Thirteen-Year Trends in Dietary Patterns among Japanese Adults in the National Health and Nutrition Survey 2003–2015: Continuous Westernization of the Japanese Diet



Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source and Analytic Sample
2.2. Dietary Assessment
2.3. Identification of Dietary Patterns
2.4. Assessment of Basic Characteristics
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Analytic Sample
3.2. Dietary Patterns
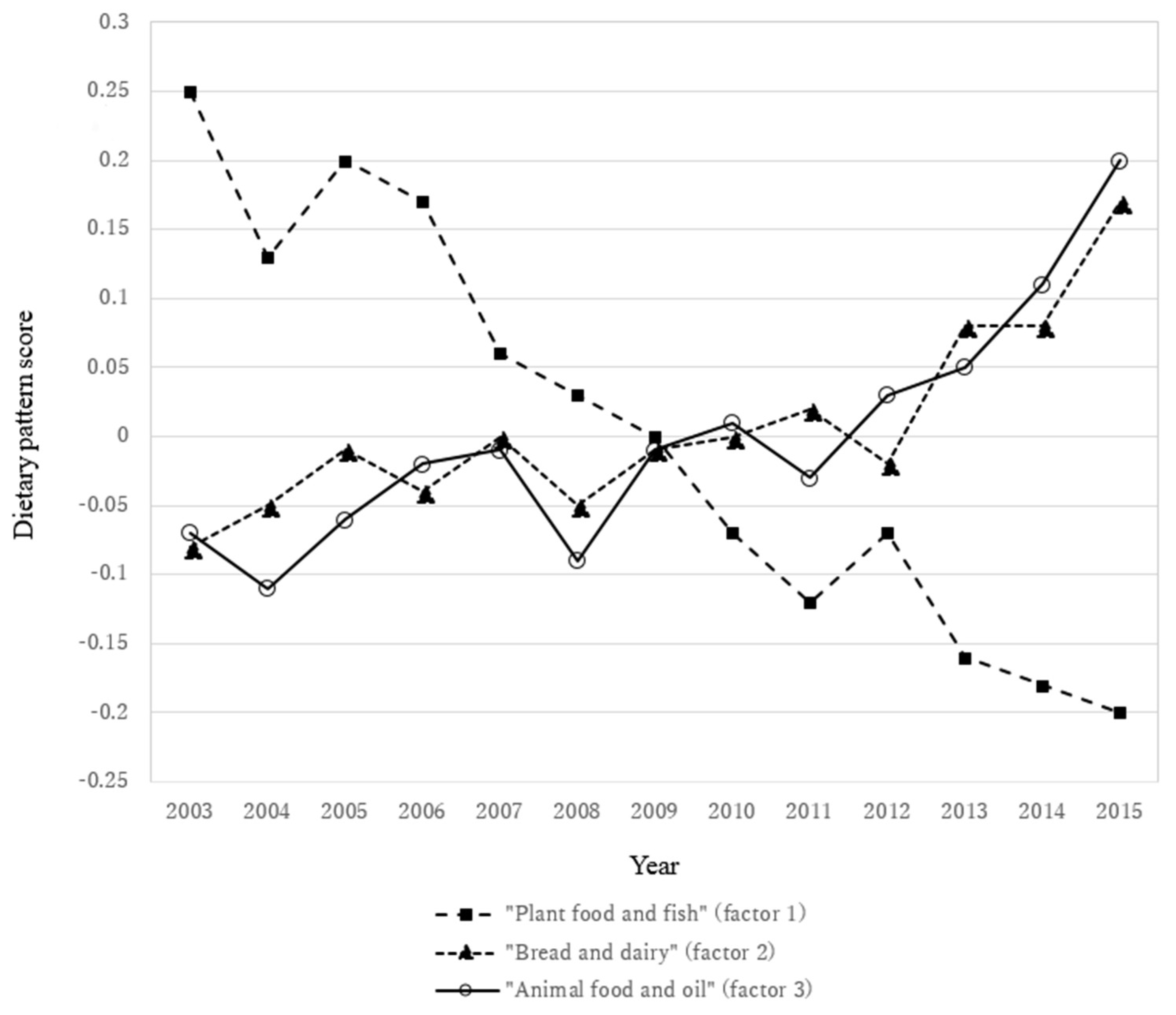
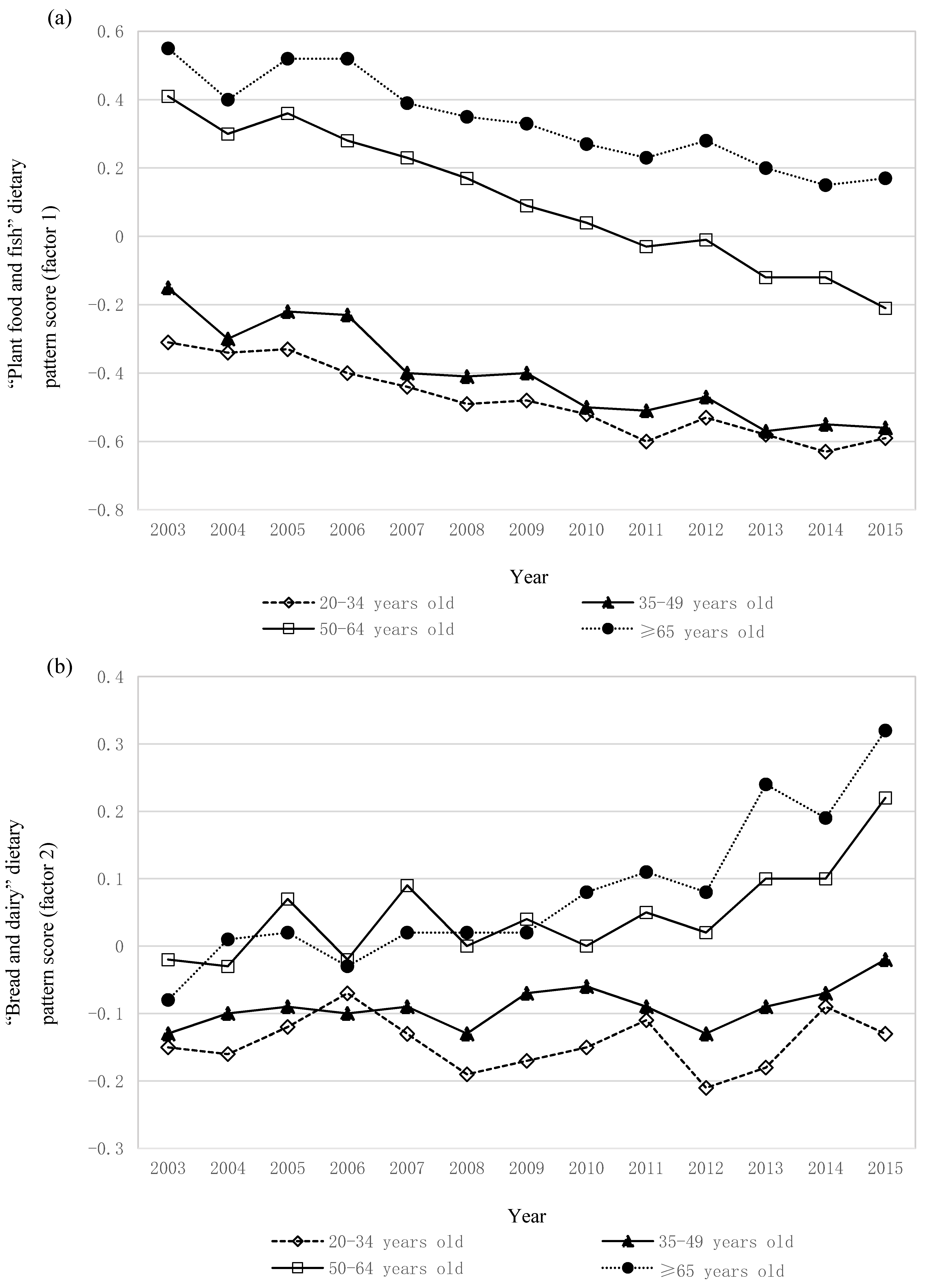
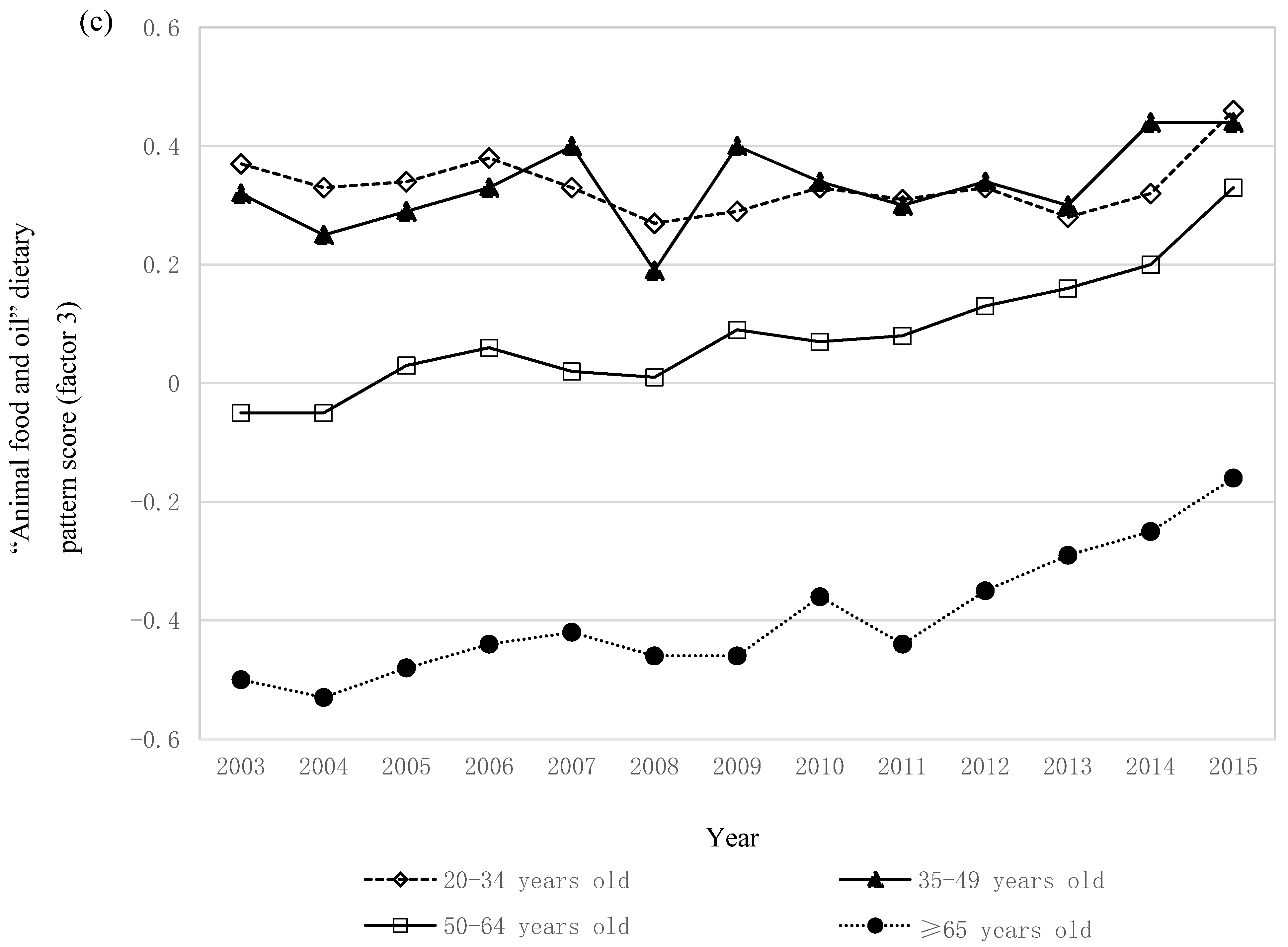
3.3. Trends in Dietary Patterns
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Rehm, C.D.; Penalvo, J.L.; Afshin, A.; Mozaffarian, D. Dietary intake among US adults, 1999–2012. JAMA 2016, 315, 2542–2553. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Kant, A.K. Dietary patterns and health outcomes. J. Am. Diet. Assoc. 2004, 104, 615–635. [Google Scholar] [CrossRef] [PubMed]
- Newby, P.K.; Tucker, K.L. Empirically derived eating patterns using factor or cluster analysis: A review. Nutr. Rev. 2004, 62, 177–203. [Google Scholar] [CrossRef] [PubMed]
- Ax, E.; Warensjo Lemming, E.; Becker, W.; Andersson, A.; Lindroos, A.K.; Cederholm, T.; Sjogren, P.; Fung, T.T. Dietary patterns in Swedish adults; results from a national dietary survey. Br. J. Nutr. 2016, 115, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Beck, K.L.; Jones, B.; Ullah, I.; McNaughton, S.A.; Haslett, S.J.; Stonehouse, W. Associations between dietary patterns, socio-demographic factors and anthropometric measurements in adult New Zealanders: An analysis of data from the 2008/09 New Zealand Adult Nutrition Survey. Eur. J. Nutr. 2018, 57, 1421–1433. [Google Scholar] [CrossRef] [PubMed]
- Bell, L.K.; Edwards, S.; Grieger, J.A. The relationship between dietary patterns and metabolic health in a representative sample of adult Australians. Nutrients 2015, 7, 6491–6505. [Google Scholar] [CrossRef] [PubMed]
- Heidemann, C.; Scheidt-Nave, C.; Richter, A.; Mensink, G.B.M. Dietary patterns are associated with cardiometabolic risk factors in a representative study population of German adults. Br. J. Nutr. 2011, 106, 1253–1262. [Google Scholar] [CrossRef] [PubMed]
- Hearty, A.P.; Gibney, M.J. Comparison of cluster and principal component analysis techniques to derive dietary patterns in Irish adults. Br. J. Nutr. 2009, 101, 598–608. [Google Scholar] [CrossRef] [PubMed]
