The Antisecretory Factor in Plasma and Breast Milk in Breastfeeding Mothers—A Prospective Cohort Study in Sweden

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and Ethical Approvals
2.2. Questionnaire
2.3. Samplings and Analysis of Antisecretory Factor (AF), Lactoferrin and Calcium
2.4. Samplings and Analysis of Oral Candida Colonization in Infants
2.5. Data Analyzes
3. Results
3.1. Descriptive Results
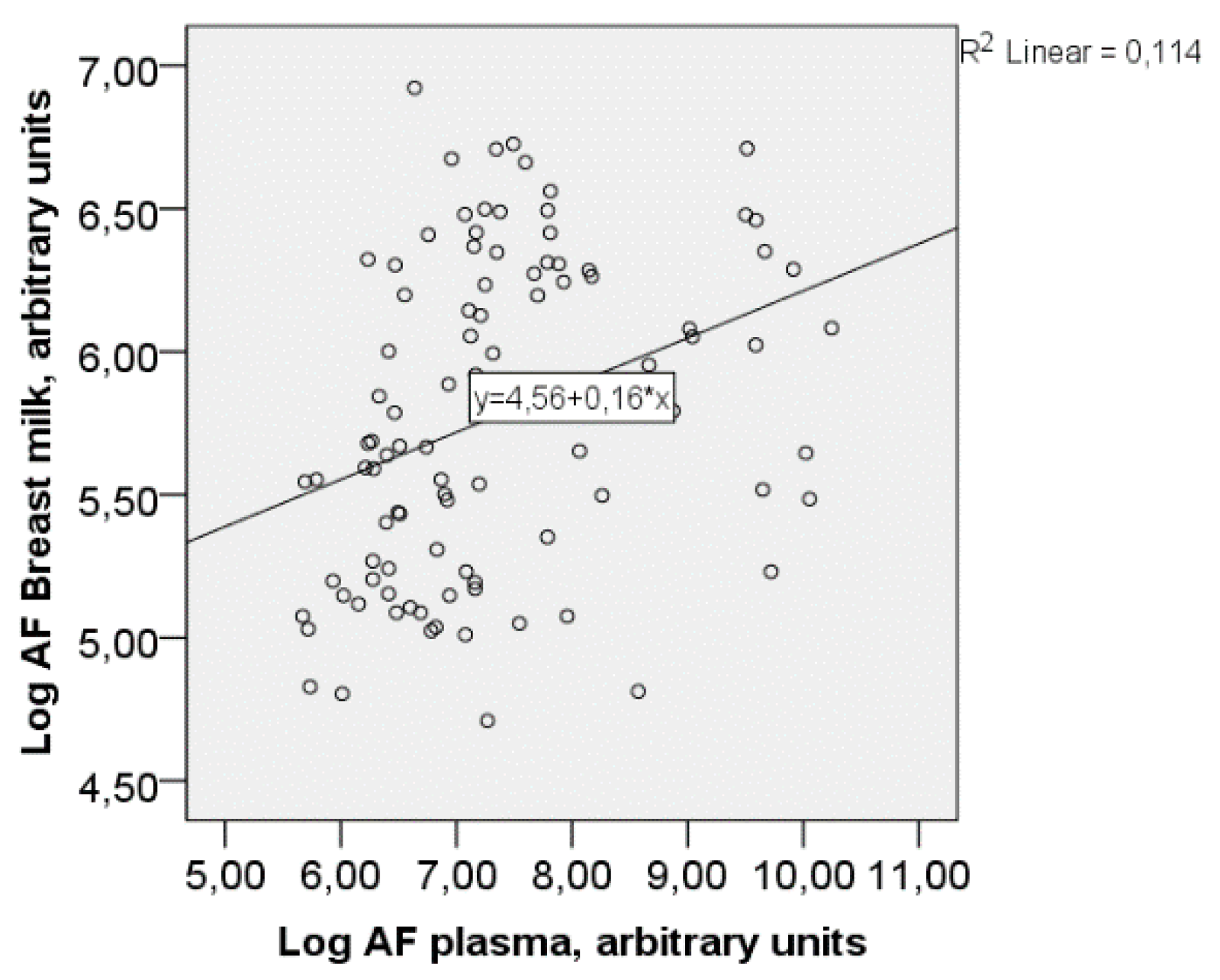
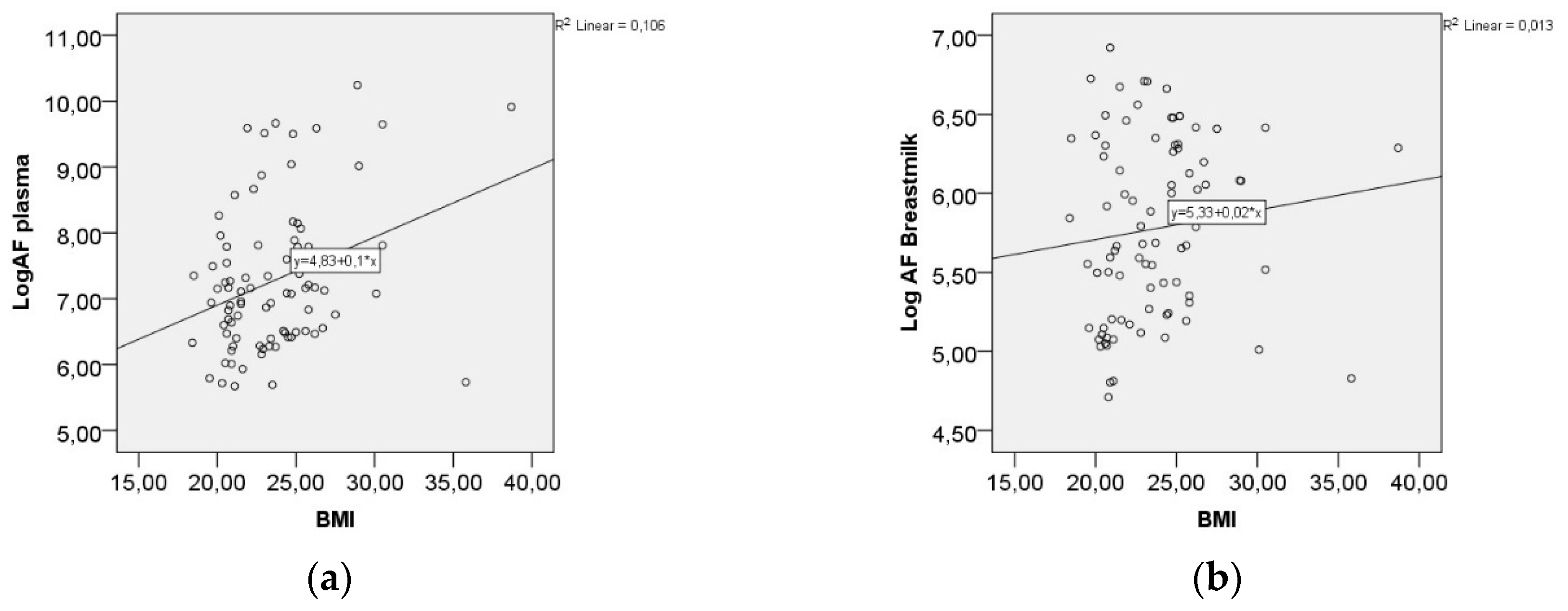
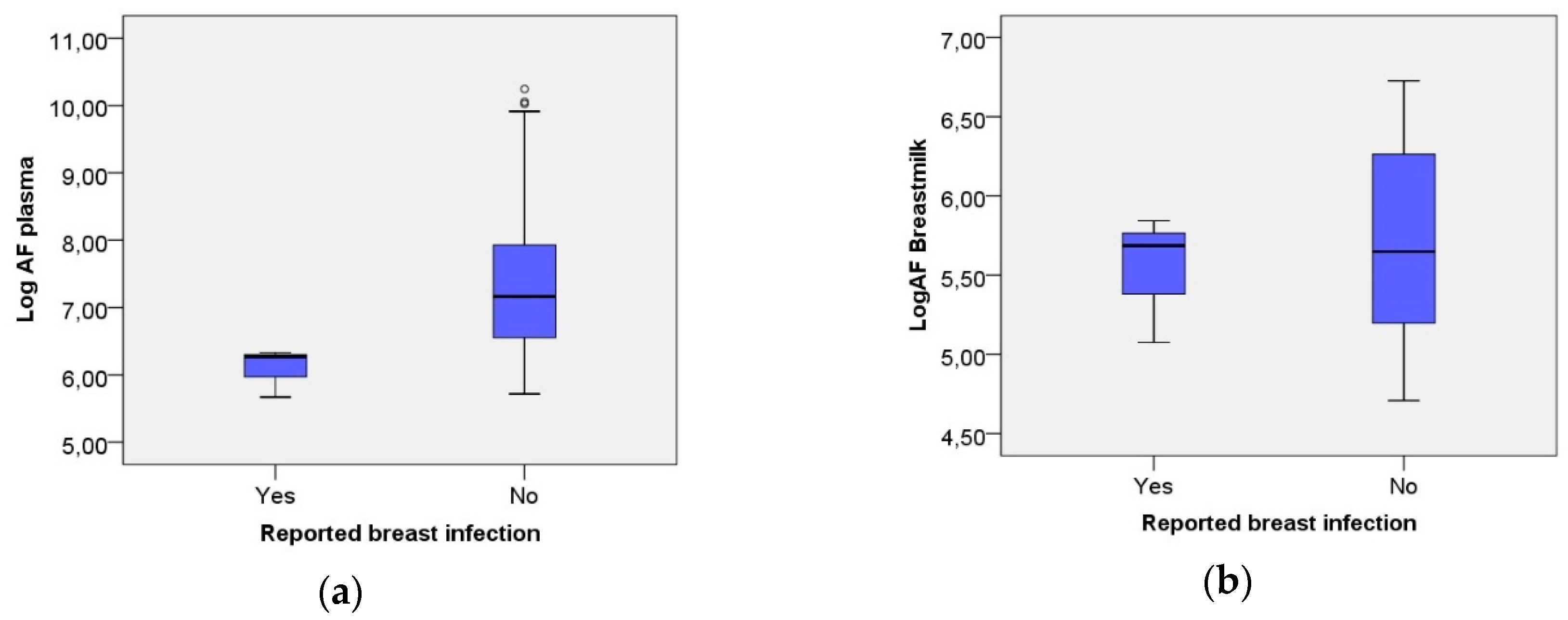
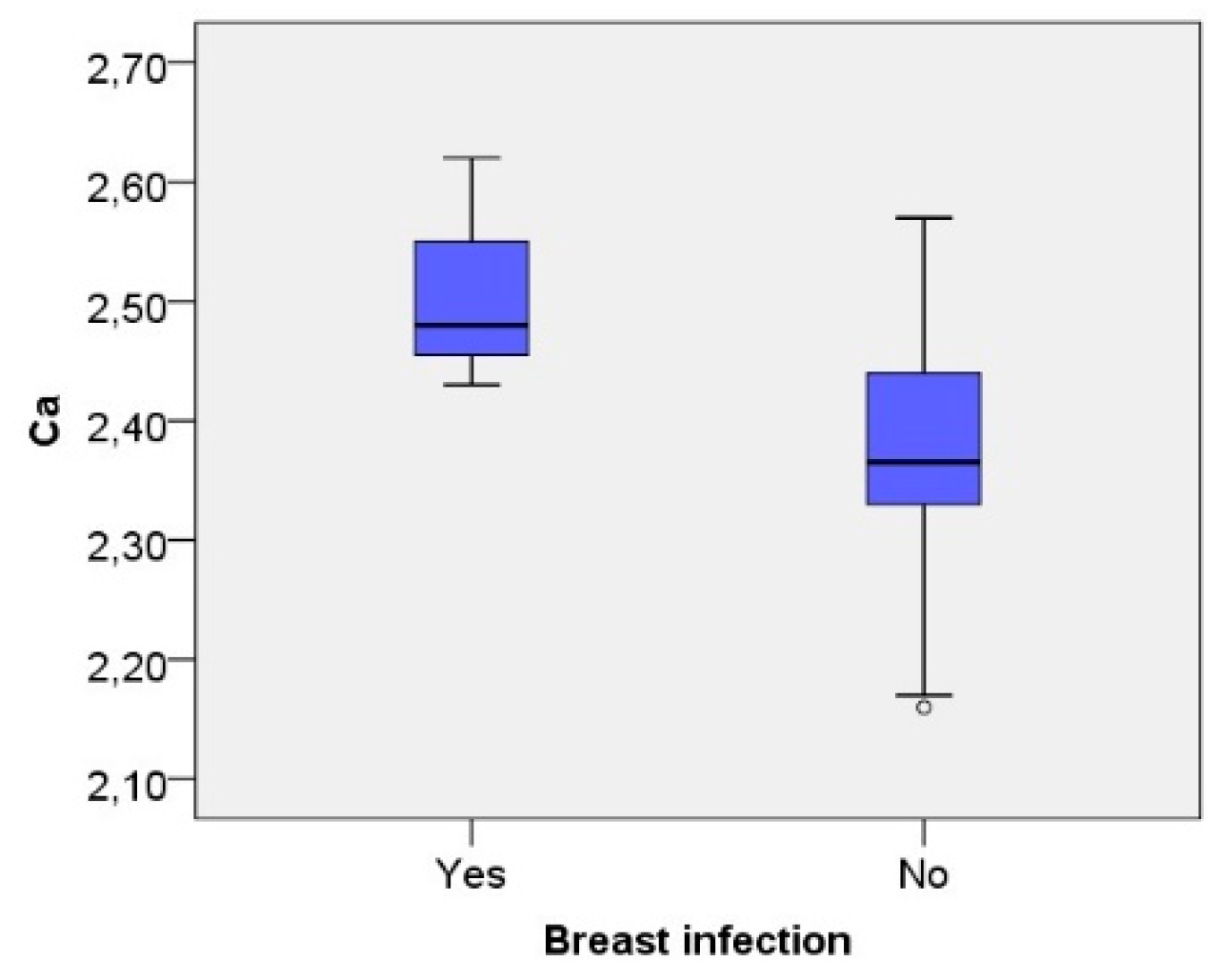
3.2. Analytical Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Goldenberg, R.L.; Culhane, J.F.; Iams, J.D.; Romero, R. Epidemiology and causes of preterm birth. Lancet 2008, 371, 75–84. [Google Scholar] [CrossRef]
- Blencowe, H.; Cousens, S.; Chou, D.; Oestergaard, M.; Say, L.; Moller, A.B.; Kinney, M.; Lawn, J.; Born Too Soon Preterm Birth, A. Born too soon: The global epidemiology of 15 million preterm births. Reprod. Health 2013, 10, S2. [Google Scholar] [CrossRef] [PubMed]
- Ballard, O.; Morrow, A.L. Human milk composition: Nutrients and bioactive factors. Pediatr. Clin. N. Am. 2013, 60, 49–74. [Google Scholar] [CrossRef] [PubMed]
- Berens, P.D. Breast pain: Engorgement, nipple pain, and mastitis. Clin. Obstet. Gynecol. 2015, 58, 902–914. [Google Scholar] [CrossRef] [PubMed]
- Inch, S.; Fisher, C. Breastfeeding: Early problems. Pract. Midwife 2000, 3, 12–15. [Google Scholar] [PubMed]
- Jahanfar, S.; Ng, C.J.; Teng, C.L. Antibiotics for mastitis in breastfeeding women. Cochrane Database Syst. Rev. 2009. [Google Scholar] [CrossRef]
