The Role of Choice in Weight Loss Strategies: A Systematic Review and Meta-Analysis




Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Study Selection
2.3. Data Analysis
3. Results
3.1. Systematic Review
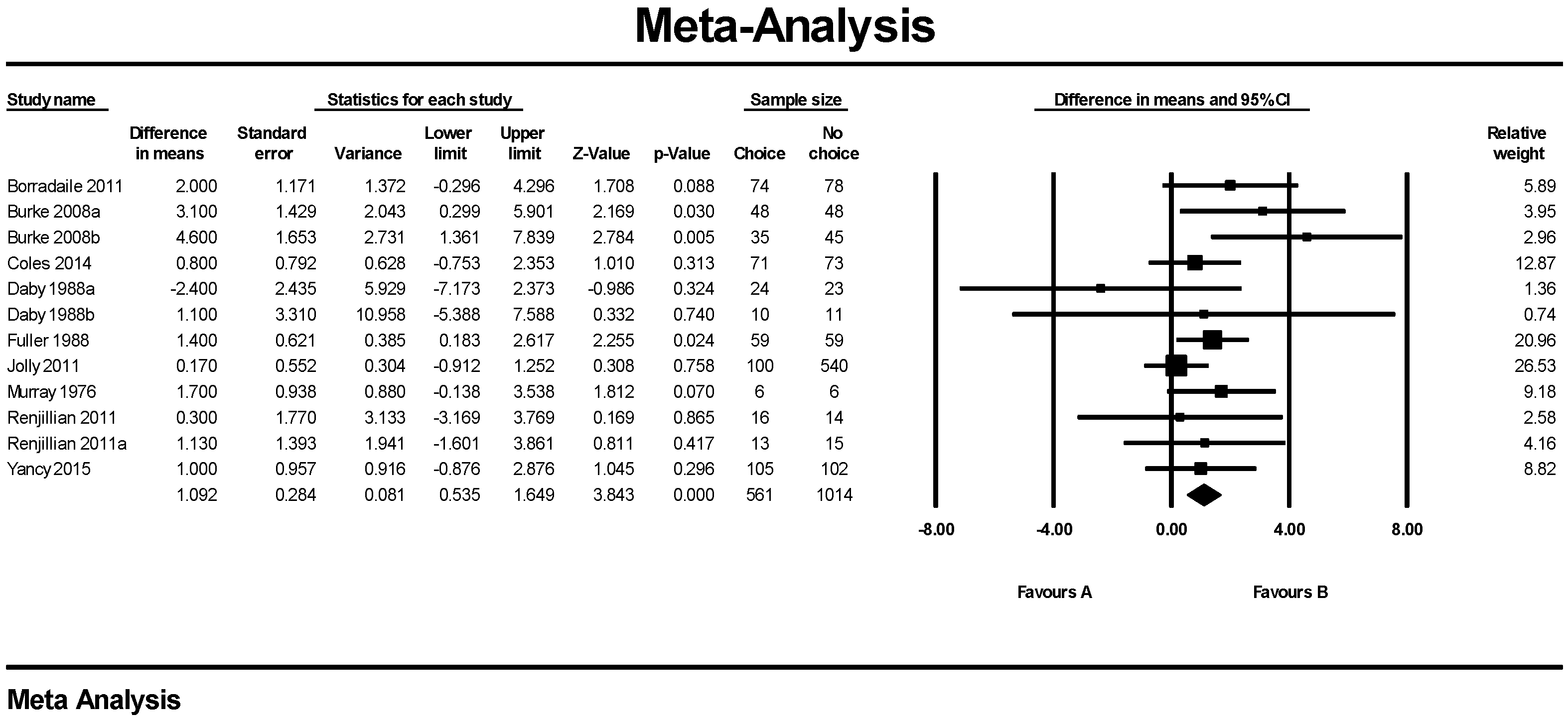
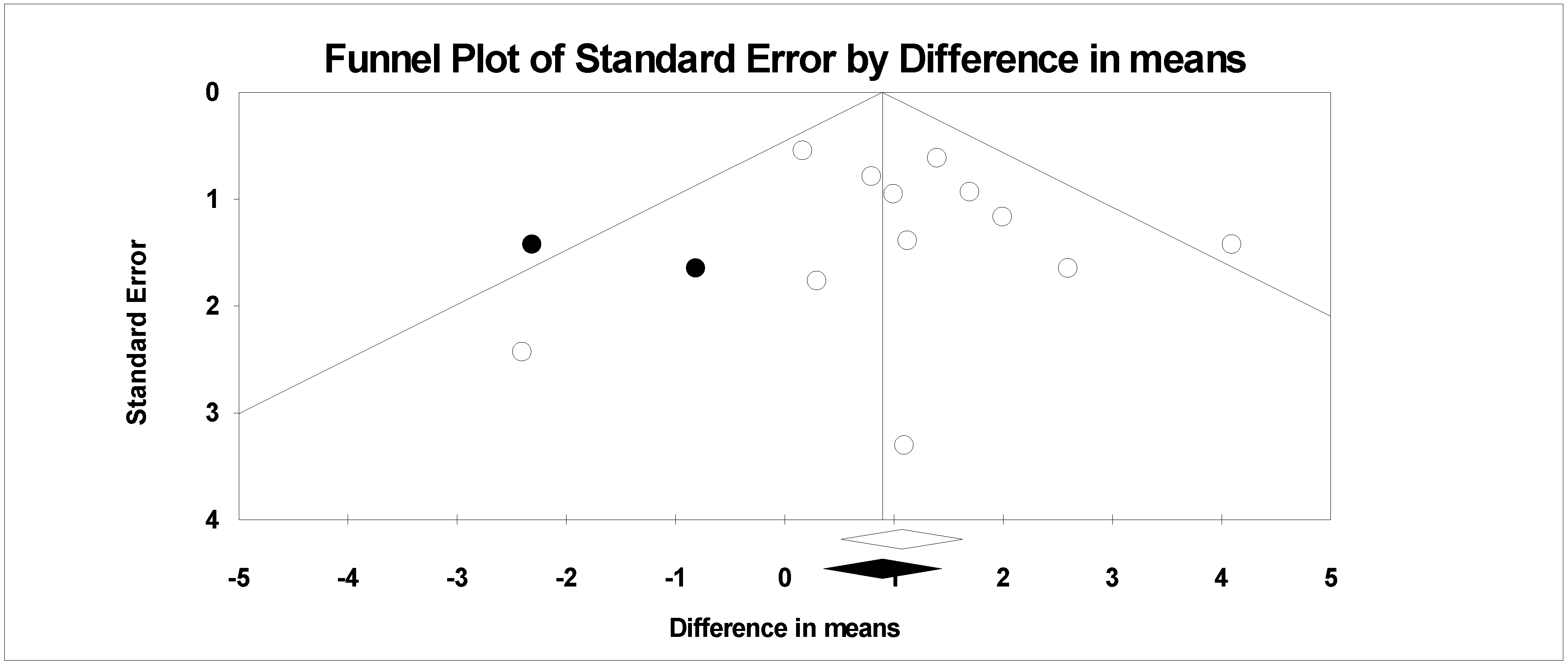
3.2. Meta-Analysis
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Conflicts of Interest
References
- World Health Organisation. Obesity: Situation and Trends. Available online: http://www.who.int/gho/ncd/risk_factors/obesity_text/en (accessed on 1 February 2018).
