Body Composition Changes in Weight Loss: Strategies and Supplementation for Maintaining Lean Body Mass, a Brief Review


{kind=link}
{kind=link}
Abstract
1. Introduction
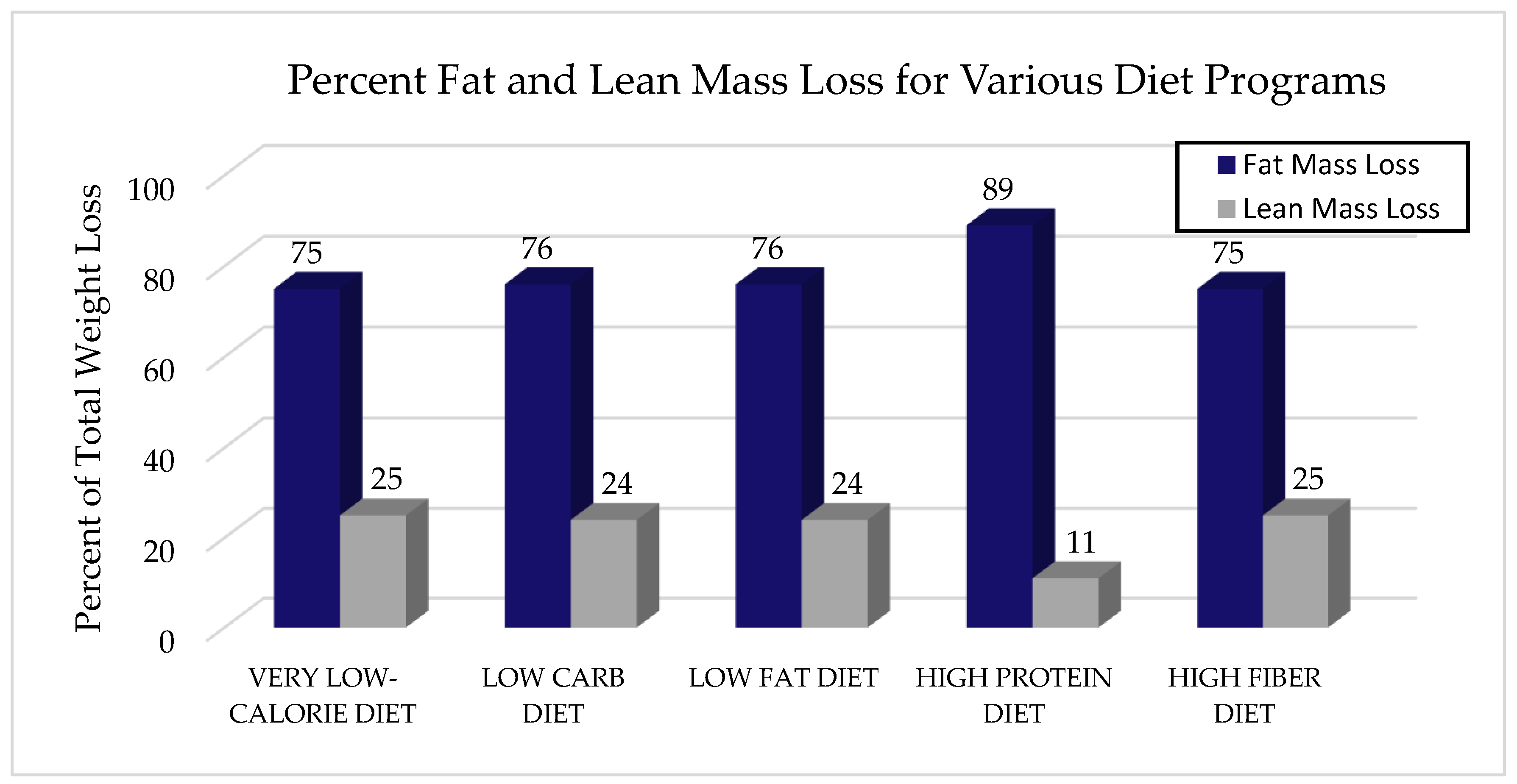
2. Weight Loss Strategies
2.1. Very Low-Calorie Diet
2.2. Ketogenic Diet
2.3. High Protein Diet
2.4. High Fiber Diet
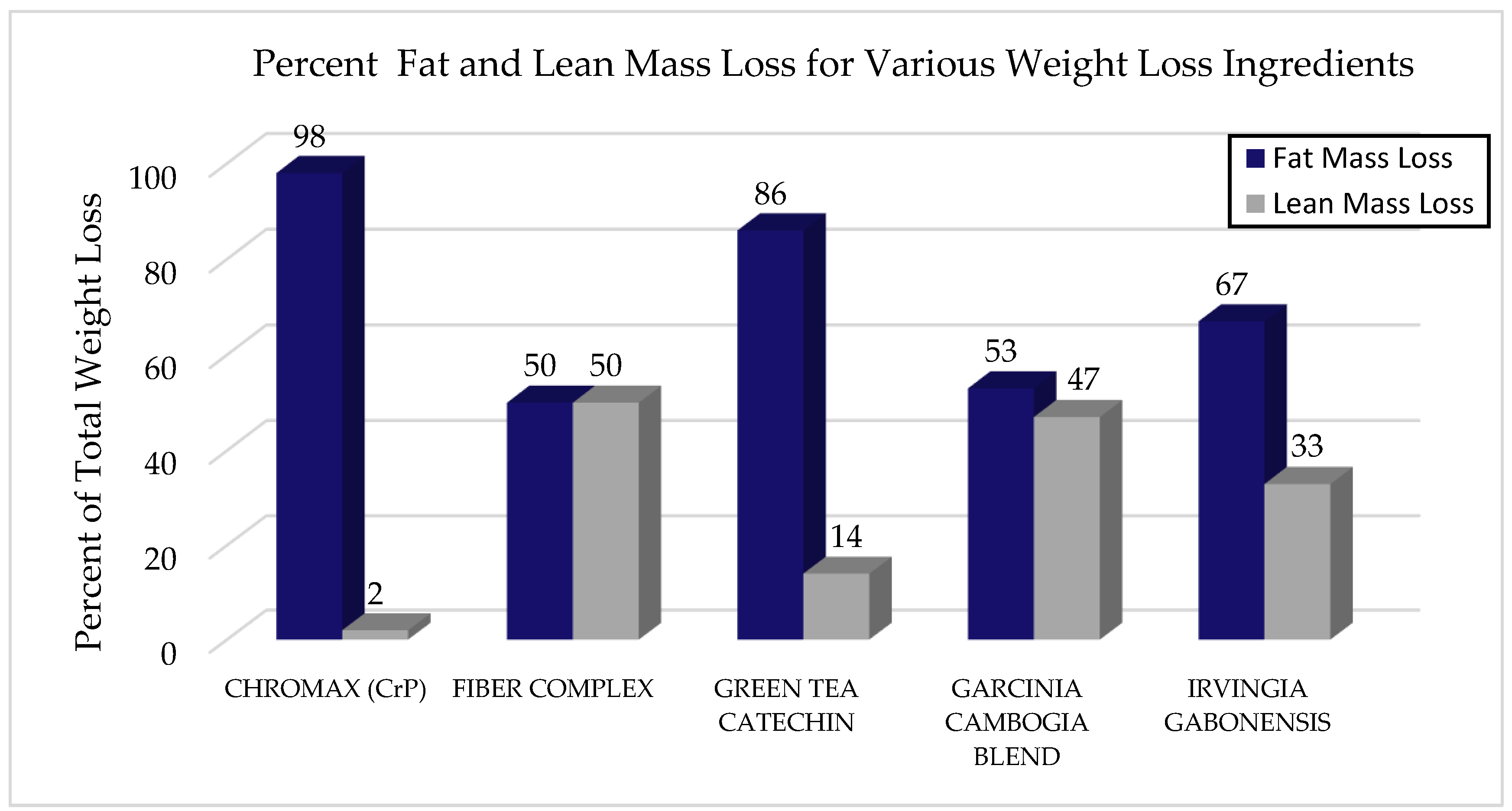
3. Dietary Supplements and Body Composition
3.1. Chromium Picolinate
3.2. Fiber Complex
3.3. Green Tea
3.4. Garcinia Cambogia
3.5. Irvingia Gabonensis
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ogden, C.L.; Carroll, M.D.; Fryar, C.D.; Flegal, K.M. Prevalence of obesity among adults and youth: United States, 2011–2014. NCHS data brief, No. 219; National Center for Health Statistics: Hyattsville, MD, USA, 2015.