- Kerver, J.M.; Yang, E.J.; Obayashi, S.; Bianchi, L.; Song, W.O. Meal and snack patterns are associated with dietary intake of energy and nutrients in US adults. J. Am. Diet. Assoc. 2006, 106, 46–53. [Google Scholar] [CrossRef] [PubMed]
- Gibson, S.; Ashwell, M. Dietary patterns among British adults: Comparability with dietary guidelines for salt/sodium, fat, saturated fat and sugars. Public Health Nutr. 2011, 14, 1323–1336. [Google Scholar] [CrossRef] [PubMed]
- Bertin, M.; Touvier, M.; Dubuisson, C.; Dufour, A.; Havard, S.; Lafay, L.; Volatier, J.L.; Lioret, S. Dietary patterns of French adults: Associations with demographic, socio-economic and behavioural factors. J. Hum. Nutr. Diet. 2016, 29, 241–254. [Google Scholar] [CrossRef] [PubMed]
- Knudsen, V.K.; Matthiessen, J.; Biltoft-Jensen, A.; Sorensen, M.R.; Groth, M.V.; Trolle, E.; Christensen, T.; Fagt, S. Identifying dietary patterns and associated health-related lifestyle factors in the adult Danish population. Eur. J. Clin. Nutr. 2014, 68, 736–740. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; He, Y.; Li, Y.; Luan, D.; Yang, X.; Zhai, F.; Ma, G. Dietary patterns and hypertension among Chinese adults: A nationally representative cross-sectional study. BMC Public Health 2011, 11, 925. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.Y.; Kim, J.M.; Kim, Y. Associations between dietary patterns and hypertension among Korean adults: The Korean National Health and Nutrition Examination Survey (2008–2010). Nutr. Res. Pract. 2013, 7, 224–232. [Google Scholar] [CrossRef] [PubMed]
- Htun, N.C.; Suga, H.; Imai, S.; Shimizu, W.; Takimoto, H. Food intake patterns and cardiovascular risk factors in Japanese adults: Analyses from the 2012 National Health and nutrition survey, Japan. Nutr. J. 2017, 16, 61. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, S. The value of the National Health and Nutrition Survey in Japan. Lancet 2011, 378, 1205–1206. [Google Scholar] [CrossRef]
- Ikeda, N.; Saito, E.; Kondo, N.; Inoue, M.; Ikeda, S.; Satoh, T.; Wada, K.; Stickley, A.; Katanoda, K.; Mizoue, T.; et al. What has made the population of Japan healthy? Lancet 2011, 378, 1094–1105. [Google Scholar] [CrossRef]
- Micha, R.; Khatibzadeh, S.; Shi, P.; Andrews, K.G.; Engell, R.E.; Mozaffarian, D. Global, regional and national consumption of major food groups in 1990 and 2010: A systematic analysis including 266 country-specific nutrition surveys worldwide. BMJ Open 2015, 5, e008705. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour and Welfare, Japan. The National Health and Nutrition Survey, Japan. Available online: http://www.mhlw.go.jp/bunya/kenkou/kenkou_eiyou_chousa.html (accessed on 25 July 2018). (In Japanese)
