Cross-Cultural Adaptation, Validity, and Reproducibility of the Mediterranean Islands Study Food Frequency Questionnaire in the Elderly Population Living in the Spanish Mediterranean

 ,
, 
Abstract
1. Introduction
2. Experimental Methods
2.1. Study Population
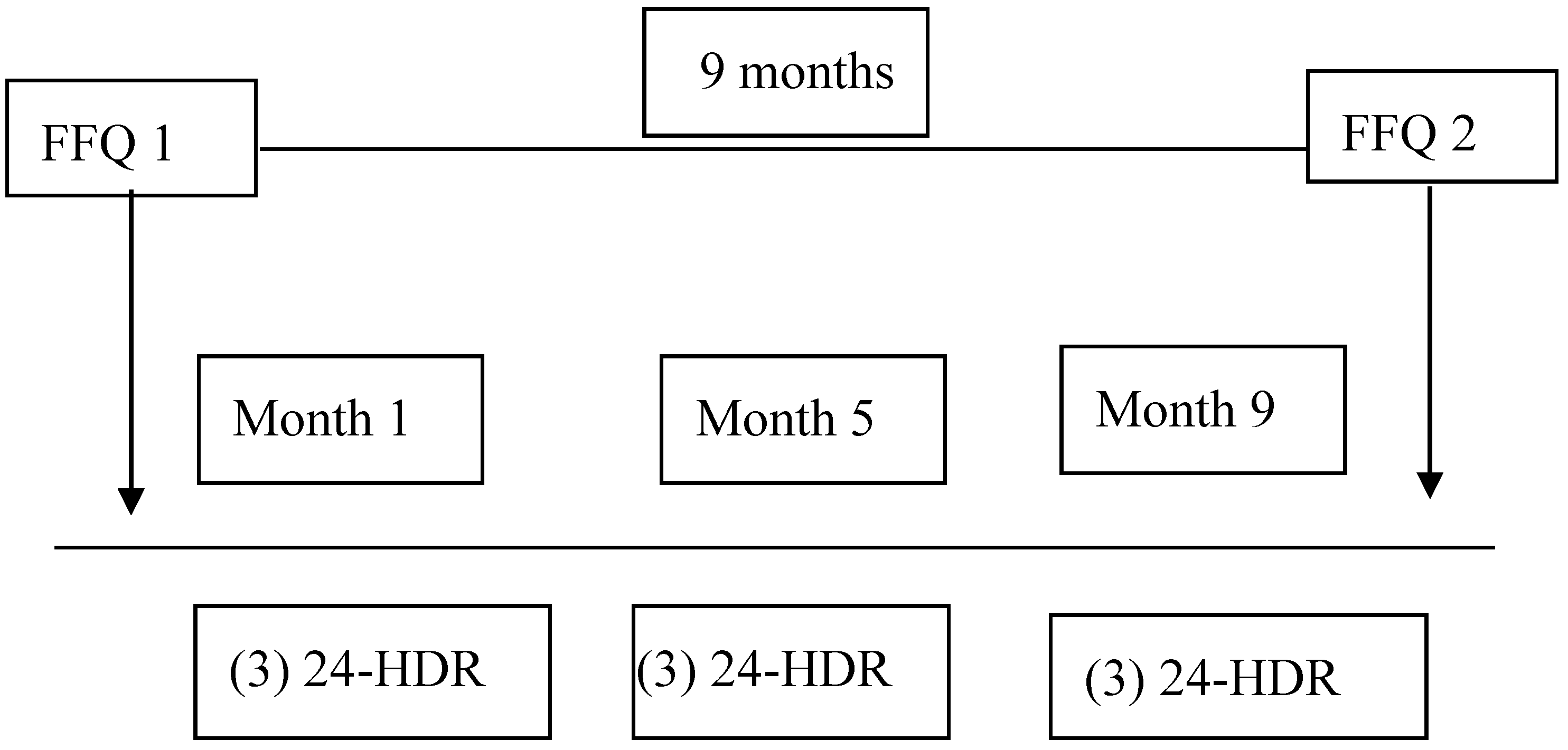
2.2. Study Design
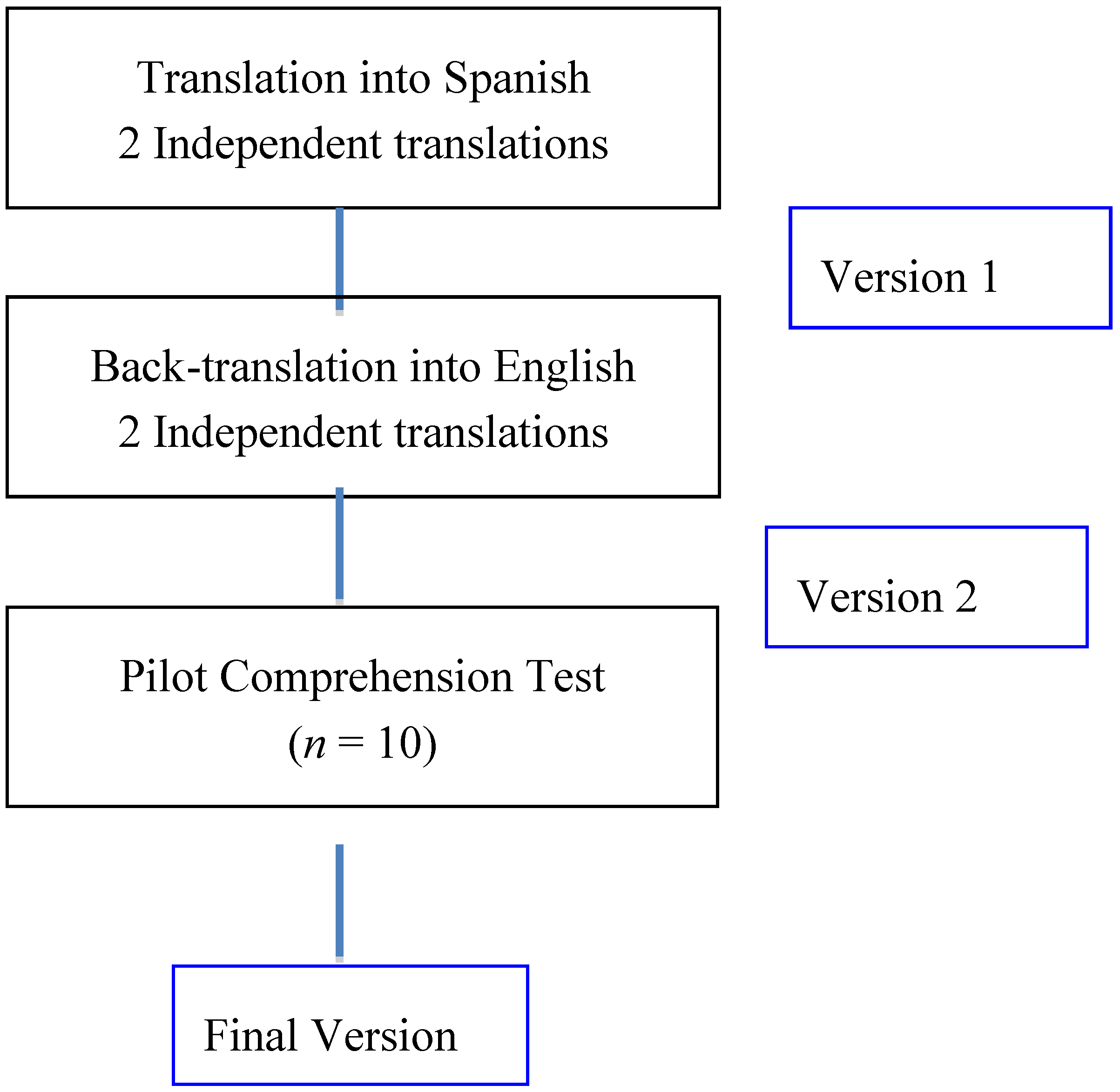
2.3. Cross-Cultural Translation and Adaptation
2.3.1. Direct Translation
2.3.2. Back-Translation
2.3.3. Pilot Comprehension Test
2.4. Instruments and Diet Evaluation
2.4.1. MEDIS-FFQ
2.4.2. 24-h Dietary Recall
2.5. Procedure
2.6. Ethical Considerations
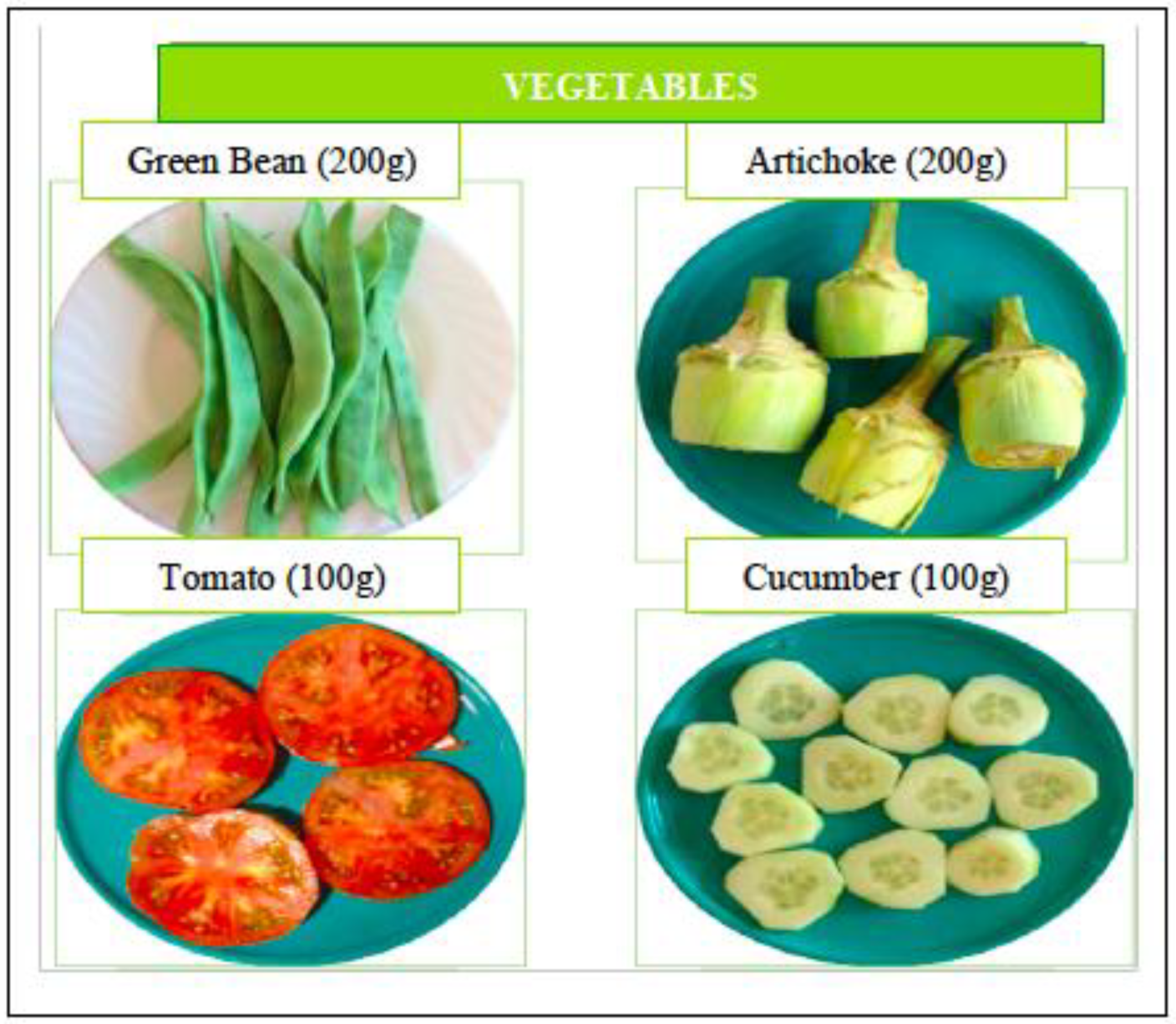
2.7. Calculation of Food Quantities and Nutrient Estimates
2.8. Statistical Analysis
2.8.1. Reproducibility
2.8.2. Validity
3. Results
3.1. Cross-Cultural Adaptation
3.2. Nutrient and Food Group Intakes
3.3. Reproducibility
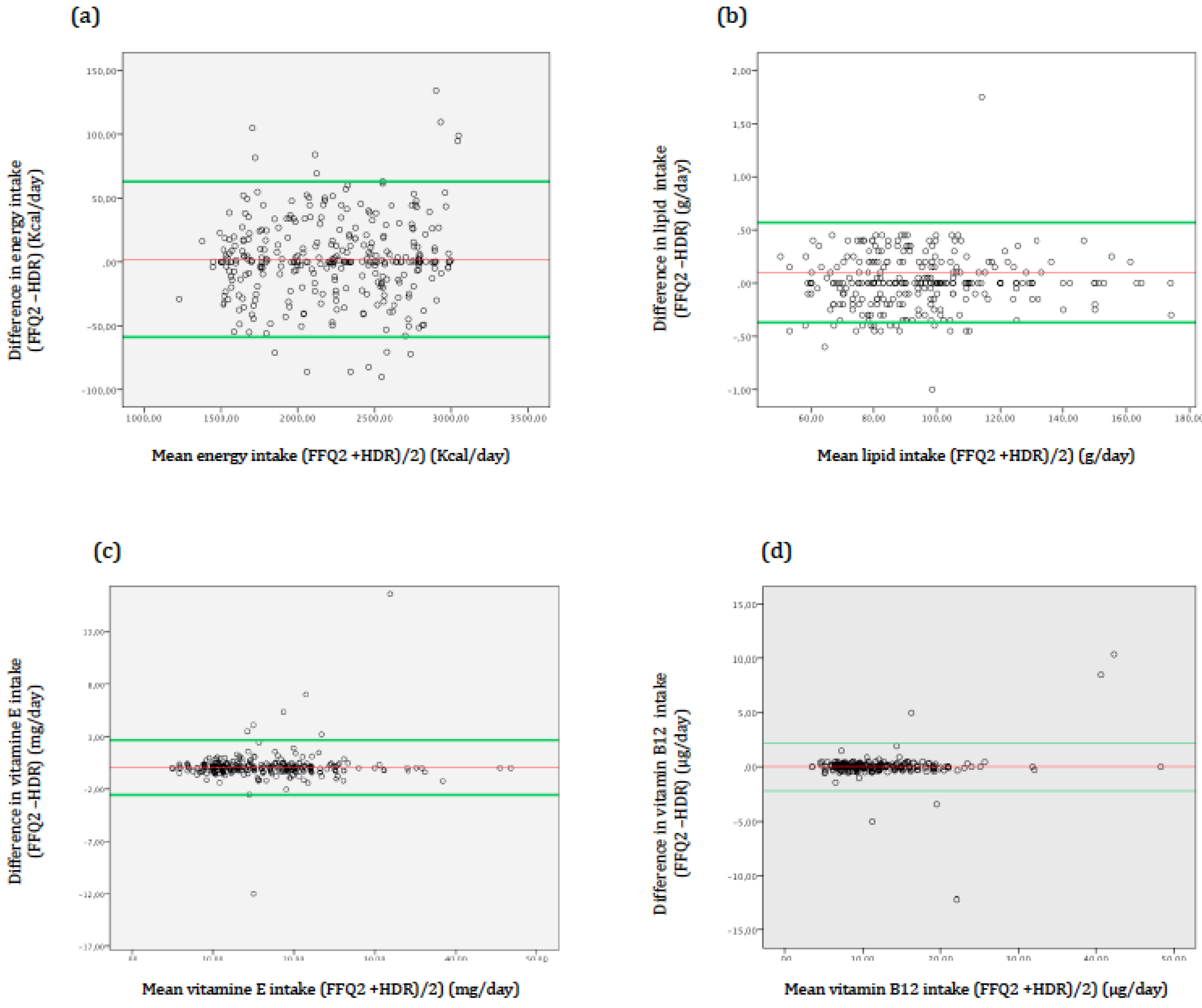
3.4. Validation
4. Discussion
4.1. Reproducibility
4.2. Validation
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Rodriguez, I.T.; Ballart, J.F.; Pastor, G.C.; Jordà, E.B.; Val, V.A. Validation of a short questionnaire on frequency of dietary intake: Reproducibility and validity. Nutr. Hosp. 2008, 23, 242–252. [Google Scholar] [PubMed]
- Liu, X.; Wang, X.; Lin, S.; Song, Q.; Lao, X.; Yu, I.T. Reproducibility and validity of a food frequency questionnaire for assessing dietary consumption via the dietary pattern method in a Chinese rural population. PLoS ONE 2015, 10, e0134627. [Google Scholar] [CrossRef] [PubMed]
- Cantin, J.; Latour, E.; Ferland-Verry, R.; Morales Salgado, S.; Lambert, J.; Faraj, M.; Nigam, A.; Morales Salgado, S.; Lambert, J.; Faraj, M.; Nigam, A. Validity and reproducibility of a food frequency questionnaire focused on the Mediterranean diet for the Quebec population. Nutr. Metab. Cardiovasc Dis. 2016, 26, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Schroder, H.; Fito, M.; Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventós, R.; Ros, E.; Salaverría, I.; Fiol, M.; et al. A short screener is valid for assessing Mediterranean diet adherence among older Spanish men and women. J. Nutr. 2011, 141, 1140–1145. [Google Scholar] [CrossRef] [PubMed]
- Jia, X.; Craig, L.C.; Aucott, L.S.; Milne, A.C.; McNeill, G. Repeatability and validity of a food frequency questionnaire in free-living older people in relation to cognitive function. J. Nutr. Health Aging 2008, 12, 735–741. [Google Scholar] [PubMed]
