1. Introduction
Since the World Health Organization confirmed COVID-19 as a global pandemic, countries around the world have gradually made various efforts to inhibit its infection or co-exist with the virus. Nurses are critical members of the entire medical system, and they play a pivotal role in providing medical care [
1]. However, with the COVID-19 epidemic, the lack of medical manpower has forced hospital volunteers to play an important role. If hospitals can effectively take advantage of volunteer manpower, the quality of medical services be ameliorated and the social image of volunteer services can be better shaped [
2]. However, through offering voluntary services during this time, their physical, psychological, and work goals have changed. Liu and Hsieh [
3] pointed out impacts of COVID-19 and its related epidemic prevention measures on the management of hospital volunteer services. In other words, with COVID-19, the psychological and physical costs of hospital volunteers’ services have grown. This study investigated the influence of changes in work resources on aspects of hospital volunteers’ services (such as flow experience and subjective well-being). Furthermore, hospital volunteers carry out helping behaviors out of social public welfare responsibilities. In addition to the voluntary services in their career planning, hospital volunteers have access to leisure activities and obtain a work–life balance. Stebbins [
4] divided public leisure into casual leisure and serious leisure. Hospital volunteers engage in voluntary services in hospitals not only for time-killing purposes but also for serious leisure. In other words, they are active in participation, and they treat voluntary services as a leisure activity while being seriously involved. They regard voluntary services as leisure activities and seriously participate in them, so as to obtain a sense of happiness [
5] and flow experience [
6].
The impact of volunteers’ flow experience on subjective well-being has also been demonstrated by relevant research [
7]. Therefore, with COVID-19, the impact of changes in hospital volunteers’ work resources on their leisure involvement is likely to be one of the key factors for the commitment of voluntary manpower in the future. Furthermore, the influence of hospital volunteers’ leisure involvement on flow experience and well-being may also have a bearing on their willingness to persist in voluntary services in the future.
It can be seen from the relevant literature that the research topics on volunteers during the COVID-19 epidemic are diversified. For example, [
8] probed into the difficulties faced by Australian volunteers at the beginning of the COVID-19 epidemic. They put forward that the economic recession and growing social isolation appearing in society may increase the demand for certain forms of volunteer services. Tejativaddhana et al. [
9] took Thai volunteers as research subjects to further explore the significant contributions of volunteers to disease control. Pickell and Williams [
10] probed into the efficacy of virtual voluntary services during the COVID-19 epidemic, and manifested that such services can ease the pressure on medical personnel, reduce the risk of viral infection, and make patients and family life return to normal. Based on the above, during the COVID-19 epidemic, topics about the psychological and physiological costs of hospital volunteers in the workplace and how voluntary services affect their mental health have been rarely discussed. Therefore, this research took hospital volunteers as the research subjects and conducted an empirical study on the subjective well-being of hospital volunteers during the COVID-19 pandemic from a mental health perspective.
People are often confronted with different work resources in the workplace, including physical, psychological, or social resources. Demerouti et al. [
11] first proposed the job demands–resources (JD-R) model. Its basic assumption is that each occupation has two types of work characteristics—work demand and work resources, which constitute the overall model applicable to all occupational environments. The theory of work resources originates from the conservation of resources theory, which insists that people will have the motivation to acquire, preserve, and hold resources they consider valuable or the means they should own [
12]. Demerouti and Bakker [
13] further pointed out that work resources can be divided into the organizational level, interpersonal level, position level, and task level. Specifically, the organizational level includes salary, career opportunities, and job security; the interpersonal level is about supervisors’ and colleagues’ support and team atmosphere; the job level involves role clarity and the degree of participation in decision making; the task level contains skill diversity, job integrity, task importance, autonomy, and performance feedback. Different levels of job requirements and work resources interact with each other and produce varying effects on organizational members, which can lead to job burnout, work pressure, or work engagement. Under the COVID-19 epidemic, it is worth further exploring whether changes in the work resources of hospital volunteers will have an impact on the completion of tasks.
When people participate in a specific leisure activity and commit their time and energy to it, the psychological state of triggering motivation can be regarded as the degree of involvement in the leisure activity. Havitz and Dimanche [
14] demonstrated that leisure involvement is the degree of awareness and cognitive perception between the individual and the activity itself, the tourism destination, or the equipment being used. In other words, when individuals participate in preferred activities, their engagement and concentration can be generated through the cognitive levels of the importance of the activity, the pleasure value, and the symbolic value. From this definition, it can be seen that the deeper people’s involvement in leisure is, the higher the degree of concern to be involved in leisure. Hospital volunteers perform voluntary services as a kind of serious leisure, which can represent the degree of involvement of volunteers in unpaid services. Relevant research has also confirmed the impact of the serious leisure of volunteer participants on leisure involvement. For example, Wei [
15] took volunteers at the 2018 Taichung World Flora Exposition as the research subjects, and the results show that the serious leisure of volunteers positively and significantly affects leisure involvement. Chen [
16] suggested that the mutual progress and happiness of volunteers’ serious leisure can remarkably predict leisure involvement. As for the dimension of leisure involvement, most research uses the three dimensions proposed by [
17] as the benchmark, namely, attraction, self-expression, and centrality. Attraction refers to the importance and pleasure of a certain activity for participants; self-expression refers to the need of participants to pursue self-realization and the expression of personal identity after participation in the activity; and centrality refers to the subjective identification value of participants’ involvement in leisure activities by their lifestyle. Hsu and Chen [
18] put forward similar views, indicating that the reasons for different levels of involvement include personal values, emotions, and interests. In the process of engaging in leisure activities, individuals can experience physical and psychological improvement and the enhancement of interpersonal relationships. These individuals’ feelings are leisure benefits.