- Okubo, H.; Murakami, K.; Sasaki, S.; Kim, M.K.; Hirota, N.; Notsu, A.; Fukui, M.; Date, C. Relative validity of dietary patterns derived from a self-administered diet history questionnaire using factor analysis among Japanese adults. Public Health Nutr. 2010, 13, 1080–1089. [Google Scholar] [CrossRef] [PubMed]
- Shimazu, T.; Kuriyama, S.; Hozawa, A.; Ohmori, K.; Sato, Y.; Nakaya, N.; Nishino, Y.; Tsubono, Y.; Tsuji, I. Dietary patterns and cardiovascular disease mortality in Japan: A prospective cohort study. Int. J. Epidemiol. 2007, 36, 600–609. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, A.; Asakura, K.; Uechi, K.; Masayasu, S.; Sasaki, S. Dietary patterns extracted from the current Japanese diet and their associations with sodium and potassium intakes estimated by repeated 24 h urine collection. Public Health Nutr. 2016, 19, 2580–2591. [Google Scholar] [CrossRef] [PubMed]
- Maruyama, K.; Iso, H.; Date, C.; Kikuchi, S.; Watanabe, Y.; Wada, Y.; Inaba, Y.; Tamakoshi, A. Dietary patterns and risk of cardiovascular deaths among middle-aged Japanese: JACC Study. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 519–527. [Google Scholar] [CrossRef] [PubMed]
- Akter, S.; Nanri, A.; Pham, N.M.; Kurotani, K.; Mizoue, T. Dietary patterns and metabolic syndrome in a Japanese working population. Nutr. Metab. 2013, 10, 30. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.K.; Sasaki, S.; Sasazuki, S.; Tsugane, S. Prospective study of three major dietary patterns and risk of gastric cancer in Japan. Int. J. Cancer 2004, 110, 435–442. [Google Scholar] [CrossRef] [PubMed]
- Monma, Y.; Niu, K.; Iwasaki, K.; Tomita, N.; Nakaya, N.; Hozawa, A.; Kuriyama, S.; Takayama, S.; Seki, T.; Takeda, T.; et al. Dietary patterns associated with fall-related fracture in elderly Japanese: A population based prospective study. BMC Geriatr. 2010, 10, 31. [Google Scholar] [CrossRef] [PubMed]
- Okubo, H.; Inagaki, H.; Gondo, Y.; Kamide, K.; Ikebe, K.; Masui, Y.; Arai, Y.; Ishizaki, T.; Sasaki, S.; Nakagawa, T.; et al. Association between dietary patterns and cognitive function among 70-year-old Japanese elderly: A cross-sectional analysis of the SONIC study. Nutr. J. 2017, 16, 56. [Google Scholar] [CrossRef] [PubMed]
