.G.; Škrabáková, Z.; Gonzalez-Gross, M.; Valtueña, J.; De Henauw, S.; Moreno, L.; Damsgaard, C.T.; Michaelsen, K.F.; Mølgaard, C.; et al. Vitamin D deficiency in Europe: Pandemic? Am. J. Clin. Nutr. 2016, 103, 1033–1044. [Google Scholar] [CrossRef] [PubMed]
- Jääskeläinen, T.; Itkonen, S.T.; Lundqvist, A.; Erkkola, M.; Koskela, T.; Lakkala, K.; Dowling, K.G.; Hull, G.L.; Kröger, H.; Karppinen, J.; et al. The positive impact of general vitamin D food fortification policy on vitamin D status in a representative adult Finnish population: Evidence from an 11-y follow-up based on standardized 25-hydroxyvitamin D data. J. Clin. Nutr. 2017, 105, 1512–1520. [Google Scholar] [CrossRef] [PubMed]
- EFSA (European Food Safety Authority). Scientific opinion on the tolerable upper intake level of vitamin D. EFSA J. 2012, 10, 2813. [Google Scholar]
- O’Neill, C.M.; Kazantzidis, A.; Ryan, M.J.; Barber, N.; Sempos, C.T.; Durazo-Arvizu, R.A.; Jorde, R.; Grimnes, G.; Eiriksdottir, G.; Gudnason, V.; et al. Seasonal Changes in Vitamin D-Effective UVB Availability in Europe and Associations with Population Serum 25-Hydroxyvitamin D. Nutrients 2016, 8, 533. [Google Scholar] [CrossRef] [PubMed]
- Van Schoor, N.M.; Lips, P. Worldwide vitamin D status. Best Pract. Res. Clin. Endocrinol. Metab. 2011, 25, 671–680. [Google Scholar] [CrossRef] [PubMed]
- Spiro, A.; Buttriss, J.L. Vitamin D: An overview of vitamin D status and intake in Europe. Nutr. Bull. 2014, 39, 322–350. [Google Scholar] [CrossRef] [PubMed]
- Helldán, A.; Raulio, S.; Kosola, M.; Tapanainen, H.; Ovaskainen, M.L.; Virtanen, S. Finravinto 2012—Tutkimus. The National FINDIET 2012 Survey. Report 16/2013, 187 s. Helsinki 2013. Available online: https://www.julkari.fi/bitstream/handle/10024/110839/THL_RAP2013_016_%26sliitteet.pdf (accessed on 26 August 2018). (In Finnish).
- Livsmedels-och Näringsintag Bland Vuxna i Sverige. Report. Available online: https://www.livsmedelsverket.se/globalassets/publikationsdatabas/rapporter/2011/riksmaten_2010_20111.pdf (accessed on 26 August 2018). (In Swedish).
- Consumption of Fishery and Aquaculture Products. 2011. Available online: https://ec.europa.eu/fisheries/ 6-consumption_en (accessed on 8 August 2018).
