

Worries About Air Pollution from the Unsustainable Use of Studded Tires and Cruise Ships—A Preliminary Study on the Relationship Between Worries and Health Complaints Due to Seasonal Pollution

 ,
,  , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Collection
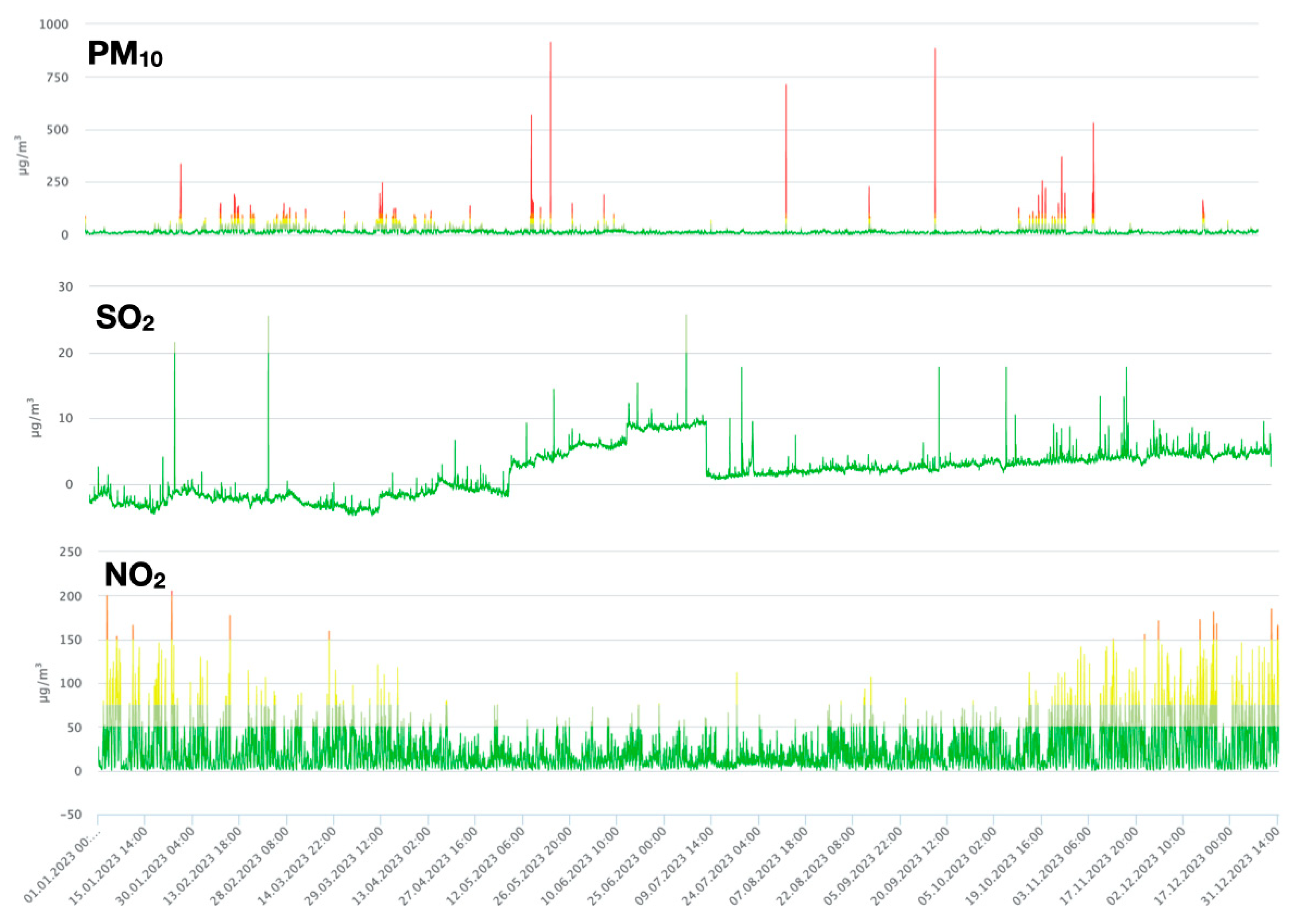
2.2. Air Pollution Measurements in Recruitment Timeframe
2.3. Survey
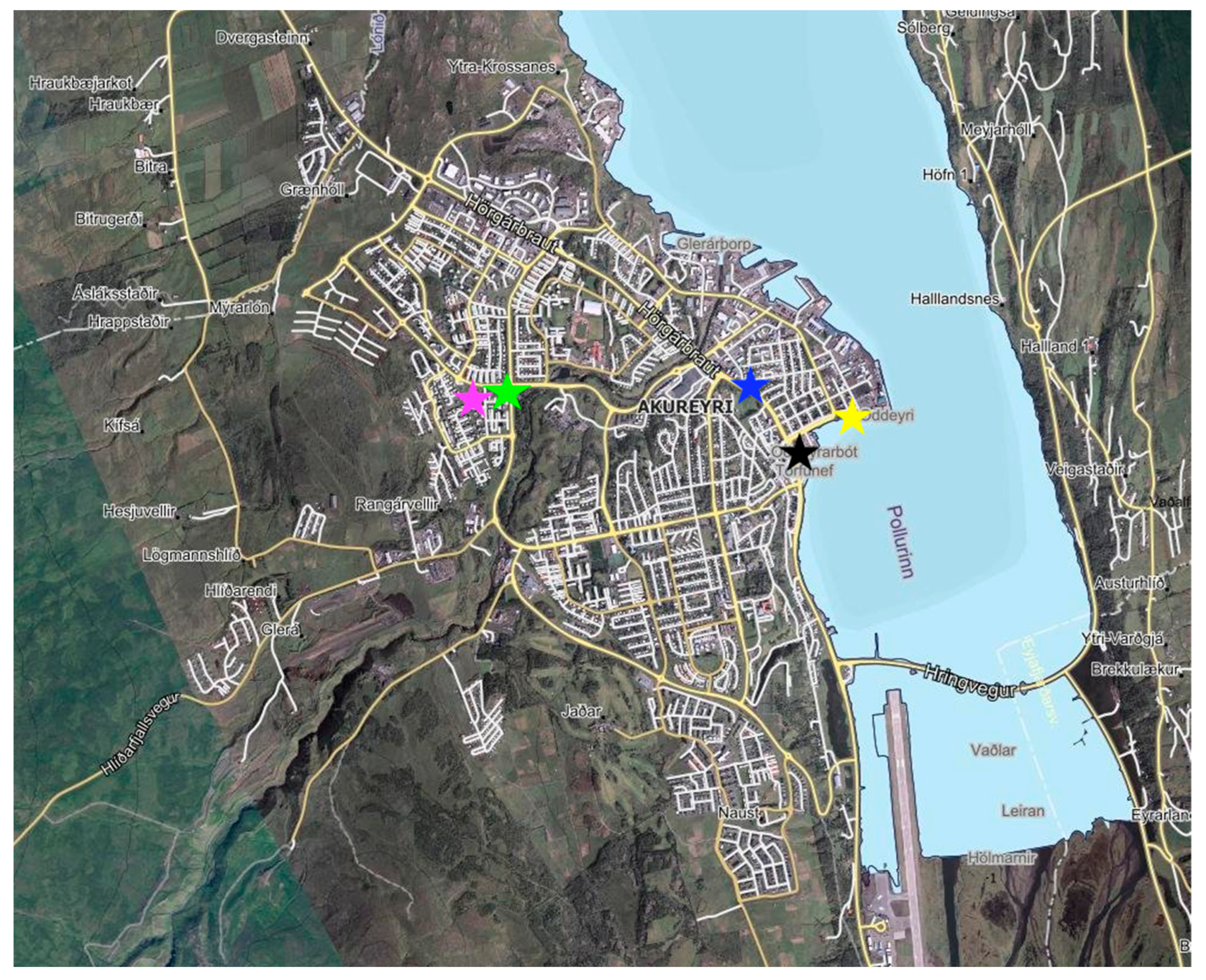
2.4. Neighborhood Analysis
2.5. Statistical Analysis
3. Results
3.1. Sample
3.2. Air Pollution in Recruitment Timeframe
3.3. Health Complaints and Worries
3.4. Distance from Pollution Sources
4. Discussion
4.1. Worries About Air Pollution from Different Sources
4.2. Worries About Air Pollution and Their Relation to Mental Health Indicators
4.3. Seasonality of Air Pollution and Seasonal Variations in Health and Well-Being
4.4. Challenging Recruitment: Is It the Topic?
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AUDIT-C | Alcohol User Disorder Identification Test |
| BIS | Bergen insomnia scale |
| HEAS | Hogg eco-anxiety scale |
| HINTS | Health Information National Trends Survey |
| NO2 | nitrogen oxide |
| PM | particulate matter |
| SO2 | sulphur dioxide |
| SPAQ | Seasonal Pattern Assessment Questionnaire |
| WHO | World Health Organization |
References
- Cohen, A.J.; Brauer, M.; Burnett, R.; Anderson, H.R.; Frostad, J.; Estep, K.; Balakrishnan, K.; Brunekreef, B.; Dandona, L.; Dandona, R.; et al. Estimates and 25-Year Trends of the Global Burden of Disease Attributable to Ambient Air Pollution: An Analysis of Data from the Global Burden of Diseases Study 2015. Lancet 2017, 389, 1907–1918. [Google Scholar] [CrossRef]
- Fuller, R.; Landrigan, P.J.; Balakrishnan, K.; Bathan, G.; Bose-O’Reilly, S.; Brauer, M.; Caravanos, J.; Chiles, T.; Cohen, A.; Corra, L.; et al. Pollution and Health: A Progress Update. Lancet Planet. Health 2022, 6, e535–e547. [Google Scholar] [CrossRef] [PubMed]
- Kelly, F.J.; Fussell, J.C. Size, Source and Chemical Composition as Determinants of Toxicity Attributable to Ambient Particulate Matter. Atmos. Environ. 2012, 60, 504–526. [Google Scholar] [CrossRef]
- Harrison, R.M.; Yin, J. Particulate Matter in the Atmosphere: Which Particle Properties are Important for its Effects on Health? Sci. Total Environ. 2000, 249, 85–101. [Google Scholar] [CrossRef]
- Cori, L.; Donzelli, G.; Gorini, F.; Bianchi, F.; Curzio, O. Risk Perception of Air Pollution: A Systematic Review Focused on Particulate Matter Exposure. Int. J. Environ. Res. Public Health 2020, 17, 6424. [Google Scholar] [CrossRef]
- Li, J.; Li, W.X.; Bai, C.; Song, Y. Particulate Matter-induced Epigenetic Changes and Lung Cancer. Clin. Respir. J. 2017, 11, 539–546. [Google Scholar] [CrossRef] [PubMed]