- Okubo, H.; Sasaki, S.; Horiguchi, H.; Oguma, E.; Miyamoto, K.; Hosoi, Y.; Kim, M.K.; Kayama, F. Dietary patterns associated with bone mineral density in premenopausal Japanese farmwomen. Am. J. Clin. Nutr. 2006, 83, 1185–1192. [Google Scholar] [CrossRef] [PubMed]
- Okubo, H.; Sasaki, S.; Murakami, K.; Kim, M.K.; Takahashi, Y.; Hosoi, Y.; Itabashi, M. Three major dietary patterns are all independently related to the risk of obesity among 3760 Japanese women aged 18–20 years. Int. J. Obes. 2008, 32, 541–549. [Google Scholar] [CrossRef] [PubMed]
- Tada, N.; Maruyama, C.; Koba, S.; Tanaka, H.; Birou, S.; Teramoto, T.; Sasaki, J. Japanese dietary lifestyle and cardiovascular disease. J. Atheroscler. Thromb. 2011, 18, 723–734. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, N.; Takimoto, H.; Imai, S.; Miyachi, M.; Nishi, N. Data resource profile: The Japan National Health and Nutrition Survey (NHNS). Int. J. Epidemiol. 2015, 44, 1842–1849. [Google Scholar] [CrossRef] [PubMed]
- Murakami, K.; Livingstone, M.B.; Okubo, H.; Sasaki, S. Energy density of the diets of Japanese adults in relation to food and nutrient intake and general and abdominal obesity: A cross-sectional analysis from the 2012 National Health and Nutrition Survey, Japan. Br. J. Nutr. 2017, 117, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Murakami, K.; Livingstone, M.B.E.; Sasaki, S. Establishment of a meal coding system for the characterization of meal-based dietary patterns in Japan. J. Nutr. 2017, 147, 2093–2101. [Google Scholar] [CrossRef] [PubMed]
- Council for Science and Technology. Standard Tables of Food Composition in Japan, Fifth Revised and Enlarged Edition; National Printing Bureau: Tokyo, Japan, 2005. (In Japanese)
- Iwaoka, F.; Yoshiike, N.; Date, C.; Shimada, T.; Tanaka, H. A validation study on a method to estimate nutrient intake by family members through a household-based food-weighing survey. J. Nutr. Sci. Vitaminol. 2001, 47, 222–227. [Google Scholar] [CrossRef] [PubMed]
- Murakami, K.; Livingstone, M.B.E.; Okubo, H.; Sasaki, S. Younger and older ages and obesity are associated with energy intake underreporting but not overreporting in Japanese boys and girls aged 1–19 years: The National Health and Nutrition Survey. Nutr. Res. 2016, 36, 1153–1161. [Google Scholar] [CrossRef] [PubMed]
- Murakami, K.; Livingstone, M.B.E.; Okubo, H.; Sasaki, S. Prevalence and characteristics of misreporting of energy intake in Japanese adults: The 2012 National Health and Nutrition Survey. Asia Pac. J. Clin. Nutr. 2018, 27, 441–450. [Google Scholar] [CrossRef] [PubMed]
