Ethnic Differences in Magnesium Intake in U.S. Older Adults: Findings from NHANES 2005–2016



 ,
,  ,
, 
 , and
, and
Abstract
1. Introduction
2. Materials and Methods
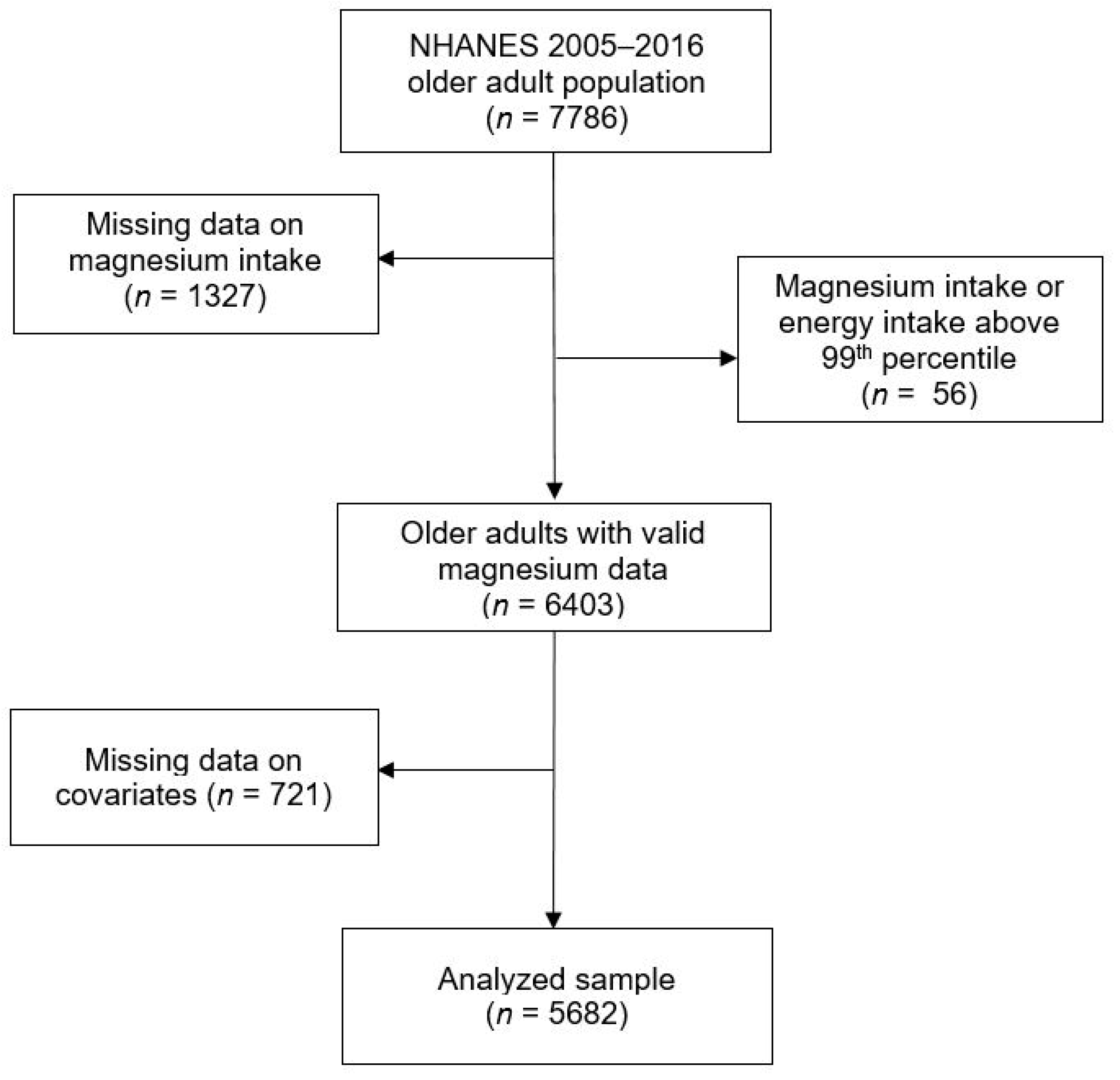
2.1. Study Population
2.2. Dietary Assessment
2.3. Ethnicity
2.4. Covariates
2.5. Statistical Analyses
3. Results
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Arnaud, M.J. Update on the assessment of magnesium status. Br. J. Nutr. 2008, 99, S24–S36. [Google Scholar] [CrossRef] [PubMed]
- Killilea, D.W.; Maier, J.A.M. A connection between magnesium deficiency and aging: New insights from cellular studies. Magnes Res. 2008, 21, 77–82. [Google Scholar] [PubMed]
- Barbagallo, M.; Dominguez, L.J. Magnesium and aging. Curr. Pharm. Des. 2010, 16, 832–839. [Google Scholar] [CrossRef] [PubMed]
- Billard, J.M. Ageing, hippocampal synaptic activity and magnesium. Magnes Res. 2006, 19, 199–215. [Google Scholar]
- Dominguez, L.J.; Barbagallo, M.; Lauretani, F.; Bandinelli, S.; Bos, A.; Corsi, A.M.; Simonsick, E.M.; Ferrucci, L. Magnesium and muscle performance in older persons: The InCHIANTI study. Am. J. Clin. Nutr. 2006, 84, 419–426. [Google Scholar] [CrossRef]
- Veronese, N.; Stubbs, B.; Maggi, S.; Notarnicola, M.; Barbagallo, M.; Firth, J.; Dominguez, L.J.; Caruso, M.G. Dietary magnesium and incident frailty in older people at risk for knee osteoarthritis: An eight-year longitudinal study. Nutrients 2017, 9, 1253. [Google Scholar] [CrossRef]
- Veronese, N.; Stubbs, B.; Solmi, M.; Noale, M.; Vaona, A.; Demurtas, J.; Maggi, S. Dietary magnesium intake and fracture risk: Data from a large prospective study. Br. J. Nutr. 2017, 117, 1570–1576. [Google Scholar] [CrossRef]