- Colić Barić, I.; Keser, I.; Bituh, M.; Rumbak, I.; Rumora Samarin, I.; Beljan, K.; Gežin, L.; Lazinica, G. Vitamin D Status and Prevalence of Inadequacy in Croatian Population; Book of Abstracts of 4th International Congress of Nutritionists: Zadar, Hrvatska, 2016; p. 97. [Google Scholar]
- Laktasic-Zerjavic, N.; Korsic, M.; Crncevic-Orlic, Z.; Kovac, Z.; Polasek, O.; Soldo-Juresa, D. Vitamin D status, dependence on age, and seasonal variations in the concentration of vitamin D in Croatian postmenopausal women initially screened for osteoporosis. Clin. Rheumatol. 2010, 29, 861–867. [Google Scholar] [CrossRef]
- Kaić-Rak, A.; Antonic, K. (Eds.) Food and Drink Composition Database; Zavod za zaštitu zdravlja SR Hrvatske: Zagreb, Croatia, 1990. (In Croatian) [Google Scholar]
- FAO/ WHO, Food and Agriculture Organization of the United Nations/ World Health Organization. Preparation and Use of Food-Based Dietary Guidelines, Report of a Joint FAO/WHO Consultation Nicosia, Cyprus; WHO: Geneva, Switzerland, 1996. [Google Scholar]
- Hacker-Thompson, A.; Schloetter, M.; Sellmeyer, D.E. Validation of a dietary vitamin D questionnaire using multiple diet records and the block 98 health habits and history questionnaire in healthy postmenopausal women in northern California. J. Acad. Nutr. Diet. 2012, 112, 419–423. [Google Scholar] [CrossRef]
- Pritchard, J.M.; Seechurn, T.; Atkinson, S.A. A food frequency questionnaire for the assessment of calcium, vitamin D and vitamin K: A pilot validation study. Nutrients 2010, 2, 805–819. [Google Scholar] [CrossRef]
- Sadat-Ali, M.; Al Elq, A.H.; Al-Turki, H.A.; Al-Mulhim, F.A.; Al-Ali, A.K. Influence of vitamin D levels on bone mineral density and osteoporosis. Ann. Saudi Med. 2011, 31, 602–608. [Google Scholar] [CrossRef]
- Zareef, T.A.; Jackson, R.T.; Alkahtani, A.A. Vitamin D Intake among Premenopausal Women Living in Jeddah: Food Sources and Relationship to Demographic Factors and Bone Health. J. Nutr. Metab. 2018, 19, 8570986. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.; Kim, S.; Lim, Y.; Ha, Y.; Chang, J.; Kim, J.; Min, Y.; Chung, H. Validation of new food frequency questionnaire for assesment of calcium and vitamin D intake in Korean women. J. Bone Metab. 2013, 20, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Djekic-Ivankovic, M.; Weiler, H.A.; Nikolic, M.; Kadvan, A.; Gurinovic, M.; Mandic, L.M.; Glibetic, M. Validity of an FFQ assessing the vitamin D intake of young Serbian women living in a region without food fortification: The method of triads model. Public Health Nutr. 2016, 19, 437–445. [Google Scholar] [CrossRef] [PubMed]
- Głąbska, D.; Guzek, D.; Sidor, P.; Włodarek, D. Vitamin D Dietary intake questionnaire validation conducted among young Polish women. Nutrients 2016, 8, 36. [Google Scholar] [CrossRef] [PubMed]
- Itkonen, S.T.; Erkkola, M.; Skaffari, E.; Saaristo, P.; Saarnio, E.M.; Viljakainen, H.T.; Kärkkäinen, M.U.; Lamberg-Allardt, C.J. Development and validation of an interview-administered FFQ for assessment of vitamin D and calcium intakes in Finnish women. Br. J. Nutr. 2016, 28, 115–1100. [Google Scholar] [CrossRef] [PubMed]
- Bärebring, L.; Amberntsson, A.; Winkvist, A.; Augustin, H. Validation of Dietary Vitamin D Intake from Two Food Frequency Questionnaires, Using Food Records and the Biomarker 25-Hydroxyvitamin D among Pregnant Women. Nutrients 2018, 10, 745. [Google Scholar] [CrossRef] [PubMed]
- Mulligan, A.A.; Luben, R.N.; Bhaniani, A.; Parry-Smith, D.J.; O’Connor, L.; Khawaja, A.P.; Forouhi, N.G.; Khaw, K.-T. A new tool for converting food frequency questionnaire data into nutrient and food group values: FETA research methods and availability. BMJ Open 2014, e004503. [Google Scholar] [CrossRef] [PubMed]
- Kiely, M.; Collins, A.; Lucey, A.J.; Andersen, R.; Cashman, K.D.; Hennessy, Á. Development, validation and implementation of a quantitative food frequency questionnaire to assess habitual vitamin D intake. J. Hum. Nutr. Diet. 2016, 29, 495–504. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute/National Institutes of Health. Register of Validated Short Dietary Assessment Instruments. Available online: https://epi.grants.cancer.gov/diet/shortreg/ (accessed on 26 August 2018).
- Kunachowicz, H.; Nadolna, J.; Przygoda, B.; Iwanow, K. (Eds.) Food Composition Tables; PZWL: Warsaw, Poland, 2005. (In Polish) [Google Scholar]
- USDA National Nutrient Database for Standard Reference Legacy Release, April 2018. Available online: https://ndb.nal.usda.gov/ndb/search/list (accessed on 8 August 2018).