- Johnston, B.C.; Kanters, S.; Bandayrel, K.; Wu, P.; Naji, F.; Siemieniuk, R.A.; Ball, G.D.; Busse, J.W.; Thorlund, K.; Guyatt, G.; et al. Comparison of weight loss among named diet programs in overweight and obese adults: A meta-analysis. JAMA 2014, 312, 923–933. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.D.; Ryan, D.H.; Apovian, C.M.; Ard, J.D.; Comuzzie, A.G.; Donato, K.A.; Hu, F.B.; Hubbard, V.S.; Jakicic, J.M.; Kushner, R.F.; et al. 2013 AHA/ACC/TOS Guideline for the management of overweight and obesity in adults. J. Am. Coll. Cardiol. 2014, 63, 2985–3023. [Google Scholar] [CrossRef] [PubMed]
- Sacks, F.M.; Bray, G.A.; Carey, V.J.; Smith, S.R.; Ryan, D.H.; Anton, S.D.; McManus, K.; Champagne, C.M.; Bishop, L.M.; Laranjo, N.; et al. Comparison of weight-loss diets with different compositions of fat, protein, and carbohydrates. N. Eng. J. Med. 2009, 360, 859–873. [Google Scholar] [CrossRef] [PubMed]
- Franz, M.J.; VanWormer, J.J.; Crain, A.L.; Boucher, J.L.; Histon, T.; Caplan, W.; Bowman, J.D.; Pronk, N.P. Weight-loss outcomes: A systematic review and meta-analysis of weight-loss clinical trials with a minimum 1-year follow-up. J. Am. Diet Assoc. 2017, 107, 1755–1767. [Google Scholar] [CrossRef] [PubMed]
- Pagoto, S.L.; Appelhans, B.M. A call for an end to the diet debates. JAMA 2013, 310, 687–688. [Google Scholar] [CrossRef] [PubMed]
- Dansinger, M.L.; Gleason, J.A.; Griffith, J.L.; Selker, H.P.; Schaefer, E.J. Comparison of the Atkins, Ornish, weight watchers, and zone diets for weight loss and heart disease risk reduction: A randomized trial. JAMA 2005, 293, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, I.; Stampfer, M.J.; Schwarzfuchs, D.; Shai, I.; DIRECT Group. Adherence and success in long-term weight loss diets: The dietary intervention randomized controlled trial (DIRECT). J. Am. Coll. Nutr. 2009, 28, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Jiandani, D.; Wharton, S.; Rotondi, M.A.; Ardern, C.I.; Kuk, J.L. Predictors of early attrition and successful weight loss in patients attending an obesity management program. BMC Obes. 2016, 3, 14. [Google Scholar] [CrossRef] [PubMed]
- Lemstra, M.; Bird, Y.; Nwankwo, C.; Rogers, M.; Moraros, J. Weight loss intervention adherence and factors promoting adherence: A meta-analysis. Patient Prefer. Adher. 2016, 10, 1547–1559. [Google Scholar]
- Sykes-Muskett, B.J.; Prestwich, A.; Lawton, R.J.; Armitage, C.J. The utility of monetary contingency contracts for weight loss: A systematic review and meta-analysis. Health Psychol. Rev. 2015, 9, 434–451. [Google Scholar] [CrossRef] [PubMed]
- Finkelstein, E.A.; Linnan, L.A.; Tate, D.F.; Birken, B.E. A pilot study testing the effect of different levels of financial incentives on weight loss among overweight employees. J. Occup. Environ. Med. 2007, 49, 981–989. [Google Scholar] [CrossRef] [PubMed]
- Epstein, L.H. Role of behavior theory in behavioral medicine. J. Consult. Clin. Psychol. 1992, 60, 493–498. [Google Scholar] [CrossRef] [PubMed]
- Lindhiem, O.; Bennett, C.B.; Trentacosta, C.J.; McLear, C. Client preferences affect treatment satisfaction, completion, and clinical outcome: A meta-analysis. Clin. Psychol. Rev. 2014, 34, 506–517. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef] [PubMed]