- Varraso, R.; Garcia-Aymerich, J.; Monier, F.; Le Moual, N.; De Batlle, J.; Miranda, G.; Pison, C.; Romieu, I.; Kauffmann, F.; Maccario, J. Assessment of dietary patterns in nutritional epidemiology: Principal component analysis compared with confirmatory factor analysis. Am. J. Clin. Nutr. 2012, 96, 1079–1092. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Western Pacific Region. International Association for the Study of Obesity Task Force. In The Asia-Pacific Perspective: Redefining Obesity and Its Treatment; Health Communications Australia: Sydney, Australia, 2000; pp. 15–21. [Google Scholar]
- Murakami, K.; Livingstone, M.B.E.; Sasaki, S. Diet quality scores in relation to metabolic risk factors in Japanese adults: A cross-sectional analysis from the 2012 National Health and Nutrition Survey, Japan. Eur. J. Nutr. 2018. [Google Scholar] [CrossRef] [PubMed]
- Okubo, H.; Sasaki, S.; Murakami, K.; Yokoyama, T.; Hirota, N.; Notsu, A.; Fukui, M.; Date, C. Designing optimal food intake patterns to achieve nutritional goals for Japanese adults through the use of linear programming optimization models. Nutr. J. 2015, 14, 57. [Google Scholar] [CrossRef] [PubMed]
- Kondo, I.; Ojima, T.; Nakamura, M.; Hayasaka, S.; Hozawa, A.; Saitoh, S.; Ohnishi, H.; Akasaka, H.; Hayakawa, T.; Murakami, Y.; et al. Consumption of Dairy Products and Death from Cardiovascular Disease in the Japanese General Population: The NIPPON DATA80. J. Epidemiol. 2013, 23, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Asakura, K.; Uechi, K.; Masayasu, S.; Sasaki, S. Sodium sources in the Japanese diet: Difference between generations and sexes. Public Health Nutr. 2016, 19, 2011–2023. [Google Scholar] [CrossRef] [PubMed]
- Takimoto, H.; Saito, A.; Htun, N.C.; Abe, K. Food items contributing to high dietary salt intake among Japanese adults in the 2012 National Health and Nutrition Survey. Hypertens. Res. 2018, 41, 209–212. [Google Scholar] [CrossRef] [PubMed]
- Marques-Vidal, P.; Gaspoz, J.M.; Theler, J.M.; Guessous, I. Twenty-year trends in dietary patterns in French-speaking Switzerland: Toward healthier eating. Am. J. Clin. Nutr. 2017, 106, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Livingstone, M.B.; Black, A.E. Markers of the validity of reported energy intake. J. Nutr. 2003, 133, 895S–920S. [Google Scholar] [CrossRef] [PubMed]