- Ingman, W.V.; Glynn, D.J.; Hutchinson, M.R. Inflammatory mediators in mastitis and lactation insufficiency. J. Mammary Gland Biol. Neoplasia 2014, 19, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Andreas, N.J.; Kampmann, B.; Mehring Le-Doare, K. Human breast milk: A review on its composition and bioactivity. Early Hum. Dev. 2015, 91, 629–635. [Google Scholar] [CrossRef] [PubMed]
- Lonnerdal, B. Bioactive proteins in breast milk. J. Paediatr. Child Health 2013, 49 (Suppl. 1), 1–7. [Google Scholar] [CrossRef] [PubMed]
- Donovan, S.M.; Wang, M.; Li, M.; Friedberg, I.; Schwartz, S.L.; Chapkin, R.S. Host-microbe interactions in the neonatal intestine: Role of human milk oligosaccharides. Adv. Nutr. 2012, 3, 450s–455s. [Google Scholar] [CrossRef] [PubMed]
- Hanson, L.A. Session 1: Feeding and infant development breast-feeding and immune function. Proc. Nutr. Soc. 2007, 66, 384–396. [Google Scholar] [CrossRef] [PubMed]
- Cabrera-Rubio, R.; Collado, M.C.; Laitinen, K.; Salminen, S.; Isolauri, E.; Mira, A. The human milk microbiome changes over lactation and is shaped by maternal weight and mode of delivery. Am. J. Clin. Nutr. 2012, 96, 544–551. [Google Scholar] [CrossRef] [PubMed]
- Lange, S.; Lönnroth, I. The antisecretory factor: Synthesis, anatomical and cellular distribution, and biological action in experimental and clinical studies. Int. Rev. Cytol. 2001, 210, 39–75. [Google Scholar] [PubMed]
- Zaman, S.; Aamir, K.; Lange, S.; Jennische, E.; Silfverdal, S.A.; Hanson, L.A. Antisecretory factor effectively and safely stops childhood diarrhoea: A placebo-controlled, randomised study. Acta Paediatr. 2014, 103, 659–664. [Google Scholar] [CrossRef] [PubMed]