- Ye, Q.; Hong, X.; Wang, Z.; Yang, H.; Chen, X.; Zhou, H.; Wang, C.; Lai, Y.; Sun, L.; Xu, F. Reproducibility and validity of an FFQ developed for adults in Nanjing, China. Br. J. Nutr. 2016, 115, 887–894. [Google Scholar] [CrossRef] [PubMed]
- Eysteinsdottir, T.; Thorsdottir, I.; Gunnarsdottir, I.; Steingrimsdottir, L. Assessing validity of a short food frequency questionnaire on present dietary intake of elderly Icelanders. Nutr. J. 2012, 11, 12. [Google Scholar] [CrossRef] [PubMed]
- Bassett, J.K.; English, D.R.; Fahey, M.T.; Forbes, A.B.; Gurrin, L.C.; Simpson, J.A.; Brinkman, M.T.; Giles, G.G.; Hodge, A.M. Validity and calibration of the FFQ used in the Melbourne collaborative cohort study. Public Health Nutr. 2016, 19, 2357–2368. [Google Scholar] [CrossRef] [PubMed]
- Presse, N.; Shatenstein, B.; Kergoat, M.J.; Ferland, G. Validation of a semi-quantitative food frequency questionnaire measuring dietary vitamin K intake in elderly people. J. Am. Diet. Assoc. 2009, 109, 1251–1255. [Google Scholar] [CrossRef] [PubMed]
- Saravia, L.; Gonzalez-Zapata, L.I.; Rendo-Urteaga, T.; Ramos, J.; Collese, T.S.; Bove, I.; Delgado, C.; Tello, F.; Iglesia, I.; Gonçalves Sousa, E.D.; et al. Development of a food frequency questionnaire for assessing dietary intake in children and adolescents in South America. Obesity 2018, 26, S31–S40. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, M.; Yuan, Z.; Lin, L.; Hu, B.; Wang, X.; Yang, Y.; Chen, X.; Jin, L.; Lu, M.; Ye, W. Reproducibility and relative validity of a food frequency questionnaire developed for adults in Taizhou, China. PLoS ONE 2012, 7, e48341. [Google Scholar] [CrossRef] [PubMed]
- Ma, Z.F.; Skeaff, S.A. Assessment of population iodine status. In Iodine Deficiency Disorders and Their Elimination; Pearce, E.N., Ed.; Springer International Publishing: Cham, Switzerland, 2017; pp. 15–28. [Google Scholar]
- Villegas, R.; Yang, G.; Liu, D.; Xiang, Y.B.; Cai, H.; Zheng, W.; Shu, X.O. Validity and reproducibility of the food-frequency questionnaire used in the Shanghai men’s health study. Br. J. Nutr. 2007, 97, 993–1000. [Google Scholar] [CrossRef] [PubMed]
- Escobar, P.C.; Lerma, J.C.; Marin, D.H.; Donat Aliaga, E.; Masip Simó, E.; Polo Miquel, B.; Ribes Koninckx., C. Development and validation of two food frequency questionnaires to assess gluten intake in children up to 36 months of age. Nutr. Hosp. 2015, 32, 2080–2090. [Google Scholar]