- Riedl, M.A. The Effect of Air Pollution on Asthma and Allergy. Curr. Allergy Asthma Rep. 2008, 8, 139–146. [Google Scholar] [CrossRef]
- Kim, K.; Jahan, S.A.; Kabir, E. A Review on Human Health Perspective of Air Pollution with Respect to Allergies and Asthma. Environ. Int. 2013, 59, 41–52. [Google Scholar] [CrossRef]
- Sabour, S.; Harzand-Jadidi, S.; Jafari-Khounigh, A.; Zarea Gavgani, V.; Sedaghat, Z.; Alavi, N. The Association between Ambient Air Pollution and Migraine: A Systematic Review. Environ. Monit. Assess. 2024, 196, 271. [Google Scholar] [CrossRef]
- Thompson, J. Airborne Particulate Matter: Human Exposure and Health Effects. J. Occup. Environ. Med. 2018, 60, 392–423. [Google Scholar] [CrossRef]
- Mills, N.L.; Donaldson, K.; Hadoke, P.W.; Boon, N.A.; MacNee, W.; Cassee, F.R.; Sandström, T.; Blomberg, A.; Newby, D.E. Adverse Cardiovascular Effects of Air Pollution. Nat. Clin. Pract. Cardiovasc. Med. 2009, 6, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Fiordelisi, A.; Piscitelli, P.; Trimarco, B.; Coscioni, E.; Iaccarino, G.; Sorriento, D. The Mechanisms of Air Pollution and Particulate Matter in Cardiovascular Diseases. Heart Fail. Rev. 2017, 22, 337–347. [Google Scholar] [CrossRef]
- Lisabeth, L.D.; Escobar, J.D.; Dvonch, J.T.; Sánchez, B.N.; Majersik, J.J.; Brown, D.L.; Smith, M.A.; Morgenstern, L.B. Ambient Air Pollution and Risk for Ischemic Stroke and Transient Ischemic Attack. Ann. Neurol. 2008, 64, 53–59. [Google Scholar] [CrossRef]
- Block, M.L.; Calderón-Garcidueñas, L. Air Pollution: Mechanisms of Neuroinflammation and CNS Disease. Trends Neurosci. 2009, 32, 506–516. [Google Scholar] [CrossRef]
- Shi, L.; Wu, X.; Danesh Yazdi, M.; Braun, D.; Abu Awad, Y.; Wei, Y.; Liu, P.; Di, Q.; Wang, Y.; Schwartz, J.; et al. Long-Term Effects of PM2.5 on Neurological Disorders in the American Medicare Population: A Longitudinal Cohort Study. Lancet Planet. Health 2020, 4, e557–e565. [Google Scholar] [CrossRef]
- Buoli, M.; Grassi, S.; Caldiroli, A.; Carnevali, G.S.; Mucci, F.; Iodice, S.; Cantone, L.; Pergoli, L.; Bollati, V. Is there a Link between Air Pollution and Mental Disorders? Environ. Int. 2018, 118, 154–168. [Google Scholar] [CrossRef] [PubMed]
- Shim, J.; Byun, G.; Lee, J. Exposure to Particulate Matter as a Potential Risk Factor for Attention-Deficit/Hyperactivity Disorder in Korean Children and Adolescents (KNHANES 2008–2018). Int. J. Environ. Res. Public health 2022, 19, 13966. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Sohn, J.H.; Cho, S.J.; Seo, H.Y.; Hwang, I.; Hong, Y.; Kim, K. Association between Short-Term Air Pollution Exposure and Attention-Deficit/Hyperactivity Disorder-Related Hospital Admissions among Adolescents: A Nationwide Time-Series Study. Environ. Pollut. (1987) 2020, 266, 115369. [Google Scholar] [CrossRef]
