
Evaluation of Household Water Treatment Technologies for Cholera Eradication in Sub-Saharan Africa: Epidemiological and Economic Perspectives


Abstract
1. Introduction
2. Methodology
2.1. Study Area
2.2. Epidemiological Analysis
2.3. Economic Evaluation and Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Cholera Fact Sheet. 2019. Available online: https://www.who.int/news-room/fact-sheets/detail/cholera (accessed on 11 July 2020).
- Weill, F.X.; Domman, D.; Njamkepo, E.; Tarr, C.; Rauzier, J.; Fawal, N.; Keddy, K.H.; Salje, H.; Moore, S.; Mukhopadhyay, A.K.; et al. Genomic history of the seventh pandemic of cholera in Africa. Science 2017, 358, 785–789. [Google Scholar] [CrossRef] [PubMed]
- Mandal, S.; Mandal, M.D.; Pal, N.K. Cholera: A great global concern. Asian Pac. J. Trop. Med. 2011, 4, 573–580. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.; Nelson, A.R.; Lopez, A.L.; Sack, R.B. Updated global burden of cholera in endemic countries. PLoS Negl. Trop. Dis. 2015, 9, e0003832. [Google Scholar] [CrossRef] [PubMed]
- Nigeria Centre for Disease Control. Cholera Outbreak in Nigeria: Situation Report; Nigeria Centre for Disease Control: Abuja, Nigeria, 2021. Available online: https://ncdc.gov.ng/themes/common/files/sitreps/45e62c2c2378c3bbf3d7b6bbd862f7ed.pdf (accessed on 11 July 2023).
- Fagbamila, I.O.; Abdulkarim, M.A.; Aworh, M.K.; Uba, B.; Balogun, M.S.; Nguku, P.; Gandi, A.Y.; Abdullahi, I.; Okolocha, E.C.; Kwaga, J.K.P.; et al. Cholera outbreak in some communities in North-East Nigeria, 2019: An unmatched case-control study. BMC Public Health 2023, 23, 446. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Cameroon: Cholera Outbreak—2021. Disease Outbreak News. 2021. Available online: https://www.who.int/csr/don/27-march-2021-cholera-cameroon/en/ (accessed on 11 July 2023).
- World Health Organization. Cholera Outbreak in Malawi, March 2022—February 2023. 2023. Available online: https://www.who.int/emergencies/disease-outbreak-news/item/2023-DON305 (accessed on 11 July 2023).
- Mengel, M.A.; Delrieu, I.; Heyerdahl, L.; Gessner, B.D. Cholera outbreaks in Africa. Curr. Top. Microbiol. Immunol. 2014, 379, 117–144. [Google Scholar] [CrossRef] [PubMed]
- Sack, D.A.; Sack, R.B.; Nair, G.B.; Siddique, A.K. Cholera. Lancet 2004, 363, 223–233. [Google Scholar] [CrossRef]
- World Health Organization. Ending Cholera—A Global Roadmap to 2030. Global Task Force on Cholera Control. Ending Cholera—A Global Roadmap to 2030. Available online: https://www.gtfcc.org/wp-content/uploads/2019/10/gtfcc-ending-cholera-a-global-roadmap-to-2030.pdf (accessed on 11 July 2023).