- Vioque, J.; Navarrete-Munoz, E.M.; Gimenez-Monzo, D.; García-de-la-Hera, M.; Granado, F.; Young, I.S.; Ramón, R.; Ballester, F.; Murcia, M.; Rebagliato, M.; Iñiguez, C. INMA-Valencia Cohort Study. Reproducibility and validity of a food frequency questionnaire among pregnant women in a Mediterranean area. Nutr. J. 2013, 12, 26. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Ballart, J.D.; Pinol, J.L.; Zazpe, I.; Corella, D.; Carrasco, P.; Toledo, E.; Perez-Bauer, M.; Martínez-González, M.A.; Salas-Salvadó, J.; Martín-Moreno, J.M. Relative validity of a semi-quantitative food-frequency questionnaire in an elderly Mediterranean population of Spain. Br. J. Nutr. 2010, 103, 1808–1816. [Google Scholar] [CrossRef] [PubMed]
- Martin-Moreno, J.M.; Boyle, P.; Gorgojo, L.; Maisonneuve, P.; Fernandez-Rodriguez, J.C.; Salvini, S.; Willett, W.C. Development and validation of a food frequency questionnaire in Spain. Int J. Epidemiol. 1993, 22, 512–519. [Google Scholar] [CrossRef] [PubMed]
- Wild, D.; Grove, A.; Martin, M.; Eremenco, S.; McElroy, S.; Verjee-Lorenz, A.; Erikson, P. Principles of good practice for the translation and cultural adaptation process for patient-reported outcomes (PRO) measures: Report of the ISPOR task force for translation and cultural adaptation. Value Health 2005, 8, 94–104. [Google Scholar] [CrossRef] [PubMed]
- Tyrovolas, S.; Pounis, G.; Bountziouka, V.; Polychronopoulos, E.; Panagiotakos, D.B. Repeatability and validation of a short, semi-quantitative food frequency questionnaire designed for older adults living in Mediterranean areas: The MEDIS-FFQ. J. Nutr. Elderly 2010, 29, 311–324. [Google Scholar] [CrossRef] [PubMed]
- Jones, E.; McLean, R.; Davies, B.; Hawkins, R.; Meiklejohn, E.; Ma, Z.F.; Skeaff, S. Adequate iodine status in New Zealand School children post-fortification of bread with iodised salt. Nutrients 2016, 8, 298. [Google Scholar] [CrossRef] [PubMed]
- Willet, W. Nutritional Epidemiology, 3rd ed.; Oxford University Press: New York, NY, USA, 2013. [Google Scholar]
- Verdú, J.M. Tabla de Composición de Alimentos, 4nd ed.; Universidad de Granada: Granada, Spain, 2003. [Google Scholar]