- Zhang, Z.; Zhao, D.; Hong, Y.S.; Chang, Y.; Ryu, S.; Kang, D.; Monteiro, J.; Shin, H.C.; Guallar, E.; Cho, J. Long-Term Particulate Matter Exposure and Onset of Depression in Middle-Aged Men and Women. Environ. Health Perspect. 2019, 127, 77001. [Google Scholar] [CrossRef]
- Braithwaite, I.; Zhang, S.; Kirkbride, J.B.; Osborn, D.P.J.; Hayes, J.F. Air Pollution (Particulate Matter) Exposure and Associations with Depression, Anxiety, Bipolar, Psychosis and Suicide Risk: A Systematic Review and Meta-Analysis. Environ. Health Perspect. 2019, 127, 126002. [Google Scholar] [CrossRef]
- Yue, J.; Liu, H.; Li, H.; Liu, J.; Hu, Y.; Wang, J.; Lu, L.; Wang, F. Association between Ambient Particulate Matter and Hospitalization for Anxiety in China: A Multicity Case-Crossover Study. Int. J. Hyg. Environ. Health 2020, 223, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Hwang, I.Y.; Choi, D.; Kim, J.A.; Choi, S.; Chang, J.; Goo, A.J.; Ko, A.; Lee, G.; Kim, K.H.; Son, J.S.; et al. Association of Short-Term Particulate Matter Exposure with Suicide Death among Major Depressive Disorder Patients: A Time-Stratified Case-Crossover Analysis. Sci. Rep. 2022, 12, 8471. [Google Scholar] [CrossRef]
- Chirico, F.; Magnavita, N. Letter to the Editor (January 1, 2019) Concerning the Paper “Impact of Air Pollution on Depression and Suicide”. Int. J. Occup. Med. Environ. Health 2019, 32, 413–414. [Google Scholar] [CrossRef] [PubMed]
- Gładka, A.; Rymaszewska, J.; Zatoński, T. Impact of Air Pollution on Depression and Suicide. Int. J. Occup. Med. Environ. Health 2018, 31, 711–721. [Google Scholar] [CrossRef] [PubMed]
- Zanobetti, A.; Redline, S.; Schwartz, J.; Rosen, D.; Patel, S.; O’Connor, G.T.; Lebowitz, M.; Coull, B.A.; Gold, D.R. Associations of PM10 with Sleep and Sleep-Disordered Breathing in Adults from Seven U.S. Urban Areas. Am. J. Respir. Crit. Care medicine 2010, 182, 819–825. [Google Scholar] [CrossRef]
- Yu, H.; Chen, P.; Paige Gordon, S.; Yu, M.; Wang, Y. The Association between Air Pollution and Sleep Duration: A Cohort Study of Freshmen at a University in Beijing, China. Int. J. Environ. Res. Public Health 2019, 16, 3362. [Google Scholar] [CrossRef]
- Abou-khadra, M. Association between PM^sub 10^ Exposure and Sleep of Egyptian School Children. Sleep Breath. 2013, 17, 653. [Google Scholar] [CrossRef]
- Xu, J.; Zhou, J.; Luo, P.; Mao, D.; Xu, W.; Nima, Q.; Cui, C.; Yang, S.; Ao, L.; Wu, J.; et al. Associations of Long-Term Exposure to Ambient Air Pollution and Physical Activity with Insomnia in Chinese Adults. Sci. Total Environ. 2021, 792, 148197. [Google Scholar] [CrossRef]
- Tiseo, C.; Vacca, A.; Felbush, A.; Filimonova, T.; Gai, A.; Glazyrina, T.; Hubalek, I.A.; Marchenko, Y.; Overeem, L.H.; Piroso, S.; et al. Migraine and Sleep Disorders: A Systematic Review. J. Headache Pain 2020, 21, 126. [Google Scholar] [CrossRef]
