

Are Sustainable Health Workforces Possible? Issues and a Possible Remedy


Abstract
1. Introduction
2. Sustainable Health, Care and Workforces
3. Health Workforce Governance and Planning
3.1. Health Workforce Governance
3.2. Health Workforce Planning
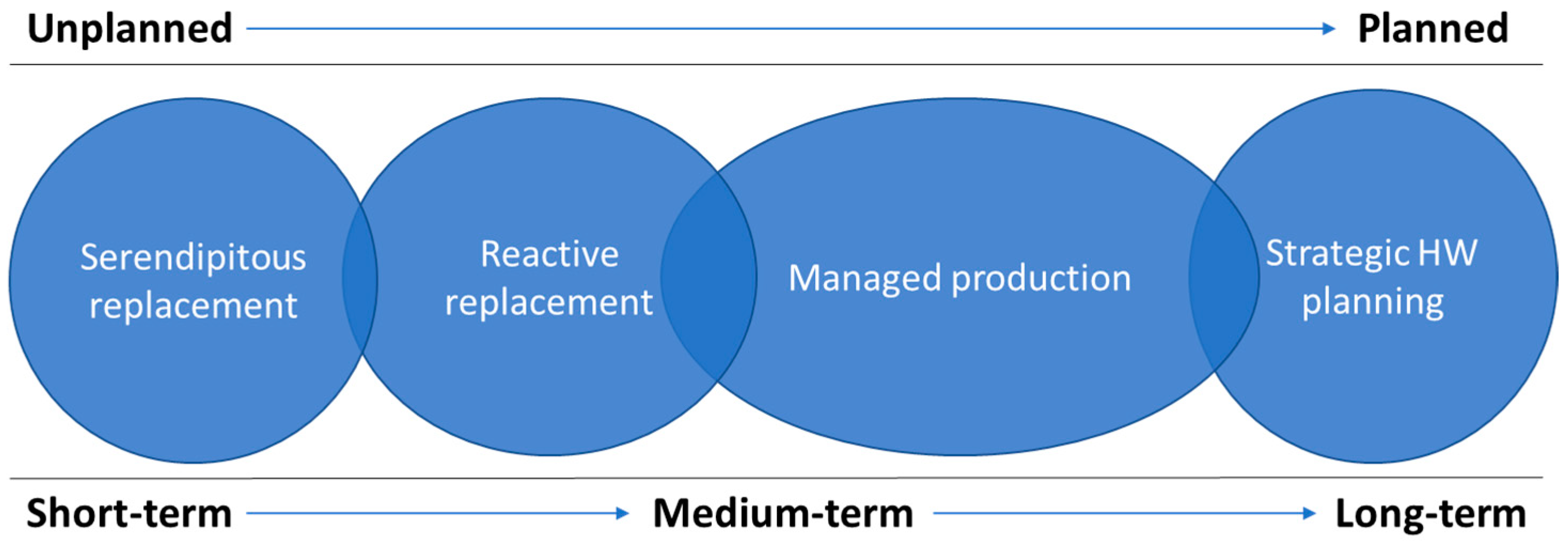
3.3. Health Workforce Planning Types
4. Discussion
4.1. Towards Sustainable Workforces
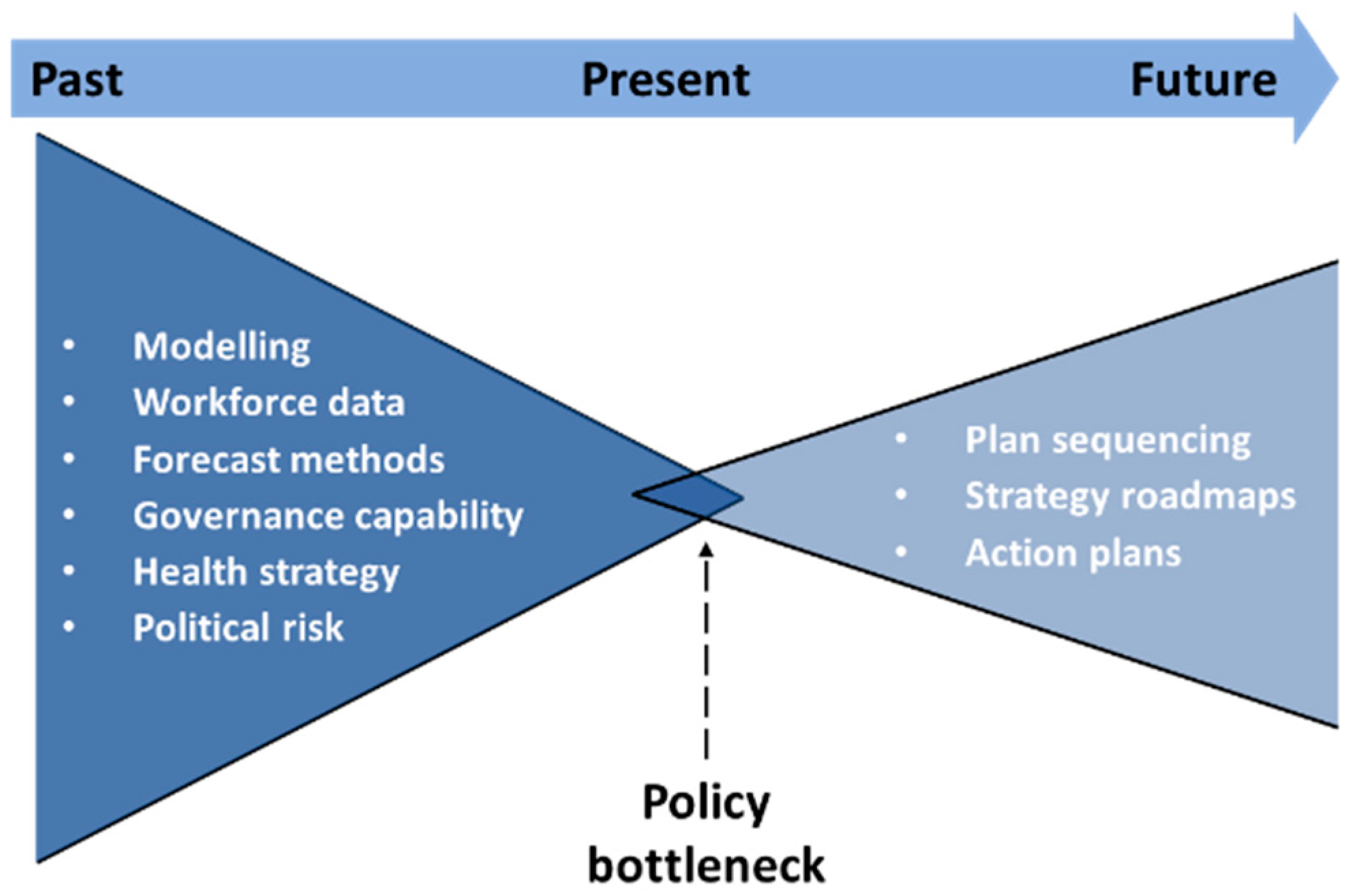
4.2. Introducing Backcasting
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19. 11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 3 July 2022).
- European Observatory on Health Systems and Policies COVID-19 Health System Response Monitor (HSRM). Available online: https://eurohealthobservatory.who.int/monitors/hsrm/overview (accessed on 3 July 2022).
- Bandyopadhyay, S.; Baticulon, R.E.; Kadhum, M.; Alser, M.; Ojuka, D.K.; Badereddin, Y.; Kamath, A.; Parepalli, S.A.; Brown, G.; Iharchane, S.; et al. Infection and mortality of healthcare workers worldwide from COVID-19: A systematic review. BMJ Glob. Health 2020, 5, e003097. [Google Scholar] [CrossRef] [PubMed]
- De Raeve, P.; Adams, E.; Xyrichis, A. The impact of the COVID-19 pandemic on nurses in Europe: A critical discussion of policy failures and opportunities for future preparedness. Int. J. Nurs. Stud. Adv. 2021, 3, 100032. [Google Scholar] [CrossRef]