- Rossato, S.L.; Olinto, M.T.; Henn, R.L.; Moreira, L.B.; Camey, S.A.; Anjos, L.A.; Wahrlich, V.; Waissmann, W.; Fuchs, F.D.; Fuchs, S.C. Seasonal variation in food intake and the interaction effects of sex and age among adults in southern Brazil. Eur. J. Clin. Nutr. 2015, 69, 1015–1022. [Google Scholar] [CrossRef] [PubMed]
- Sidor, P.; Głąbska, D.; Włodarek, D. Analysis of the dietary factors contributing to the future osteoporosis risk in young Polish women. Rocz. Panstw. Zakl. Hig. 2016, 67, 279–285. [Google Scholar] [PubMed]
- Cade, J.; Thompson, R.; Burley, V.; Warm, D. Development, validation and utilisation of food-frequency questionnaires—A review. Public Health Nutr. 2002, 5, 567–587. [Google Scholar] [CrossRef] [PubMed]
- Willett, W.; Lenart, E. Reproducibility and validity of food frequency questionnaires. In Nutritional Epidemilogy, 3rd ed.; Willett, W., Ed.; Oxford University Press: Oxford, UK, 1985. [Google Scholar]
- Głąbska, D.; Książek, A.; Guzek, D. Development and Validation of the Brief Folate-Specific Food Frequency Questionnaire for Young Women’s Diet Assessment. Int. J. Environ. Res. Public Health 2017, 14, 1574. [Google Scholar] [CrossRef] [PubMed]
- Głąbska, D.; Malowaniec, E.; Guzek, D. Validity and Reproducibility of the Iodine Dietary Intake Questionnaire Assessment Conducted for Young Polish Women. Int. J. Environ. Res. Public Health 2017, 29, 700. [Google Scholar] [CrossRef] [PubMed]
- Barrett, J.S.; Gibson, P.R. Development and validation of a comprehensive semi-quantitative food frequency questionnaire that includes FODMAP intake and glycemic index. J. Am. Diet. Assoc. 2010, 110, 1469–1476. [Google Scholar] [CrossRef] [PubMed]
- Myles, P.S.; Cui, J. Using the Bland-Altman method to measure agreement with repeated measures. Br. J. Anaesth. 2007, 99, 309–311. [Google Scholar] [CrossRef] [PubMed]
- Tabacchi, G.; Filippi, A.R.; Breda, J.; Censi, L.; Amodio, E.; Napoli, G.; Bianco, A.; Jemni, M.; Firenze, A.; Mammina, C. Comparative validity of the ASSO–Food Frequency Questionnaire for the web-based assessment of food and nutrients intake in adolescents. Food Nutr. Res. 2015, 59, 26216. [Google Scholar] [CrossRef] [PubMed]
- Giavarina, D. Understanding Bland Altman analysis. Biochem. Med. 2015, 25, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Masson, L.F.; McNeill, G.; Tomany, J.O.; Simpson, J.A.; Peace, H.S.; Wei, L.; Bolton-Smith, C. Statistical approaches for assessing the relative validity of a food-frequency questionnaire, use of correlation coefficients and the kappa statistic. Public Health Nutr. 2003, 6, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine; Committee to Review Dietary Reference Intakes for Vitamin D and Calcium, Food and Nutrition Board. Dietary Reference Intakes for Calcium and Vitamin D; National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Shrout, P.E.; Fleiss, J.L. Intraclass Correlations: Uses in Assessing Rater Reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef] [PubMed]
- Cicchetti, D.V. Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychol. Assess. 1994, 6, 284–290. [Google Scholar] [CrossRef]
- Verbeke, W.; Vackier, I. Individual determinants of fish consumption: Application of the theory of planned behaviour. Appetite 2005, 44, 67–82. [Google Scholar] [CrossRef] [PubMed]
- You, C.-H.; Kim, B.-G.; Kim, Y.-M.; Lee, S.-A.; Kim, R.-B.; Seo, J.-W.; Hong, Y.-S. Relationship between Dietary Mercury Intake and Blood Mercury Level in Korea. J. Korean Med. Sci. 2014, 29, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Tollosa, D.N.; Van Camp, J.; Huybrechts, I.; Huybregts, L.; Van Loco, J.; De Smet, S.; Sterck, E.; Rabâi, C.; Van Hecke, T.; Vanhaecke, L. Validity and Reproducibility of a Food Frequency Questionnaire for Dietary Factors Related to Colorectal Cancer. Nutrients 2017, 9, 1257. [Google Scholar] [CrossRef] [PubMed]
- Sahashi, Y.; Tsuji, M.; Wada, K.; Tamai, Y.; Nakamura, K.; Nagata, C. Validity and reproducibility of food frequency questionnaire in Japanese children aged 6 years. J. Nutr. Sci. Vitaminol. (Tokyo). 2011, 57, 372–376. [Google Scholar] [CrossRef] [PubMed]
- Serra-Majem, L.; Pfrimer, K.; Doreste-Alonso, J.; Ribas-Barba, L.; Sánchez-Villegas, A.; Ortiz-Andrellucchi, A.; Henríquez-Sánchez, P. Dietary assessment methods for intakes of iron, calcium, selenium, zinc and iodine. Br. J. Nutr. 2009, 102, 38–55. [Google Scholar] [CrossRef] [PubMed]
- Williams, P.L.; Innis, S.M. Food frequency questionnaire for assessing infant iron nutrition. Can. J. Diet. Pract. Res. 2005, 66, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Heath, A.L.; Skeaff, C.M.; Gibson, R.S. The relative validity of a computerized food frequency questionnaire for estimating intake of dietary iron and its absorption modifiers. Eur. J. Clin. Nutr. 2000, 54, 592–599. [Google Scholar] [CrossRef] [PubMed]
- MRI. National Verzehrs Studie II, Ergebnisbericht, Teil 2. In Die bundesweite Befragung zur Ernährung von Jugendlichen und Erwachsenen; Max Rubner-Institut Bundesforschungsinstitut für Ernährung und Lebensmittel: Karlsruhe, Germany, 2008; p. 307. [Google Scholar]