- Taylor, D.L.; Kahawita, T.M.; Cairncross, S.; Ensink, J.H. The Impact of Water, Sanitation and Hygiene Interventions to Control Cholera: A Systematic Review. PLoS ONE 2015, 10, e0135676. [Google Scholar] [CrossRef] [PubMed]
- Freeman, M.C.; Clasen, T.; Dreibelbis, R.; Saboori, S.; Greene, L.E.; Brumback, B.; Muga, R.; Rheingans, R. The impact of a school-based water supply and treatment, hygiene, and sanitation programme on pupil diarrhoea: A cluster-randomized trial. Epidemiol. Infect. 2014, 142, 340–351. [Google Scholar] [CrossRef] [PubMed]
- Clasen, T.F.; Alexander, K.T.; Sinclair, D.; Boisson, S.; Peletz, R.; Chang, H.H.; Majorin, F.; Cairncross, S. Interventions to improve water quality for preventing diarrhoea. Cochrane Database Syst. Rev. 2015, 2015, CD004794. [Google Scholar] [CrossRef] [PubMed]
- Gebrewahd, A.; Adhanom, G.; Gebremichail, G.; Kahsay, T.; Berhe, B.; Asfaw, Z.; Tadesse, S.; Gebremedhin, H.; Negash, H.; Tesfanchal, B.; et al. Bacteriological quality and associated risk factors of drinking water in Eastern zone, Tigrai, Ethiopia, 2019. Trop. Dis. Travel Med. Vaccines 2020, 6, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Lessler, J.; Moore, S.M.; Luquero, F.J.; McKay, H.S.; Grais, R.; Henkens, M.; Mengel, M.; Dunoyer, J.; M’Bangombe, M.; Lee, E.C.; et al. Mapping the burden of cholera in sub-Saharan Africa and implications for control: An analysis of data across geographical scales. Lancet 2018, 391, 1908–1915. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Results of Round I of the Household Water Treatment Evaluation Scheme; WHO: Geneva, Switzerland, 2016; Available online: https://www.who.int/publications/i/item/9789241509947 (accessed on 11 July 2023).
- World Health Organization. Results of Round II of the WHO Household Water Treatment Evaluation Scheme; WHO: Geneva, Switzerland, 2019; Available online: https://www.who.int/publications/i/item/9789241516037 (accessed on 11 July 2023).
- Haas, C.N.; Rose, J.B.; Gerba, C.P. Quantitative Microbial Risk Assessment; John Wiley & Sons: New York, NY, USA, 1999. [Google Scholar]
- Ali, M.; Emch, M.; von Seidlein, L.; Yunus, M.; Sack, D.A.; Holmgren, J. Herd immunity conferred by killed oral cholera vaccines in Bangladesh: A reanalysis. Lancet Glob. Health 2005, 366, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Bwire, G.; Munier, A.; Ouedraogo, I.; Heyerdahl, L.; Komakech, H.; Kagirita, A.; Wood, R.; Mhlanga, R.; Njanpop-Lafourcade, B.; Malimbo, M.; et al. Epidemiology of cholera outbreaks and socio-economic characteristics of the communities in the fishing villages of Uganda: 2011–2015. PLoS Negl. Trop. Dis. 2017, 11, e0005407. [Google Scholar] [CrossRef] [PubMed]
- World Bank. Poverty and Shared Prosperity 2018: Piecing Together the Poverty Puzzle; World Bank: Washington, DC, USA, 2019. [Google Scholar]
- United Nations. World Population Prospects 2019: Highlights (ST/ESA/SER.A/423). United Nations Department of Economic and Social Affairs, Population Division. 2019. Available online: https://population.un.org/wpp/Publications/Files/WPP2019_10KeyFindings.pdf (accessed on 11 July 2023).
- Kirigia, J.M.; Sambo, H.B.; Yokouide, A.; Soumbey-Alley, E. Economic burden of cholera in the WHO African region. BMC Int. Health Hum. Rights 2009, 9, 8. [Google Scholar] [CrossRef] [PubMed]
- Briceño-Garmendia, C.; Smits, K.; Foster, V. Financing Public Infrastructure in Sub-Saharan Africa: Patterns and Emerging Issues; World Bank: Washington, DC, USA, 2008; Available online: http://hdl.handle.net/10986/28238 (accessed on 11 July 2023).