Flow experience is a pleasant and positive psychological state. When individuals are fully engaged in an activity, they will have all kinds of feelings when their skills and external challenges reach a balance [
19]. In other words, with a change in the relationship between challenges and skills, individuals’ feelings will also vary. On one hand, when the difficulty of the challenges increases, individuals must learn new skills. On the other hand, when personal skills are improved, people will seek more difficult challenges to obtain a flow experience and feel a sense of accomplishment and happiness. While this experience model forms a virtuous cycle, people can obtain leisure experience from flow experience. Csikszentmihalyi [
20] pointed out the nine characteristics of flow experience: clear goals, unambiguous feedback, challenge–skill balance, action–awareness merging, concentration on the task at hand, sense of control, loss of self-consciousness, the transformation of time, and automatic experience. Hence, it can be known that the flow experience is not easy to obtain, as it can only be achieved when relevant conditions are ripe. Moneta and Csikszentmihalyi [
21] summed up the characteristics of flow experience to illustrate this kind of special leisure experience. First, the function generated from the pleasurable experience depends on subjective experience variables, including challenges and skills. Second, the experience function with a speculative element has no end or extreme, because the flow theory does not limit the optimal experience. Through the flow experience, individuals can continue to pursue harder challenges and greater pleasure. In terms of the measurement of flow experience, [
20] first proposed the original flow model and pointed out that skills and challenges are the keys to affect the flow model. When personal skills and challenges are balanced, a flow experience will occur; when skills outweigh challenges, boredom will be generated and interest will be lost; when challenges outweigh skills, anxiety will be produced and control over the situation will be lacking. Therefore, only when the levels of skills and challenges are high and reach a balance will an individual have the flow experience, show interest in it, and pursue a higher level of flow experience. However, the original flow model was designed for more complex sports, and it cannot be applied to people engaged in general leisure activities. Therefore, Massimini and Carli [
22] proposed an eight-dimensional flow model (indifference, concern, anxiety, awakening, fluency, control, boredom, and relaxation) that divides skills and challenges into three levels (low, medium, and high).
In addition to pursuing physical health, people also spare no effort to pursue mental health, which is one of the reasons why well-being is valued. In 1984, Diener [
23] suggested that subjective well-being that refers to a state of happiness means having more positive emotions, fewer negative emotions, and a higher sense of life satisfaction. Specifically, having more positive emotions and fewer negative emotions reflects the emotional level of subjective well-being, while having a higher sense of life satisfaction reflects the cognitive level of subjective well-being. Seligman and Csikszentmihalyi [
24] opined that subjective well-being is regarded as a valuable experience as well as a positive personal psychological state. Edwards et al. [
25] held a similar view, pointing out that subjective well-being is the core indicator of mental health, and is based on the discussion of hedonic well-being. They emphasized that happiness is more than just the absence of mental illness. Happiness is the most ideal manifestation of the human psychological function and experience. In other words, whether individuals feel happy or not can be referred to as a subjective statement of their current physical and psychological state and whether they are satisfied with life. Yen and Xu [
26] considered that subjective well-being can be divided into three levels after integrating relevant research results: (1) life satisfaction, which refers to the subjective satisfaction of individuals with their current overall life, including physical and spiritual aspects; (2) positive emotion, which refers to the happy state that individuals experience mentally or emotionally and is often related to social activities, a sense of satisfaction, and pleasant events; and (3) negative emotion, which refers to the unpleasant state that individuals experience mentally or emotionally and is often related to subjective pressure, poor coping styles, health problems, and unpleasant events. From the perspective of these three levels, subjective well-being is a holistic concept that enables people to make statements about their own emotions and further understand their psychological and emotional states.