- Huffman, A. COVID-19 Surges Then Crickets and the Impact on the Emergency Department Workforce. Ann. Emerg. Med. 2022, 79, A11–A14. [Google Scholar] [CrossRef]
- Hamouche, S. COVID-19 and employees’ mental health: Stressors, moderators and agenda for organizational actions. Emerald Open Res. 2020, 2, 15. [Google Scholar] [CrossRef]
- López-Cabarcos, M.A.; López-Carballeira, A.; Ferro-Soto, C. New ways of working and public healthcare professionals’ well-being: The response to face the COVID-19 pandemic. Sustainability 2020, 12, 8087. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Wherton, J.; Shaw, S.; Morrison, C. Video consultations for COVID-19. BMJ 2020, 368, m998. [Google Scholar] [CrossRef]
- Buchan, J.; Williams, G.A.; Zapata, T. Governing health workforce responses during COVID-19. Eurohealth 2021, 27, 41–48. [Google Scholar]
- Neilson, M. Immigration health Green List: Top Health Official Urges Ministers to Take Action on Healthcare Workforce Shortages. Available online: https://www.nzherald.co.nz/nz/politics/immigration-health-green-list-top-health-official-urges-ministers-take-action-on-healthcare-workforce-shortages/W3M7FEZRBVFXNDNT2TROWRDN4U/ (accessed on 20 November 2022).