- Elmadfa, I.; Freisling, H.; Nowak, V.; Hofstä, *!!! REPLACE !!!*; dter, D.; Hasenegger, V.; Ferge, M.; Fröhler, M.; Fritz, K.; Meyer, A.L.; Putz, P.; et al. Österreichischer Ernährungsbericht 2008 (Austrian Nutrition Report 2008); Institut für Ernährungswissenschaften der Universität Wien, Bundesministerium für Gesundheit: Wien, Austria, 2009; p. 454. [Google Scholar]
- Walton, J. (Ed.) National Adult Nutrition Survey; IUNA (Irish Universities Nutrition Alliance): Cork, Ireland, 2011. [Google Scholar]
- Van Rossum, C.T.M.; Fransen, H.P.; Verkaik-Kloosterman, J.; Buurma-Rethans, E.J.M.; Ocké, M.C. Dutch National Food Consumption Survey 2007–2010: Diet of Children and Adults Aged 7 to 69 Years; National Institute for Public Health and the Environment: The Netherlands, 2011; p. 148. [Google Scholar]
- Pedersen, A.N.; Fagt, S.; Groth, M.V.; Christensen, T.; Biltoft-Jensen, A.; Matthiessen, J.; Lyhne Andersen, N.; Kørup, K.; Hartkopp, H.; Hess Ygil, K.; et al. Danskernes, Kostvaner 2003–2008: Hovedresultater (Dietary Habits in Denmark 2003–2008. Main Results); DTU Fødevareinstituttet: Søborg, Denmark; 2010; p. 200. [Google Scholar]
- Jungert, A.; Spinneker, A.; Nagel, A.; Neuhäuser-Berthold, M. Dietary intake and main food sources of vitamin D as a function of age, sex, vitamin D status, body composition, and income in an elderly German cohort. Food Nutr. Res. 2014, 58, 23632. [Google Scholar] [CrossRef] [PubMed]
- Hill, K.M.; Jonnalagadda, S.S.; Albertson, A.M.; Joshi, N.A.; Weaver, C.M. Top food sources contributing to vitamin D intake and the association of ready-to-eat cereal and breakfast consumption habits to vitamin D intake in Canadians and United States Americans. J. Food Sci. 2012, 77, 170–175. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, K.; Nashimoto, M.; Hori, Y.; Yamamoto, M. Serum 25-hydroxyvitamin D concentrations and related dietary factors in peri- and postmenopausal Japanese women. Am. J. Clin. Nutr. 2000, 71, 1161–1165. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| The Food Items Included into Cro-VIDEO-FFQ Questionnaire | The Vitamin D Content Per 1 Serving (µg) | ||||
|---|---|---|---|---|---|
| Group of Products | Products | Serving Size | Frequency | ||
| Fresh and smoked fish | Salmon, rainbow trout, herring, eel | 50 g (deck of cards) | Monthly | Salmon | 7.50 |
| Rainbow trout | 7.80 | ||||
| Herring | 9.50 | ||||
| Eel | 15.00 | ||||
| Halibut, mackerel, brook trout, sole, tuna | 50 g (deck of cards) | Monthly | Halibut | 2.50 | |
| Mackerel | 2.50 | ||||
| Brook trout | 1.05 | ||||
| Sole | 4.00 | ||||
| Tuna | 3.60 | ||||