- Stern, L.; Iqbal, N.; Seshadri, P.; Chicano, K.L.; Daily, D.A.; McGrory, J.; Williams, M.; Gracely, E.J.; Samaha, F.F. The effects of low-carbohydrate versus conventional weight loss diets in severely obese adults: One-year follow-up of a randomized trial. Ann. Intern. Med. 2004, 140, 778–785. [Google Scholar] [CrossRef] [PubMed]
- Forbes, G. Longitudinal changes in adult fat-free mass: Influence of body weight. Am. J. Clin. Nutr. 1999, 70, 1025–1031. [Google Scholar] [CrossRef] [PubMed]
- Tsai, A.; Wadden, T.A. Systematic review: An evaluation of major commercial weight loss programs in the United States. Ann. Intern. Med. 2005, 142, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Ravussin, E.; Lillioja, S.; Knowler, W.C.; Christin, L.; Freymond, D.; Abbott, W.G.; Boyce, V.; Howard, B.V.; Bogardus, C. Reduced rate of energy expenditure as a risk factor for body-weight gain. N. Engl. J. Med. 1988, 318, 467–472. [Google Scholar] [CrossRef] [PubMed]
- Dulloo, A.; Jacquet, J.; Montani, J.P. How dieting makes some fatter: From a perspective of human body composition autoregulation. Proc. Nutr. Soc. 2012, 71, 379–389. [Google Scholar] [CrossRef] [PubMed]
- Jo, E.; Worts, P.R.; Elam, M.L.; Brown, A.F.; Khamoui, A.V.; Kim, D.H.; Yeh, M.-C.; Ormsbee, M.J.; Prado, C.M.; Cain, A.; et al. Resistance training during a 12-week protein supplemented VLCD treatment enhances weight-loss outcomes in obese patients. Clin. Nutr. 2017. [Google Scholar] [CrossRef] [PubMed]
- Kaats, G.R.; Blum, K.; Fisher, J.A.; Adelman, J.A. Effects of chromium picolinate supplementation on body composition: A randomized, double-masked, placebo-controlled study. Curr. Ther. Res. 1996, 57, 747. [Google Scholar] [CrossRef]
- Anderson, R.A.; Kozlovsky, A.S. Chromium intake, absorption and excretion of subjects consuming self-selected diets. Am. J. Clin. Nutr. 1985, 41, 1177–1183. [Google Scholar] [CrossRef] [PubMed]
- McCarty, M.F. Homologous physiological effects of phenformin and chromium picolinate. Med. Hypotheses 1993, 41, 316–324. [Google Scholar] [CrossRef]
- Felig, P. Amino acid metabolism in man. Annu. Rev. Biochem. 1975, 44, 933–955. [Google Scholar] [CrossRef] [PubMed]
- Press, R.I.; Geller, J.; Evans, G.W. The effect of chromium picolinate on serum cholesterol and apolipoprotein fractions in human subjects. West. J. Med. 1990, 152, 41–45. [Google Scholar] [PubMed]
- Tian, H.; Guo, X.; Wang, X.; He, Z.; Sun, R.; Ge, S.; Zhang, Z. Chromium picolinate supplementation for overweight or obese adults. Cochrane Database Syst. Rev. 2013, 11. [Google Scholar] [CrossRef] [PubMed]
- Kaats, G.R.; Blum, K.; Pullin, D.; Keith, S.C.; Wood, R. A randomized, double-masked, placebo-controlled study of the effects of chromium picolinate supplementation on body composition: A replication and extension of a previous study. Curr. Ther. Res. 1998, 59, 379–388. [Google Scholar] [CrossRef]
- Aragon, A.A.; Schoenfeld, B.J.; Wildman, R.; Kleiner, S.; VanDusseldorp, T.; Taylor, L.; Earnest, C.P.; Arciero, P.J.; Wilborn, C.; Kalman, D.S.; et al. International society of sports nutrition position stand: Diets and body composition. J. Intern. Soc. Sports Nutr. 2017, 14, 16. [Google Scholar] [CrossRef] [PubMed]
