1. Introduction
Human milk usually provides all the nutrients a human infant requires for the first 6 months of life. As well as the essential macro and micro-nutrients, breast milk contains many distinctive bioactive molecules that protect the new-born against pathogens and inflammation, and contribute to immune system maturation, organ development, and healthy microbial colonization [
1,
2]. The benefits of breastfeeding on the health and wellbeing of the infant are well recognized and include the prevention of infections, optimal neurodevelopment, and may limit the development of allergy, obesity and diabetes later in life [
3,
4,
5]. The World Health Organization (WHO) [
6] and the national advisory bodies of many countries, including New Zealand (NZ) [
7], actively support and promote breastfeeding by their strong recommendations that all infants should be exclusively breastfed for the first 6 months of life and that breastfeeding be continued with appropriate complementary foods for 2 years and beyond postpartum. For infants who are not breastfed, human milk composition is used as an important reference in decisions on the adequacy of surrogate infant nutrition products.
Human milk composition varies considerably within and between mothers and even within a single milk expression. This multidimensional variation in composition is believed to be an adaptation to the infants’ changing needs [
8,
9,
10], and geographical region and food supply [
11,
12]. The variations in human milk composition between individual women and populations have been reported to be in response to cultural differences such as diet and other lifestyle factors [
13,
14], environmental factors, such as mineral content of the soil that is then reflected in the mineral density of the foods grown there [
15], and human genetic differences [
16]. However, human milk composition data has not been collected from all world regions and populations. Therefore, studies of human milk composition in other regions and populations are important, particularly with regard to micronutrient concentrations and the proportions of specific lipids where a large variability has been noted from existing studies [
14,
17,
18,
19].
There is limited information available on the nutrient composition of breast milk from NZ mothers. Early research on breast milk from NZ women, by Deem [
20,
21], investigated diurnal variation in fat content and the influence of dietary macronutrient content on breast milk composition. Recent published information on breast milk composition in NZ women has focused on the levels of environmental contaminants in breast milk [
22], the micronutrient iodine [
23,
24,
25,
26] and the macronutrient and amino acid compositions [
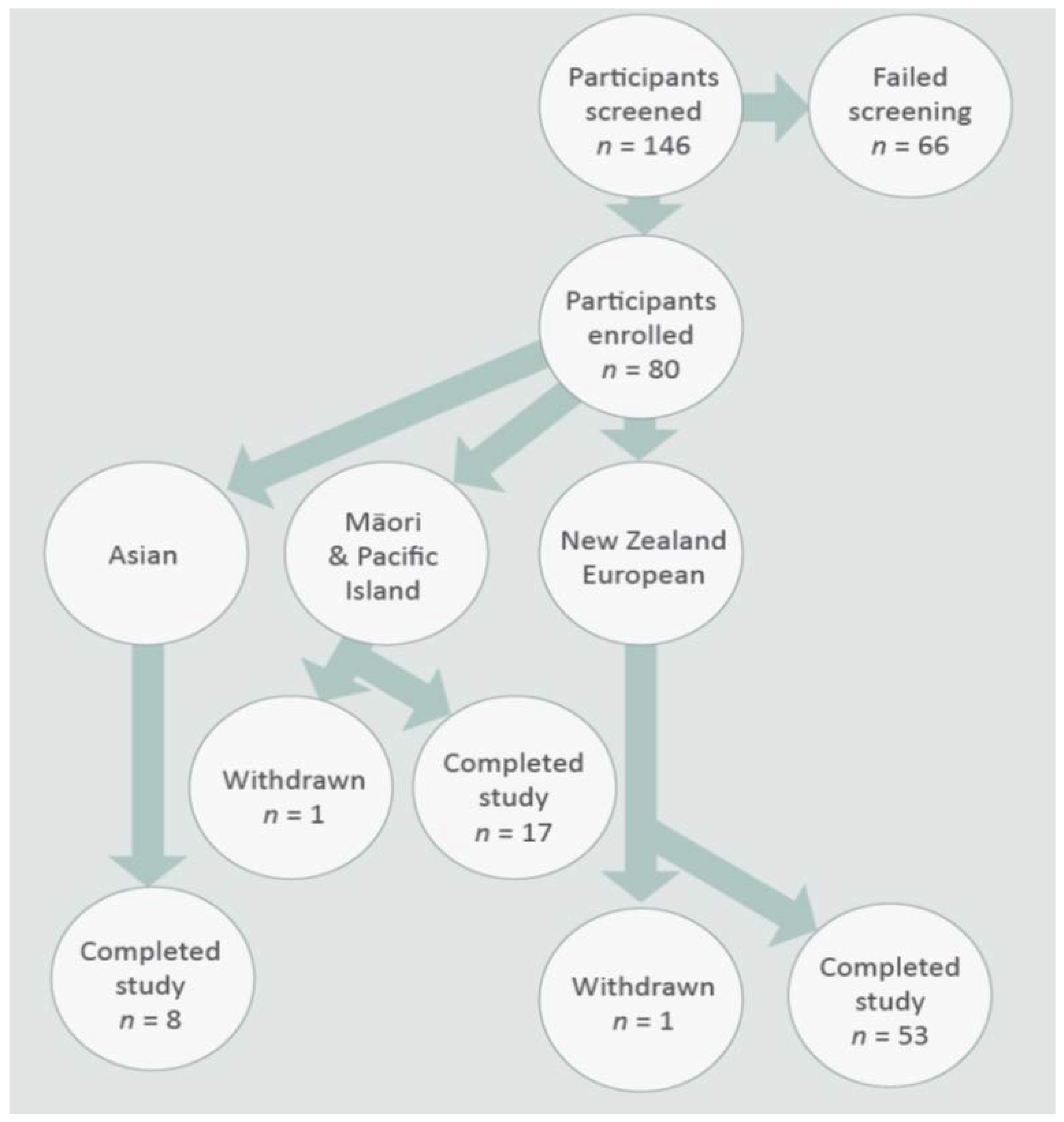
27]. In the present study, we investigated the composition of breast milk of an ethnically mixed population of NZ women as a first representation of the New Zealand national population. The main ethnic groups in NZ are the indigenous Māori (14.9%) and three major immigrant populations from the Pacific Islands (7.4%), Asia (11.8%) and Europe (74.0%) [