| Cod, flounder, plaice, pollock, hake, bass, zander, pike | 50 g (deck of cards) | Monthly | Cod | 0.50 | |
| Flounder | 0.40 | ||||
| Plaice | 0.40 | ||||
| Pollock | 0.50 | ||||
| Hake | 0.50 | ||||
| Bass | 0.40 | ||||
| Zander | 0.35 | ||||
| Pike | 0.45 | ||||
| Other fish (to be specified) | 50 g (deck of cards) | Monthly | Depending on the product | ||
| Fish products | Herrings, sardines, and tuna products | 100 g (e.g., 2 rollmops, small can of tuna, 2/3 of can of herrings) | Monthly | 12.36 | |
| Other fish products | 100 g (e.g., 1/3 of can of fish stew) | 0.93 | |||
| Dairy products | Milk and milk beverages (yoghurt, kefir, buttermilk, cream) | 250 g (1 glass) | Weekly | 0.28 | |
| Vitamin D fortified products (to be specified) | 250 g (1 glass) | Depending on the product | |||
| Rennet, blue and soft penicillium cheese | 20 g (1 slice) | 0.09 | |||
| Feta cheese | 15 g (1 slice) | 0.08 | |||
| Cottage cheese | 50 g (1 thick slice, 2 tablespoons) | 0.08 | |||
| Processed cheese | 25 g (1 slice, 1 spoon, 1 triangle serving) | 0.07 | |||
| Homogenized cheese | 150 g (1 package) | 0.23 | |||
| Dairy ice cream | 40 g (1 scoop) | Monthly | 0.30 | ||
| Eggs | Egg | 50 g (1 medium egg) | Weekly | 0.85 | |
| Egg yolk | 20 g (1 yolk) | 0.90 | |||
| Meat and meat products | Meat | 100 g (palm of small hand) | Weekly | 0.75 | |
| Meat products | 15 g (thin slice of ham, 3 slices of sausage) | 0.09 | |||
| Cereals | White wheat and confectionery bread | 35 g (1 slice, small roll) | Weekly | 0.06 | |
| Cooked egg pasta | 100 g of cooked (1 glass) | 0.25 | |||
| Fats | Butter, butter products, pork fat | 5 g (1 teaspoon) | Daily | 0.03 | |
| Fortified margarine | 5 g (1 teaspoon) | 0.31 | |||
| 3-Day Dietary Record | Cro-VIDEO-FFQ1 * | Cro-VIDEO-FFQ2 * | ||
|---|---|---|---|---|
| Mean ± standard deviation (µg) | 2.4 ± 1.7 | 3.5 ± 1.8 | 3.8 ± 1.5 | |
| Median (µg) | 1.9 ** | 3.3 ** | 3.6 ** | |
| Minimum (µg) | 0.2 | 1.1 | 1.4 | |
| Maximum ([µg) | 8.0 | 10.6 | 7.8 | |
| Individuals characterized by adequate intake in comparison with EAR level [40] | N | 1 | 0 | 0 |
| [%] | 1.6 | 0 | 0 | |
| Individuals characterized by inadequate intake in comparison with EAR level [40] | N | 62 | 63 | 63 |
| [%] | 98.4 | 100 | 100 | |
| Group of Products | Share of Vitamin D Intake (%) | Vitamin D Intake (µg) | ||||
|---|---|---|---|---|---|---|
| Mean ± Standard Deviation | Median | Minimum–Maximum | Mean ± Standard Deviation | Median | Minimum–Maximum | |
| Fish and fish products | 43.2 ± 26.0 | 43.8 * | 0–96.6 | 1.8 ± 1.9 | 1.4 * | 0–9.9 |
| Meat and meat products | 20.4 ± 13.4 | 17.2 * | 0–59.6 | 0.6 ± 0.3 | 0.6 * | 0–1.3 |