- Afzal, M.; Cometto, G.; Rosskam, E.; Sheikh, M. Global Health Workforce Alliance: Increasing the momentum for health workforce development. Rev. Peru. Med. Exp. Salud Publica 2011, 28, 298–307. [Google Scholar] [CrossRef]
- Godue, C.; Cameron, R.; Borrell, R.M. Capacity building in human resources for health: The experience of the region of the Americas. Can. J. Public Health 2016, 107, e347–e354. [Google Scholar] [CrossRef]
- Pan American Health Organization. Strategy on Human Resources for Universal Access to Health and Universal Health Coverage; Pan American Health Organization: Washington DC, USA, 2017; Available online: https://iris.paho.org/handle/10665.2/53838 (accessed on 15 December 2022).
- Zapata, T.; Zakoji, M.; Kanda, M.; Travis, P.; Tangcharoensathien, V.; Buchan, J.; Jhalani, M. Implementing a decade of strengthening the health workforce in the WHO South-East Asia Region: Achievements and way forward for primary health care. WHO South-East Asia J. Public Health 2021, 10, S76–S86. [Google Scholar] [CrossRef]
- World Health Organization. Global Strategy on Human Resources for Health: Workforce 2030; World Health Organization: Geneva, Switzerland, 2016; ISBN 9789241511131. [Google Scholar]
- Global Health Workforce Alliance, World Health Organization. A Universal Truth: No Health without a Workforce; Global Health Workforce Alliance, World Health Organization: Geneva, Switzerland, 2014; ISBN 9789241506762. [Google Scholar]
- Dussault, G. Bringing the health workforce challenge to the policy agenda. In The Palgrave International Handbook of Healthcare Policy and Governance; Kuhlmann, E., Blank, R.H., Bourgeault, I.L., Wendt, C., Eds.; Palgrave Macmillan: London, UK, 2015; pp. 273–288. ISBN 978-1-137-38493-5. [Google Scholar]
- United Nations. Transforming Our World: The 2030 Agenda for Sustainable Development; United Nations: New York, NY, USA, 2015; Available online: https://sdgs.un.org/sites/default/files/publications/21252030%20Agenda%20for%20Sustainable%20Development%20web.pdf (accessed on 13 December 2022).
- Moore, J.E.; Mascarenhas, A.; Bain, J.; Straus, S.E. Developing a comprehensive definition of sustainability. Implement. Sci. 2017, 12, 110. [Google Scholar] [CrossRef] [PubMed]
- Stirman, S.W.; Kimberly, J.; Cook, N.; Calloway, A.; Castro, F.; Charns, M. The sustainability of new programs and innovations: A review of the empirical literature and recommendations for future research. Implement. Sci. 2012, 7, 17. [Google Scholar] [CrossRef] [PubMed]
- Gorman, D.F. Towards a sustainable and fit-for-purpose health workforce-lessons from New Zealand. Med. J. Aust. 2012, 1 (Suppl. 3), 32–36. [Google Scholar] [CrossRef]
- Birch, S. Health human resource planning for the new millennium: Inputs in the production of health, illness, and recovery in populations. Can. J. Nurs. Res. 2002, 33, 109–114. [Google Scholar]
- Lennox, L.; Maher, L.; Reed, J. Navigating the sustainability landscape: A systematic review of sustainability approaches in healthcare. Implement. Sci. 2018, 3, 27. [Google Scholar] [CrossRef]
- Dal Poz, M.R.; Sepulveda, H.R.; Costa Couto, M.H.; Godue, C.; Padilla, M.; Cameron, R.; de Andrade Vidaurre Franco, T. Assessment of human resources for health programme implementation in 15 Latin American and Caribbean countries. Hum. Resour. Health 2015, 13, 24. [Google Scholar] [CrossRef]
- WHO Regional Office for Europe. Health and Care Workforce in Europe: Time to Act; WHO Regional Office for Europe: Copenhagen, Denmark, 2022. [Google Scholar]
- Cho, M.; Levin, R. Implementación del plan de acción de recursos humanos en salud y la respuesta a la pandemia por la COVID-19. Rev. Panam. Salud Publica 2022, 46, e52. [Google Scholar] [CrossRef]
- Pan American Health Organization. Plan de Acción Sobre Recursos Humanos Para el Acceso Universal a la Salud y Cobertura Universal de Salud 2018–2023: Progress Report to the 59th Directing Council of PAHO. CD59/INF/16; PAHO: Washington, DC, USA, 2021; Available online: https://www.paho.org/es/documentos/cd59inf16-plan-accion-sobre-recursos-humanos-para-acceso-universal-salud-cobertura (accessed on 15 December 2022).