28]. We note here that some NZ citizens identify with more than one ethnic group resulting in the total being greater than 100%. The secondary aims of this study were to determine the dietary nutrient intakes of breastfeeding women, compare these to recommended intakes, to assess if the diets were different between different ethnic groups, and if this had any impact on breastmilk composition.
4. Discussion
This study is the first to measure and compare breast milk composition and nutrient intakes from an ethnically representative proportion of NZ mothers. We found that the breast milk nutrient profiles of women from different ethnicities were similar in their macronutrient composition, but there were differences in the concentrations of some fatty acids and magnesium. Dietary intakes were different for protein, total energy, saturated and polyunsaturated fat, calcium, phosphorus, zinc, iodine, vitamin A equivalents, and folate. The serves of dairy products, chicken and legumes consumed by the mothers were different between the ethnic groups. There were weak positive associations with breast milk concentrations of some fatty acids and magnesium with dietary fatty acid and magnesium intakes.
Our study population was representative of the main ethnic groups present in NZ. Recent census figures [
28], reported that 74.0% of the NZ population identifies themselves as Europeans, 11.8% as Asian and 22.3% as Māori and Pacific Island. This is very similar to the proportions in our study population: 68% NZ European, 10% Asian, and 22% Māori and Pacific Island. Other demographic characteristics of the participants were also similar across the different ethnicities. Categorization of the participants’ BMI was also representative of the NZ population with 40% classified as overweight and 30% as obese—reflecting the results reported by the NZ Ministry of Health [
33] of 35% overweight and 30% obese. While the Māori and Pacific Island participants had significantly higher body weights and BMI in the present study, the actual values were lower or similar to those reported (BMI 28.7 vs. 32.8) in a recent national health survey [
33]; as were the BMI’s for Asian (BMI 22.5 vs. 24.4) and NZ European (BMI 27.2 vs. 27.9) participants. Weight gain during pregnancy is normal due to the growth of the fetus, placenta, and amniotic fluid [
34], and postpartum weight loss may be influenced by infant nursing mode [
35]. In normal weight mothers, the gestational weight gain has been found to be approximately 13 kg [
36], and weight loss has been reported to be variable with between 8 and 9 kg at 1 month postpartum and 4 and 11 kg at 3 months postpartum [
35,
37]. Gestational weight gain is associated with ethnicity, socio-demographic, lifestyle, and pregnancy characteristics within populations but which of these factors is predominant is unknown [
38]. We weighed the mothers in the present study at six weeks postpartum when postpartum weight loss may not be completed.