- Hoie, L.H.; Bruusgaard, D.; Thom, E. Reduction of body mass and change in body composition on a very low calorie diet. Int. J. Obes. Relat. Metab. Disord. 1993, 17, 17–20. [Google Scholar] [PubMed]
- Frisch, S.; Zittermann, A.; Berthold, H.K.; Götting, C.; Kuhn, J.; Kleesiek, K.; Stehle, P.; Körtke, H. A randomized controlled trial on the efficacy of carbohydrate-reduced or fat-reduced diets in patients attending a telemedically guided weight loss program. Cardiovasc. Diabetol. 2009, 8, 36. [Google Scholar] [CrossRef] [PubMed]
- Burton-Freeman, B. Dietary fiber and energy regulation. J. Nutr. 2000, 130, 272S–275S. [Google Scholar] [CrossRef]
- Hall, K.D.; Chen, K.Y.; Guo, J.; Lam, Y.Y.; Leibel, R.L.; Mayer, L.E.S.; Reitman, M.L.; Rosenbaum, M.; Smith, S.R.; Walsh, B.T.; et al. Energy expenditure and body composition changes after an isocaloric ketogenic diet in overweight and obese men. Am. J. Clin. Nutr. 2016, 104, 324–333. [Google Scholar] [CrossRef]
- Gomez-Arbelaez, D.; Bellido, D.; Castro, A.I.; Ordoñez-Mayan, L.; Carreira, J.; Galban, C.; Martinez-Olmos, M.A.; Crujeiras, A.B.; Sajoux, I.; Casanueva, F.F. Body composition changes after very-low-calorie ketogenic diet in obesity evaluated by 3 standardized methods. J. Clin. Endocrinol. Metab. 2017, 102, 488–498. [Google Scholar] [CrossRef]
- Tinsley, G.M.; Willoughby, D.S. Fat-free mass changes during ketogenic diets and the potential role of resistance training. Int. J. Sport Nutr. Exerc. Metab. 2016, 26, 78–92. [Google Scholar] [CrossRef]
- Trumbo, P.; Schlicker, S.; Yates, A.A.; Poos, M. Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein and amino acids. J. Am. Diet. Assoc. 2002, 102, 1621–1630. [Google Scholar] [CrossRef]
- Hector, A.J.; Phillips, S.M. Protein recommendations for weight loss in elite athletes: A focus on body composition and performance. Int. J. Sport Nutr. Exerc. Metab. 2018, 28, 170–177. [Google Scholar] [CrossRef] [PubMed]
- Mettler, S.; Mitchell, N.; Tipton, K.D. Increased protein intake reduces lean body mass loss during weight loss in athletes. Med. Sci. Sports Exerc. 2010, 42, 326–337. [Google Scholar] [CrossRef]
- Longland, T.M.; Oikawa, S.Y.; Mitchell, C.J.; Devries, M.C.; Phillips, S.M. Higher compared with lower dietary protein during an energy deficit combined with intense exercise promotes greater lean mass gain and fat mass loss: A randomized trial. Am. J. Clin. Nutr. 2016, 103, 738–746. [Google Scholar] [CrossRef] [PubMed]
- Kerksick, C.; Thomas, A.; Campbell, B.; Taylor, L.; Wilborn, C.; Marcello, B.; Roberts, M.; Pfau, E.; Grimstvedt, M.; Opusunju, J.; et al. Effects of a popular exercise and weight loss program on weight loss, body composition, energy expenditure and health in obese women. Nutr. Metab. 2009, 6, 23. [Google Scholar] [CrossRef] [PubMed]
- Bachmann, C.; Faserkomplex, D. Ein Fasernkomplex zur Gewichts-reduktion und-kontrolle. Available online: https://www.rosenfluh.ch/arsmedici-thema-phytotherapie-2010-04-05/ein-fasernkomplex-zur-gewichtsreduktion-und-kontrolle (accessed on 5 November 2018).