- Bernier, M.; Avard, J. Self-efficacy, outcome, and attrition in a weight-reduction program. Cognit. Ther. Res. 1986, 10, 319–338. [Google Scholar] [CrossRef]
- Elfhag, K.; Rössner, S. Who succeeds in maintaining weight loss? A conceptual review of factors associated with weight loss maintenance and weight regain. Obes. Rev. 2005, 6, 67–85. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, P.J.; Going, S.B.; Houtkooper, L.B.; Cussler, E.C.; Metcalfe, L.L.; Blew, R.M.; Sardinha, L.B.; Lohman, T.G. Pretreatment predictors of attrition and successful weight management in women. Int. J. Obes. Relat. Metab. Disord. 2004, 28, 1124–1133. [Google Scholar] [CrossRef] [PubMed]
- Kofta, M. Freedom of choice and moral behavior. In Development and Maintenance of Prosocial Behavior; Staub, E., Ed.; Springer US: Boston, MA, USA, 1984; pp. 257–269. [Google Scholar]
- Schifter, D.E.; Ajzen, I. Intention, perceived control, and weight loss: An application of the theory of planned behavior. J. Pers. Soc. Psychol. 1985, 49, 843–851. [Google Scholar] [CrossRef] [PubMed]
- Madigan, C.D.; Pavey, T.; Daley, A.J.; Jolly, K.; Brown, W.J. Is weight cycling associated with adverse health outcomes? A cohort study. Prev. Med. 2018, 108, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Marcus, S.M.; Stuart, E.A.; Wang, P.; Shadish, W.R.; Steiner, P.M. Estimating the causal effect of randomization versus treatment preference in a doubly randomized preference trial. Psychol. Methods 2012, 17, 244–254. [Google Scholar] [CrossRef] [PubMed]
- Borradaile, K.E.; Halpern, S.D.; Wyatt, H.R.; Klein, S.; Hill, J.O.; Bailer, B.; Brill, C.; Stein, R.I.; Miller, B.V., 3rd; Foster, G.D. Relationship between treatment preference and weight loss in the context of a randomized controlled trial. Obesity 2012, 20, 1218–1222. [Google Scholar] [CrossRef] [PubMed]
- Yancy, W.S., Jr.; Mayer, S.B.; Coffman, C.J.; Smith, V.A.; Kolotkin, R.L.; Geiselman, P.J.; McVay, M.A.; Oddone, E.Z.; Voils, C.I. Effect of allowing choice of diet on weight loss: A randomized trial. Ann. Intern. Med. 2015, 162, 805–814. [Google Scholar] [CrossRef] [PubMed]
- Renjilian, D.A.; Perri, M.G.; Nezu, A.M.; McKelvey, W.F.; Shermer, R.L.; Anton, S.D. Individual versus group therapy for obesity: Effects of matching participants to their treatment preferences. J. Consult. Clin. Psychol. 2001, 69, 717–721. [Google Scholar] [CrossRef] [PubMed]
- Burke, L.E.; Warziski, M.; Styn, M.A.; Music, E.; Hudson, A.G.; Sereika, S.M. A randomized clinical trial of a standard versus vegetarian diet for weight loss: The impact of treatment preference. Int. J. Obes. 2008, 32, 166–176. [Google Scholar] [CrossRef] [PubMed]
- Murray, D.C. Preferred versus nonpreferred treatment and self-control training versus determination raising as treatments of obesity: A pilot study. Psychol. Rep. 1976, 38, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Daby, R. Expressed Preference for, and Assignment to One of Two Weight Loss Programs: Effects on Weight Loss and Weight Loss Maintenance. Ph.D. Thesis, Vanderbilt University, Nashville, TN, USA, 1990. [Google Scholar]
- Coles, L.T.; Fletcher, E.A.; Galbraith, C.E.; Clifton, P.M. Patient freedom to choose a weight loss diet in the treatment of overweight and obesity: A randomized dietary intervention in type 2 diabetes and pre-diabetes. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 64. [Google Scholar] [CrossRef] [PubMed]