- Zhou, F.; Li, S.; Xu, H. Insomnia, Sleep Duration, and Risk of Anxiety: A Two-Sample Mendelian Randomization Study. J. Psychiatr. Res. 2022, 155, 219–225. [Google Scholar] [CrossRef]
- Riemann, D.; Krone, L.B.; Wulff, K.; Nissen, C. Sleep, Insomnia, and Depression. Neuropsychopharmacology 2020, 45, 74–89. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Wu, C.; Gan, Y.; Qu, X.; Lu, Z. Insomnia and the Risk of Depression: A Meta-Analysis of Prospective Cohort Studies. BMC Psychiatry 2016, 16, 375. [Google Scholar] [CrossRef] [PubMed]
- Baglioni, C.; Battagliese, G.; Feige, B.; Spiegelhalder, K.; Nissen, C.; Voderholzer, U.; Lombardo, C.; Riemann, D. Insomnia as a Predictor of Depression: A Meta-Analytic Evaluation of Longitudinal Epidemiological Studies. J. Affect. Disord. 2011, 135, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Bai, K.; Chuang, K.; Chen, C.; Jhan, M.; Hsiao, T.; Cheng, T.; Chang, L.; Chang, T.; Chuang, H. Microglial Activation and Inflammation Caused by Traffic-Related Particulate Matter. Chem.-Biol. Interact. 2019, 311, 108762. [Google Scholar] [CrossRef]
- Kafu-Quvane, B.; Mlaba, S. Assessing the Impact of Quarrying as an Environmental Ethic Crisis: A Case Study of Limestone Mining in a Rural Community. Int. J. Environ. Res. Public health 2024, 21, 458. [Google Scholar] [CrossRef]
- Ammons, S.; Aja, H.; Ghazarian, A.A.; Lai, G.Y.; Ellison, G.L. Perception of Worry of Harm from Air Pollution: Results from the Health Information National Trends Survey (HINTS). BMC Public Health 2022, 22, 1–1254. [Google Scholar] [CrossRef]
- Boluda-Verdú, I.; Senent-Valero, M.; Casas-Escolano, M.; Matijasevich, A.; Pastor-Valero, M. Fear for the Future: Eco-Anxiety and Health Implications, a Systematic Review. J. Environ. Psychol. 2022, 84, 101904. [Google Scholar] [CrossRef]
- Bellani, L.; Ceolotto, S.; Elsner, B.; Pestel, N. The Political Fallout of Air Pollution. Proc. Natl. Acad. Sci. USA 2024, 121, e2314428121. [Google Scholar] [CrossRef]
- Celic, J.; Valcic, S.; Bistrovic, M. Air Pollution from Cruise Ships. In Proceedings of the Proceedings ELMAR-2014, Zadar, Croatia, 10–12 September 2014; pp. 1–4. [Google Scholar] [CrossRef]
- Poplawski, K.; Setton, E.; McEwen, B.; Hrebenyk, D.; Graham, M.; Keller, P. Impact of Cruise Ship Emissions in Victoria, BC, Canada. Atmos. Environ. (1994) 2011, 45, 824–833. [Google Scholar] [CrossRef]
- Simonsen, M.; Gössling, S.; Walnum, H.J. Cruise Ship Emissions in Norwegian Waters: A Geographical Analysis. J. Transp. Geogr. 2019, 78, 87–97. [Google Scholar] [CrossRef]
- Lloret, J.; Carreño, A.; Carić, H.; San, J.; Fleming, L.E. Environmental and Human Health Impacts of Cruise Tourism: A Review. Mar. Pollut. Bull. 2021, 173, 112979. [Google Scholar] [CrossRef]