- Murakami, K.; Livingstone, M.B. Prevalence and characteristics of misreporting of energy intake in US adults: NHANES 2003–2012. Br. J. Nutr. 2015, 114, 1294–1303. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, S.; Takahashi, T.; Iitoi, Y.; Iwase, Y.; Kobayashi, M.; Ishihara, J.; Akabane, M.; Tsugane, S. Food and nutrient intakes assessed with dietary records for the validation study of a self-administered food frequency questionnaire in JPHC Study Cohort I. J. Epidemiol. 2003, 13, S23–S50. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, K.; Hoshino, Y.; Kodama, K.; Yamamoto, M. Reliability of self-reported body height and weight of adult Japanese women. J. Biosoc. Sci. 1999, 31, 555–558. [Google Scholar] [CrossRef] [PubMed]
- Wada, K.; Tamakoshi, K.; Tsunekawa, T.; Otsuka, R.; Zhang, H.; Murata, C.; Nagasawa, N.; Matsushita, K.; Sugiura, K.; Yatsuya, H.; et al. Validity of self-reported height and weight in a Japanese workplace population. Int. J. Obes. Relat. Metab. Disord. 2005, 29, 1093–1099. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Health and Nutrition. The Current Status of National Nutrition. Available online: http://www.nibiohn.go.jp/eiken/chosa/kokumin_eiyou/ (accessed on 25 July 2018). (In Japanese)





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | p for Trend b | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | ||
| Sample size | 7062 | 5675 | 5469 | 6062 | 5954 | 6198 | 6047 | 5581 | 5197 | 19,717 | 5393 | 5298 | 4874 | |
| Sex, n (%) | 0.30 | |||||||||||||
| Male | 3129 (44.3) | 2517 (44.4) | 2434 (44.5) | 2706 (44.6) | 2682 (45.1) | 2775 (44.8) | 2702 (44.7) | 2488 (44.6) | 2330 (44.8) | 8712 (44.2) | 2469 (45.8) | 2425 (45.8) | 2188 (44.9) | |
| Female | 3933 (55.7) | 3158 (55.7) | 3035 (55.5) | 3356 (55.4) | 3272 (55.0) | 3423 (55.2) | 3345 (55.3) | 3093 (55.4) | 2867 (55.2) | 11,005 (55.8) | 2924 (54.2) | 2873 (54.2) | 2686 (55.1) | |
| Age category, n (%) | <0.0001 | |||||||||||||
| 20–34 years | 1117 (15.8) | 919 (16.2) | 806 (14.7) | 921 (15.2) | 792 (13.3) | 750 (12.1) | 747 (12.4) | 659 (11.8) | 604 (11.6) | 2111 (10.7) | 579 (10.7) | 516 (9.7) | 462 (9.5) | |
| 35–49 years | 1630 (23.1) | 1254 (22.1) | 1175 (21.5) | 1346 (22.2) | 1449 (24.3) | 1271 (20.5) | 1414 (23.4) | 1278 (22.9) | 1181 (22.7) | 4341 (22.0) | 1211 (22.5) | 1079 (20.4) | 1098 (22.5) | |
| 50–64 years | 2117 (30.0) | 1798 (31.7) | 1626 (29.7) | 1827 (30.1) | 1768 (29.7) | 1889 (30.5) | 1764 (29.2) | 1611 (28.9) | 1492 (28.7) | 5685 (28.8) | 1389 (25.8) | 1460 (27.6) | 1306 (26.8) | |