- Fuller, T.C. The Role of Patient Preference for Treatment Type in the Modification of Weight Loss Behavior. Ph.D. Thesis, Michigan State University, Ann Arbor, MI, USA, 1988. [Google Scholar]
- Jolly, K.; Lewis, A.; Beach, J.; Denley, J.; Adab, P.; Deeks, J.J.; Daley, A.; Aveyard, P. Comparison of range of commercial or primary care led weight reduction programmes with minimal intervention control for weight loss in obesity: Lighten up randomised controlled trial. BMJ 2011, 343, d6500. [Google Scholar] [CrossRef] [PubMed]
- Caltabiano, M.L.; Shellshear, J. Palatability versus healthiness as determinants of food preferences in young adults: A comparison of nomothetic and idiographic analytic approaches. Aust. N. Z. J. Public Health 1998, 22, 547–551. [Google Scholar] [CrossRef] [PubMed]
- Bellisle, F.; Le Magnen, J. The structure of meals in humans: Eating and drinking patterns in lean and obese subjects. Physiol. Behav. 1981, 27, 649–658. [Google Scholar] [CrossRef]
- Bellisle, F.; Lucas, F.; Amrani, R.; Le Magnen, J. Deprivation, palatability and the micro-structure of meals in human subjects. Appetite 1984, 5, 85–94. [Google Scholar] [CrossRef]
- Spiegel, T.A.; Shrager, E.E.; Stellar, E. Responses of lean and obese subjects to preloads, deprivation, and palatability. Appetite 1989, 13, 45–69. [Google Scholar] [CrossRef]
- Grossi, E.; Dalle Grave, R.; Mannucci, E.; Molinari, E.; Compare, A.; Cuzzolaro, M.; Marchesini, G. Complexity of attrition in the treatment of obesity: Clues from a structured telephone interview. Int. J. Obes. 2006, 30, 1132–1137. [Google Scholar] [CrossRef] [PubMed]
- Dalle Grave, R.; Calugi, S.; Molinari, E.; Petroni, M.L.; Bondi, M.; Compare, A.; Marchesini, G.; QUOVADIS Study Group. Weight loss expectations in obese patients and treatment attrition: An observational multicenter study. Obes. Res. 2005, 13, 1961–1969. [Google Scholar] [CrossRef] [PubMed]
- Bennett, G.A.; Jones, S.E. Dropping out of treatment for obesity. J. Psychosom. Res. 1986, 30, 567–573. [Google Scholar] [CrossRef]
- Inelmen, E.M.; Toffanello, E.D.; Enzi, G.; Gasparini, G.; Miotto, F.; Sergi, G.; Busetto, L. Predictors of drop-out in overweight and obese outpatients. Int. J. Obes. 2005, 29, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Perri, M.G.; Nezu, A.M.; Patti, E.T.; McCann, K.L. Effect of length of treatment on weight loss. J. Consult. Clin. Psychol. 1989, 57, 450–452. [Google Scholar] [CrossRef] [PubMed]
- Jeffery, R.W.; Drewnowski, A.; Epstein, L.H.; Stunkard, A.J.; Wilson, G.T.; Wing, R.R.; Hill, D.R. Long-term maintenance of weight loss: Current status. Health Psychol. 2000, 19, 5–16. [Google Scholar] [CrossRef] [PubMed]
- Lohman, T.; Wright, J. Maintenance of long-term weight loss: Future directions. Quest 2004, 56, 105–119. [Google Scholar] [CrossRef]
- Greenway, F.L.; Bray, G.A.; Marlin, R.L. Methods to maximize retention in weight loss studies. Obes. Res. 1999, 7, 593–596. [Google Scholar] [CrossRef] [PubMed]
- Swift, J.K.; Callahan, J.L. The impact of client treatment preferences on outcome: A meta-analysis. J. Clin. Psychol. 2009, 65, 368–381. [Google Scholar] [CrossRef] [PubMed]