- Johansson, C.; Norman, M.; Gidhagen, L. Spatial & Temporal Variations of PM10 and Particle Number Concentrations in Urban Air. Environ. Monit. Assess. 2007, 127, 477–487. [Google Scholar] [PubMed]
- Furberg, A.; Arvidsson, R.; Molander, S. Live and Let Die? Life Cycle Human Health Impacts from the use of Tire Studs. Int. J. Environ. Res. Public Health 2018, 15, 1774. [Google Scholar] [CrossRef] [PubMed]
- Guðmundsson, G.; Finnbjörnsdóttir, R.G.; Jóhannsson, Þ.; Rafnsson, V. Loftmengun Á Íslandi Og Áhrif Hennar Á Heilsu Manna. Laeknabladid 2019, 2019, 443–452. [Google Scholar] [CrossRef]
- Fridriksson, J.; Wise, N.; Scott, P. Iceland’s Bourgeoning Cruise Industry: An Economic Opportunity or a Local Threat? Local Econ. 2020, 35, 143–154. [Google Scholar] [CrossRef]
- Environmental Agency Iceland. Air Quality Information System Iceland; Environmental Agency Iceland: Reykjavik, Iceland, 2024. [Google Scholar]
- Icelandic Tourist Board. Skemmtiferðaskip; Icelandic Tourist Board: Reykjavik, Iceland, 2023. [Google Scholar]
- Harbour Akureyri. Cruise Ships Arrivals Table Akureyri; Harbour Akureyri: Akureyri, Iceland, 2024. [Google Scholar]
- Waters, A.R.; Warner, E.L.; Vaca Lopez, P.L.; Kirchhoff, A.C.; Ou, J.Y. Perceptions and Knowledge of Air Pollution and its Health Effects among Caregivers of Childhood Cancer Survivors: A Qualitative Study. BMC Cancer 2021, 21, 1070. [Google Scholar] [CrossRef]
- Chen, Y.; Liu, X. Determinants of Beijing Residents’ Intentions to Take Protective Behaviors Against Smog: An Application of the Health Belief Model. Health Commun. 2023, 38, 447–459. [Google Scholar] [CrossRef]
- D’Antoni, D.; Auyeung, V.; Walton, H.; Fuller, G.W.; Grieve, A.; Weinman, J. The Effect of Evidence and Theory-Based Health Advice Accompanying Smartphone Air Quality Alerts on Adherence to Preventative Recommendations during Poor Air Quality Days: A Randomised Controlled Trial. Environ. Int. 2019, 124, 216–235. [Google Scholar] [CrossRef] [PubMed]
- Kheirbek, I.; Haney, J.; Douglas, S.; Ito, K.; Caputo, S.; Matte, T. The Public Health Benefits of Reducing Fine Particulate Matter through Conversion to Cleaner Heating Fuels in New York City. Environ. Sci. Technol. 2014, 48, 13573–13582. [Google Scholar] [CrossRef]
- Bush, K.; Kivlahan, D.R.; McDonell, M.B.; Fihn, S.D.; Bradley, K.A. The AUDIT Alcohol Consumption Questions (AUDIT-C): An Effective Brief Screening Test for Problem Drinking. Arch. Intern. Med. 1998, 158, 1789–1795. [Google Scholar] [CrossRef]
- Rosenthal, N.E. Seasonal Pattern Assessment Questionnaire (SPAQ). 1987. Available online: https://med-fom-ubcsad.sites.olt.ubc.ca/files/2013/11/SPAQ-SAD.pdf (accessed on 14 March 2025).