| ≥65 years | 2198 (31.1) | 1704 (30.0) | 1862 (34.1) | 1968 (32.5) | 1945 (32.7) | 2288 (36.9) | 2122 (35.1) | 2033 (36.4) | 1920 (36.9) | 7580 (38.4) | 2214 (41.1) | 2243 (42.3) | 2008 (41.2) | |
| Occupation, n (%) | <0.0001 | |||||||||||||
| Professional/manager | 1019 (14.4) | 872 (15.4) | 878 (16.1) | 838 (13.8) | 994 (16.7) | 895 (14.4) | 912 (15.1) | 831 (14.9) | 772 (14.9) | 2745 (13.9) | 828 (15.4) | 726 (13.7) | 772 (15.8) | |
| Sales/service/clerical | 1701 (24.1) | 1386 (24.4) | 1385 (25.3) | 1490 (24.6) | 1451 (24.4) | 1392 (22.5) | 1462 (24.2) | 1402 (25.1) | 1262 (24.3) | 4838 (24.5) | 1330 (24.7) | 1261 (23.8) | 1195 (24.5) | |
| Security/transportation/labor | 1585 (22.4) | 1133 (20.0) | 1053 (19.3) | 1330 (21.9) | 1121 (18.8) | 1255 (20.3) | 1217 (20.1) | 960 (17.2) | 924 (17.8) | 3844 (19.5) | 833 (15.5) | 934 (17.6) | 768 (15.8) | |
| Nonworker | 2757 (39.0) | 2284 (40.3) | 2153 (39.4) | 2404 (39.7) | 2388 (40.1) | 2656 (42.9) | 2456 (40.6) | 2388 (42.8) | 2239 (43.1) | 8290 (42.0) | 2402 (44.5) | 2377 (44.9) | 2139 (43.9) | |
| Body mass index, kg/m2 | 23.0 ± 3.5 | 22.9 ± 3.4 | 23.1 ± 3.5 | 23.0 ± 3.4 | 23.0 ± 3.6 | 23.0 ± 3.4 | 23.0 ± 3.6 | 23.0 ± 3.5 | 23.0 ± 3.5 | 23.0 ± 3.5 | 22.9 ± 3.6 | 23.0 ± 3.5 | 23.0 ± 3.6 | 0.74 |
| Weight status, n (%) c | 0.45 | |||||||||||||
| Underweight | 533 (7.6) | 424 (7.5) | 389 (7.1) | 418 (6.9) | 447 (7.5) | 469 (7.6) | 468 (7.7) | 441 (7.9) | 413 (8.0) | 1498 (7.6) | 467 (8.7) | 404 (7.6) | 372 (7.6) | |
| Normal weight | 4746 (67.2) | 3848 (67.8) | 3695 (67.6) | 4115 (67.9) | 4011 (67.4) | 4220 (68.1) | 4043 (66.9) | 3701 (66.3) | 3477 (66.9) | 13,250 (67.2) | 3613 (67.0) | 3572 (67.4) | 3320 (68.1) | |
| Overweight | 1783 (25.3) | 1403 (24.7) | 1385 (25.3) | 1529 (25.2) | 1496 (25.1) | 1509 (24.4) | 1536 (25.4) | 1439 (25.8) | 1307 (25.2) | 4969 (25.2) | 1313 (24.4) | 1322 (25.0) | 1182 (24.3) | |
| Current smoking, n (%) | <0.0001 | |||||||||||||
| No | 5134 (72.7) | 4212 (74.2) | 4176 (76.4) | 4629 (76.4) | 4512 (75.8) | 4864 (78.5) | 4650 (76.9) | 4517 (80.9) | 4207 (81.0) | 16,135 (81.8) | 4385 (81.3) | 4308 (81.3) | 4059 (83.3) | |
| Yes | 1928 (27.3) | 1463 (25.8) | 1293 (23.6) | 1433 (23.6) | 1442 (24.2) | 1334 (21.5) | 1397 (23.1) | 1064 (19.1) | 990 (19.1) | 3582 (18.2) | 1008 (18.7) | 990 (18.7) | 815 (16.7) | |
| Factor 1 “Plant Food and Fish” Pattern | Factor 2 “Bread and Dairy” Pattern | Factor 3 “Animal Food and Oil” Pattern | |