The macronutrient composition of human milk is known to vary within mothers and during lactation, and yet it is conserved across populations despite variations in maternal nutritional status [
39,
40]. We found no statistically significant differences in the macronutrient concentrations in the breast milk of NZ women of different ethnicity. Breast milk samples collected in this study had similar protein (1.2%), carbohydrate (7.5%), and fat (3.8%) concentrations to those reported in the literature for mature hind milk [
6,
8,
40,
41,
42]. Lipids can be the most variable macronutrient of human breast milk. For example, hind milk, defined as the last milk of a feed, may contain higher concentrations (4.79–6.07 g/100 mL) of milk fat than that found in foremilk (1.14–2.63 g/100 mL), defined as the initial milk of a feed [
43]. Milk fat content has also been reported to be significantly lower in night (37.2 g/L; 10:01 pm to 4:00 am) and morning (37.1 g/L; 4:01 am to 10:00 am) feed samples than those from day (42.8 g/L; 10:01 am to 4:00 pm) and evening (43.2 g/L; 4:01 to 10:00 pm) feeds [
21,
44]. Total fat, dry matter, and energy contents of human milk are also known to increase markedly during the feed (water content decreases accordingly) as the breast is emptied [
45]. The breast milk samples in the present study were collected from the first feed of the day (first feed after sunrise) and after the baby was fed and were, therefore, samples of hind milk. The mean fat content of 3.79% found in the present study is within the ranges for hind milk and milk collected in the morning when milk fat content is lower [
44].
Calcium, phosphorous and magnesium concentrations in maternal serum are tightly regulated and it has been reported that there is little effect of maternal dietary intake of these minerals on their concentrations in human milk [
46,
47]. The mean concentrations of calcium and magnesium in mature milk reported in the literature are approximately 280 mg/L and 35 mg/L, respectively [
46,
48,