- Magnusson, A. Validation of the Seasonal Pattern Assessment Questionnaire (SPAQ). J. Affect. Disord. 1996, 40, 121–129. [Google Scholar] [CrossRef]
- Pallesen, S.; Bjorvatn, B.; Nordhus, I.H.; Sivertsen, B.; Hjørnevik, M.; Morin, C.M. A New Scale for Measuring Insomnia: The Bergen Insomnia Scale. Percept. Mot. Ski. 2008, 107, 691–706. [Google Scholar] [CrossRef]
- Höller, Y.; Gudjónsdottir, B.E.; Valgeirsdóttir, S.K.; Heimisson, G.T. The Effect of Age and Chronotype on Seasonality, Sleep Problems, and Mood. Psychiatry Res. 2021, 297, 113722. [Google Scholar] [CrossRef] [PubMed]
- Lipton, R.B.; Dodick, D.; Sadovsky, R.; Kolodner, K.; Endicott, J.; Hettiarachchi, J.; Harrison, W. A Self-Administered Screener for Migraine in Primary Care: The ID Migraine Validation Study. Neurology 2003, 61, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Hogg, T.L.; Stanley, S.K.; O’Brien, L.V.; Wilson, M.S.; Watsford, C.R. The Hogg Eco-Anxiety Scale: Development and Validation of a Multidimensional Scale. Glob. Environ. Change 2021, 71, 102391. [Google Scholar] [CrossRef]
- World Health Organization. WHO Global Air Quality Guidelines: Particulate Matter (PM2.5 and PM10), Ozone, Nitrogen Dioxide, Sulfur Dioxide and Carbon Monoxide; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Bergstra, A.D.; Brunekreef, B.; Burdorf, A. The Mediating Role of Risk Perception in the Association between Industry-Related Air Pollution and Health. PLoS ONE 2018, 13, e0196783. [Google Scholar] [CrossRef]
- United States Environmental Protection Agency; Office of Air and Radiation; U.S. Consumer Product Safety Commission. The Inside Story: A Guide to Indoor Air Quality. Available online: https://www.epa.gov/indoor-air-quality-iaq/inside-story-guide-indoor-air-quality (accessed on 14 March 2025).
- Óskarsson, F.; St. Ásgeirsdóttir, R. Radon in Icelandic Cold Groundwater and Low-Temperature Geothermal Water. Procedia Earth Planet. Sci. 2017, 17, 229–232. [Google Scholar] [CrossRef]
- Statistics Iceland, H.I. Iceland among Countries with Fewest Smokers; Statistics Iceland: Reykjavik, Iceland, 2017. [Google Scholar]
- Sigurjónsson, B.Þ. The Relationship between Housing Dampness and Mold and Self-Assessed Health. Master’s Thesis, Health Economics at the Faculty of Economics, School of Social Sciences, University of Iceland, Reykjavik, Iceland, 2016. [Google Scholar]
- Carlsen, H.K.; Ilyinskaya, E.; Baxter, P.J.; Schmidt, A.; Thorsteinsson, T.; Pfeffer, M.A.; Barsotti, S.; Dominici, F.; Finnbjornsdottir, R.G.; Jóhannsson, T.; et al. Increased Respiratory Morbidity Associated with Exposure to a Mature Volcanic Plume from a Large Icelandic Fissure Eruption. Nat. Commun. 2021, 12, 2161. [Google Scholar] [CrossRef]
- Kaufman, A.R.; Twesten, J.E.; Suls, J.; McCaul, K.D.; Ostroff, J.S.; Ferrer, R.A.; Brewer, N.T.; Cameron, L.D.; Halpern-Felsher, B.; Hay, J.L.; et al. Measuring Cigarette Smoking Risk Perceptions. Nicotine Tob. Res. 2020, 22, 1937–1945. [Google Scholar] [CrossRef]
- Do, E.K.; Fallavollita, W.L.; Bonat, B.; Fugate-Laus, K.; Rossi, B.C.; Fuemmeler, B.F. Student Attitudes Toward Tobacco use and Tobacco Policies on College Campuses. J. Community Health 2020, 45, 751–760. [Google Scholar] [CrossRef]
- Gany, F.; Bari, S.; Prasad, L.; Leng, J.; Lee, T.; Thurston, G.D.; Gordon, T.; Acharya, S.; Zelikoff, J.T. Perception and Reality of Particulate Matter Exposure in New York City Taxi Drivers. J. Expo. Sci. Environ. Epidemiol. 2017, 27, 221–226. [Google Scholar] [CrossRef]
- Reames, T.G.; Bravo, M.A. People, Place and Pollution: Investigating Relationships between Air Quality Perceptions, Health Concerns, Exposure, and Individual- and Area-Level Characteristics. Environ. Int. 2019, 122, 244–255. [Google Scholar] [CrossRef]