- Bourgeault, I.L.; Maier, C.B.; Dieleman, M.; Ball, J.; MacKenzie, A.; Nancarrow, S.; Nigenda, G.; Sidat, M. The COVID-19 pandemic presents an opportunity to develop more sustainable health workforces. Hum. Resour. Health 2020, 18, 83. [Google Scholar] [CrossRef] [PubMed]
- Kuhlmann, E.; Batenburg, R.; Dussault, G. Where health workforce governance research meets health services management. Health Serv. Manag. Res. 2016, 29, 21–24. [Google Scholar] [CrossRef]
- Kuhlmann, E.; Batenburg, R.; Dussault, G. Health workforce governance in Europe. Health Policy 2015, 119, 1515–1516. [Google Scholar] [CrossRef]
- Barbazza, E.; Langins, M.; Kluge, H.; Tello, J. Health workforce governance: Processes, tools and actors towards a competent workforce for integrated health services delivery. Health Policy 2015, 119, 1645–1654. [Google Scholar] [CrossRef] [PubMed]
- Fritzen, S.A. Strategic management of the health workforce in developing countries: What have we learned? Hum. Resour. Health 2007, 5, 4. [Google Scholar] [CrossRef] [PubMed]
- Dussault, G.; Buchan, J.; Sermeus, W.; Padaiga, Z. Assessing Future Health Workforce Needs; World Health Organisation: Copenhagen, Denmark, 2010; ISSN 2077-1584. [Google Scholar]
- Padilha, A.; Kasonde, J.; Mukti, G.; Crisp, N.; Takemi, K.; Buch, E. Human resources for universal health coverage: Leadership needed. Bull. World Health Organ. 2013, 91, 800–800A. [Google Scholar] [CrossRef] [PubMed]
- Figueroa, C.A.; Harrison, R.; Chauhan, A.; Meyer, L. Priorities and challenges for health leadership and workforce management globally: A rapid review. BMC Health Serv. Res. 2019, 19, 239. [Google Scholar] [CrossRef] [PubMed]
- Martineau, T.; Ozano, K.; Raven, J.; Mansour, W.; Bay, F.; Nkhoma, D.; Badr, E.; Baral, S.; Regmi, S.; Caffrey, M. Improving health workforce governance: The role of multi-stakeholder coordination mechanisms and human resources for health units in ministries of health. Hum. Resour. Health 2022, 20, 47. [Google Scholar] [CrossRef]
- Hastings, S.E.; Armitage, G.D.; Mallinson, S.; Jackson, K.; Suter, E. Exploring the relationship between governance mechanisms in healthcare and health workforce outcomes: A systematic review. BMC Health Serv. Res. 2014, 14, 479. [Google Scholar] [CrossRef]
- Kuhlmann, E.; Burau, V. Strengthening stakeholder involvement in health workforce governance: Why we need to talk about power. J. Health Serv. Res. Policy 2018, 23, 66–68. [Google Scholar] [CrossRef]
- Cometto, G.; Nartey, E.; Zapata, T.; Kanda, M.; Md, Y.; Narayan, K.; Pritasari, K.; Irufa, A.; Lamichhane, R.; De Silva, D.; et al. Analysing public sector institutional capacity for health workforce governance in the South-East Asia region of WHO. Hum. Resour. Health 2019, 17, 43. [Google Scholar] [CrossRef]
- Voorberg, W.; Bekkers, V.; Flemig, S.; Timeus, K.; Tonurist, P.; Tummers, L. Does co-creation impact public service delivery? The importance of state and governance traditions. Public Money Manag. 2017, 37, 365–372. [Google Scholar] [CrossRef]
- Imison, C.; Buchan, J.; Xavier, S. NHS Workforce Planning: Limitations and Possibilities; King’s Fund: London, UK, 2009; Available online: https://www.kingsfund.org.uk/sites/files/kf/NHS-Workforce-Planning-Candace-Imison-James-Buchan-Su-Xavier-Kings-Fund-November-2009.pdf (accessed on 16 January 2023).
