Calcium and Phosphate Metabolism, Blood Lipids and Intestinal Sterols in Human Intervention Studies Using Different Sources of Phosphate as Supplements—Pooled Results and Literature Search


Abstract
1. Introduction
2. Materials and Methods
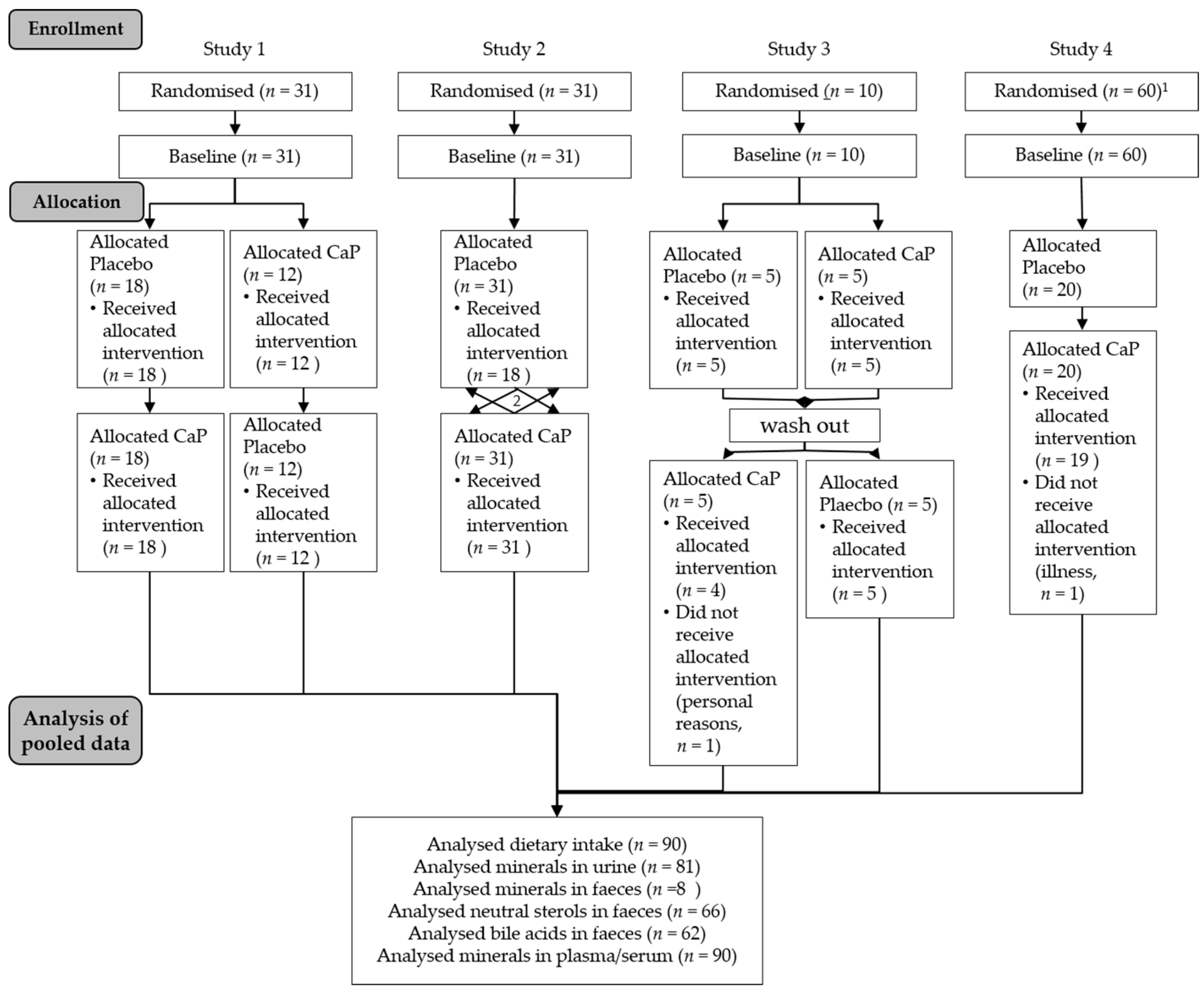
2.1. Study Design and Subjects
2.2. Supplement
2.3. Sample Preparation
2.4. Food Analysis
2.5. Blood Analysis
2.6. Faecal and Urine Analysis
2.7. Absorption and Balance of Calcium and Phosphorus
2.8. Statistics
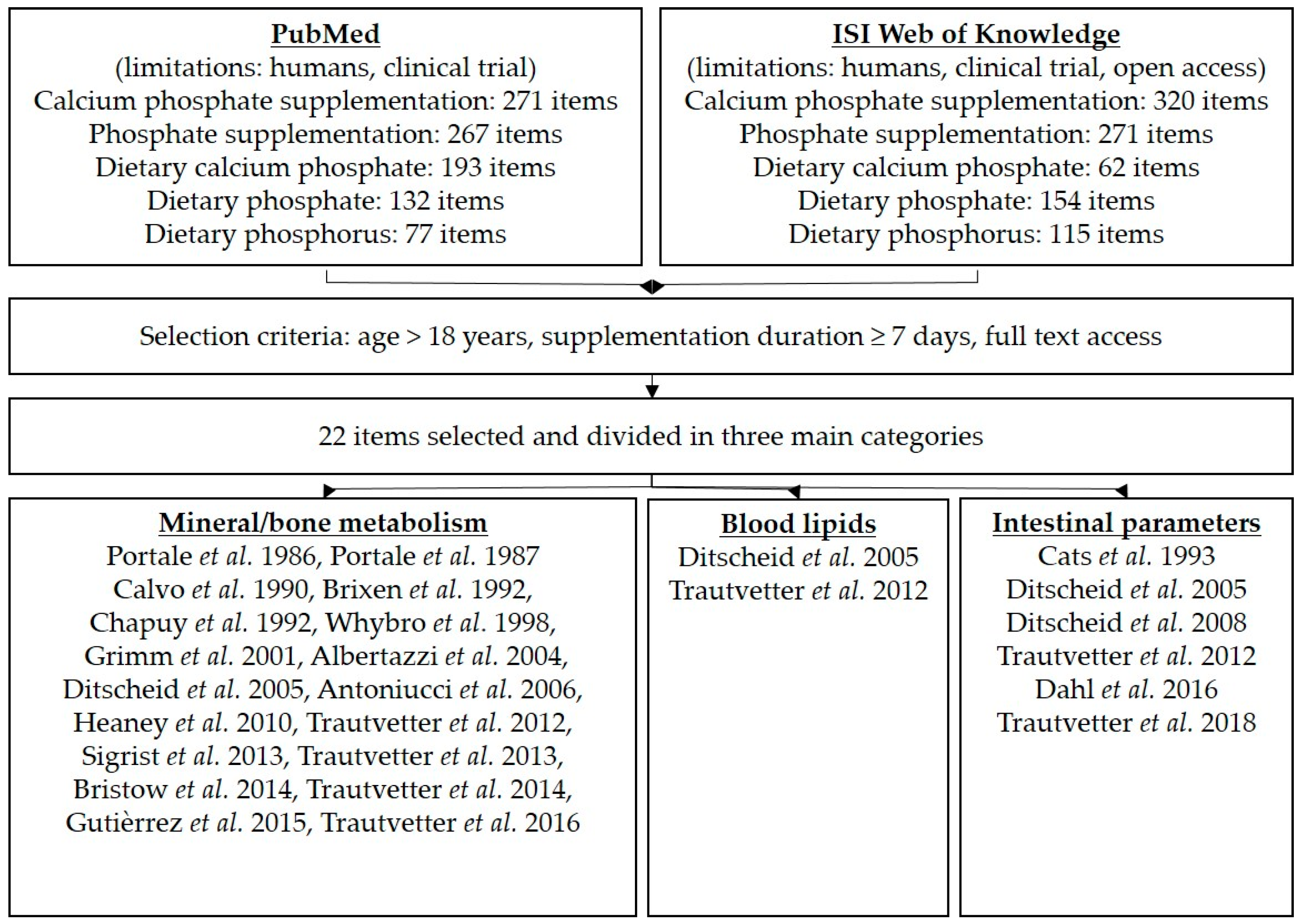
2.9. Literature Search
3. Results
3.1. Results of the Pooled Study
3.1.1. Dietary Intake of Macronutrients and Minerals
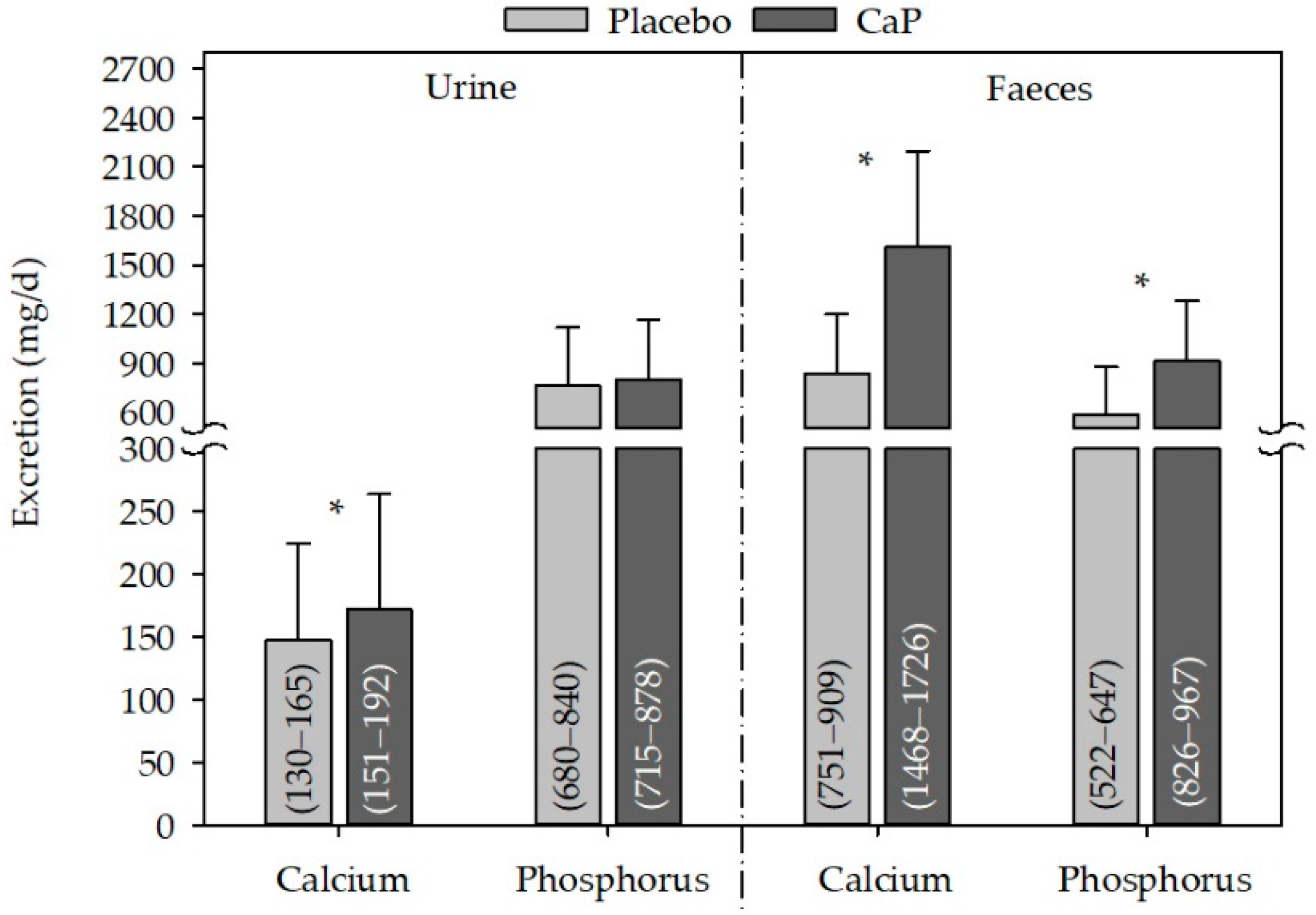
3.1.2. Minerals
3.1.3. Blood Lipids
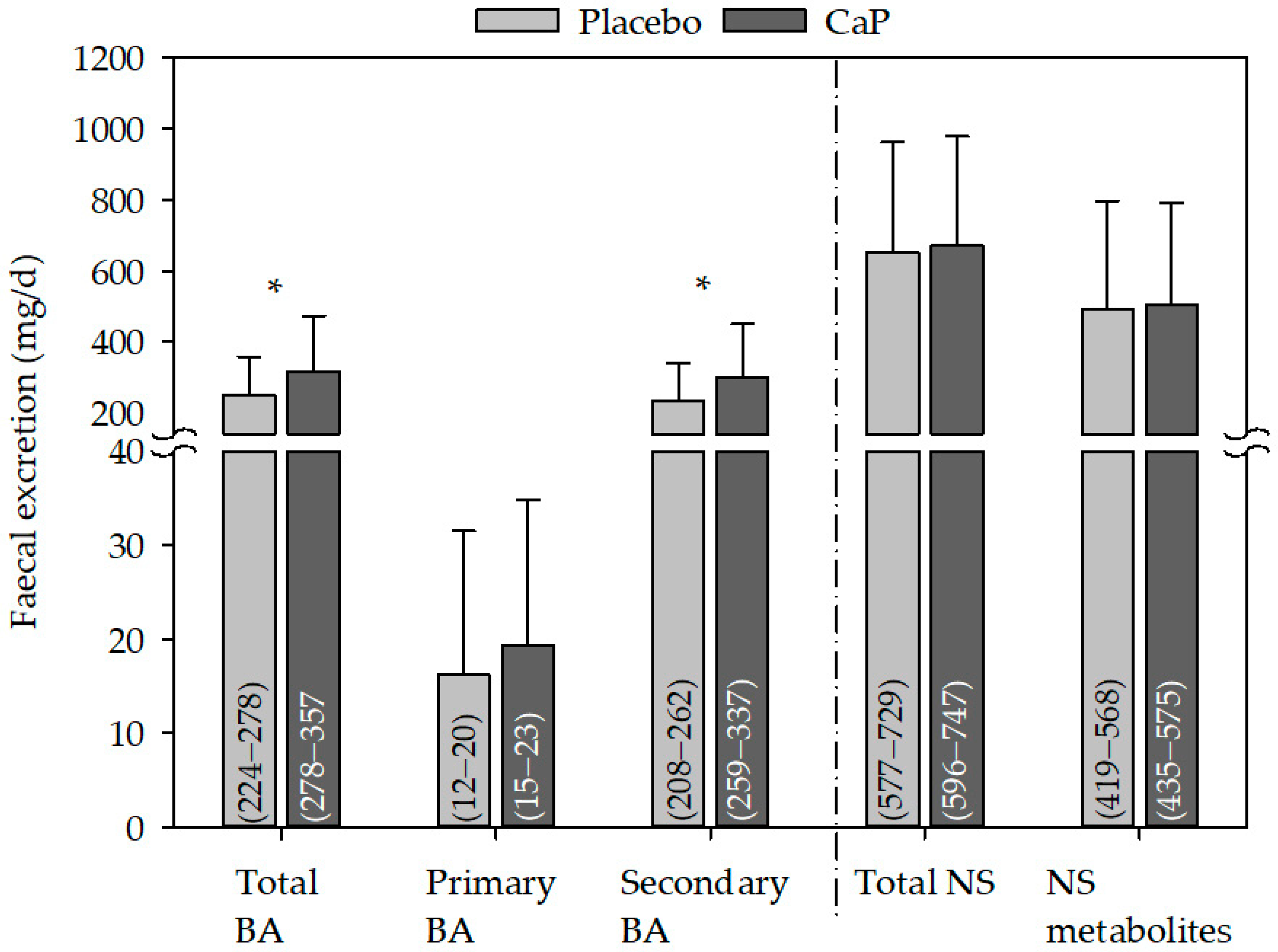
3.1.4. Faecal Sterols
3.2. Results of the Literature Search
3.2.1. Metabolism of Phosphorus and Calcium
3.2.2. Blood Lipids
3.2.3. Intestinal Parameters
4. Discussion
4.1. Metabolism of Calcium and Phosphorus
4.2. Bile Acids and Blood Lipids
4.3. Toxicological Aspects
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Calvo, M.S.; Lamberg-Allardt, C.J. Phosphorus. Adv. Nutr. 2015, 6, 860–862. [Google Scholar] [CrossRef] [PubMed]
- Berndt, T.; Kumar, R. Novel mechanisms in the regulation of phosphorus homeostasis. Physiology 2009, 24, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Dhingra, R.; Sullivan, L.M.; Fox, C.S.; Wang, T.J.; D’Agostino, R.B.; Gaziano, J.M.; Vasan, R.S. Relations of serum phosphorus and calcium levels to the incidence of cardiovascular disease in the community. Arch. Intern. Med. 2007, 167, 879–885. [Google Scholar] [CrossRef] [PubMed]
- Tonelli, M.; Sacks, F.; Pfeffer, M.; Gao, Z.; Curhan, G.; Cholesterol And Recurrent Events Trial Investigators. Relation between serum phosphate level and cardiovascular event rate in people with coronary disease. Circulation 2005, 112, 2627–2633. [Google Scholar] [CrossRef] [PubMed]
- Lampila, L.E. Applications and functions of food-grade phosphates. Ann. N. Y. Acad. Sci. 2013, 1301, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Calvo, M.S.; Uribarri, J. Contributions to total phosphorus intake: All sources considered. Semin. Dial. 2013, 26, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Ritz, E.; Hahn, K.; Ketteler, M.; Kuhlmann, M.K.; Mann, J. Phosphate additives in food—a health risk. Dtsch. Arztebl. Int. 2012, 109, 49–55. [Google Scholar] [PubMed]
- Lederer, E. Regulation of serum phosphate. J. Physiol. 2014, 592, 3985–3995. [Google Scholar] [CrossRef] [PubMed]
- Takeda, E.; Yamamoto, H.; Yamanaka-Okumura, H.; Taketani, Y. Increasing dietary phosphorus intake from food additives: Potential for negative impact on bone health. Adv. Nutr. 2014, 5, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Van der Meer, R.; Lapre, J.A.; Govers, M.; Kleibeuker, J.H. Mechanisms of the intestinal effects of dietary fats and milk products on colon carcinogenesis. Cancer Lett. 1997, 114, 75–83. [Google Scholar] [CrossRef]
- Ditscheid, B.; Keller, S.; Jahreis, G. Cholesterol metabolism is affected by calcium phosphate supplementation in humans. J. Nutr. 2005, 135, 1678–1682. [Google Scholar] [CrossRef] [PubMed]
- Trautvetter, U.; Ditscheid, B.; Kiehntopf, M.; Jahreis, G. A combination of calcium phosphate and probiotics beneficially influences intestinal lactobacilli and cholesterol metabolism in humans. Clin. Nutr. 2012, 31, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Trautvetter, U.; Camarinha-Silva, A.; Jahreis, G.; Lorkowski, S.; Glei, M. High phosphorus intake and gut-related parameters—results of a randomized placebo-controlled human intervention study. Nutr. J. 2018, 17, 23. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, H.; Bernstein, C.; Payne, C.M.; Dvorak, K. Bile acids as endogenous etiologic agents in gastrointestinal cancer. World J. Gastroenterol. 2009, 15, 3329–3340. [Google Scholar] [CrossRef] [PubMed]
- Van der Meer, R.; Kleibeuker, J.H.; Lapre, J.A. Calcium phosphate, bile acids and colorectal cancer. Eur. J. Cancer Prev. 1991, 1 (Suppl. 2), 55–62. [Google Scholar] [CrossRef] [PubMed]