- Nikolopoulou, M.; Kleissl, J.; Linden, P.F.; Lykoudis, S. Pedestrians’ Perception of Environmental Stimuli through Field Surveys: Focus on Particulate Pollution. Sci. Total Environ. 2011, 409, 2493–2502. [Google Scholar] [CrossRef] [PubMed]
- Tilt, B. Perceptions of Risk from Industrial Pollution in China: A Comparison of Occupational Groups. Hum. Organ. 2006, 65, 115–127. [Google Scholar] [CrossRef]
- Félag Íslenskra Bifreiðaeigenda. Vetrardekkja Könnun FÍB; Félag Íslenskra Bifreiðaeigenda: Reykjavik, Iceland, 2021. [Google Scholar]
- Brody, S.D.; Peck, B.M.; Highfield, W.E. Examining Localized Patterns of Air Quality Perception in Texas: A Spatial and Statistical Analysis. Risk Anal. 2004, 24, 1561–1574. [Google Scholar] [CrossRef]
- Boso, À.; Álvarez, B.; Oltra, C.; Garrido, J.; Muñoz, C.; Hofflinger, Á. Out of Sight, Out of Mind: Participatory Sensing for Monitoring Indoor Air Quality. Environ. Monit. Assess. 2020, 192, 104. [Google Scholar] [CrossRef]
- Christodoulou, N.; Laaidi, K.; Geoffroy, P.A. Eco-Anxiety: Towards a Medical Model and the New Framework of Ecolalgia. Bipolar Disord. 2024, 26, 532–547. [Google Scholar] [CrossRef]
- Muthuraman, K.; Sankaran, A.; Subramanian, K. Association between Sleep-Related Cognitions, Sleep-Related Behaviors, and Insomnia in Patients with Anxiety and Depression: A Cross-Sectional Study. Indian J. Psychol. Med. 2024, 46, 228–237. [Google Scholar] [CrossRef]
- Olatunji, B.O.; Knowles, K.A.; Cox, R.C.; Cole, D.A. Linking Repetitive Negative Thinking and Insomnia Symptoms: A Longitudinal Trait-State Model. J. Anxiety Disord. 2023, 97, 102732. [Google Scholar] [CrossRef]
- Peres, M.F.P.; Mercante, J.P.P.; Tobo, P.R.; Kamei, H.; Bigal, M.E. Anxiety and Depression Symptoms and Migraine: A Symptom-Based Approach Research. J. Headache Pain 2017, 18, 37. [Google Scholar] [CrossRef] [PubMed]
- Han, L.; Wang, K.; Cheng, Y.; Du, Z.; Rosenthal, N.E.; Primeau, F. Summer and Winter Patterns of Seasonality in Chinese College Students: A Replication. Compr. Psychiatry 2000, 41, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, N.E.; Sack, D.A.; Gillin, J.C.; Lewy, A.J.; Goodwin, F.K.; Davenport, Y.; Mueller, P.S.; Newsome, D.A.; Wehr, T.A. Seasonal Affective Disorder: A Description of the Syndrome and Preliminary Findings with Light Therapy. Arch. Gen. Psychiatry 1984, 41, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Kasper, S.; Wehr, T.A.; Bartko, J.J.; Gaist, P.A.; Rosenthal, N.E. Epidemiological Findings of Seasonal Changes in Mood and Behavior: A Telephone Survey of Montgomery County, Maryland. Arch. Gen. Psychiatry 1989, 46, 823–833. [Google Scholar] [PubMed]
- Town of Reyjavík, I. Let’s Not use Studded Tires in Reykjavík. 2024. Available online: https://reykjavik.is/en/news/2023/lets-not-use-studded-tires-reykjavik (accessed on 14 March 2025).
- Ólafsson, Á. Rafrænn Teljari Fylgist Með Nagladekkjanotkun Á Akureyri [Digital Monitoring of the Use of Studded Tires in Akureyri]. ruv.is 2025. Available online: https://www.ruv.is/frettir/innlent/2025-04-09-rafraenn-teljari-fylgist-med-nagladekkjanotkun-a-akureyri-441115 (accessed on 14 March 2025).
- Hinriksdóttir; Rakel. Lögreglan: Stutt Í Sektir Fyrir Naglana [Police: Short Time Until Studded Tires Will be Fined]. 2025. Available online: https://www.akureyri.net/is/moya/news/logreglan-stutt-i-sektir-fyrir-naglana (accessed on 14 March 2025).
- Stefánsson, I. Hvetja Akureyringa Til Að Skipta Út Nagladekkjunum. [Motivate Inhabitants of Akureyri to Change Studded Tires]. kaffid.is 2021. Available online: https://www.kaffid.is/hvetja-akureyringa-til-ad-skipta-ut-nagladekkjunum/ (accessed on 14 March 2025).
- Jósefsdóttir, S.D. Akureyringar Ósáttir Við Reykmengun: Fólk Er Komið Með Nóg [“People in Akureyri Not Satisfied with Air Pollution: “People have had enough”]. visir.is 2023. Available online: https://www.visir.is/g/20232436675d/akureyringar-osattir-vid-reykmengun-folk-er-komid-med-nog- (accessed on 14 March 2025).