- Barbagallo, M.; Dominguez, L.J. Magnesium and type 2 diabetes. World J. Diabetes 2015, 6, 1152–1157. [Google Scholar] [CrossRef]
- Guerrero-Romero, F.; Rodríguez-Morán, M. The effect of lowering blood pressure by magnesium supplementation in diabetic hypertensive adults with low serum magnesium levels: A randomized, double-blind, placebo-controlled clinical trial. J. Hum. Hypertens. 2009, 23, 245–251. [Google Scholar] [CrossRef]
- Wolf, F.I.; Maier, J.A.M.; Nasulewicz, A.; Feillet-Coudray, C.; Simonacci, M.; Mazur, A.; Cittadini, A. Magnesium and neoplasia: From carcinogenesis to tumor growth and progression or treatment. Arch. Biochem. Biophys. 2007, 458, 24–32. [Google Scholar] [CrossRef]
- Rosanoff, A.; Weaver, C.M.; Rude, R.K. Suboptimal magnesium status in the United States: Are the health consequences underestimated? Nutr. Rev. 2012, 70, 153–164. [Google Scholar] [CrossRef] [PubMed]
- Veronese, N.; Berton, L.; Carraro, S.; Bolzetta, F.; De Rui, M.; Perissinotto, E.; Toffanello, E.D.; Bano, G.; Pizzato, S.; Miotto, F.; et al. Effect of oral magnesium supplementation on physical performance in healthy elderly women involved in a weekly exercise program: A randomized controlled trial. Am. J. Clin. Nutr. 2014, 100, 974–981. [Google Scholar] [CrossRef] [PubMed]
- DiNicolantonio, J.J.; O’Keefe, J.H.; Wilson, W. Subclinical magnesium deficiency: A principal driver of cardiovascular disease and a public health crisis. Open Heart 2018, 5, e000668corr1. [Google Scholar] [CrossRef] [PubMed]
- Office of Dietary Supplements—Magnesium. Available online: https://ods.od.nih.gov/factsheets/Magnesium-HealthProfessional/ (accessed on 8 November 2018).