- Svensson, K.; Lange, S.; Lönnroth, I.; Widström, A.M.; Hanson, L. Induction of anti-secretory factor in human milk may prevent mastitis. Acta Paediatr. 2004, 93, 1228–1231. [Google Scholar] [CrossRef] [PubMed]
- Davidson, T.S.; Hickey, W.F. Distribution and immunoregulatory properties of antisecretory factor. Lab. Investig. 2004, 84, 307–319. [Google Scholar] [CrossRef] [PubMed]
- Ulgheri, C.; Paganini, B.; Rossi, F. Antisecretory factor as a potential health-promoting molecule in man and animals. Nutr. Res. Rev. 2010, 23, 300–313. [Google Scholar] [CrossRef] [PubMed]
- Lange, S.; Martinsson, K.; Lonnroth, I.; Goransson, L. Plasma level of antisecretory factor (ASF) and its relation to post-weaning diarrhoea in piglets. J. Vet. Med. Ser. B 1993, 40, 113–118. [Google Scholar] [CrossRef]
- Bjorck, S.; Bosaeus, I.; Ek, E.; Jennische, E.; Lonnroth, I.; Johansson, E.; Lange, S. Food induced stimulation of the antisecretory factor can improve symptoms in human inflammatory bowel disease: A study of a concept. Gut 2000, 46, 824–829. [Google Scholar] [CrossRef] [PubMed]
- Stecksen-Blicks, C.; Granstrom, E.; Silfverdal, S.A.; West, C.E. Prevalence of oral candida in the first year of life. Mycoses 2015, 58, 550–556. [Google Scholar] [CrossRef] [PubMed]
- Johansson, E.; Lange, S.; Lonnroth, I. Identification of an active site in the antisecretory factor protein. Biochim. Biophys. Acta 1997, 1362, 177–182. [Google Scholar] [CrossRef]
- Johansson, E.; Lonnroth, I.; Jonson, I.; Lange, S.; Jennische, E. Development of monoclonal antibodies for detection of antisecretory factor activity in human plasma. J. Immunol. Methods 2009, 342, 64–70. [Google Scholar] [CrossRef] [PubMed]