- Ditscheid, B.; Keller, S.; Jahreis, G. Faecal steroid excretion in humans is affected by calcium supplementation and shows gender-specific differences. Eur. J. Nutr. 2009, 48, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Trautvetter, U.; Jahreis, G. Effect of supplementary calcium phosphate on plasma gastrointestinal hormones in a double-blind, placebo-controlled, cross-over human study. Br. J. Nutr. 2014, 111, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Trautvetter, U.; Kiehntopf, M.; Jahreis, G. Postprandial effects of calcium phosphate supplementation on plasma concentration-double-blind, placebo-controlled cross-over human study. Nutr. J. 2013, 12, 30. [Google Scholar] [CrossRef] [PubMed]
- Trautvetter, U.; Neef, N.; Leiterer, M.; Kiehntopf, M.; Kratzsch, J.; Jahreis, G. Effect of calcium phosphate and vitamin D 3 supplementation on bone remodelling and metabolism of calcium, phosphorus, magnesium and iron. Nutr. J. 2014, 13, 6. [Google Scholar] [CrossRef] [PubMed]
- Trautvetter, U.; Jahreis, G.; Kiehntopf, M.; Glei, M. Consequences of a high phosphorus intake on mineral metabolism and bone remodeling in dependence of calcium intake in healthy subjects—A randomized placebo-controlled human intervention study. Nutr. J. 2016, 15, 7. [Google Scholar] [CrossRef] [PubMed]
- Trautvetter, U.; Ditscheid, B.; Jahreis, G.; Glei, M. Habitual intakes, food sources and excretions of phosphorus and calcium in three german study collectives. Nutrients 2018, 10, 171. [Google Scholar] [CrossRef] [PubMed]
- Keller, S.; Jahreis, G. Determination of underivatised sterols and bile acid trimethyl silyl ether methyl esters by gas chromatography-mass spectrometry-single ion monitoring in faeces. J. Chromatogr. B 2004, 813, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Albertazzi, P.; Steel, S.A.; Howarth, E.M.; Purdie, D.W. Comparison of the effects of two different types of calcium supplementation on markers of bone metabolism in a postmenopausal osteopenic population with low calcium intake: A double-blind placebo-controlled trial. Climacteric 2004, 7, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Chapuy, M.C.; Arlot, M.E.; Duboeuf, F.; Brun, J.; Crouzet, B.; Arnaud, S.; Delmas, P.D.; Meunier, P.J. Vitamin d3 and calcium to prevent hip fractures in the elderly women. N. Engl. J. Med. 1992, 327, 1637–1642. [Google Scholar] [CrossRef] [PubMed]
- Heaney, R.P.; Recker, R.R.; Watson, P.; Lappe, J.M. Phosphate and carbonate salts of calcium support robust bone building in osteoporosis. Am. J. Clin. Nutr. 2010, 92, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Bristow, S.M.; Gamble, G.D.; Stewart, A.; Horne, L.; House, M.E.; Aati, O.; Mihov, B.; Horne, A.M.; Reid, I.R. Acute and 3-month effects of microcrystalline hydroxyapatite, calcium citrate and calcium carbonate on serum calcium and markers of bone turnover: A randomised controlled trial in postmenopausal women. Br. J. Nutr. 2014, 112, 1611–1620. [Google Scholar] [CrossRef] [PubMed]
- Dahl, W.J.; Ford, A.L.; Coppola, J.A.; Lopez, D.; Combs, W.; Rohani, A.; Ukhanova, M.; Culpepper, T.; Tompkins, T.A.; Christman, M.; et al. Calcium phosphate supplementation increases faecal lactobacillus spp. In a randomised trial of young adults. Benef. Microbes. 2016, 7, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Cats, A.; Mulder, N.H.; de Vries, E.G.; Oremus, E.T.; Kreumer, W.M.; Kleibeuker, J.H. Calcium phosphate: An alternative calcium compound for dietary prevention of colon cancer? A study on intestinal and faecal parameters in healthy volunteers. Eur. J. Cancer Prev. 1993, 2, 409–415. [Google Scholar] [CrossRef] [PubMed]
- Portale, A.A.; Halloran, B.P.; Murphy, M.M.; Morris, R.C., Jr. Oral intake of phosphorus can determine the serum concentration of 1,25-dihydroxyvitamin d by determining its production rate in humans. J. Clin. Invest. 1986, 77, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Portale, A.A.; Halloran, B.P.; Morris, R.C., Jr. Dietary intake of phosphorus modulates the circadian rhythm in serum concentration of phosphorus. Implications for the renal production of 1,25-dihydroxyvitamin D. J. Clin. Investig. 1987, 80, 1147–1154. [Google Scholar] [CrossRef] [PubMed]