49]. The observed concentrations of calcium and magnesium in breast milk reported here are in agreement with these values. However, we found that the mean magnesium concentration of breast milk from NZ European mothers was significantly higher than for the Asian and Māori and Pacific Island mothers, though there was not a statistically significant difference in dietary magnesium intake between ethnicities. We did observe a weak positive association with breast milk magnesium content and dietary intake which is in contrast to the literature [
46,
47] and may warrant further investigation.
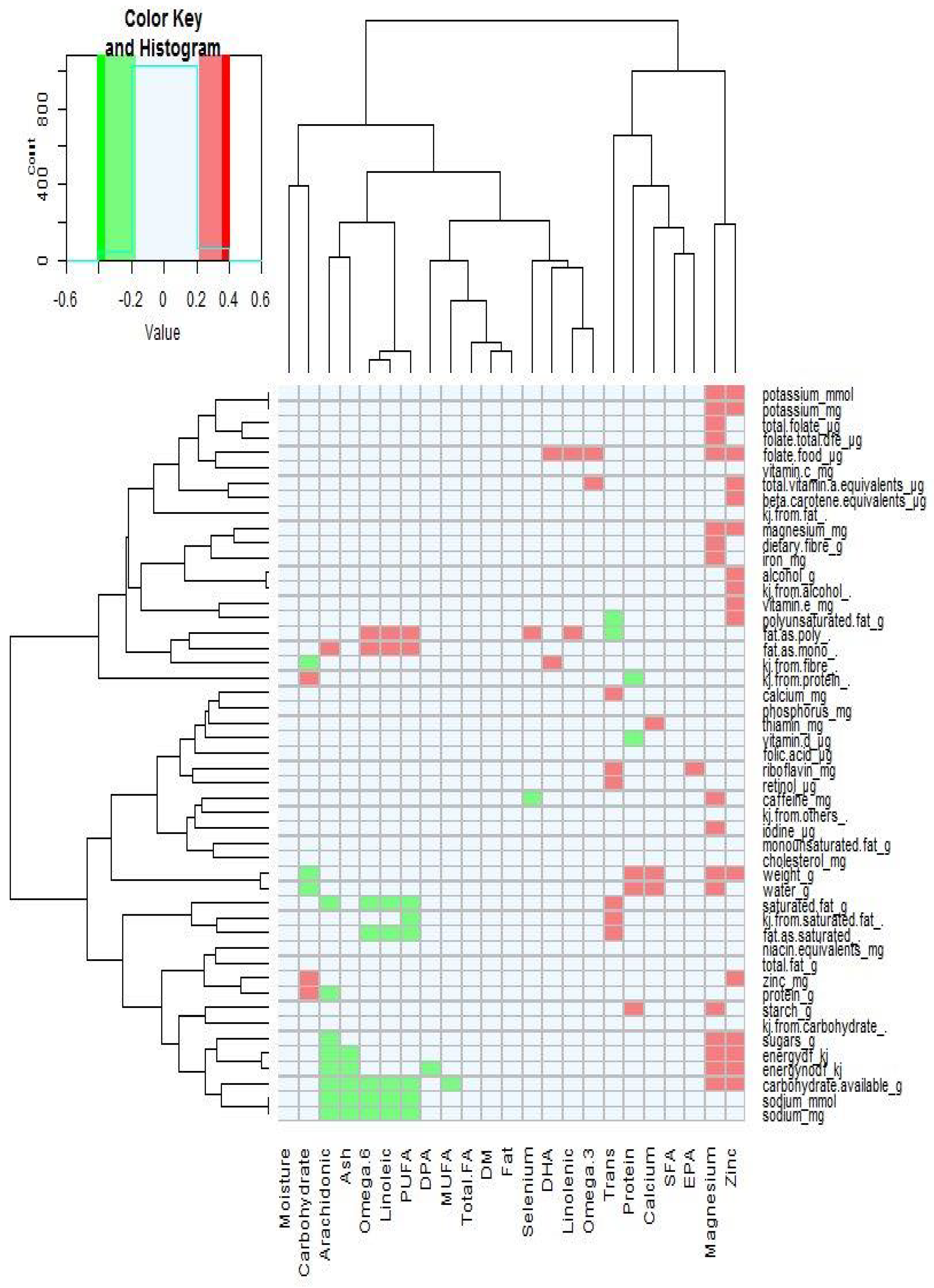
The mean concentrations of zinc and selenium in the breast milk collected in the present study were 2.21 mg/kg and 0.014 mg/kg, respectively, and there were no significant differences between mothers of different ethnicity. Zinc concentrations in human milk decrease over lactation and steeply decline over the first month of lactation from that found in colostrum (>10 mg/L) and then gradually to 0.5 mg/L by the twelfth month of lactation (Casey 1989). The dietary intake of zinc has mostly been reported in the literature as having little impact on the concentrations found in breast milk [
14,
48,
50]. Two studies, however, reported that zinc supplementation may influence zinc concentration in late lactation [
51,
52], which is in agreement for the positive association found here (
Figure 2). The selenium concentrations in mature breast milk have been reported to be between 10–30 µg/L [
53], with higher concentrations found at the initiation of lactation (41 µg/L) and decreasing as lactation progresses [
54]. Worldwide, there are major differences in the selenium content of soils and therefore in the food supply [
15], and NZ has one of the lowest estimated adult selenium intakes and blood serum concentrations in the world [
55]. Rural African women’s selenium breast milk concentrations were low when their dietary selenium intakes were low [
56]. In contrast, Debski et al. [
57] reported that the selenium breast milk concentrations of lacto-ovo-vegetarian women (22.2 ng/mL) were greater than that of non-vegetarian women (16.8 ng/mL), but there was no significant differences in selenium intake between the two groups. We found no significant differences in breast milk selenium concentrations between the mothers of different ethnicity in the present study. No selenium dietary intake data are reported here as this data was not available for dietary analysis.