- Elimian, K.; Yennan, S.; Musah, A.; Akinleye, D.; Abdulraheem, A.; Shittu, O. Epidemiology, diagnostics, and factors associated with mortality during a cholera epidemic in Nigeria, October 2020–October 2021: A retrospective analysis of national surveillance data. BMJ Open 2022, 12, e063703. [Google Scholar] [CrossRef] [PubMed]
- World Bank. Water Supply and Sanitation in Sub-Saharan Africa: The World Bank’s Commitment to Basic Needs in Africa; World Bank Publications: Washington, DC, USA, 1993. [Google Scholar]
- International Water and Sanitation Centre (IRC). Water, Sanitation, and Hygiene: Sustainable Development and Multisectoral Approaches. 2009. Available online: https://www.ircwash.org/sites/default/files/113-090.pdf (accessed on 11 July 2023).
- Chew, J.F.; Corlin, L.; Ona, F.; Pinto, S.; Fenyi-Baah, E.; Osei, B.G.; Gute, D.M. Water Source Preferences and Water Quality Perceptions among Women in the Eastern Region, Ghana: A Grounded Theory Study. Int. J. Environ. Res. Public Health 2019, 16, 3835. [Google Scholar] [CrossRef] [PubMed]
- Ojomo, E.; Elliott, M.; Goodyear, L.; Forson, M.; Bartram, J. Sustainability and scale-up of household water treatment and safe storage practices: Enablers and barriers to effective implementation. Int. J. Hyg. Environ. Health 2015, 218, 281–291. [Google Scholar] [CrossRef] [PubMed]