- Palacios, C.; Trak, M.A.; Betancourt, J.; Joshipura, K.; Tucker, K.L. Validation and reproducibility of a semi-quantitative FFQ as a measure of dietary intake in adults from Puerto Rico. Public Health Nutr. 2015, 18, 2550–2558. [Google Scholar] [CrossRef] [PubMed]
- Pandey, D.; Bhatia, V.; Boddula, R.; Singh, H.K.; Bhatia, E. Validation and reproducibility of a food frequency questionnaire to assess energy and fat intake in affluent north Indians. Natl. Med. J. India. 2005, 18, 230–235. [Google Scholar] [PubMed]
- Bohlscheid-Thomas, S.; Hoting, I.; Boeing, H.; Boeing, H.; Wahrendorf, J. Reproducibility and relative validity of energy and macronutrient intake of a food frequency questionnaire developed for the German part of the EPIC project. European prospective investigation into cancer and nutrition. Int. J. Epidemiol. 1997, 26, S71–S81. [Google Scholar] [CrossRef] [PubMed]
- Deschamps, V.; de Lauzon-Guillain, B.; Lafay, L.; Borys, J.M.; Charles, M.A.; Romon, M. Reproducibility and relative validity of a food-frequency questionnaire among French adults and adolescents. Eur. J. Clin. Nutr. 2009, 63, 282–291. [Google Scholar] [CrossRef] [PubMed]
- Osowski, J.M.; Beare, T.; Specker, B. Validation of a food frequency questionnaire for assessment of calcium and bone-related nutrient intake in rural populations. J. Am. Diet. Assoc. 2007, 107, 1349–1355. [Google Scholar] [CrossRef] [PubMed]
- Jackson, M.D.; Motswagole, B.S.; Kwape, L.D.; Kobue-Lekalake, R.I.; Rakgantswana, T.B.; Mongwaketse, T.; Mokotedi, M.; Jackson-Malete, J. Validation and reproducibility of an FFQ for use among adults in Botswana. Public Health Nutr. 2013, 16, 1995–2004. [Google Scholar] [CrossRef] [PubMed]
- Giovannelli, J.; Dallongeville, J.; Wagner, A.; Bongard, V.; Laillet, B.; Marecaux, N.; Ruidavets, J.B.; Haas, B.; Ferrieres, J.; et al. Validation of a short, qualitative food frequency questionnaire in French adults participating in the MONA LISA-NUT study 2005–2007. J. Acad. Nutr. Diet 2014, 114, 552–561. [Google Scholar] [CrossRef] [PubMed]
- Pakseresht, M.; Sharma, S. Validation of a quantitative food frequency questionnaire for Inuit population in Nunavut, Canada. J. Hum. Nutr. Diet 2010, 23, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Yan, H.; Dibley, M.J.; Shen, Y.; Li, Q.; Zeng, L. Validity and reproducibility of a semi-quantitative food frequency questionnaire for use among pregnant women in rural China. Asia Pac. J. Clin. Nutr. 2008, 17, 166–177. [Google Scholar] [PubMed]