- Calvo, M.S.; Kumar, R.; Heath, H. Persistently elevated parathyroid hormone secretion and action in young women after four weeks of ingesting high phosphorus, low calcium diets. J. Clin. Endocrinol. Metab. 1990, 70, 1334–1340. [Google Scholar] [CrossRef] [PubMed]
- Brixen, K.; Nielsen, H.K.; Charles, P.; Mosekilde, L. Effects of a short course of oral phosphate treatment on serum parathyroid hormone(1–84) and biochemical markers of bone turnover: A dose-response study. Calcif. Tissue Int. 1992, 51, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Whybro, A.; Jagger, H.; Barker, M.; Eastell, R. Phosphate supplementation in young men: Lack of effect on calcium homeostasis and bone turnover. Eur. J. Clin. Nutr. 1998, 52, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Antoniucci, D.M.; Yamashita, T.; Portale, A.A. Dietary phosphorus regulates serum fibroblast growth factor-23 concentrations in healthy men. J. Clin. Endocrinol. Metab. 2006, 91, 3144–3149. [Google Scholar] [CrossRef] [PubMed]
- Sigrist, M.; Tang, M.; Beaulieu, M.; Espino-Hernandez, G.; Er, L.; Djurdjev, O.; Levin, A. Responsiveness of FGF-23 and mineral metabolism to altered dietary phosphate intake in chronic kidney disease (CKD): Results of a randomized trial. Nephrol. Dial. Transplant. 2013, 28, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, O.M.; Luzuriaga-McPherson, A.; Lin, Y.; Gilbert, L.C.; Ha, S.W.; Beck, G.R., Jr. Impact of phosphorus-based food additives on bone and mineral metabolism. J. Clin. Endocrinol. Metab. 2015, 100, 4264–4271. [Google Scholar] [CrossRef] [PubMed]
- Grimm, M.; Müller, A.; Hein, G.; Fünfstück, R.; Jahreis, G. High phosphorus intake only slightly affects serum minerals, urinary pyridinium crosslinks and renal function in young women. Eur. J. Clin. Nutr. 2001, 55, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Newmark, H.L.; Wargovich, M.J.; Bruce, W.R. Colon cancer and dietary fat, phosphate, and calcium: A hypothesis. J. Natl. Cancer Inst. 1984, 72, 1323–1325. [Google Scholar] [PubMed]
- Van der Meer, R.; Welberg, J.W.; Kuipers, F.; Kleibeuker, J.H.; Mulder, N.H.; Termont, D.S.; Vonk, R.J.; De Vries, H.T.; De Vries, E.G. Effects of supplemental dietary calcium on the intestinal association of calcium, phosphate, and bile acids. Gastroenterology 1990, 99, 1653–1659. [Google Scholar] [CrossRef]
- Termine, J.D.; Posner, A.S. Calcium phosphate formation in vitro: I. Factors affecting initial phase separation. Arch. Biochem. Biophys. 1970, 140, 307–317. [Google Scholar] [CrossRef]
- Kemi, V.E.; Karkkainen, M.U.; Lamberg-Allardt, C.J.E. High phosphorus intakes acutely and negatively affect ca and bone metabolism in a dose-dependent manner in healthy young females. Br. J. Nutr. 2006, 96, 545–552. [Google Scholar] [PubMed]
- Zemel, M.B.; Linkswiler, H.M. Calcium metabolism in the young adult male as affected by level and form of phosphorus intake and level of calcium intake. J. Nutr. 1981, 111, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Hegsted, M.; Schuette, S.A.; Zemel, M.B.; Linkswiler, H.M. Urinary calcium and calcium balance in young men as affected by level of protein and phosphorus intake. J. Nutr. 1981, 111, 553–562. [Google Scholar] [CrossRef] [PubMed]
- Kemi, V.E.; Kärkkäinen, M.U.M.; Rita, H.J.; Laaksonen, M.M.L.; Outila, T.A.; Lamberg-Allardt, C.J.E. Low calcium:Phosphorus ratio in habitual diets affects serum parathyroid hormone concentration and calcium metabolism in healthy women with adequate calcium intake. Br. J. Nutr. 2010, 103, 561–568. [Google Scholar] [CrossRef] [PubMed]
- Govers, M.J.A.P.; Termont, D.S.M.L.; Van der Meer, R. Mechanism of the antiproliferative effect of milk mineral and other calcium supplements on colonic epithelium. Cancer Res. 1994, 54, 95–100. [Google Scholar] [PubMed]
- Govers, M.J.; Termont, D.S.; Van Aken, G.A.; Van der Meer, R. Characterization of the adsorption of conjugated and unconjugated bile acids to insoluble, amorphous calcium phosphate. J. Lipid Res. 1994, 35, 741–748. [Google Scholar] [PubMed]
- Van der Meer, R.; De Vries, H.T. Differential binding of glycine-conjugated and taurine-conjugated bile-acids to insoluble calcium-phosphate. Biochem. J. 1985, 229, 265–268. [Google Scholar] [CrossRef] [PubMed]