- Ford, E.S.; Mokdad, A.H. Dietary magnesium intake in a national sample of U.S. adults. J. Nutr. 2003, 133, 2879–2882. [Google Scholar] [CrossRef] [PubMed]
- Ford, E.S. Race, education, and dietary cations: Findings from the Third National Health and Nutrition Examination Survey. Ethn. Dis. 1998, 8, 10–20. [Google Scholar] [PubMed]
- Hiza, H.A.B.; Casavale, K.O.; Guenther, P.M.; Davis, C.A. Diet Quality of Americans Differs by Age, Sex, Race/Ethnicity, Income, and Education Level. J. Acad. Nutr. Diet. 2013, 113, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Adams, I.K.R.; Spees, C.K.; Krok, J.L.; Taylor, C.A. Poor diet quality across ethnic groups and gender in U.S. adults: National Health and Nutrition Examination Survey (NHANES) 2005–2012. J. Nutr. Educ. Behav. 2017, 49, S83. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. NHANES—National Health and Nutrition Examination Survey Homepage. 2018. Available online: https://www.cdc.gov/nchs/nhanes/index.htm (accessed on 7 November 2018).
- Ahluwalia, N.; Dwyer, J.; Terry, A.; Moshfegh, A.; Johnson, C. Update on NHANES dietary data: Focus on collection, release, analytical considerations, and uses to inform public policy. Adv. Nutr. 2016, 7, 121–134. [Google Scholar] [CrossRef]
- Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults. National Heart, Lung, and Blood Institute; NHLBI Obesity Education Initiative Expert Panel on the Identification, Evaluation, and Treatment of Obesity in Adults (US): Bethesda, MD, USA, 1998.
- Curtin, L.R.; Mohadjer, L.K.; Dohrmann, S.M.; Montaquila, J.M.; Kruszan-Moran, D.; Mirel, L.B.; Carroll, M.D.; Hirsch, R.; Schober, S.; Johnson, C.L. The national health and nutrition examination survey: Sample design, 1999–2006. Vital Health Stat. 2 2012, 1–39. [Google Scholar]
- Jee, S.H.; Miller, E.R.; Guallar, E.; Singh, V.K.; Appel, L.J.; Klag, M.J. The effect of magnesium supplementation on blood pressure: A meta-analysis of randomized clinical trials. Am. J. Hypertens. 2002, 15, 691–696. [Google Scholar] [CrossRef]
- Song, Y.; He, K.; Levitan, E.B.; Manson, J.E.; Liu, S. Effects of oral magnesium supplementation on glycaemic control in Type 2 diabetes: A meta-analysis of randomized double-blind controlled trials. Diabet. Med. 2006, 23, 1050–1056. [Google Scholar] [PubMed]
- Diabetes UK. Diabetes in the UK 2010: Key Statistics on Diabetes. Available online: https://www.diabetes.org.uk/resources-s3/2017-11/diabetes_in_the_uk_2010.pdf (accessed on 11 July 2018).