- Ono, T.; Lafortune, G.; Schoenstein, M. Health Workforce Planning in OECD Countries: A Review of 26 Projection Models from 18 Countries; OECD Health Working Papers, No. 62; OECD Publishing: Paris, France, 2013. [Google Scholar] [CrossRef]
- Snowden Hopkins, F. The planning mission before us. In Handbook of Futures Research; Folwes, J., Ed.; Greenwood Press: Westport, CT, USA, 1978; pp. 779–790. ISBN 0837198852. [Google Scholar]
- Bloor, K.; Maynard, A. Planning Human Resources in Health Care: Towards an Economic Approach—An International Comparative Review; CHSRF: Ottawa, ON, Canada, 2003. [Google Scholar]
- Birch, S. Health Workforce Planning: Australia and Canada. In Proceedings of the International Workshop on Health and Social Care Workforce Planning, Dublin, Ireland, 7 June 2022; Available online: https://www.youtube.com/watch?v=HAAfyUUhr90 (accessed on 13 December 2022).
- Bohmer, R.M.J.; Imison, C. Lessons from England’s health care workforce redesign: No quick fixes. Health Aff. 2013, 3, 2025–2031. [Google Scholar] [CrossRef]
- Gorman, D.F. Developing health care workforces for uncertain futures. Acad. Med. 2015, 90, 400–403. [Google Scholar] [CrossRef] [PubMed]
- Richardson, E.; Nino, B. Georgia: Health system review. Health Syst. Transit. 2017, 19, 1–90. Available online: https://eurohealthobservatory.who.int/publications/i/georgia-health-system-review-2017 (accessed on 12 December 2022).
- Kostova Neda, M.; Snezhana, C.; Ponce Ninez, A.; van Ginneken, E.; Winkelmann, J. The former Yugoslav Republic of Macedonia: Health System review. Health Syst. Transit. 2017, 19, 1–160. Available online: https://eurohealthobservatory.who.int/publications/i/the-former-yugoslav-republic-of-macedonia-health-system-review-2017 (accessed on 12 December 2022).
- Onvlee, O.; Kaitelidou, D.; Scotter, C.; Dieleman, M. Navigating the political and technical challenges of developing a national HRH strategy: A case study in Greece. Health Policy 2021, 125, 1574–1579. [Google Scholar] [CrossRef] [PubMed]
- Kroneman, M.; Boerma, W.; van den Berg, M.; Groenewegen, P.; de Jong, J.; van Ginneken, E. The Netherlands: Health system review. Health Syst. Transit. 2016, 18, 1–239. Available online: https://eurohealthobservatory.who.int/publications/i/netherlands-health-system-review-2016 (accessed on 12 December 2022).
- Van Greuningen, M.; Batenburg, R.S.; Van der Velden, L.F.J. Ten years of health workforce planning in the Netherlands: A tentative evaluation of GP planning as an example. Hum. Resour. Health 2012, 10, 21. [Google Scholar] [CrossRef]
- Pearse, J.; Robertson, E.; Brownwood, I.; Cho, O.; Mitchell, S. Building a sustainable health workforce: Using clinical data to inform workforce planning. In Proceedings of the 35th Patient Classification Systems International Conference, Reykjavík, Iceland, 27–30 September 2022; Available online: http://www.pcsinternational.org/conference/PCSI2022/assets/PCSI2022_abstract_74.html (accessed on 12 December 2022).
- Willis, G. Robust Workforce Planning Framework: An Introduction; CfWI Technical Paper Series No. 0001; Centre for Workforce Intelligence: London, UK, 2014; Available online: http://www.cfwi.org.uk/publications/robust-workforce-planning-an-introduction (accessed on 12 December 2022).
- World Health Organization. Models and Tools for Health Workforce Planning and Projections; World Health Organization: Geneva, Switzerland, 2010; pp. 1–16. ISBN 978 92 4 159901 6. [Google Scholar]
- World Health Organization. Health Workforce 2030: Towards a Global Strategy on Human Resources for Health; World Health Organization: Geneva, Switzerland, 2015; ISBN 978 92 4 150862 9. [Google Scholar]
- Dunn, W.N. Public Policy Analysis: An Introduction, 6th ed.; Routledge: New York, NY, USA, 2018; ISBN 9781315181226. [Google Scholar]
- National Health Workforce Planning and Research Collaboration. Alternative Approaches to Health Workforce Planning: Final Report; Health Workforce Australia: Adelaide, Australia, 2011; pp. 1–56. [Google Scholar]
- Rees, G.H.; Crampton, P.; Gauld, R.; MacDonell, S. New Zealand’s health workforce planning should embrace complexity and uncertainty. N. Z. Med. J. 2018, 131, 109–115. Available online: https://journal.nzma.org.nz/journal-articles/new-zealand-s-health-workforce-planning-should-embrace-complexity-and-uncertainty (accessed on 12 December 2022).