|---|---|---|---|
| Rice | 0.34 | −0.55 | 0.16 |
| Bread | −0.19 | 0.64 | 0.16 |
| Noodles | −0.21 | 0.04 | 0.02 |
| Other grains | 0.00 | 0.06 | 0.25 |
| Potatoes | 0.36 | 0.00 | 0.16 |
| Sugar | 0.33 | 0.34 | 0.09 |
| Pulses | 0.41 | −0.03 | −0.07 |
| Nuts | 0.18 | 0.17 | −0.03 |
| Green and yellow vegetables | 0.50 | 0.19 | 0.07 |
| Other vegetables | 0.48 | 0.01 | 0.33 |
| Vegetable and fruit juice | −0.03 | 0.15 | 0.04 |
| Pickled vegetables | 0.30 | −0.14 | −0.09 |
| Fruit | 0.43 | 0.40 | −0.22 |
| Mushrooms | 0.30 | 0.04 | 0.08 |
| Seaweeds | 0.30 | −0.01 | −0.04 |
| Fish | 0.31 | −0.04 | −0.15 |
| Shellfish | 0.08 | −0.06 | 0.17 |
| Sea products | 0.27 | −0.12 | −0.04 |
| Red meat | 0.02 | −0.10 | 0.48 |
| Processed meat | −0.09 | 0.12 | 0.37 |
| Chicken | −0.01 | −0.05 | 0.24 |
| Eggs | 0.12 | −0.03 | 0.39 |
| Dairy products | 0.15 | 0.54 | −0.08 |
| Animal fat | −0.09 | 0.29 | 0.25 |
| Vegetable oil | 0.00 | 0.11 | 0.64 |
| Confectioneries | −0.01 | 0.23 | −0.08 |
| Alcoholic beverages | −0.03 | −0.24 | 0.28 |
| Tea | 0.34 | 0.05 | −0.22 |
| Coffee | −0.12 | 0.23 | 0.28 |
| Soft drinks | −0.12 | 0.00 | 0.21 |
| Salt-based seasonings | 0.60 | −0.22 | 0.16 |
| Variability explained (%) | 7.43 | 5.64 | 5.57 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murakami, K.; Livingstone, M.B.E.; Sasaki, S. Thirteen-Year Trends in Dietary Patterns among Japanese Adults in the National Health and Nutrition Survey 2003–2015: Continuous Westernization of the Japanese Diet. Nutrients 2018, 10, 994. https://doi.org/10.3390/nu10080994
Murakami K, Livingstone MBE, Sasaki S. Thirteen-Year Trends in Dietary Patterns among Japanese Adults in the National Health and Nutrition Survey 2003–2015: Continuous Westernization of the Japanese Diet. Nutrients. 2018; 10(8):994. https://doi.org/10.3390/nu10080994
Chicago/Turabian StyleMurakami, Kentaro, M. Barbara E. Livingstone, and Satoshi Sasaki. 2018. "Thirteen-Year Trends in Dietary Patterns among Japanese Adults in the National Health and Nutrition Survey 2003–2015: Continuous Westernization of the Japanese Diet" Nutrients 10, no. 8: 994. https://doi.org/10.3390/nu10080994
APA StyleMurakami, K., Livingstone, M. B. E., & Sasaki, S. (2018). Thirteen-Year Trends in Dietary Patterns among Japanese Adults in the National Health and Nutrition Survey 2003–2015: Continuous Westernization of the Japanese Diet. Nutrients, 10(8), 994. https://doi.org/10.3390/nu10080994