- Kim, D.W.; Song, S.; Lee, J.E.; Oh, K.; Shim, J.; Kweon, S.; Paik, H.Y.; Joung, H. Reproducibility and validity of an FFQ developed for the Korea national health and nutrition examination survey (KNHANES). Public Health Nutr. 2015, 18, 1369–1377. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (N = 341) | Women (N = 191) | Men (N = 150) | |
|---|---|---|---|
| N (%) | N (%) | N (%) | |
| Age | |||
| Mean | 72.59 | 73.38 | 71.58 |
| SD | 8.29 | 8.16 | 8.38 |
| Weight | |||
| Mean (kg) | 74.68 | 70.25 | 80.32 |
| SD | 12.89 | 11.67 | 12.18 |
| BMI | |||
| Mean | 27.61 | 27.69 | 27.52 |
| SD | 6.72 | 4.69 | 4.79 |
| Years of education | |||
| None | 43 (12.60) | 30 (15.70) | 13 (8.70) |
| 1–5 years | 66 (19.51) | 38 (19.90) | 28 (18.70) |
| 5–10 years | 123 (36.12) | 68 (35.60) | 55 (36.70) |
| >10 years | 109 (32.00) | 55 (28.80) | 54 (36.00) |
| Place of Residence | |||
| Urban | 271 (79.47) | 150 (78.50) | 121 (80.70) |
| Rural | 70 (20.53) | 41 (21.50) | 29 (19.30) |
| Civil Status | |||
| Married | 218 (63.93) | 114 (59.70) | 104 (69.30) |
| Widowed | 89 (26.10) | 60 (31.43) | 29 (19.30) |
| Divorced | 12 (3.52) | 7 (3.70) | 5 (3.30) |
| Single | 10 (2.93) | 6 (3.10) | 4 (2.70) |
| Living as a couple | 12 (3.52) | 4 (2.10) | 8 (5.30) |
| Alcohol Consumption | |||
| No | 150 (43.79) | 106 (55.50) | 44 (29.30) |
| Yes, usually | 32 (9.38) | 5 (2.60) | 27 (18.00) |
| Yes, occasional | 159 (46.63) | 80 (41.90) | 79 (52.70) |
| Tobacco Consumption | |||
| No | 257 (75.37) | 156 (81.68) | 104 (69.30) |
| Yes, usually | 65 (19.06) | 30 (15.70) | 35 (23.30) |
| Yes, occasional | 16 (4.69) | 5 (2.60) | 11 (7.30) |
| Physical Activity | |||
| No | 92 (26.98) | 56 (29.30) | 36 (24.00) |
| <2.5 h/week | 66 (19.35) | 42 (22.00) | 24 (16.00) |
| 2.5–7 h/week | 126 (36.95) | 74 (38.70) | 52 (34.70) |
| >7 h/week | 57 (16.74) | 19 (9.90) | 38 (25.30) |
| Food Groups | FFQ 1 | FFQ 2 | 24-HDR | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | |
| Dairy products (g) | 377.87 | 233.87 | 344.08 | 218.33 | 356.89 | 200.33 |
| Starchy foods (g) | 213.02 | 141.67 | 212.67 | 77.30 | 200.89 | 89.76 |
| Meat (g) | 140.04 | 87.42 | 140.89 | 75.28 | 145.98 | 77.89 |
| Fish (g) | 98.99 | 75.39 | 99.71 | 74.56 | 97.76 | 70.54 |
| Legumes (g) | 70.52 | 50.53 | 69.68 | 49.87 | 72.34 | 45.67 |
| Vegetables (g) | 205.45 | 122.84 | 207.65 | 123.45 | 201.76 | 121.98 |