- Govers, M.J.; Termont, D.S.; Lapre, J.A.; Kleibeuker, J.H.; Vonk, R.J.; Van der Meer, R. Calcium in milk products precipitates intestinal fatty acids and secondary bile acids and thus inhibits colonic cytotoxicity in humans. Cancer Res. 1996, 56, 3270–3275. [Google Scholar] [PubMed]
- Reid, I.R. Effects of calcium supplementation on circulating lipids—Potential pharmacoeconomic implications. Drugs Aging 2004, 21, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Weiner, M.L.; Salminen, W.F.; Larson, P.R.; Barter, R.A.; Kranetz, J.L.; Simon, G.S. Toxicological review of inorganic phosphates. Food Chem. Toxicol. 2001, 39, 759–786. [Google Scholar] [CrossRef]
- Deutsche Gesellschaft für Ernährung; Österreichische Gesellschaft für Ernährung, Schweizerische Gesellschaft für Ernährung. Referenzwerte für die Nährstoffzufuhr (loose-leaf collection), 3rd ed.; Neuer Umschau Buchverlag: Frankfurt am Main, Germany, 2017; Volume 2, ISBN 978-3-86528-148-7. [Google Scholar]
- Bovee-Oudenhoven, I.M.; Wissink, M.L.; Wouters, J.T.; Van der Meer, R. Dietary calcium phosphate stimulates intestinal lactobacilli and decreases the severity of a salmonella infection in rats. J. Nutr. 1999, 129, 607–612. [Google Scholar] [CrossRef] [PubMed]
- Blaine, J.; Chonchol, M.; Levi, M. Renal control of calcium, phosphate, and magnesium homeostasis. Clin. J. Am. Soc. Nephrol. 2015, 10, 1257–1272. [Google Scholar] [CrossRef] [PubMed]
- Pires, A.; Sobrinho, L.; Ferreira, H.G. The calcium/phosphorus homeostasis in chronic kidney disease: From clinical epidemiology to pathophysiology. Acta Med. Port. 2017, 30, 485–492. [Google Scholar] [CrossRef] [PubMed]
- Adeney, K.L.; Siscovick, D.S.; Ix, J.H.; Seliger, S.L.; Shlipak, M.G.; Jenny, N.S.; Kestenbaum, B.R. Association of serum phosphate with vascular and valvular calcification in moderate. J. Am. Soc. Nephrol. 2009, 20, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Uribarri, J. Phosphorus homeostasis in normal health and in chronic kidney disease patients with special emphasis on dietary phosphorus intake. Semin. Dial. 2007, 20, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Coresh, J.; Balk, E.; Kausz, A.T.; Levin, A.; Steffes, M.W.; Hogg, R.J.; Perrone, R.D.; Lau, J.; Eknoyan, G. National kidney foundation practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Ann. Intern. Med. 2003, 139, 137–147. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study 1 | Study 2 | Study 3 | Study 4 | |
|---|---|---|---|---|
| Study characteristics | ||||
| Design | Double-blind, placebo-controlled | |||
| Cross-over | Cross-over | Cross-over | Parallel | |
| Year | 2002 | 2006 | 2010 | 2011 |
| Supplement, dosage and duration | Ca5(PO4)3OH, 0.5 g P/day 1.0 g Ca/day, 4 weeks | Ca5(PO4)3OH, 0.5 g P/day 1.0 g Ca/day, 4 weeks | Ca5(PO4)3OH, 0.5 g P/day 1.0 g Ca/day, 3 weeks | Ca5(PO4)3OH, 0.5 g P/day 1.0 g Ca/day, 8 weeks |
| CaCO3, 1.0 g Ca/day, 4 weeks | Vitamin D3, 10 µg/day, 8 weeks | |||
| Ca3(PO4)2, 0.52 g P/day 1.0 g Ca/day, 4 weeks | Ca5(PO4)3OH + Vitamin D3 0.5 g P/day 1.0 g Ca/day, 10 µg/day vitamin D3, 8 weeks * | |||
| Placebo, 4 weeks | Placebo, 4 weeks | Placebo, 3 weeks | Placebo, 2 weeks | |
| Analyses | ||||
| Minerals in serum/plasma | ✓ | ✓ | ✓ | ✓ |
| Minerals in urine/faeces | ✓ | ✓ | ✓ | |
| Blood lipids | ✓ | ✓ | ✓ | |
| Faecal sterols | ✓ | ✓ | ✓** | |
| Characteristics | All | Women | Men |
|---|---|---|---|
| n | 90 | 42 | 48 |
| Age (year) | 28 ± 9 | 29 ± 10 | 27 ± 8 |
| BMI (kg/m2) | 23 ± 3 | 22 ± 4 | 23 ± 3 |
| Parameter | Placebo | CaP | Change |
|---|---|---|---|
| Energy | 9 ± 2 | 9 ± 2 | 013 ± 1 |
| (MJ/day) | (7–9) | (9–10) | (−0.09–0.3) |
| Fat | 84 ± 25 | 85 ± 27 | 0.7 ± 15 |
| (g/day) | (79–90) | (79–91) | (−2–4) |
| Protein | 82 ± 19 | 82 ± 19 | 0.3 ± 12 |
| (g/day) | (78–86) | (78–86) | (−2–3) |
| Carbohydrates | 265 ± 49 | 271 ± 56 | 5 ± 36 |
| (g/day) | (255–276) | (259–282) | (−3–13) |
| Calcium | 1069 ± 289 | 2088 * ± 314 | 1019 # ± 209 |
| (mg/day) | (1009–1130) | (2022–2154) | (975–1063) |
| Calcium | 16 ± 4 | 31 * ± 6 | 15 # ±4 |
| (mg/kg bw.) | (15–17) | (30–32) | (14–16) |
| Phosphorus | 1434 ± 315 | 1924 * ± 323 | 490 # ± 199 |
| (mg/day) | (1368–1500) | (1857–1992) | (449–532) |
| Phosphorus | 21 ± 4 | 28 * ± 5 | 7 # ± 3 |
| (mg/kg bw.) | (20–22) | (27–29) | (7–8) |