- Filipkowski, K.B.; Smyth, J.M.; Rutchick, A.M.; Santuzzi, A.M.; Adya, M.; Petrie, K.J.; Kaptein, A.A. Do Healthy People Worry? Modern Health Worries, Subjective Health Complaints, Perceived Health, and Health Care Utilization. Int. J. Behav. Med. 2010, 17, 182–188. [Google Scholar] [CrossRef]
- Tane, E.G.; Amorós-Pérez, A.; Martínez-Gómez, L.; Román-Martínez, M.C.; Lillo-Ródenas, M.A. Review and Comparative Analysis of the Particulate Matter Generated in Conventional Cigarettes and Heated Tobacco Products—Mainstream and Environmental Emissions. Environ. Adv. 2024, 16, 100552. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Locations | PM2.5 | PM10 | ||
|---|---|---|---|---|
| Mean | SD | Mean | SD | |
| Oddeyrin: | 466.26 | 509.63 | 611.33 | 653.85 |
| Port | 361.69 | 409.55 | 496 | 564.6 |
| Main street | 570.83 | 580.38 | 726.66 | 722.12 |
| Giljahverfi: | 174.41 | 316 | 242.28 | 366.62 |
| Nursery school | 148.27 | 255.7 | 229.92 | 349.69 |
| School | 197.07 | 363.15 | 252.52 | 385.92 |
| Questionnaire | Median | Min | Max | Mean | SD | n Above Threshold |
|---|---|---|---|---|---|---|
| Seasonality: GSS | 4 | 0 | 15 | 4.71 | 3.91 | n = 5; >10 |
| Insomnia: BIS | 10 | 0 | 42 | 10.98 | 9.66 | n = 18 |
| Migraine: MIG | 0 | 0 | 3 | 0.78 | 1.04 | n = 5; >2 |
| Eco-anxiety: HEAS | 1 | 0 | 38 | 4.19 | 6.65 | - |
| Alcohol consumption: AUDIT-C | 2 | 0 | 10 | 2.44 | 2.25 | n = 1; >7 |
| Caffeine per day | 2 | 0 | 10 | 2.35 | 2.02 | - |
| Item | Not at All | a Little | Some | a Lot |
|---|---|---|---|---|
| Outdoor air pollution | 11 | 18 | 15 | 1 |
| Indoor air pollution | 26 | 10 | 9 | 0 |
| Air pollution from studded tires | 14 | 14 | 15 | 2 |
| Air pollution from cruise ships | 13 | 8 | 16 | 8 |
| Seasonality GSS | Insomnia BIS | Migraine MIG | Eco-Anxiety HEAS | Alcohol AUDIT-C | Caffeine per Day | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Worries about air pollution… | rho | p | rho | p | rho | p | rho | p | rho | p | rho | p |
| outdoors | 0.09 | 0.568 | 0.43 | 0.003 * | 0.37 | 0.014 | 0.40 | 0.008 | −0.07 | 0.640 | −0.19 | 0.220 |
| indoors | 0.24 | 0.113 | 0.31 | 0.036 | 0.57 | 0.00005 * | 0.30 | 0.054 | −0.18 | 0.261 | −0.08 | 0.626 |
| from studded tires | 0.01 | 0.940 | 0.25 | 0.100 | 0.31 | 0.039 | 0.48 | 0.001 * | <0.01 | 0.987 | −0.05 | 0.730 |
| from cruise ships | −0.03 | 0.881 | 0.22 | 0.146 | 0.46 | 0.001 * | 0.26 | 0.088 | −0.06 | 0.696 | −0.01 | 0.960 |
| Item | Spring | Summer | Fall | Winter |
|---|---|---|---|---|
| Feel best | 22 | 36 | 14 | 6 |
| Feel worse | 6 | 1 | 14 | 31 |
| Gain the most weight | 4 | 7 | 8 | 28 |
| Lose the most weight | 11 | 18 | 7 | 12 |
| Sleep most | 4 | 5 | 17 | 29 |
| Sleep less | 11 | 30 | 7 | 6 |
| Socialize more | 23 | 26 | 16 | 20 |
| Socialize less | 4 | 6 | 8 | 29 |
| Eat most | 5 | 9 | 7 | 30 |
| Eat least | 9 | 13 | 15 | 13 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Höller, Y.; Zelinski, L.; Sesseljuson, L.D.; Pálmadóttir, A.D.; Latini, A.; Matthews, A.; Ásmundsdóttir, Á.M.; Guðmundsson, L.S.; Ólafsson, R.P. Worries About Air Pollution from the Unsustainable Use of Studded Tires and Cruise Ships—A Preliminary Study on the Relationship Between Worries and Health Complaints Due to Seasonal Pollution. Sustainability 2025, 17, 4634. https://doi.org/10.3390/su17104634
Höller Y, Zelinski L, Sesseljuson LD, Pálmadóttir AD, Latini A, Matthews A, Ásmundsdóttir ÁM, Guðmundsson LS, Ólafsson RP. Worries About Air Pollution from the Unsustainable Use of Studded Tires and Cruise Ships—A Preliminary Study on the Relationship Between Worries and Health Complaints Due to Seasonal Pollution. Sustainability. 2025; 17(10):4634. https://doi.org/10.3390/su17104634
Chicago/Turabian StyleHöller, Yvonne, Lada Zelinski, Leon Daði Sesseljuson, Ara Dan Pálmadóttir, Asia Latini, Audrey Matthews, Ásta Margrét Ásmundsdóttir, Lárus Steinþór Guðmundsson, and Ragnar Pétur Ólafsson. 2025. "Worries About Air Pollution from the Unsustainable Use of Studded Tires and Cruise Ships—A Preliminary Study on the Relationship Between Worries and Health Complaints Due to Seasonal Pollution" Sustainability 17, no. 10: 4634. https://doi.org/10.3390/su17104634
APA StyleHöller, Y., Zelinski, L., Sesseljuson, L. D., Pálmadóttir, A. D., Latini, A., Matthews, A., Ásmundsdóttir, Á. M., Guðmundsson, L. S., & Ólafsson, R. P. (2025). Worries About Air Pollution from the Unsustainable Use of Studded Tires and Cruise Ships—A Preliminary Study on the Relationship Between Worries and Health Complaints Due to Seasonal Pollution. Sustainability, 17(10), 4634. https://doi.org/10.3390/su17104634