- Cox, A.J.; West, N.P.; Cripps, A.W. Obesity, inflammation, and the gut microbiota. Lancet Diabetes Endocrinol. 2015, 3, 207–215. [Google Scholar] [CrossRef]
- Hassiotou, F.; Hartmann, P.E. At the dawn of a new discovery: The potential of breast milk stem cells. Adv. Nutr. 2014, 5, 770–778. [Google Scholar] [CrossRef] [PubMed]
- Bode, L.; McGuire, M.; Rodriguez, J.M.; Geddes, D.T.; Hassiotou, F.; Hartmann, P.E.; McGuire, M.K. It’s alive: Microbes and cells in human milk and their potential benefits to mother and infant. Adv. Nutr. 2014, 5, 571–573. [Google Scholar] [CrossRef] [PubMed]
- Hassiotou, F.; Hepworth, A.R.; Metzger, P.; Tat Lai, C.; Trengove, N.; Hartmann, P.E.; Filgueira, L. Maternal and infant infections stimulate a rapid leukocyte response in breastmilk. Clin. Transl. Immunol. 2013, 2, e3. [Google Scholar] [CrossRef] [PubMed]
- Riskin, A.; Almog, M.; Peri, R.; Halasz, K.; Srugo, I.; Kessel, A. Changes in immunomodulatory constituents of human milk in response to active infection in the nursing infant. Pediatr. Res. 2012, 71, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Andrews, J.I.; Fleener, D.K.; Messer, S.A.; Hansen, W.F.; Pfaller, M.A.; Diekema, D.J. The yeast connection: Is candida linked to breastfeeding associated pain? Am. J. Obstet. Gynecol. 2007, 197, 424. [Google Scholar] [CrossRef] [PubMed]
- Jimenez, E.; Arroyo, R.; Cardenas, N.; Marin, M.; Serrano, P.; Fernandez, L.; Rodriguez, J.M. Mammary candidiasis: A medical condition without scientific evidence? PLoS ONE 2017, 12, e0181071. [Google Scholar] [CrossRef] [PubMed]