| Parameter | Placebo | CaP | Change |
|---|---|---|---|
| Total cholesterol | 4.80 ± 1.06 | 4.65 * ± 1.03 | −0.15 ± 0.47 |
| (mmol/L) | (4.6–5.0) | (4.4–4.9) | (−0.25–(−0.04)) |
| HDL-cholesterol | 1.45 ± 0.37 | 1.48 ± 0.38 | 0.03 ± 0.17 |
| (mmol/L) | (1.4–1.5) | (1.4–1.6) | (−0.01–0.07) |
| LDL-cholesterol | 2.87 ± 0.94 | 2.76 * ± 0.92 | −0.11 # ± 0.42 |
| (mmol/L) | (2.7–3.1) | (2.6–3.0) | (−0.2–(−0.02)) |
| LDL:HDL-ratio | 2.12 ± 0.91 | 1.99 * ± 0.84 | −0.13 ± 0.41 |
| (1.9–2.3) | (1.8–2.2) | (−0.2–(−0.04)) | |
| Triacylglycerides | 0.99 ± 0.59 | 0.96 ± 0.37 | −0.03 ± 0.54 |
| (mmol/L) | (0.9–1.1) | (0.9–1.0) | (−0.2–0.1) |
| Parameter | Placebo | CaP | Change |
|---|---|---|---|
| iLCA | 39 ± 24 | 45 * ± 28 | 6 ± 21 |
| (mg/day) | (33–45) | (38–52) | (0.3–11.0) |
| LCA | 54 ± 31 | 69 * ± 36 | 15 # ± 24 |
| (mg/day) | (47–62) | (60–78) | (8.4–20.8) |
| iDCA | 34 ± 24 | 37 ± 40 | 3 ± 28 |
| (mg/day) | (28–40) | (27–47) | (−4.1–9.9) |
| DCA | 98 ± 43 | 135 * ± 73 | 36 ± 56 |
| (mg/day) | (88–109) | (116–153) | (22.2–50.5) |
| CDCA | 6 ± 4 | 7 * ± 5 | 1 # ± 4 |
| (mg/day) | (5–7) | (6–8) | (0.02–2.3) |
| CA | 10 ± 12 | 12 ± 11 | 2 ± 11 |
| (mg/day) | (7–13) | (9–15) | (−0.9–4.8) |
| 12keto DCA | 8 ± 7 | 11 * ± 12 | 4 ± 9 |
| (mg/day) | (6–9) | (8–15) | (1.5–6.0) |
| Parameter | Placebo | CaP | Change |
|---|---|---|---|
| Coprostanol | 430 ± 265 | 443 ± 259 | 160 ± 152 |
| (mg/day) | (365–496) | (379–506) | (−47–71) |
| Cholesterol | 160 ± 153 | 166 ±187 | 6 ± 121 |
| (mg/day) | (123–198) | (120–212) | (−24–36) |
| Cholestanol | 14 ± 8 | 13 ± 9 | −0.5 ± 5 |
| (mg/day) | (12–16) | (11–16) | (−1.6–0.7) |
| Coprostanone | 41 ± 43 | 40 ± 33 | −1.0 ± 34 |
| (mg/day) | (30–51) | (32–48) | (−9.3–7.3) |
| Cholestanone | 3 ± 3 | 3 ± 2 | 0.1 ± 2 |
| (mg/day) | (2–4) | (3–4) | (−0.4–0.6) |
| Cholestenone | 5 ± 4 | 5 ± 4 | 0 ± 3 |
| (mg/day) | (4–6) | (4–6) | (−0.8–0.9) |
| Study Design | Results 1 | Comments/More Results 2 | |
|---|---|---|---|
| Calcium Phosphate Supplementation | |||
| [23] A | -153 postmenopausal women, >60 years -double-blind, placebo-controlled, parallel design -group TCP: ossein-hydroxyyapatit (TCP; aCa: 500 mg, bCa: 651 mg, aP: 258 mg *) -group OHC: tricalcium phosphate (OHC, aCa: 500 mg, bCa: 563 mg, aP: 258 mg *) -group placebo (bCa: 679 mg) -6 months (analysis after 3 and 6 months) | -uCa↑ after both supplements, OHC > TCP | -TCP is the ash of OHC, OHC included inorganic matrix -markers of bone formation ↓ after TCP and OHC -bone resorption marker and bone mineral density = after TCP and OHC |
| [24] A | -3270 healthy older women, 84 ± 6 years -placebo-controlled, parallel design -group tricalcium phosphate (aCa: 1,2 g, bCa: 511 mg + 20 µg, aP: 620 mg *, vitamin D3) -group placebo: (bCa: 514 mg) -18 months | -sCa = in tricalcium phosphate group -sCa ↓ in placebo group | -hip fractures and nonvertebral fractures ↓ in tricalcium phosphate group -PTH ↓ in tricalcium phosphate group -1,25-(OH)2D ↑ in the tricalcium phosphate group -bone density of proximal femur ↑ in tricalcium phosphate group and ↓ in placebo group |
| [11], A, B, C | -double-blind, placebo-controlled, cross-over design -31 healthy young women and men, 25 ± 2 years -test diet: CaP (aCa: 1000 mg; bCa: 1104 mg, aP: 500 mg, bP: 1498 mg) -placebo diet (bCa: 1193 mg, bP: 1528 mg) -4 weeks each diet | -sCa = after CaP and placebo -uCa, fCa, and fP ↑ after CaP -total cholesterol ↓ after CaP -fBA (total and secondary) ↑ after CaP -faecal cholestenone and cholesterol ↑ after CaP -faecal coprostanol and cholestanol ↓ after CaP | |
| [16] A, C | -31 healthy young women and men, 25 ± 2 years -double-blind, placebo-controlled, cross-over design -test diet: CaP (aCa: 1000 mg; bCa: 1104 mg, aP: 500 mg, bP: 1498 mg) -placebo diet (bCa: 1193 mg, bP: 1528 mg) -4 weeks each diet | -faecal LCA; DCA and 12keto DCA ↑ after CaP -iLCA in faecal water ↓ after CaP -total NS ↓ after CaP -genotoxicity of faecal water = after CaP | |