- Prüss-Ustün, A.; Wolf, J.; Bartram, J.; Clasen, T.; Cumming, O.; Freeman, M.C.; Gordon, B.; Hunter, P.R.; Medlicott, K.; Johnston, R. Burden of disease from inadequate water, sanitation, and hygiene for selected adverse health outcomes: An updated analysis with a focus on low- and middle-income countries. Int. J. Environ. Res. Public Health 2019, 222, 765–777. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
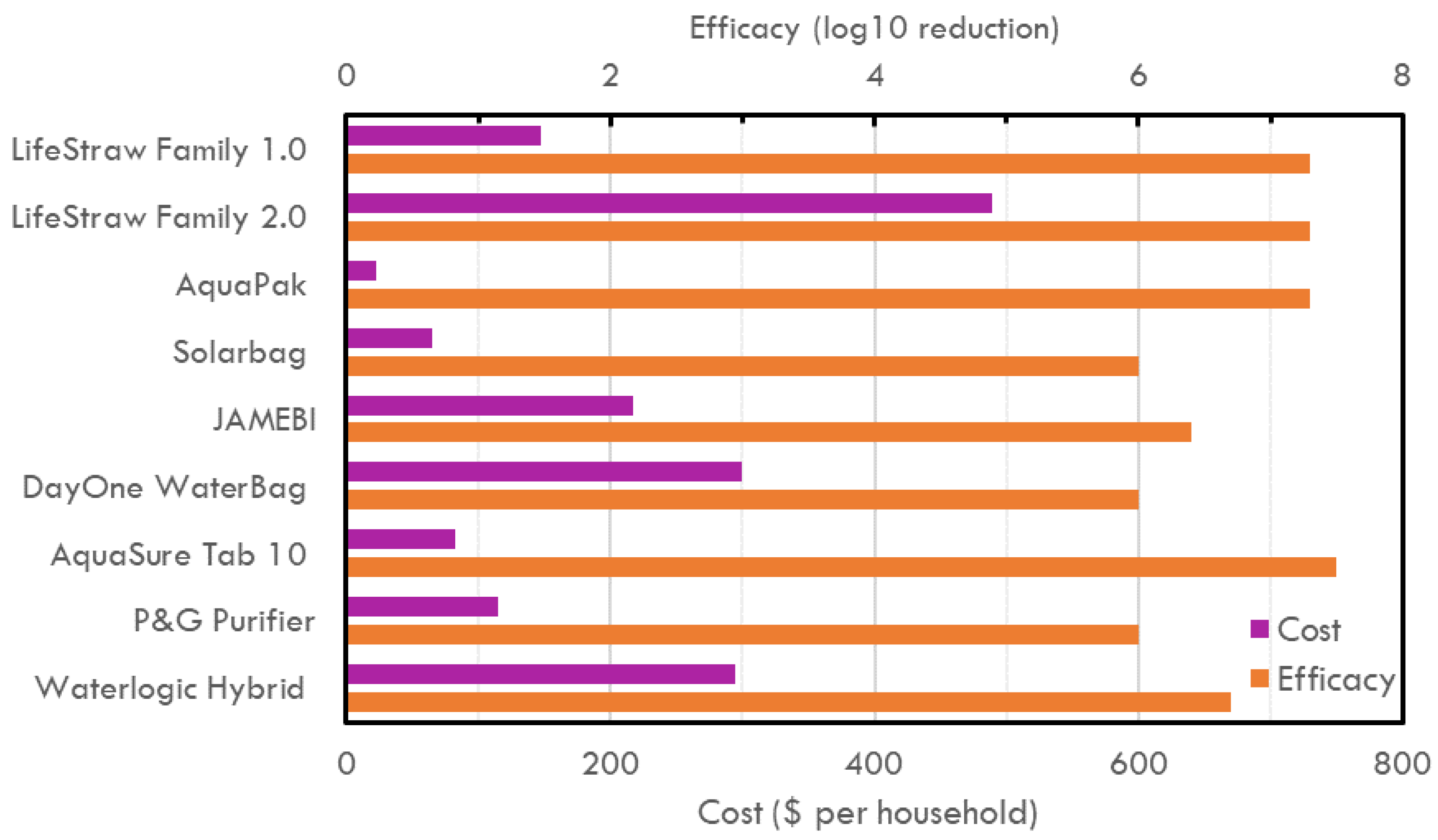
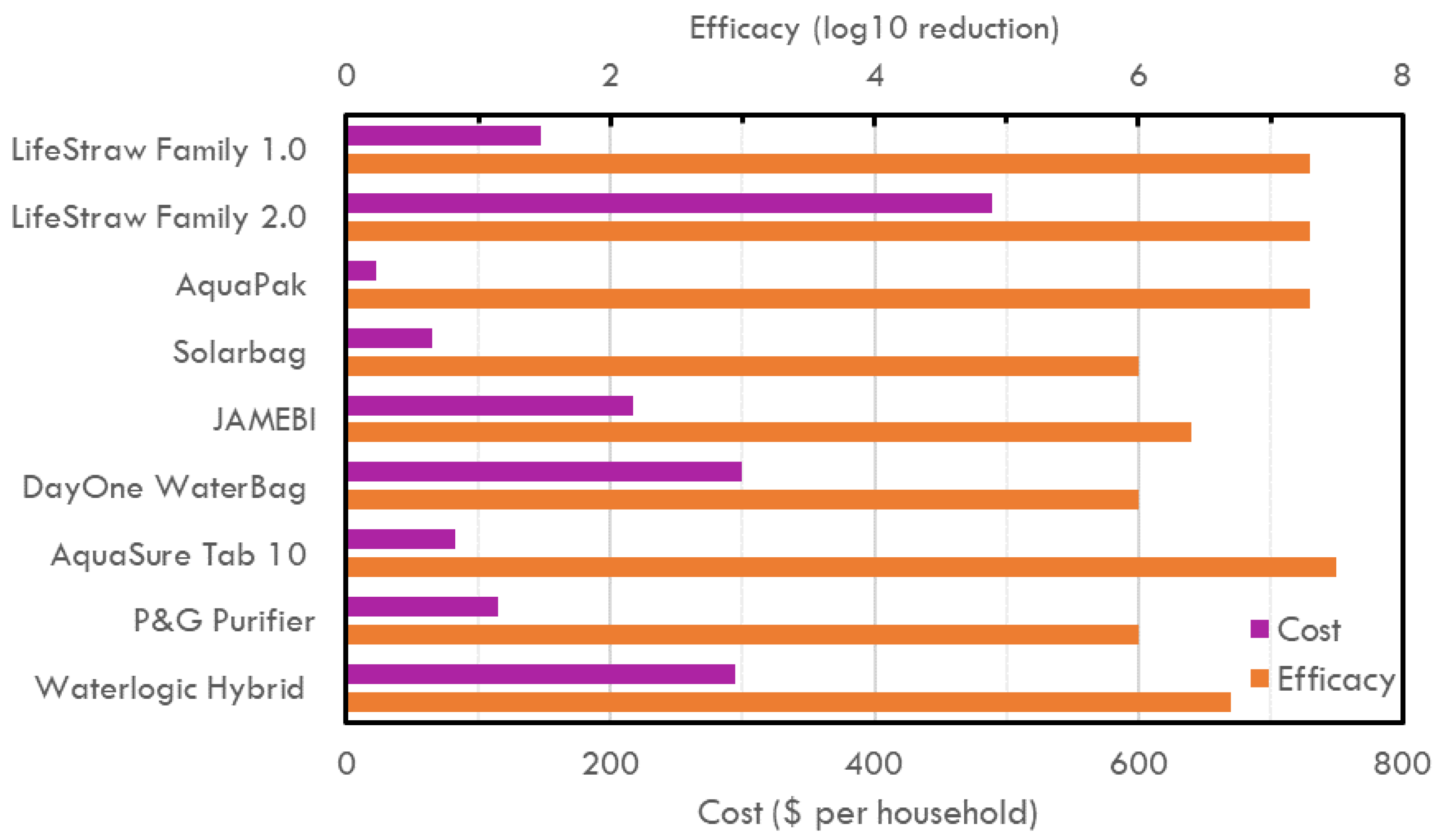
| HWT Products | Functional Mechanism | Total Cost (USD) Maximum Cost per Year | Efficacy (CFU/mL) | Storage and Capacity | Durability | Convenience of Use |
|---|---|---|---|---|---|---|
| LifeStraw | Microorganisms are physically removed through ultrafiltration from water as it is forced through hollow fiber membranes of pore size 0.1 µm–1 µm under gravitational pressure. Filter flow rate is 12 L/h. | Family 1.0: 147 Family 2.0: 489.3 | 7.3 | Family 1.0: NO (can hang on wall) Family 2.0: YES (tabletop) 5.5 L. | Filter and tap to be replaced after 2–3 months. Products have a lifespan of 3–5 years | Needs user training and a reliable supply chain. Daily backwash and pre-filter cleaning recommended. Not energy-deficient. |