- Morenga, L.A.; Levers, M.T.; Williams, S.M.; Rachel, C.; Brown, R.C.; Mann, J. Comparison of high protein and high fiber weight-loss diets in women with risk factors for the metabolic syndrome: A randomized trial. Nutr. J. 2011, 10, 40. [Google Scholar] [CrossRef]
- Chomentowski, P.; Dubé, J.J.; Amati, F.; Stefanovic-Racic, M.; Zhu, S.; Toledo, F.G.; Goodpaster, B.H. Moderate exercise attenuates the loss of skeletal muscle mass that occurs with intentional caloric restriction–induced weight loss in older, overweight to obese adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2009, 64, 575–580. [Google Scholar] [CrossRef]
- Miller, W.C.; Koceja, D.M.; Hamilton, E.J. A meta-analysis of the past 25 years of weight loss research using diet, exercise or diet plus exercise intervention. Int. J. Obes. 1997, 21, 941–947. [Google Scholar] [CrossRef]
- Evans, G.W. The effect of chromium picolinate on insulin controlled parameters in humans. Int. J. Biosoc. Med. Res. 1989, 11, 163–180. [Google Scholar]
- Kristensen, M.; Jensen, M.G. Dietary fibres in the regulation of food intake. Importance of viscosity. Appetite 2011, 56, 65–70. [Google Scholar] [CrossRef]
- Grube, B.; Chong, P.W.; Alt, F.; Uebelhack, R. Weight maintenance with Litramine (IQP-G-002AS): A 24-week double-blind, randomized, placebo-controlled study. J. Obes. 2015, 9531–9538. [Google Scholar] [CrossRef] [PubMed]
- Semwal, R.B.; Semwal, D.K.; Vermaak, I.; Vilijoen, A. A comprehensive scientific overview of Garcinia cambogia. Fitoterapia 2015, 102, 134–148. [Google Scholar] [CrossRef] [PubMed]
- Suksomboon, N.; Poolsup, N.; Yuwanakorn, A. Systematic review and meta-analysis of the efficacy and safety of chromium supplementation in diabetes. J. Clin. Pharm. Ther. 2014, 39, 292–306. [Google Scholar] [CrossRef] [PubMed]
- Eckerson, J.M. Weight Loss Nutritional Supplements. In Nutritional Supplements in Sports and Exercise, 2nd ed.; Greenwood, M., Cooke, M., Eds.; Springer: Basel, Sitzerland, 2015; pp. 159–185. [Google Scholar]
- Bhadori, B.; Wallner, S.; Schneider, H.; Wascher, T.C.; Toplak, H. Effect of chromium yeast and chromium picolinate on body composition of obese, non-diabetic patients during and after a formula diet. Acta Med. Austriaca 1997, 24, 185–187. [Google Scholar]
- Bulbulian, R.; Pringle, D.D.; Liddy, M.S. Chromium picolinate supplementation in male and female swimmers. Med. Sci. Sports Exerc. 1996, 28, 111. [Google Scholar] [CrossRef]
- Grube, B.; Chong, P.W.; Lau, K.Z.; Orzechowski, H.-D. A natural fiber complex reduces body weight in the overweight and obese: A double-blind, randomized, placebo-controlled study. Obesity 2013, 21, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Wen, Y.; Du, Y.; Yan, X.; Guo, H.; Rycroft, J.A.; Boon, N.; Kovacs, E.M.R.; Mela, D.J. Effects of catechin enriched green tea on body composition. Obesity 2010, 18, 773–779. [Google Scholar] [CrossRef]