- Cawley, S.; Farrell, S.; Byrne, D.G.; Turner, M.J.; Clune, B.; McCartney, D. Pilot evaluation of an online weight management programme. Ir. Med. J. 2017, 110, 496. [Google Scholar] [CrossRef] [PubMed]
- Williams, R.L.; Wood, L.G.; Collins, C.E.; Callister, R. Effectiveness of weight loss interventions—Is there a difference between men and women: A systematic review. Obes. Rev. 2015, 16, 171–186. [Google Scholar] [CrossRef] [PubMed]
- Robertson, C.; Avenell, A.; Boachie, C.; Stewart, F.; Archibald, D.; Douglas, F.; Hoddinott, P.; van Teijlingen, E.; Boyers, D. Should weight loss and maintenance programmes be designed differently for men? A systematic review of long-term randomised controlled trials presenting data for men and women: The ROMEO project. Obes. Res. Clin. Pract. 2016, 10, 70–84. [Google Scholar] [CrossRef] [PubMed]
- Pagoto, S.L.; Schneider, K.L.; Oleski, J.L.; Luciani, J.M.; Bodenlos, J.S.; Whited, M.C. Male inclusion in randomized controlled trials of lifestyle weight loss interventions. Obesity 2012, 20, 1234–1239. [Google Scholar] [CrossRef] [PubMed]
- Hussain, H.Y. Trends Analysis and Predictive Prevalence of Global Adult’s Obesity 2010-2016, Burden of Socio Economic Contexts. J. Publ. Health 2017, 1, 2. [Google Scholar]
- Madigan, C.D.; Roalfe, A.; Daley, A.J.; Jolly, K. What factors influence weight loss in participants of commercial weight loss programmes? Implications for health policy. Obes. Res. Clin. Pract. 2017, 11, 709–717. [Google Scholar] [CrossRef] [PubMed]
- Stubbs, R.J.; Brogelli, D.J.; Barber, J.; Pallister, C.; Whybrow, S.; Avery, A.; Lavin, J. Service evaluation of weight outcomes as a function of initial BMI in 34,271 adults referred to a primary care/commercial weight management partnership scheme. BMC Res. Notes 2013, 6, 161. [Google Scholar] [CrossRef] [PubMed]
- Binda, A.; Jaworski, P.; Kudlicka, E.; Ciesielski, A.; Cabaj, H.; Tarnowski, W. The impact of selected factors on parameters of weight loss after sleeve gastrectomy. Videosurg. Other Miniinvasive Tech. 2016, 11, 288–294. [Google Scholar] [CrossRef] [PubMed]
- Ochner, C.N.; Jochner, M.C.; Caruso, E.A.; Teixeira, J.; Xavier Pi-Sunyer, F. Effect of preoperative body mass index on weight loss following obesity surgery. Surg. Obes. Relat. Dis. 2013, 9, 423–427. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Study Design | Study Population | Start (n) | End (n) (% of Attrition) | Strategy | Option to Change Diet | Study Outcome * Mean ± Standard Deviation ** Mean (95% Confidence Interval) |
|---|---|---|---|---|---|---|---|
| Borradaile et al. [23] | RCT, over 2 years. Baseline data collected, weekly data for 20 weeks, fortnightly for week 20–40 and every other month for remainder of 2 years. | 18–65 years BMI 30–40 kg/m2 | 250 | 157 (37.2%) | Treatment preference assessed prior to, but independent of, randomization into either low-carbohydrate or low-fat diet. Preference congruent (n = 74); no strong preference (n = 98); preference incongruent (n = 78). | No | At 24 months ** Treatment congruent (a); ↓7.7 kg (↓9.3 to ↓6.1) Treatment incongruent (b); ↓9.7 kg (↓11.4 to ↓8.1) No strong preference (c); ↓11.2 kg (↓12.6 to ↓9.7) p = 0.04 (a) and (b) p = 0.0004 (a) and (c) |