| [25] A | -211 postmenopausal osteoporotic women, 60–85 years -randomised, positive-comparator, 2-arm, single-blind -arm 1: tricalcium phosphate salt (aCa: 1800 mg, aP: 930 mg *, bP: <1000 mg) + 20 µg/day teripatide (osteoporosis therapy) + 1000 IU vitamin D -arm 2: calcium carbonate (aCa: 1800 mg, bP: < 1000 mg) + 20 µg/day teripatide (osteoporosis therapy) + 1000 IU vitamin D -12 months | -sPO4 ↑ after tricalcium phosphate supplementation (also calcium carbonate group) -uP/Crea and uCa/Crea ↑ after tricalcium phosphate supplementation -sCa= | -bone resorption marker ↑ in both groups |
| [12] A, B, C | -32 men and women, 25 ± 5 years -double-blind, placebo-controlled, cross-over design -test diet 1: CaP + probiotic (1010 CFU/day) (aCa: 1000 mg; bCa: 807 mg, aP: 500 mg, bP: 1316 mg) -test diet 2: probiotic (1010 CFU/d) (bCa: 873 mg, bP: 1379 mg) -placebo diet (bCa: 866 mg, bP: 1367 mg) -4 weeks each diet | -fCa and fP ↑ after CaP + probiotic -total cholesterol and LDL-cholesterol ↓ after CaP + probiotic -f secondary BA ↑ after CaP + probiotic -faecal lactobacilli and supplemented probiotic strain ↑ after CaP + probiotic and probiotic | |
| [18] A | -9 young men, 27 ± 4 years -double-blind, placebo-controlled, cross-over design -test diet: CaP (aCa: 1000 mg, bCa: 915, aP: 500 mg, bP: 1531 mg) -placebo diet (bCa: 926 mg, bP: 1542 mg) -3 weeks each diet | -sPO4 und sCa= after CaP -AUC pCa after three weeks CaP ↑ -AUC pPO4 after three weeks CaP= | |
| [26], A | -100 postmenopausal women, 71 ± 5 years -single-blind, placebo-controlled, parallel design -group 1: calcium citrate (aCa: 1000 mg, bCa: 970 mg) -group 2: calcium carbonate (aCa: 1000 mg, bCa: 810 mg) -group 3: microcrystalline hydroxyapatite preparation 1 (MCHA, aCa: 1000 mg, bCa: 890 mg) -group 4: microcrystalline hydroxyapatite preparation 2 (MCHB, aCa: 1000 mg, bCa: 780 mg) -placebo group (bCa: 900 mg) -3 months | -sPO4 after MCHA/MCHB supplementation ↓ as compared with baseline | -no differences after 3 months between calcium carbonate and citrate or between the two MCH preparations → citrate and carbonate as well as 2 MCH preparations were pooled and analysed together -sCa ↑ after citrate/carbonate supplementation -PTH ↓ after all interventions as compared with placebo -bone markers ↓ after all interventions as compared with placebo |
| [19], A | -60 men and women, 42 ± 12 years -double-blind, placebo-controlled, parallel design -group 1: CaP (aCa: 1000 mg, bCa: 1014 mg, aP: 500 mg, bP: 1333 mg) -group 2: vitamin D (10 µg/day, bCa: 916 mg, bP: 1324 mg) -group 3: CaP + vitamin D (10 µg, aCa: 1000 mg, bCa: 872 mg, aP: 500 mg, bP: 1205 mg) -8 weeks each intervention -before the interventions, 2 weeks of placebo in each group (bCa: approximately 900 mg, bP: 1300 mg) -supplement: CaP and vitamin D3 | -uCa ↑ after CaP as compared with placebo -fCa and fP ↑ after CaP and CaP + vitamin D as compared with placebo -uP and pPO4 = after CaP as compared with placebo -pCa ↑ after all interventions as compared with placebo | -25-(OH)D ↑ after vitamin D and CaP + vitamin D after 8 weeks→ after 4 weeks only in the CaP + vitamin D group -PTH = after all interventions as compared with placebo -bone markers = after all interventions as compared with placebo |
| [27] C | Study 1 -15 men and women, 20.4 ± 1.6 years -double-blind, cross over design -test diet 1: tricalcium phosphate (aCa: 500 mg, aP: 258 mg *) -test diet 2: calcium carbonate (aCa: 500 mg) -2 weeks each diet Study 2 -17 men and women, 25.2 ± 6.8 years -double-blind, cross over design -test diet 1: 2 probiotic strains -test diet 2: 2 probiotic strains + calcium carbonate (aCa: 500 mg) -test diet 3: 2 probiotic strains + tricalcium phosphate (aCa: 500 mg, aP: 258 mg *) -2 weeks each diet | -Study 1: faecal Lactobacillus ssp. counts = -Study 2: faecal Lactobacillus ssp. counts ↑ after probiotic + tricalcium phosphate as compared with baseline | Study 2: faecal Lactobacillus ssp. counts = after probiotic with calcium carbonate |
| [28] C | -14 men and women, 25–37 years -single-arm-study -control period 1: habitual diet (bCa: 1400 mg. bP: 1700 mg) -test diet: tricalcium phosphate (Ca3(PO4)2, aCa: 1500 mg, bCa: 1400 mg; aP: 750 mg *, bP: 1700 mg) -control period 2: habitual diet (bCa: 1400 mg, bP: 1700 mg) -1 weeks each period and diet | -cytolytic activity and intestinal alkaline phosphatase of faecal water, fBA, ffats = after tricalcium phosphate | -modulation of duodenal bile acids (no significant effect) after tricalcium phosphate |