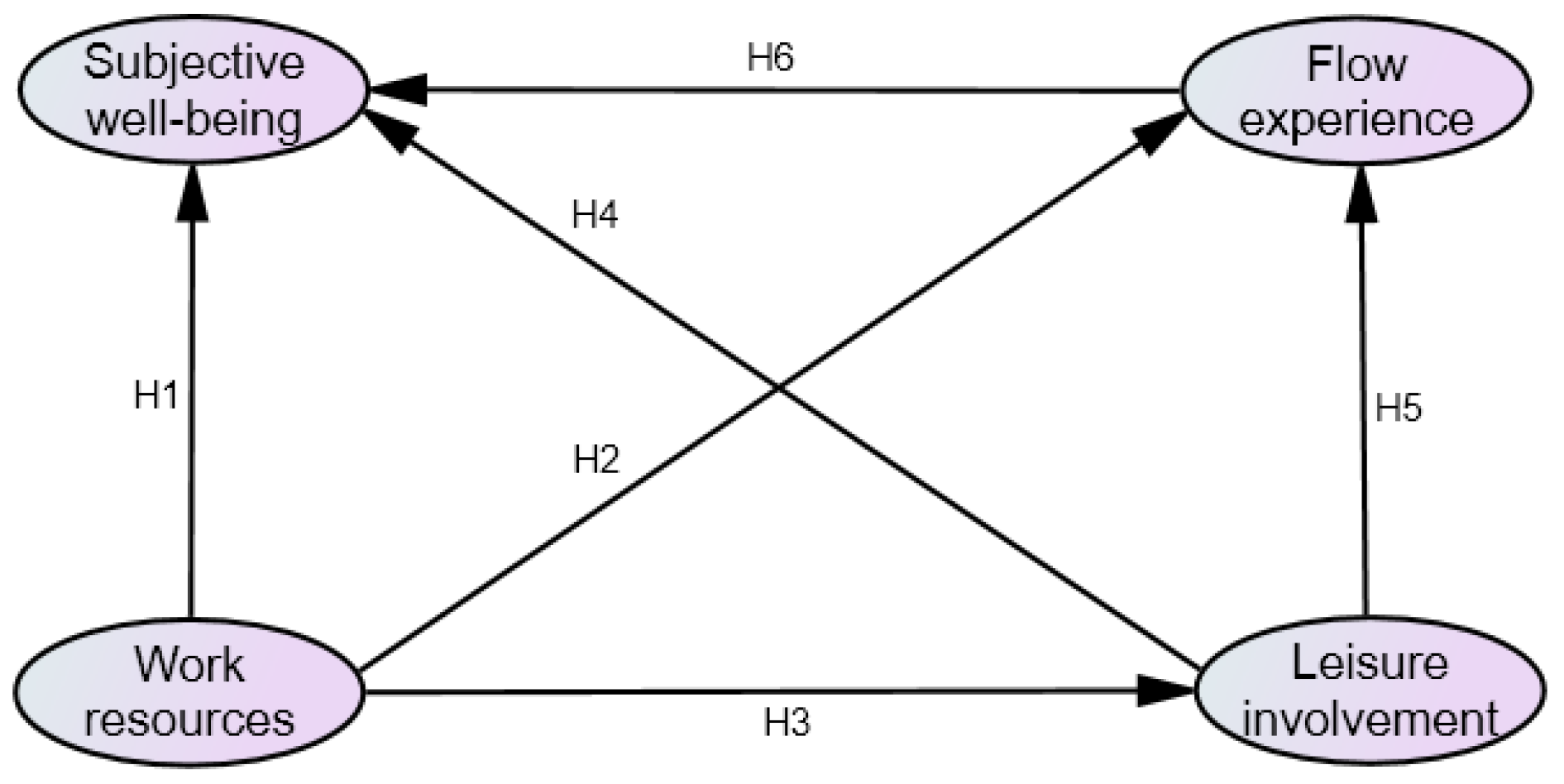
In terms of the relationships among the variables in this study, Hsieh [
27] took pharmaceutical industry workers as the research subjects to explore the relationships among the resources, abilities, and well-being of pharmaceutical industry employees. His study showed that work resources affect subjective well-being. Therefore, the current study assumed that the work resources of hospital volunteers have a significant impact on subjective well-being. Schaufeli and Bakker [
28] conducted research on work needs, work resources, and exhaustion, and their research results manifested that work resources affect the flow experience. Based on their research results, the current study assumed that the work resources of hospital volunteers have a significant impact on the flow experience. Lien [
29] took educational administrators working in colleges and universities as the research subjects to explore the issues related to leisure involvement. She found that work resources have a significant positive relationship with leisure involvement. Based on the discussion of relevant research, the current study assumed that the work resources of hospital volunteers have a significant impact on leisure involvement. Cheng and Lu [
30] took 322 surfing participants as the research subjects in their study, and the research results indicated that the leisure involvement of surfing participants has a positive impact on their subjective well-being. Thus, the current study assumed that the leisure involvement of hospital volunteers has a significant impact on subjective well-being. Tao et al. [
31] conducted an empirical analysis of leisure participants in urban parks, and their research results show that leisure involvement has a significant impact on flow experience. According to that research conclusion, the present study assumed that hospital volunteers’ leisure involvement has a significant impact on flow experience. Tse et al. [
32] revealed that flow experience has a significant impact on subjective well-being in the research targeting a sense of happiness. Therefore, the present study assumed that the flow experience of hospital volunteers has a significant impact on subjective well-being. In addition, the mediation effect of leisure involvement on work resources and flow experience has also been demonstrated by relevant research [
29].


 and
and 
{kind=link}
{kind=link}