| AquaPak | Contaminated water heats at >65 °C using sunlight to eliminates all types of microorganisms, bacteria, viruses, and protozoa. It has colored wax that melts at 65 °C, indicating that water is safe for consumption. | 23 | 7.3 | YES (can hold 5 L of water). | The AquaPak can be reused daily and has a lifespan of 3 years. | Simple to use and no maintenance required. Minimal likelihood of recontamination when held in disinfecting container. Relatively long time to treat water and variability depending on sun intensity. |
| Solarbag | Solar powered-solar-activated nanotechnology. Suitable for highly turbid water. It uses Pur-Blue Dye Indicator for the first time to test the duration required throughout the treatment process. Photocatalysis breaks down blue dye in water at the same rate as contaminants. | 65.5 | 6.0 | YES (can hold 10 L of water). | Puralytics Solarbag lasts for 7 years. | Simple to use. No maintenance required. Minimal likelihood of recontamination when held in disinfecting container. Relatively long time to treat water and variability depending on sun intensity. |
| JAMEBI | Solar Powered (UV + Heat) technology. Heats water to 75 °C using sunlight, in the heat exchanger’s outer pipe. Then, the solar thermal panel pasteurizes at ~80 °C for 4 min. Pasteurized water is cooled in the heat exchanger’s inner pipe before release. | 