- Lane, D.A.; Lip, G.Y.H. Ethnic differences in hypertension and blood pressure control in the UK. Int. J. Med. 2001, 94, 391–396. [Google Scholar] [CrossRef]
- Cauley, J.A. Defining ethnic and racial differences in osteoporosis and fragility fractures. Clin. Orthop. Relat. Res. 2011, 469, 1891–1899. [Google Scholar] [CrossRef] [PubMed]
- Bandeen-Roche, K.; Seplaki, C.L.; Huang, J.; Buta, B.; Kalyani, R.R.; Varadhan, R.; Xue, Q.L.; Walston, J.D.; Kasper, J.D. Frailty in older adults: A nationally representative profile in the United States. J. Gerontol. A Biol. Sci. Med. Sci. 2015, 70, 1427–1434. [Google Scholar] [CrossRef] [PubMed]
- Bleich, S.N.; Jarlenski, M.P.; Bell, C.N.; LaVeist, T.A. Health inequalities: Trends, progress, and policy. Annu. Rev. Public Health 2012, 33, 7–40. [Google Scholar] [CrossRef] [PubMed]
- Arber, S.; Ginn, J. Gender and inequalities in health in later life. Soc. Sci. Med. 1993, 36, 33–46. [Google Scholar] [CrossRef]
- Dunlop, D.D.; Manheim, L.M.; Song, J.; Chang, R.W. Gender and ethnic/racial disparities in health care utilization among older adults. J. Gerontol. B Psychol. Sci. Soc. Sci. 2002, 57, S221–S233. [Google Scholar] [CrossRef]
- Wang, D.D.; Leung, C.W.; Li, Y.; Ding, E.L.; Chiuve, S.E.; Hu, F.B.; Willett, W.C. Trends in dietary quality among adults in the United States, 1999 through 2010. JAMA Int. Med. 2014, 174, 1587–1595. [Google Scholar] [CrossRef]
- Satia, J.A. Diet-related disparities: Understanding the problem and accelerating solutions. J. Am. Diet. Assoc. 2009, 109, 610–615. [Google Scholar] [CrossRef]
- Kant, A.K.; Graubard, B.I.; Kumanyika, S.K. Trends in black-white differentials in dietary intakes of U.S. adults, 1971–2002. Am. J. Prev. Med. 2007, 32, 264–272. [Google Scholar] [CrossRef]
- Wang, Y.; Chen, X. How much of racial/ethnic disparities in dietary intakes, exercise, and weight status can be explained by nutrition- and health-related psychosocial factors and socioeconomic status among US adults? J. Am. Diet. Assoc. 2011, 111, 1904–1911. [Google Scholar] [CrossRef] [PubMed]
- Ethnic and Racial Minorities & Socioeconomic Status. Available online: http://www.apa.org/pi/ses/resources/publications/minorities.aspx (accessed on 8 November 2018).
- Black, C.; Moon, G.; Baird, J. Dietary inequalities: What is the evidence for the effect of the neighbourhood food environment? Health Place 2014, 27, 229–242. [Google Scholar] [CrossRef] [PubMed]
- Block, J.P.; Scribner, R.A.; DeSalvo, K.B. Fast food, race/ethnicity, and income: A geographic analysis. Am. J. Pre. Med. 2004, 27, 211–217. [Google Scholar]
- French, S.A.; Harnack, L.; Jeffery, R.W. Fast food restaurant use among women in the Pound of Prevention study: Dietary, behavioral and demographic correlates. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 1353–1359. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Caucasian | Africa American | Hispanic | Other | p | |
|---|---|---|---|---|---|
| (n = 3438) | (n = 1002) | (n = 965) | (n = 277) | ||
| Age (years), mean (SE) | 73.1 (0.1) | 72.3 (0.2) | 71.5 (0.2) | 71.3 (0.4) | <0.001 |
| Sex | 0.13 | ||||
| Men | 44.1 | 40.6 | 42.3 | 47.2 | |