| Phosphate supplementation | |||
| [29] A | -6 men, 26–40 years -single-arm study -control period: normal diet (aCa: 650 mg; bCa: 200 mg; aP: 1000 mg; bP: 500 mg) neutral sodium phosphate/potassium phosphate, calcium carbonate -test period 1: low phosphorus (aCa: 650 mg, bCa: 200 mg, bP: < 500 by phosphate binders), sodium chloride/potassium chloride, calcium carbonate -test period 2: high phosphorus (aCa: 650 mg, bCa: 200 mg, aP: 2500 mg, bP: 500 mg), sodium phosphate/potassium phosphate, calcium carbonate -9 days (control period), 10 days (test periods) | -sPO4 ↑ after high phosphorus diet increased after 1 day → ↓within 10 days as compared with control period -uP ↑; uCa ↓; sCa= after high phosphorus diet as compared with control period | -1,25-(OH)2D ↑ after low phosphorus diet as compared with control period -1,25-(OH)2D ↓ after high phosphorus diet as compared with control period -production rate of 1,25OHD ↑ after low phosphorus diet as compared with control period -production rate of 1,25OHD ↓ after high phosphorus diet as compared with control period -metabolic clearance rate of 1,25OHD= |
| [30] A | -6 men, 26–40 year -single-arm study -control period: normal diet (aCa: 650 mg; bCa: 200 mg; aP: 1000 mg; bP: 500 mg) neutral sodium phosphate/potassium phosphate, calcium carbonate -test period 1: low phosphorus (aCa: 650 mg, bCa: 200 mg, bP: < 500 mg by phosphate binders), sodium chloride/potassium chloride, calcium carbonate -test period 2: high phosphorus (aCa: 650 mg, bCa: 200 mg, aP: 2500 mg, bP: 500 mg), sodium phosphate/potassium phosphate, calcium carbonate -9 days (control period), 10 days (test periods) | -24 h mean of sPO4 ↑, with doubled peak in the afternoon rise after high phosphorus diet as compared with control diet -24 h mean of sCa=, 24 h mean of ionized Ca ↓ after high phosphorus diet as compared with control period | -24 h mean sPO4 ↓ after low phosphorus diet as compared with control period |
| [31] A | -15 young women, 18–25 years -parallel design, -control group: basal diet (bCa: 800 mg, bP: 900 mg), 56 days -experimental group: first 28 days of basal diet (bCa: 800 mg, bP: 900 mg), 28 days of high phosphorus/low calcium diet (bCa: 400 mg, bP: 1700 mg) -supplement: processed food | -sPO4 (fasting and postprandial) = -fasting sCa ↓ after high phosphorus/low calcium diet as compared with basal diet -postprandial sCa= | -PTH ↑ after high phosphorus/low calcium diet as compared with basal diet -1,25-(OH)2D= |
| [32] A | -79 postmenopausal women, 50–75 year -double-blind, placebo-controlled, parallel design -group I (aP: 750 mg) -group II (aP: 1500 mg) -group III (aP: 2250 mg) -group IV placebo -supplement: mix of ammonium phosphate, potassium phosphate, and glycerol phosphate -7 days each group | -sPO4= -uPO4/Crea ↑ with increasing phosphate → returned to normal after 7 days follow-up -uCa/Crea and sCa= | -PTH ↑ in group II/III -1,25-(OH)2D= -group II: osteocalcin ↑ |
| [33] A | Study 1 -10 healthy men, 19–32 years -randomised, cross-over design -control diet (bCa: 500 mg, bPO4: 800 mg -test diet (bCa: 500 mg, aP: 1000 mg, bPO4: 800 mg) -7 days each diet -supplement: sodium acid phosphate Study 2 -12 healthy men, 19–38 years -single-arm study -test diet 1: control diet (bCa: 1000 mg, bP: 1000 mg) -test diet 2 (bCa: 1000 mg, aP: 1000 mg, bP: 1000 mg) -test diet 3 (bCa: 1000 mg, aP: 1500 mg, bP: 1000 mg) -test diet 4: (bCa: 1000 mg, aP: 2000 mg, bP: 1000 mg) -7 days each diet -supplement: sodium acid phosphate | -both studies: uPO4 ↑ and uCa↓ after phosphorus diets as compared with control diets -sPO4 and sCa= | -PTH: Study 1 ↑ after test diet as compared with control diet and Study 2= -no change in bone markers |
| [34] A | -13 healthy men, 28–43 years -single-arm study -test diet 1: control (bCa: 850 mg, aP: 1000 mg, bP: 500 mg) -test diet 2: supplemented (bCa: 850 mg, aP: 1800 mg, bP: 500 mg) -test diet 3: restricted (bCa: 850 mg, bP: 625 mg) -9 days for each diet -supplement: sodium and potassium phosphate | -uP ↑, uCa=, sPO4, sCa = after supplemented diet as compared with control diet | -FGF23 ↓ after restriction diet as compared with supplemented and control diets -1,25-(OH)2D ↑ after restriction diet as compared with supplemented and control diets -PTH ↓ after restriction diet as compared with supplemented and control diets |