216.7 | 6.4 | NO (maximum daily output is 250 L/day) = 1,000,000 L of water throughout its lifespan. | Reusable for 20 years in daily use. | Solar-powered. No electricity required. Easy to use based on design principle. Weekly visual maintenance checks required for leaks. Annual maintenance to clean heat exchanger. Minimal need for spare parts. |
| DayOne Waterbag | Fill-add-close-mix-wait-drink, water needs to be used > 24 h. Most effective for highly turbid water. Used with P&G treatment packets (4 g packet contains Calcium Hypochlorite 0.546%, chlorine 2.17 ppm). Takes 25 min to purify with a 1.5 L/min flow rate. Treats 10 L of water. | 300 | 6.0 | YES (can hold 10 L of water). | The Waterbag provides a family of 4 with clean drinking water for up to 2 months and P&G packets lasts 3 years from the date of manufacture. | Simple to use-brief steps. No maintenance required. Minimal likelihood of recontamination Relatively long time to treat water-30 min. Not energy-deficient |
| AquaSure Tab 10 | Double-layered tablets containing ferric sulfate and sodium dichloroisocyanurate (NaDCC). Ferric sulfate acts as a coagulant and flocculant. Floccules sediment settles at the bottom of the water vessel, NaDCC acts as a disinfectant. Each tab treats 10 L of water. | 82 | 7.5 | NO (does not include