| Burke et al. [26] | RCT. Initial weekly sessions for 6 months, every 2 weeks for months 7 to 9, and monthly for months 10–12. Baseline data collected and every 6 months for 18 months. | 18–55 years BMI 27–43 kg/m2 | 176 | 132 (25%) | Participants ranked their preference for a Lacto-ovo-vegetarian diet (LOV-D) or a Standard calorie- and fat-restricted diet (STD-D) on a 3-point Likert scale. Those with mild or no preference were disqualified. Participants were randomized into four groups, preference-yes STD-D (n = 48); preference-no STD-D (n = 48); preference-yes LOV-D (n = 35); preference-no LOV-D (n = 45). | No | At 18 months * Preference-yes STD-D; ↓4.8 kg ± 6.1 Preference-yes LOV-D; ↓4.8 kg ± 6.2 Preference-no STD-D; ↓7.9 kg ± 7.8 Preference-no LOV-D; ↓9.4 kg ± 8.1 p = 0.02 difference between preference-yes and preference-no |
| Coles et al. [29] | RCT, over 12 months. Baseline data collected, data obtained every 2 weeks until month 3, then every 6 weeks until 12 months, and 3, 6 and 12 month visits. | 40–75 years BMI > 27 kg/m2 | 144 | 96 (33.3%) | Participants randomized to ‘Choice’ or ‘No Choice’ groups. ‘No Choice’ group (n = 73) was placed on a set weight loss diet (CSIRO), no change permitted. ‘Choice’ group (n = 71) chose from the CSIRO (n = 34); South Beach (n = 11) or Mediterranean diet (n = 26). | Yes at any time | At 12 months * ‘No Choice’ group; ↓3.5 kg ± 4.5 kg ‘Choice’ group; ↓2.7 kg ± 5 kg p > 0.05 |
| Daby [28] 1 | RCT. Phase I; weekly group meeting for 5 weeks. Phase II; biweekly meetings for 8 weeks and then monthly for 2 months OR weekly phone call. Baseline weight, weight at group meetings, at end of phase 2 and at trial end. | 20–60 years 40%–150% above ideal body weight Females | 82 | 47 (42.7%) | All participants attended Phase I. Participants then expressed preference for ‘Group’ based or ‘Telephone’ based interventions. Participants were randomized into two groups independent of preference. Four groups resulted, group-yes (n = 24); group-no (n = 23); telephone-yes (n = 10); telephone-no (n = 11). | No | At 33 weeks * Group-yes; ↓15.1 lbs ± 19.3 (6.8 kg ± 9) Group-no; ↓9.7 lbs ± 16.7 (4.4 kg ± 7.6) Telephone-yes; ↓7.6 lbs ± 11.8 (3.4 kg ± 5.4) Telephone-no; ↓9.86 ± 20.2 (4.5 kg ± 9.1) p > 0.05 |
| Fuller [30] 2 | RCT over 10 weeks. Baseline weight was obtained and weekly weights thereafter. | 24–65 years Overweight | 118 | 73 (38.1%) | Participants randomized to ‘Choice’ or ‘No Choice’ groups. ‘Choice’ group chose between nutrition education (n = 11), behaviour management (n = 22) or exercise (n = 19) for weight loss. ‘No Choice’ were randomly assigned to nutrition education (n = 15); behaviour management (n = 15) or exercise (n = 13) for weight loss. | No | At 10 weeks ‘Choice’ group; ↓4.5 lbs (2 kg) ‘No Choice’ group; ↓7.4 lbs (3.4 kg) p = 0.026 |
| Jolly et al. [31] | RCT over 12 weeks. Baseline data was collected during week 1 and again at 3 months. | ≥18 years BMI ≥ 30 kg/m2 with no obesity related comorbidities or ≥25 kg/m2 if South Asian BMI ≥ 28 kg/m2 with obesity related comorbidities or ≥23 kg/m2 if South Asian. | 740 | 658 (11.1%) | Participants were randomized to; Weight Watchers (n = 100); Slimming World (n = 100); Rosemary Conley (n = 100); group based, dietetics led program (n = 100); general practice one to one counselling (n = 70); pharmacy led one on one counselling (n = 70); choice of any of the six programs (n = 100) or a comparator group provided with 12 vouchers for a local fitness center. | No | At 3 months ** WW ↓5.2 kg (↓4.2 to ↓6.1) SW ↓4.3 kg (↓3.3 to ↓ 5.2) RC ↓5.3 kg (↓4.2 to ↓6.4) SD ↓3.2 kg (↓2.3 to ↓4.1) GP ↓2.2 kg (↓0.7 to ↓3.7) P ↓2.8 kg (↓1.4 to ↓4.2) Choice ↓3.8 kg (↓2.9 to ↓4.7) Control ↓3 kg (↓1.8 to ↓4.1) p > 0.05 difference between ‘Choice’ and ‘No Choice’ groups |