| Fruits (g) | 475.06 | 212.4 | 469.98 | 201.50 | 450.98 | 200.7 |
| Nuts (g) | 8.21 | 4.67 | 8.09 | 4.53 | 7.98 | 4.56 |
| Sweets (g) | 95.52 | 34.56 | 90.92 | 30.12 | 93.45 | 30.21 |
| Snacks (g) | 30.48 | 22.24 | 35.29 | 25.86 | 32.12 | 21.34 |
| EVOO (g) | 62.32 | 38.36 | 61.97 | 37.32 | 60.78 | 35.45 |
| Alcoholic beverages (g) | 98.47 | 23.34 | 103.85 | 24.67 | 100.34 | 22.34 |
| Nutrient | FFQ 1 | FFQ 2 | 24-HDR | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | |
| Energy (kcal) | 2222.49 | 455.80 | 2380.08 | 1685.59 | 2301.28 | 920.15 |
| Proteins (g) | 88.52 | 58.66 | 87.58 | 39.29 | 88.05 | 37.44 |
| Lipids (g) | 96.48 | 23.03 | 99.16 | 54.20 | 97.82 | 33.72 |
| Saturated fats (g) | 28.97 | 5.69 | 29.04 | 5.78 | 29.00 | 5.70 |
| MUFAs (g) | 42.08 | 12.22 | 40.68 | 9.99 | 41.38 | 10.23 |
| PUFAs (g) | 13.84 | 3.94 | 13.92 | 4.07 | 13.88 | 3.96 |
| Cholesterol (g) | 242.50 | 69.56 | 240.13 | 67.25 | 241.32 | 66.63 |
| Carbohydrates (g) | 283.99 | 54.23 | 284.24 | 54.72 | 284.12 | 54.46 |
| Fibre (g) | 31.15 | 9.35 | 31.52 | 10.14 | 31.33 | 9.43 |
| Potassium (mg) | 3545.14 | 721.29 | 3670.94 | 2518.52 | 3608.04 | 1432.14 |
| Sodium (mg) | 2677.46 | 670.22 | 2687.47 | 674.38 | 2682.47 | 668.83 |
| Calcium (mg) | 1198.45 | 525.36 | 1175.82 | 313.76 | 1187.14 | 371.66 |
| Iron (mg) | 12.16 | 3.27 | 12.54 | 8.41 | 12.35 | 5.13 |
| Iodide (μg) | 105.69 | 58.50 | 106.53 | 70.30 | 106.06 | 51.67 |
| Vitamin B1 (mg) | 1.57 | 1.03 | 1.53 | 0.90 | 1.55 | 0.73 |
| Vitamin B2 (mg) | 3.03 | 1.58 | 2.98 | 1.16 | 3.00 | 1.27 |
| Vitamin B6 (mg) | 2.51 | 0.85 | 2.50 | 0.85 | 2.51 | 0.84 |
| Vitamin B12 (μg) | 11.66 | 5.34 | 11.70 | 5.57 | 11.68 | 5.34 |
| Vitamin C (mg) | 255.63 | 102.32 | 255.72 | 103.77 | 255.68 | 101.92 |
| Vitamin A (μg) | 1180.73 | 890.26 | 1140.96 | 859.57 | 1160.84 | 657.02 |
| Vitamin D (μg) | 5.77 | 2.78 | 5.78 | 2.83 | 5.78 | 2.79 |
| Vitamin E (mg) | 16.09 | 6.66 | 16.25 | 6.60 | 16.17 | 6.49 |
| Nutrient | Interclass Correlation Coefficient | Agreement (%) * | Agreement Significance | |
|---|---|---|---|---|
| Unadjusted | Adjusted † | |||
| Energy (kcal) | 0.99 | - | 55.5 | <0.01 |
| Proteins (g) | 0.88 | 0.79 | 30.7 | <0.01 |
| Lipids (g) | 0.86 | 0.85 | 40.1 | <0.01 |
| Saturated fats (g) | 0.99 | 0.81 | 99.6 | <0.01 |
| MUFAs (g) | 0.81 | 0.80 | 77.8 | <0.01 |
| PUFAs (g) | 0.97 | 0.79 | 89.4 | <0.01 |