- Maki, K.C.; Reeves, M.S.; Farmer, M.; Yasunaga, K.; Matsuo, N.; Katsuragi, Y.; Komikado, M.; Tokimitsu, I.; Wilder, D.; Jones, F.; et al. Green tea catechin consumption enhances exercise-induced abdominal fat loss in overweight and obese adults. J. Nutr. 2009, 139, 264–270. [Google Scholar] [CrossRef]
- Ohia, S.E.; Opere, C.A.; LeDay, A.M.; Bagchi, M.; Bagchi, D.; Stohs, S.J. Safety and mechanism of appetite suppression by a novel hydroxycitric acid extract (HCA-SX). Mol. Cell. Biol. 2002, 238, 89–103. [Google Scholar]
- Chong, P.W.; Beah, Z.M.; Grube, B.; Riede, L. IQP-GC-101 reduces body weight and body fat mass: A randomized, double-blind, placebo controlled study. Phytother. Res. 2014, 28, 1520–1526. [Google Scholar] [CrossRef]
- Adamson, I.; Okafor, C.; Abu-Bakare, A. A supplement of Dikanut (Irvingia gabonensis) improves treatment of type II diabetics. West Afr. J. Med. 1990, 9, 108–115. [Google Scholar] [PubMed]
- Oben, J.; Ngondi, J.L.; Blum, K. Inhibition of Irvingia gabonensis seed extract (OB 131) on adipogenesis as mediated via down regulation of PPAR and Leptin genes and up-regulation of the adiponectin gene. Lipids Health Dis. 2008, 7, 44. [Google Scholar] [CrossRef] [PubMed]
- Ross, S.M. African mango (IGOB131): A proprietary seed extract of Irvingia gabonensis is found to be effective in reducing body weight and improving metabolic parameters in overweight humans. Holist. Nurs. Pract. 2011, 25, 215–217. [Google Scholar] [CrossRef] [PubMed]
- Egras, A.M.; Hamilton, W.R.; Lenz, T.L.; Monaghan, M.S. An evidence-based review of fat modifying supplemental weight loss products. J. Obes. 2011, 2011. [Google Scholar] [CrossRef] [PubMed]
- Onakpoya, I.; Davies, L.; Posadzki, P.; Ernst, E. The efficacy of irvingia gabonensis supplementation in the management of overweight and obesity: A systematic review of randomized controlled trials. J. Diet. Suppl. 2013, 10, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Ngondi, J.L.; Oben, J.E.; Minka, S.R. The effect of Irvingia gabonensis seeds on body weight and blood lipids of obese subjects in Cameroon. Lipids Health Dis. 2005, 4, 12. [Google Scholar] [CrossRef] [PubMed]


© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Willoughby, D.; Hewlings, S.; Kalman, D. Body Composition Changes in Weight Loss: Strategies and Supplementation for Maintaining Lean Body Mass, a Brief Review. Nutrients 2018, 10, 1876. https://doi.org/10.3390/nu10121876
Willoughby D, Hewlings S, Kalman D. Body Composition Changes in Weight Loss: Strategies and Supplementation for Maintaining Lean Body Mass, a Brief Review. Nutrients. 2018; 10(12):1876. https://doi.org/10.3390/nu10121876
Chicago/Turabian StyleWilloughby, Darryn, Susan Hewlings, and Douglas Kalman. 2018. "Body Composition Changes in Weight Loss: Strategies and Supplementation for Maintaining Lean Body Mass, a Brief Review" Nutrients 10, no. 12: 1876. https://doi.org/10.3390/nu10121876
APA StyleWilloughby, D., Hewlings, S., & Kalman, D. (2018). Body Composition Changes in Weight Loss: Strategies and Supplementation for Maintaining Lean Body Mass, a Brief Review. Nutrients, 10(12), 1876. https://doi.org/10.3390/nu10121876