| Eggs | 14.3 ± 12.1 | 10.7 * | 0–68.8 | 0.5 ± 0.8 | 0.4 * | 0–6.6 |
| Dairy products | 10.8 ± 7.2 | 10.0 * | 0–37.2 | 0.3 ± 0.2 | 0.3 * | 0–0.9 |
| Cereal products | 4.2 ± 5.0 | 3.2 * | 0–39.3 | 0.1 ± 0.3 | 0.1 * | 0–2.3 |
| Fats | 7.1 ± 9.8 | 2.4 * | 0–38.8 | 0.2 ± 0.4 | 0.1 * | 0–1.9 |
| The Assessed Parameters | Analysis of Validity—Cro-VIDEO-FFQ1 vs. 3-Day Dietary Record | Analysis of Reproducibility—Cro-VIDEO-FFQ1 vs. Cro-VIDEO-FFQ2 | |
|---|---|---|---|
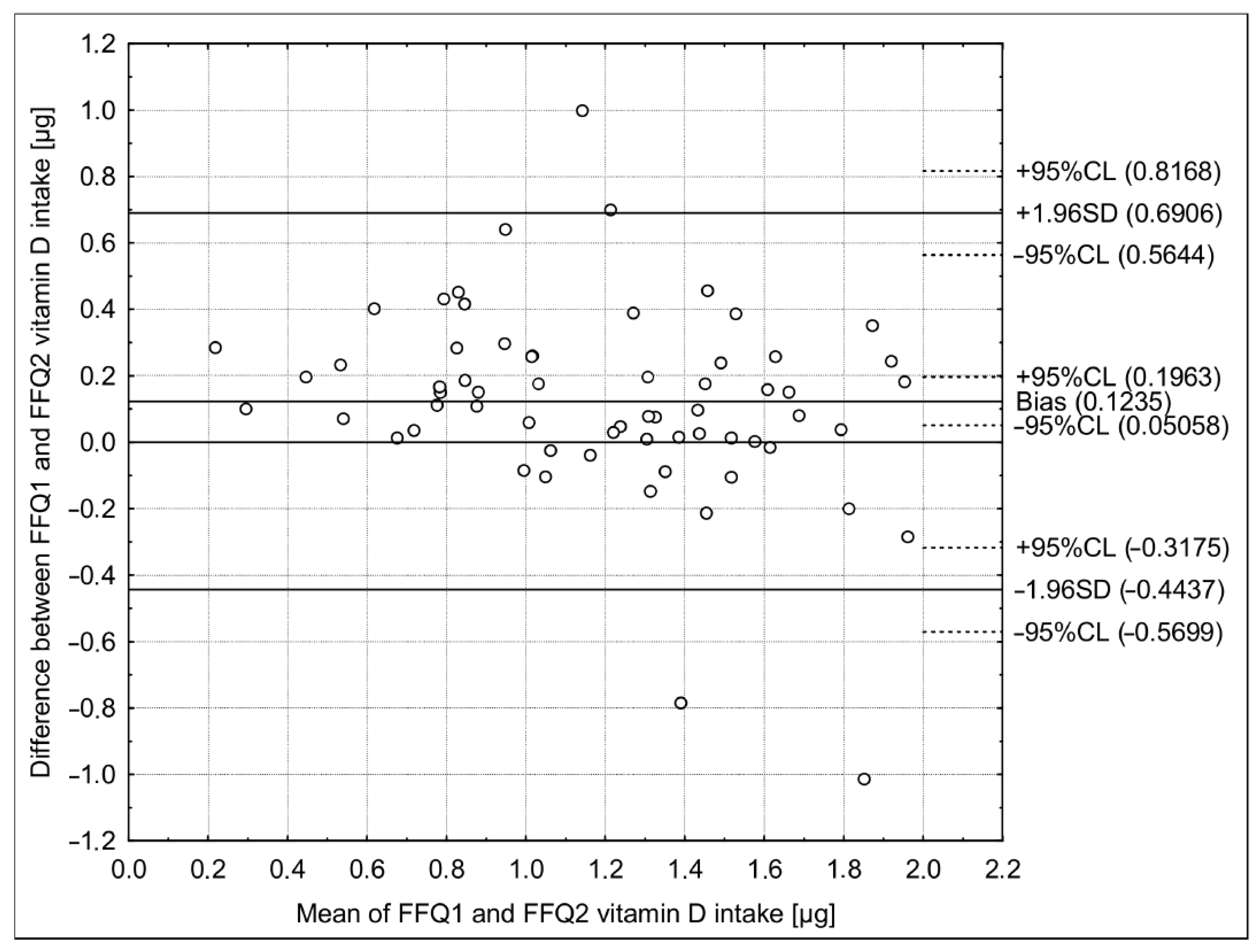
| Bland-Altman plot analysis | Mean difference | 0.55 | 0.12 |
| Limit of agreement (LoA) | −0.91–2.01 | −0.44–0.69 | |
| Analysis of quartiles | Individuals correctly classified | 20 (32%) | 47 (75%) |
| Individuals grossly misclassified | 4 (6%) | 1 (2%) | |
| Weighted κ statistic | 0.21 | 0.62 | |
| Analysis of adequacy in comparison with EAR level [40] | Individuals correctly classified | 62 (98.4%) | 63 (100%) |
| Individuals misclassified | 1 (1.6%) | 0 (0%) | |
| Analysis of correlation | p-Value | 0.0027 | <0.0001 |
| r Spearman correlation coefficient | 0.37 | 0.80 | |
| Intraclass correlation coefficient (ICC) | ICC | 0.56 | 0.81 |
| 95% confidence interval (CI) | 0.27–0.73 | 0.69–0.89 | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Głąbska, D.; Uroić, V.; Guzek, D.; Pavić, E.; Bival, S.; Jaworska, K.; Giljević, Z.; Lange, E. The Possibility of Applying the Vitamin D Brief Food Frequency Questionnaire as a Tool for a Country with No Vitamin D Data in Food Composition Tables. Nutrients 2018, 10, 1278. https://doi.org/10.3390/nu10091278
Głąbska D, Uroić V, Guzek D, Pavić E, Bival S, Jaworska K, Giljević Z, Lange E. The Possibility of Applying the Vitamin D Brief Food Frequency Questionnaire as a Tool for a Country with No Vitamin D Data in Food Composition Tables. Nutrients. 2018; 10(9):1278. https://doi.org/10.3390/nu10091278
Chicago/Turabian StyleGłąbska, Dominika, Valentina Uroić, Dominika Guzek, Eva Pavić, Sandra Bival, Kamila Jaworska, Zlatko Giljević, and Ewa Lange. 2018. "The Possibility of Applying the Vitamin D Brief Food Frequency Questionnaire as a Tool for a Country with No Vitamin D Data in Food Composition Tables" Nutrients 10, no. 9: 1278. https://doi.org/10.3390/nu10091278
APA StyleGłąbska, D., Uroić, V., Guzek, D., Pavić, E., Bival, S., Jaworska, K., Giljević, Z., & Lange, E. (2018). The Possibility of Applying the Vitamin D Brief Food Frequency Questionnaire as a Tool for a Country with No Vitamin D Data in Food Composition Tables. Nutrients, 10(9), 1278. https://doi.org/10.3390/nu10091278