The composition of human milk has been observed to be consistent across ethnicities and countries in many parameters [
58], but it is also known to be influenced by diet and particularly by intakes of fatty acids [
14]. In the present study, we found that levels of PUFAs,
n-3 and
n-6 fatty acids, docosahexaenoic acid, and linoleic acid in the breast milk of Asian women were significantly higher compared to the other two ethnicities. While the intakes of the different types of dietary fat (monounsaturated, polyunsaturated, saturated) were similar between the different ethnic groups, the Asian women consumed fewer saturated fat and the proportion of dietary monounsaturated and polyunsaturated fats of total fat consumed was higher. This is supported by the lower number of dairy serves (higher in saturated fats) and higher number of serves of chicken (higher in polyunsaturated
n-6 fatty acids) observed here in the Asian mothers. A similar result was observed for
n-6 fatty acid contents in the breast milk of rural African women who consumed little animal fat [
59].
Studies linking diet and breast milk fatty acid contents have not shown consistent results. Su et al. [
60] found differences in breast milk fatty acid content between ethnicities, but the dietary intakes of
n-3 and
n-6 PUFAs for the different ethnicities were similar. Glew et al. [
61] found no correlation between dietary intakes of α-linoleic acid and DHA and the amounts of these fatty acids in the breast milk of women from New Mexico. In contrast, a study in South Korea found that the dietary intakes of eicosapentaenoic acid (EPA), docosahexaenoic acid (DHA), omega 3 (
n-3) fatty acids, omega 6 (
n-6) fatty acids, saturated fatty acids (SFAs), and polyunsaturated fatty acids (PUFAs) were highly positively correlated, with the corresponding fatty acids in the breast milk samples [
62], while a study in China found that dietary intakes and breast milk content of long chain
n-3 PUFAs and linolenic were positively correlated [
63]. Furthermore, other studies have shown that women who consume fish and other foods containing high levels of PUFA have relatively higher breast milk
n-3 fatty acids and DHA concentrations compared to milk from women who consume diets that are low in these components [
59,
64,
65]. In our study, the consumption of monounsaturated and polyunsaturated fats and fish were similar between the three ethnic groups. There were, however, correlations between dietary kilojoules from saturated fat, and
n-6, linoleic and PUFAs in the breast milk.
Trans-fatty acids in the milk were positively correlated with dietary saturated fat intake, and negatively correlated with polyunsaturated fat intake. Fatty acids in human milk are sourced not only from dietary fat but are also mobilized from maternal body fat and synthesized in the milk glands and hepatic cells. Therefore, the fatty acids found in human milk are likely to be influenced by short term and long term fatty acid dietary intake. The lack of consistency on the effect of dietary fatty acid intake on breast milk fatty acid composition in the literature is likely due to the collection of only short term fatty acid intake data, and not long term intakes, and the complex metabolic interdependencies between dietary and milk fatty acids.
The main strength of our study is that the breast milk nutrient composition and dietary nutrient intakes has been measured in NZ mothers of different ethnicity for the first time. A strength and a limitation of this study is that our participant population was in only one region (Manawatū-Whanganui) of New Zealand. While the ethnic composition of our study population was similar to that found in the overall population of NZ, the study region included urban and rural areas but no major cities where diet and lifestyle could be different. The second limitation is the collection of breast milk after the infant had fed, as the time of milk collection is known to affect the measurement of the breast milk fat content where the concentration differs between the beginning and end of feeding and over the day night cycle. The breast milk samples in the present study comprised 1.2% protein, 3.8% fat, and 7.5% total carbohydrate, which is very similar to the data from mature breast milk (g/dL; protein 0.9–1.2, fat 3.2–3.6, lactose 7.2–7.8) collected from a number of studies reviewed by Ballard and Morrow [
40]. The third limitation is the quantity of milk collected at each sampling (30 mL), which limited the quantity and therefore the range of nutrients that could be analyzed. This timing and quantity of breast milk collection were selected to ensure the infant had been fed and the infant’s and mother’s welfare were not compromised by the breast milk sampling.

 ,
, 



{kind=link}
{kind=link}