| Women | 55.9 | 59.4 | 57.7 | 252.7 | |
| Weight status | <0.001 | ||||
| Normal | 25.6 | 21.8 | 18.3 | 45.3 | |
| Overweight | 38.2 | 31.4 | 41.1 | 30.9 | |
| Obesity | 36.2 | 46.8 | 40.6 | 23.8 | |
| Education level | <0.001 | ||||
| Below high school | 17.1 | 38.5 | 56.6 | 21.2 | |
| High school | 26.4 | 24.2 | 15.9 | 22.0 | |
| Higher than high school | 56.5 | 37.3 | 27.5 | 56.8 | |
| Annual household income | <0.001 | ||||
| <$25,000 | 25.6 | 44.5 | 50.5 | 30.2 | |
| $25,000 < $75,000 | 50.5 | 45.6 | 38.5 | 43.8 | |
| ≥$75,000 | 23.9 | 11.9 | 11.0 | 26.0 | |
| Leisure-time physical activity | <0.001 | ||||
| Inactive | 54.6 | 61.4 | 66.0 | 48.7 | |
| Active | 45.4 | 38.6 | 34.0 | 51.3 | |
| Smoking status | <0.001 | ||||
| Never | 47.6 | 47.6 | 53.6 | 52.9 | |
| Former | 45.4 | 38.7 | 35.5 | 35.0 | |
| Current | 7.0 | 13.7 | 10.9 | 12.1 | |
| Chronic conditions c | 0.419 | ||||
| No | 25.1 | 24.1 | 28.5 | 25.7 | |
| Yes | 74.9 | 75.9 | 71.5 | 74.3 | |
| Meeting recommended level of dietary magnesium intake | <0.001 | ||||
| No | 82.8 | 90.6 | 84.4 | 78.1 | |
| Yes | 17.2 | 9.4 | 15.6 | 21.9 | |
| Dietary magnesium intake (mg, day), mean (SE) | 276.4 (2.6) | 233.0 (4.4) | 260.8 (4.1) | 285.7 (8.9) | 0.028 |
| Total energy intake (kcal, day), mean (SE) | 1807.9 (12.9) | 1608.4 (25.9) | 1634.0 (25.6) | 1711.2 (44.5) | <0.001 |
| Beta-Coefficient (95% CI), p-Value a | ||||||
|---|---|---|---|---|---|---|
| Univariate | Age-Adjusted | Fully-Adjusted b | ||||
| Ethnicity | ||||||
| Caucasian | Reference | Reference | Reference | |||
| African American | −19.9 (−26.1 to −13.7) | <0.001 | −20.6 (−27.0 to −14.3) | <0.001 | −13.0 (−18.8 to −7.2) | <0.001 |
| Hispanic | 4.9 (−0.9 to 10.8) | 0.098 | 3.6 (−2.4 to 9.6) | 0.237 | 14.0 (7.5 to 20.5) | <0.001 |
| Other | 20.7 (6.7 to 34.8) | 0.004 | 19.3 (5.3 to 33.4) | 0.008 | 17.2 (3.8 to 30.5) | 0.012 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jackson, S.E.; Smith, L.; Grabovac, I.; Haider, S.; Demurtas, J.; López-Sánchez, G.F.; Soysal, P.; Redsell, S.; Isik, A.T.; Yang, L. Ethnic Differences in Magnesium Intake in U.S. Older Adults: Findings from NHANES 2005–2016. Nutrients 2018, 10, 1901. https://doi.org/10.3390/nu10121901
Jackson SE, Smith L, Grabovac I, Haider S, Demurtas J, López-Sánchez GF, Soysal P, Redsell S, Isik AT, Yang L. Ethnic Differences in Magnesium Intake in U.S. Older Adults: Findings from NHANES 2005–2016. Nutrients. 2018; 10(12):1901. https://doi.org/10.3390/nu10121901
Chicago/Turabian StyleJackson, Sarah E., Lee Smith, Igor Grabovac, Sandra Haider, Jacopo Demurtas, Guillermo F. López-Sánchez, Pinar Soysal, Sarah Redsell, Ahmet Turan Isik, and Lin Yang. 2018. "Ethnic Differences in Magnesium Intake in U.S. Older Adults: Findings from NHANES 2005–2016" Nutrients 10, no. 12: 1901. https://doi.org/10.3390/nu10121901
APA StyleJackson, S. E., Smith, L., Grabovac, I., Haider, S., Demurtas, J., López-Sánchez, G. F., Soysal, P., Redsell, S., Isik, A. T., & Yang, L. (2018). Ethnic Differences in Magnesium Intake in U.S. Older Adults: Findings from NHANES 2005–2016. Nutrients, 10(12), 1901. https://doi.org/10.3390/nu10121901