| Cholesterol (g) | 0.89 | 0.80 | 42.7 | <0.01 |
| Carbohydrates (g) | 0.99 | 0.86 | 88.7 | <0.01 |
| Fibre (g) | 0.87 | 0.78 | 71.7 | <0.01 |
| Potassium (mg) | 0.33 | 0.30 | 87.6 | <0.01 |
| Sodium (mg) | 0.99 | 0.89 | 40.1 | <0.01 |
| Calcium (mg) | 0.66 | 0.64 | 78.9 | <0.01 |
| Iron (mg) | 0.45 | 0.44 | 56.7 | <0.01 |
| Iodide (μg) | 0.43 | 0.45 | 54.7 | <0.01 |
| Vitamin B1 (mg) | 0.57 | 0.56 | 67.8 | <0.01 |
| Vitamin B2 (mg) | 0.80 | 0.81 | 67.8 | <0.01 |
| Vitamin B6 (mg) | 0.98 | 0.87 | 98.7 | <0.01 |
| Vitamin B12 (μg) | 0.96 | 0.90 | 90.7 | <0.01 |
| Vitamin C (mg) | 0.96 | 0.89 | 78.9 | <0.01 |
| Vitamin A (μg) | 0.50 | 0.49 | 55.6 | <0.01 |
| Vitamin D (μg) | 0.98 | 0.91 | 87.6 | <0.01 |
| Vitamin E (mg) | 0.98 | 0.87 | 89.8 | <0.01 |
| Nutrient | Pearson’s Correlation Coefficient | Difference of Means | ||
|---|---|---|---|---|
| Unadjusted | Adjusted * | Mean | SD | |
| Energy (kcal) | 0.97 | - | 1.97 | 31.07 |
| Proteins (g) | 0.99 | 0.98 | 0.26 | 2.01 |
| Lipids (g) | 0.95 | 0.95 | 1.34 | 24.43 |
| Saturated fats (g) | 0.99 | 0.99 | 0.03 | 0.54 |
| MUFAs (g) | 0.90 | 0.90 | −0.70 | 4.46 |
| PUFAs (g) | 0.78 | 0.80 | 0.04 | 0.61 |
| Cholesterol (g) | 0.97 | 0.97 | −1.18 | 15.52 |
| Carbohydrates (g) | 0.87 | 0.89 | 0.12 | 1.58 |
| Fibre (g) | 0.97 | 0.97 | 0.19 | 2.50 |
| Potassium (mg) | 0.97 | 0.97 | 62.90 | 1174.99 |
| Sodium (mg) | 0.89 | 0.99 | 5.00 | 68.27 |
| Calcium (mg) | 0.80 | 0.80 | −11.32 | 221.58 |
| Iron (mg) | 0.95 | 0.95 | 0.19 | 3.80 |
| Iodide (μg) | 0.84 | 0.84 | 0.46 | 38.89 |
| Vitamin B1 (mg) | 0.71 | 0.71 | −0.20 | 0.64 |
| Vitamin B2 (mg) | 0.89 | 0.89 | −0.22 | 0.56 |
| Vitamin B6 (mg) | 0.99 | 0.99 | −0.01 | 0.11 |
| Vitamin B12 (μg) | 0.98 | 0.98 | 0.2 | 1.11 |
| Vitamin C (mg) | 0.89 | 0.98 | 0.05 | 15.22 |
| Vitamin A (μg) | 0.74 | 0.78 | −19.89 | 577.95 |
| Vitamin D (μg) | 0.88 | 0.99 | 0.01 | 0.32 |
| Vitamin E (mg) | 0.76 | 0.78 | 0.08 | 1.36 |
| Nutrient | FFQ2 vs. 24-HDR | Kappa | Significance | ||
|---|---|---|---|---|---|
| Same (%) | Adjacent (%) | Extreme (%) | |||
| Energy (kcal) | 95.88 | 4.12 | 0.00 | 0.95 | <0.01 |
| Proteins (g) | 97.94 | 2.06 | 0.00 | 0.97 | <0.01 |
| Lipids (g) | 94.12 | 5.88 | 0.00 | 0.92 | <0.01 |
| Saturated fats (g) | 95.29 | 4.71 | 0.00 | 0.94 | <0.01 |
| MUFAs (g) | 90.88 | 7.35 | 0.59 | 0.88 | <0.01 |
| PUFAs (g) | 98.53 | 1.47 | 0.59 | 0.98 | <0.01 |