- Amir, L.H.; Cullinane, M.; Garland, S.M.; Tabrizi, S.N.; Donath, S.M.; Bennett, C.M.; Cooklin, A.R.; Fisher, J.R.; Payne, M.S. The role of micro-organisms (staphylococcus aureus and candida albicans) in the pathogenesis of breast pain and infection in lactating women: Study protocol. BMC Pregnancy Childbirth 2011, 11, 54. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Solomons, N.W.; Scott, M.E.; Koski, K.G. Subclinical mastitis (SCM) and proinflammatory cytokines are associated with mineral and trace element concentrations in human breast milk. J. Trace Elem. Med. Biol. 2018, 46, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Immler, R.; Simon, S.I.; Sperandio, M. Calcium signaling and related ion channels in neutrophil recruitment and function. Eur. J. Clin. Investig. 2018, e12964. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factor | Total |
|---|---|
| N = 95 | |
| Maternal characteristics | |
| Age (years) Mean (SD) (range) | 32 (4.5) 21–44 |
| Primiparous, n | 44 |
| BMI* (kg/m2) Median (range) | 23 (19.6–30.4) |
| Cesarean Section, n | 9 |
| Vaginal Candida Infection, n | 16 |
| Treatment for Candida Infection, n | 15 |
| Tobacco Use | |
| Maternal Smoking, n | 2 |
| Paternal Smoking, n | 1 |
| Maternal Use of Snuff, n | 2 |
| Infant characteristics | |
| Gestational Age < 37 Weeks | 3 |
| Birth Weight, Gram Mean (SD) | 3552 (481.5) |
| Female n | 50 |
| Oral Candida, n | 11 |
| Breast complications | |
| Pain in the Breast, n | 19 |
| Sore Nipples, n | 25 |
| Mastitis, n | 17 |
| Infection, n | 3 |
| AF Plasma Median (range) | 1240 (27,835) |
| log AF Plasma, Mean (SD) | 7.34 (1.15) |