| [35] A | -12 healthy men and women (from control group), 31–48 years -cross-over design -test diet 1: high phosphate (bP: 2000 mg) -test diet 2: low phosphate (bP: 750 mg) -test diet 3: low phosphate with phosphate binder (bP: 750 mg + phosphate binder) -7 days each test diet -supplement: non-perishable manufactured food products | -sPO4=, uP ↑, uCa = after high phosphate diet as compared with baseline | -FGF23 = after high phosphate diet as compared with baseline -PTH = after high phosphate diet as compared with baseline |
| [36] A | -10 healthy men and women, 19–45 years -single-arm design -run in period: ad libitum diets -test diet 1: low additive diet (bCa: 732 mg, bP: 1070 mg) -test diet 2: high additive diet (bCa: 677 mg, bP: 1677 mg) -2 weeks (run in period), 1 week (test diets) -supplement: phosphorus additive enhanced menus | -uP↓, uCa=, sPO4=, sCa= after high additive diet as compared with run in period | PTH=, FGF23↑, osteocalcin ↑, P1NP ↓, sclerostin ↓, osteopontin ↑ after high additive diet compared low additive diet |
| [20] A | -62 men and women, 29 ± 7 years -double-blind, placebo-controlled, parallel design -group 1 (bCa: 900 mg, aP: 1000 mg, bP: 1200 mg) -group 2: (aCa: 500 mg, bCa: 900 mg, aP: 1000 mg, bP: 1300 mg) -group 3 (aCa: 1000 mg, bCa: 900 mg, aP: 1000 mg, bP: 1300 mg) -8 weeks each intervention -before the interventions, 2 weeks of placebo in each group (bCa: appr. 900 mg, bP: 1300 mg) -supplement: calcium carbonate and monosodium phosphate | -sPO4 and sCa= -fP ↑, uP ↑, uCa↓, fCa = after intervention in group 1 (phosphate without calcium) as compared with placebo -fP↑, fCa↑, uCa = in group 2 and 3 (phosphate with calcium) | -FGF23 ↑ after all interventions as compared with placebo after four weeks and then returned to placebo values -bone marker= -PTH= |
| [13] C | -62 men and women, 29 ± 7 years -double-blind, placebo-controlled, parallel design -group 1 (bCa: 900 mg, aP: 1000 mg, bP: 1200 mg) -group 2: (aCa: 500 mg, bCa: 900 mg, aP: 1000 mg, bP: 1300 mg) -group 3 (aCa: 1000 mg, bCa: 900 mg, aP: 1000 mg, bP: 1300 mg) -8 weeks each intervention -before the interventions, 2 weeks of placebo in each group (bCa: appr. 900 mg, bP: 1300 mg) -supplement: calcium carbonate and monosodium phosphate | -geno- and cytotoxicity of FW = in all groups | -modulation in faecal short-chain fatty acids and microbiota |
| [37] A | -10 young women, 20–30 years -single-arm design -control period 1: basic diet (bCa: 1500 mg, bP: 1700 mg) -supplementation period: (bCa: 1995 mg, aP: 1600 mg, bP: 1400 mg) -control period 2: basic diet (bCa: 1500 mg, bP: 1700 mg) -2 weeks (control period 1), 6 weeks (supplementation period), 4 weeks (control period 2) -supplement: monosodium phosphate | -sPO4= | PTH, bone marker= |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trautvetter, U.; Ditscheid, B.; Jahreis, G.; Glei, M. Calcium and Phosphate Metabolism, Blood Lipids and Intestinal Sterols in Human Intervention Studies Using Different Sources of Phosphate as Supplements—Pooled Results and Literature Search. Nutrients 2018, 10, 936. https://doi.org/10.3390/nu10070936
Trautvetter U, Ditscheid B, Jahreis G, Glei M. Calcium and Phosphate Metabolism, Blood Lipids and Intestinal Sterols in Human Intervention Studies Using Different Sources of Phosphate as Supplements—Pooled Results and Literature Search. Nutrients. 2018; 10(7):936. https://doi.org/10.3390/nu10070936
Chicago/Turabian StyleTrautvetter, Ulrike, Bianka Ditscheid, Gerhard Jahreis, and Michael Glei. 2018. "Calcium and Phosphate Metabolism, Blood Lipids and Intestinal Sterols in Human Intervention Studies Using Different Sources of Phosphate as Supplements—Pooled Results and Literature Search" Nutrients 10, no. 7: 936. https://doi.org/10.3390/nu10070936
APA StyleTrautvetter, U., Ditscheid, B., Jahreis, G., & Glei, M. (2018). Calcium and Phosphate Metabolism, Blood Lipids and Intestinal Sterols in Human Intervention Studies Using Different Sources of Phosphate as Supplements—Pooled Results and Literature Search. Nutrients, 10(7), 936. https://doi.org/10.3390/nu10070936