a safe storage container). | Aquasure Tab10 expires 3 years after the manufacture date | Residual protection against recontamination Need for multiple steps to use the product. Requires additional user support. No Maintenance required. Not energy-deficient |
| P&G Purifier of Water | P&G water purification technology: Quickly treats 10 L of contaminated water. It works in three ways: Coagulation, Flocculation and Disinfection. Add-Mix-Wait–Drink. | 115 | 6.0 | NO (does not include a safe storage container). | P&G packets lasts 3 years from the date of manufacture. | Residual protection against recontamination. Need for multiple steps to use the product. Requires additional user support. No maintenance required. Not energy-deficient |
| Waterlogic Hybrid | Electric water treatment device fitted with a carbon pre-filter and UV lamp. Water passes the pre-filter and UV lamp and is dispensed through a spout, the flowrate is 1.5 L per minute. | 295 | 6.7 | NO (does not include a safe storage container). | Long life filter and lamp only need one change per year. | Electricity required. Maintenance required. Reliable supply chain is required. Simple to use. |
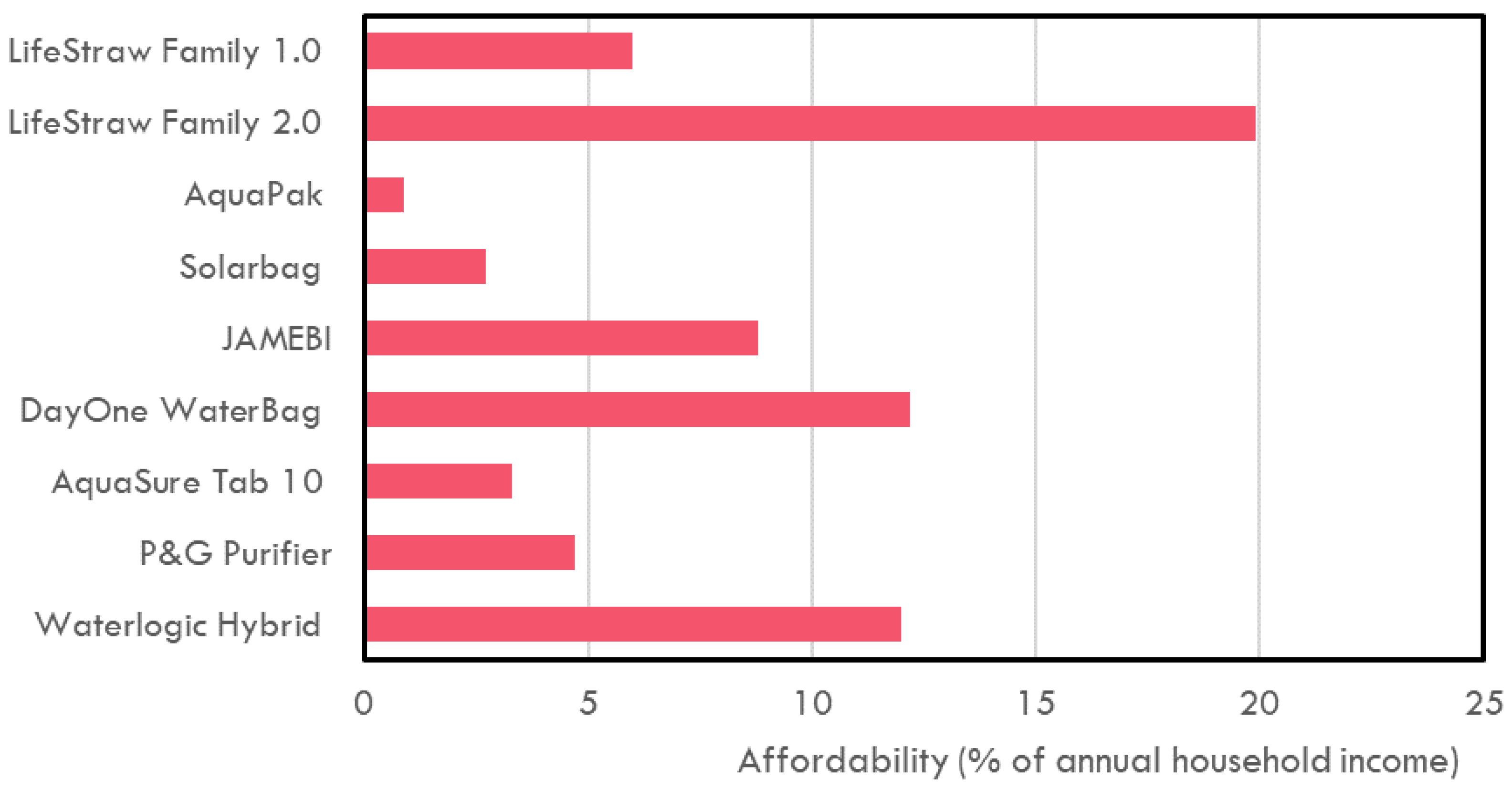
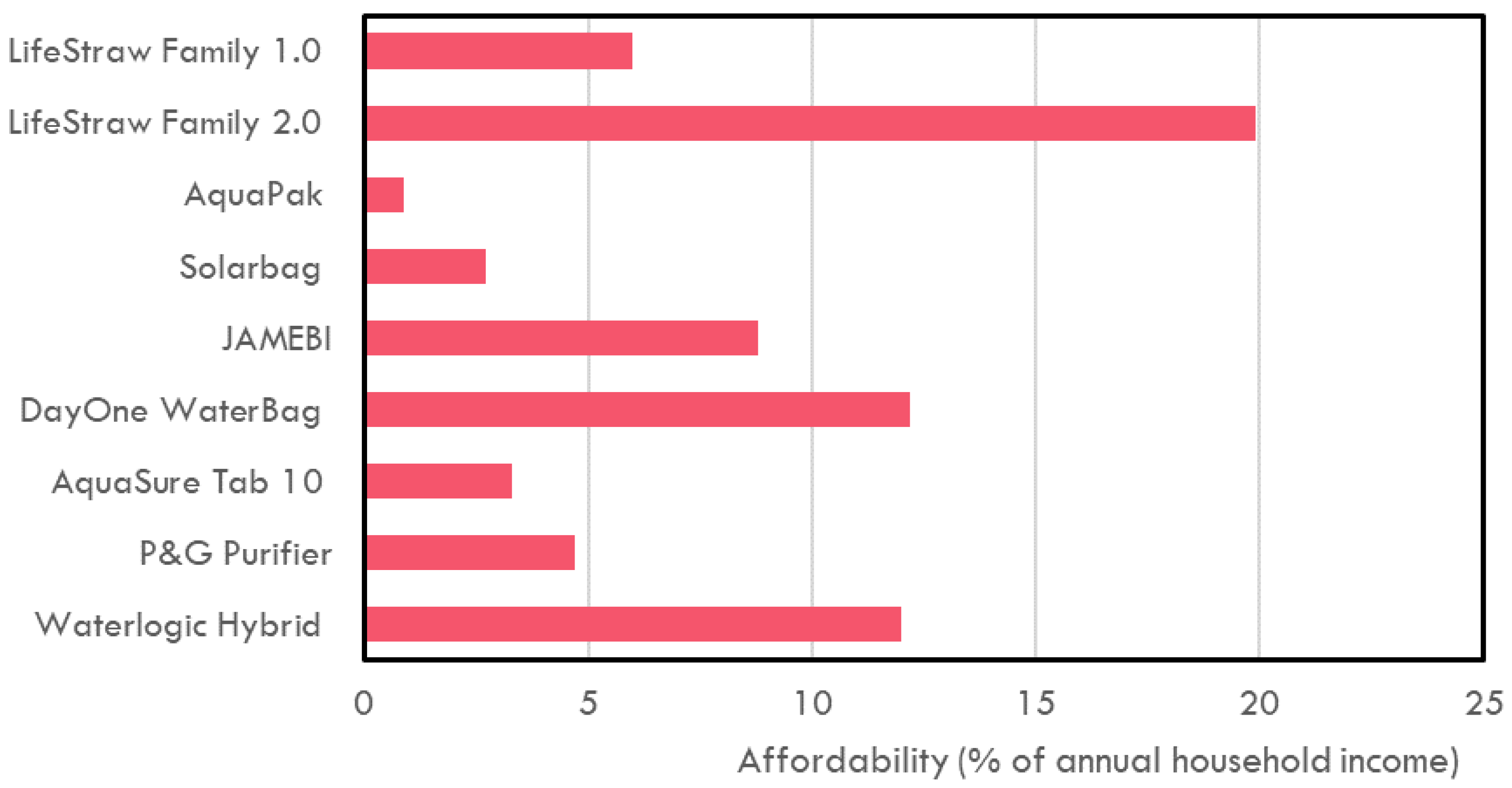
| HWT Product | Total Cost of Universal Adoption (Billion USD) |