| AF Breast Milk, Median (range) | 293 (904) |
| log AF Breast Milk, Mean (SD) | 5.77 (0.56) |
| Maternal Breast Complication | Infant Oral Candida Colonization | |||
|---|---|---|---|---|
| No Candida | Candida | p-Value | ||
| N | N | |||
| Mastitis | yes | 17 | 0 | >0.05 |
| no | 56 | 9 | ||
| Breast Infection | yes | 3 | 0 | >0.05 |
| no | 69 | 9 | ||
| Sore Nipples | yes | 23 | 2 | >0.05 |
| no | 50 | 6 | ||
| Pain in Breast/Nipples | yes | 17 | 2 | >0.05 |
| no | 56 | 7 | ||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gustafsson, A.; Granström, E.; Stecksén-Blicks, C.; West, C.E.; Silfverdal, S.-A. The Antisecretory Factor in Plasma and Breast Milk in Breastfeeding Mothers—A Prospective Cohort Study in Sweden. Nutrients 2018, 10, 1227. https://doi.org/10.3390/nu10091227
Gustafsson A, Granström E, Stecksén-Blicks C, West CE, Silfverdal S-A. The Antisecretory Factor in Plasma and Breast Milk in Breastfeeding Mothers—A Prospective Cohort Study in Sweden. Nutrients. 2018; 10(9):1227. https://doi.org/10.3390/nu10091227
Chicago/Turabian StyleGustafsson, Anna, Elisabeth Granström, Christina Stecksén-Blicks, Christina E. West, and Sven-Arne Silfverdal. 2018. "The Antisecretory Factor in Plasma and Breast Milk in Breastfeeding Mothers—A Prospective Cohort Study in Sweden" Nutrients 10, no. 9: 1227. https://doi.org/10.3390/nu10091227
APA StyleGustafsson, A., Granström, E., Stecksén-Blicks, C., West, C. E., & Silfverdal, S.-A. (2018). The Antisecretory Factor in Plasma and Breast Milk in Breastfeeding Mothers—A Prospective Cohort Study in Sweden. Nutrients, 10(9), 1227. https://doi.org/10.3390/nu10091227