| Cholesterol (g) | 96.18 | 2.94 | 0.29 | 0.95 | <0.01 |
| Carbohydrates (g) | 95.29 | 2.94 | 0.59 | 0.94 | <0.01 |
| Fibre (g) | 97.65 | 2.35 | 0.00 | 0.96 | <0.01 |
| Potassium (mg) | 98.53 | 1.47 | 0.00 | 0.98 | <0.01 |
| Sodium (mg) | 99.88 | 1.18 | 0.00 | 0.97 | <0.01 |
| Calcium (mg) | 97.65 | 1.76 | 0.29 | 0.96 | <0.01 |
| Iron (mg) | 96.18 | 3.53 | 0.00 | 0.93 | <0.01 |
| Iodide (μg) | 97.35 | 2.05 | 0.00 | 0.96 | <0.01 |
| Vitamin B1 (mg) | 83.53 | 14.12 | 2.06 | 0.78 | <0.01 |
| Vitamin B2 (mg) | 97.65 | 4.71 | 0.00 | 0.93 | <0.01 |
| Vitamin B6 (mg) | 89.44 | 10.00 | 0.00 | 0.86 | <0.01 |
| Vitamin B12 (μg) | 95.00 | 5.00 | 0.00 | 0.93 | <0.01 |
| Vitamin C (mg) | 95.29 | 4.41 | 0.00 | 0.93 | <0.01 |
| Vitamin A (μg) | 83.53 | 15.59 | 0.59 | 0.78 | <0.01 |
| Vitamin D (μg) | 92.35 | 7.64 | 0.00 | 0.89 | <0.01 |
| Vitamin E (mg) | 87.65 | 12.03 | 0.29 | 0.84 | <0.01 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zaragoza-Martí, A.; Ferrer-Cascales, R.; Hurtado-Sánchez, J.A.; Laguna-Pérez, A.; Cabañero-Martínez, M.J. Cross-Cultural Adaptation, Validity, and Reproducibility of the Mediterranean Islands Study Food Frequency Questionnaire in the Elderly Population Living in the Spanish Mediterranean. Nutrients 2018, 10, 1206. https://doi.org/10.3390/nu10091206
Zaragoza-Martí A, Ferrer-Cascales R, Hurtado-Sánchez JA, Laguna-Pérez A, Cabañero-Martínez MJ. Cross-Cultural Adaptation, Validity, and Reproducibility of the Mediterranean Islands Study Food Frequency Questionnaire in the Elderly Population Living in the Spanish Mediterranean. Nutrients. 2018; 10(9):1206. https://doi.org/10.3390/nu10091206
Chicago/Turabian StyleZaragoza-Martí, Ana, Rosario Ferrer-Cascales, José Antonio Hurtado-Sánchez, Ana Laguna-Pérez, and María José Cabañero-Martínez. 2018. "Cross-Cultural Adaptation, Validity, and Reproducibility of the Mediterranean Islands Study Food Frequency Questionnaire in the Elderly Population Living in the Spanish Mediterranean" Nutrients 10, no. 9: 1206. https://doi.org/10.3390/nu10091206
APA StyleZaragoza-Martí, A., Ferrer-Cascales, R., Hurtado-Sánchez, J. A., Laguna-Pérez, A., & Cabañero-Martínez, M. J. (2018). Cross-Cultural Adaptation, Validity, and Reproducibility of the Mediterranean Islands Study Food Frequency Questionnaire in the Elderly Population Living in the Spanish Mediterranean. Nutrients, 10(9), 1206. https://doi.org/10.3390/nu10091206