| Murray et al. [27] | RCT, over 6 months. Baseline data and weekly data was collected for 9 weeks followed by a 3 month and 6 month data collection. | ≥21 years >165 lbs (74.8 kg) Females | 12 | 9 (25%) | Participants indicated their treatment preference. Patients were independently assigned to follow the self-control method (n = 6) or determination raising (n = 6) method by chance. | No | At 6 month follow-up Preference-yes group; ↓2.8 lbs (1.3 kg) Preference-no group; ↓6.5 lbs (3 kg) p > 0.05 |
| Renjilian et al. [25] | RCT trial over 26 weeks. Baseline data was obtained, and the weekly data collected for 26 weeks. | 21–59 years BMI 28–45 kg/m2 | 75 | 58 (22.7%) | Participants indicated preference for Individual vs. Group therapy using a 6-point Likert scale, those who had a ‘slight’ preference were excluded from the study. Participants were randomized to one of the two groups. Four groups resulted; Preference-yes group (n = 16); preference-yes individual (n = 13); preference-no group (n = 14); preference-no individual (n = 15). | No | At 26 weeks * Preference-yes group ↓10.9 kg ± 4.06 Preference-no group ↓11.2 kg ± 5.6 Preference-yes individual ↓8.48 kg ± 3 Preference-no individual ↓9.61 kg ± 4.17 p > 0.05 |
| Yancy et al. [24] | Doubly randomised, preference trial over 48 weeks. Baseline data was obtained, every 2 weeks for 24 weeks, then every 4 weeks for 24 weeks. | <75 years BMI ≥ 30 kg/m2 * Participants were veterans | 207 | 175 (15.5%) | Participants completed a food preference questionnaire. Participants were randomized to a ‘Choice’ or ‘No Choice’ arm. The ‘Choice’ group received information about their food preferences in relation to 2 diet options-low carbohydrate (n = 61) or low-fat (n = 44), before choosing one. The ‘No Choice’ group were randomly assigned to the low-carbohydrate (n = 53) or low–fat (n = 49) diet. | At week 12 | At 48 weeks ** ‘Choice’ arm ↓5.7 kg (↓4.3 to ↓7) ‘No Choice’ arm ↓6.7 kg (↓5.4 to ↓8) Mean difference ↓1.1 kg (↓2.9 to ↓0.8) between groups p = 0.26 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leavy, J.M.; Clifton, P.M.; Keogh, J.B. The Role of Choice in Weight Loss Strategies: A Systematic Review and Meta-Analysis. Nutrients 2018, 10, 1136. https://doi.org/10.3390/nu10091136
Leavy JM, Clifton PM, Keogh JB. The Role of Choice in Weight Loss Strategies: A Systematic Review and Meta-Analysis. Nutrients. 2018; 10(9):1136. https://doi.org/10.3390/nu10091136
Chicago/Turabian StyleLeavy, Jill M., Peter M. Clifton, and Jennifer B. Keogh. 2018. "The Role of Choice in Weight Loss Strategies: A Systematic Review and Meta-Analysis" Nutrients 10, no. 9: 1136. https://doi.org/10.3390/nu10091136
APA StyleLeavy, J. M., Clifton, P. M., & Keogh, J. B. (2018). The Role of Choice in Weight Loss Strategies: A Systematic Review and Meta-Analysis. Nutrients, 10(9), 1136. https://doi.org/10.3390/nu10091136