|---|---|
| LifeStraw 1.0 | 2.51 |
| LifeStraw 2.0 | 8.36 |
| AquaPak | 0.39 |
| Solarbag | 1.12 |
| JAMEBI | 3.70 |
| DayOne Waterbag | 5.12 |
| AquaSure Tab 10 | 1.40 |
| P&G Purifier of Water | 1.96 |
| Waterlogic Hybrid | 5.04 |
| TCWSI | 14.97 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eruaga, M.D.; Davis, K.F. Evaluation of Household Water Treatment Technologies for Cholera Eradication in Sub-Saharan Africa: Epidemiological and Economic Perspectives. Sustainability 2024, 16, 1422. https://doi.org/10.3390/su16041422
Eruaga MD, Davis KF. Evaluation of Household Water Treatment Technologies for Cholera Eradication in Sub-Saharan Africa: Epidemiological and Economic Perspectives. Sustainability. 2024; 16(4):1422. https://doi.org/10.3390/su16041422
Chicago/Turabian StyleEruaga, Michael Damilola, and Kyle Frankel Davis. 2024. "Evaluation of Household Water Treatment Technologies for Cholera Eradication in Sub-Saharan Africa: Epidemiological and Economic Perspectives" Sustainability 16, no. 4: 1422. https://doi.org/10.3390/su16041422
APA StyleEruaga, M. D., & Davis, K. F. (2024). Evaluation of Household Water Treatment Technologies for Cholera Eradication in Sub-Saharan Africa: Epidemiological and Economic Perspectives. Sustainability, 16(4), 1422. https://doi.org/10.3390/su16041422