- Liwanag, H.J.; Uy, J.; Politico, M.R.; Padilla, M.J.; Arzobal, M.C.; Manuel, K.; Cagouia, A.l.; Tolentino, P.; Frahsa, A.; Ronquillo, K. Cocreation in Health Workforce Planning to Shape the Future of the Health Care System in the Philippines. Glob. Health Sci. Pract. 2022, 10, e2200176. [Google Scholar] [CrossRef]
- Gariboldi, M.I.; Lin, V.; Bland, J.; Auplish, M.; Cawthorne, A. Foresight in the time of COVID-19. Lancet Reg. Health West. Pac. 2021, 6, 100049. [Google Scholar] [CrossRef]
- van der Steen, M. Scenario analysis, forecasting and backcasting as policy tools. In The Routledge Handbook of Policy Tools; Howlett, M., Ed.; Routledge: New York, NY, USA, 2022; pp. 245–256. [Google Scholar] [CrossRef]
- Schmidt, J.M. Policy, planning, intelligence and foresight in government organizations. Foresight 2015, 17, 489–511. [Google Scholar] [CrossRef]
- Rees, G.H. The evolution of New Zealand’s health workforce policy and planning system: A study of workforce governance and health reform. Hum. Resour. Health 2019, 17, 51. [Google Scholar] [CrossRef] [PubMed]
- Quist, J. Backcasting. In Foresight in Organizations: Methods and Tools, 1st ed.; van der Duin, P., Ed.; Routledge: New York, NY, USA, 2016; pp. 145–164. ISBN 9781138692862. [Google Scholar]
- Gilson, L. Introduction to health policy and systems research. Health Policy and Systems Research: A Methodology Reader; Alliance for Health Policy and System Research & World Health Organization: Geneva, Switzerland, 2012; pp. 19–39. ISBN 9789241503136. [Google Scholar]
- Rees, G.H.; Crampton, P.; Gauld, R.; MacDonell, S. Rethinking health workforce planning: Capturing health system social and power interactions through actor analysis. Futures 2018, 99, 16–27. [Google Scholar] [CrossRef]
- Veenman, S.A. Futures studies and uncertainty in public policy: A case study on the ageing population in the Netherlands. Futures 2013, 53, 42–52. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Construct | Construct Description |
|---|---|
| 1 | after a defined period of time, |
| 2 | a program, clinical intervention, and/or implementation strategies continue to be delivered and/or, |
| 3 | individual behavior change (i.e., clinician, patient) is maintained, |
| 4 | the program and individual behavior change may evolve or adapt while, |
| 5 | continuing to produce benefits for individuals/systems. |
| Planning Type | Description | Weaknesses | Example Countries |
|---|---|---|---|
| Serendipitous replacement | Little formal planning intervention by Governments. Reliant on: Output of health educators, and Cultural career preference | No consideration of system demand. Reduced ability of health system to develop and embrace changes that can deliver patient benefits. | Georgia [48], North Macedonia [49] |
| Reactive replacement | Focused on maintain existing establishments of staff. Often characterized by: Ratio based models, and Reactive health workforce planning | Mismatched staffing and system demand. Prone to demographic shocks. Slow to react to change. Poor data leads to workforce replacement lagging the losses. | Greece [50] |
| Managed production | Many countries use a “Stock and Flow” planning model which uses a methodology that; Estimates replenishment level for the workforce, Estimates the workforce demand requirement, and Calculates the optimal yearly inflow balance demand and supply | Needs government support and actor consensus. Can be layered. | Netherlands [51,52], Japan [42]. |
| Strategic health workforce planning | Analysis of the complex dynamics within the health system. Relies on expert qualitative opinions of future need. Use has shown that planning like this is helpful in identifying general directions of planning. Planning for skills or anticipating the need for skills can be more effective. | Planning for specific professions is very complex. Can have wide confidence margins. | Australia [53], Canada [42], UK [54] |
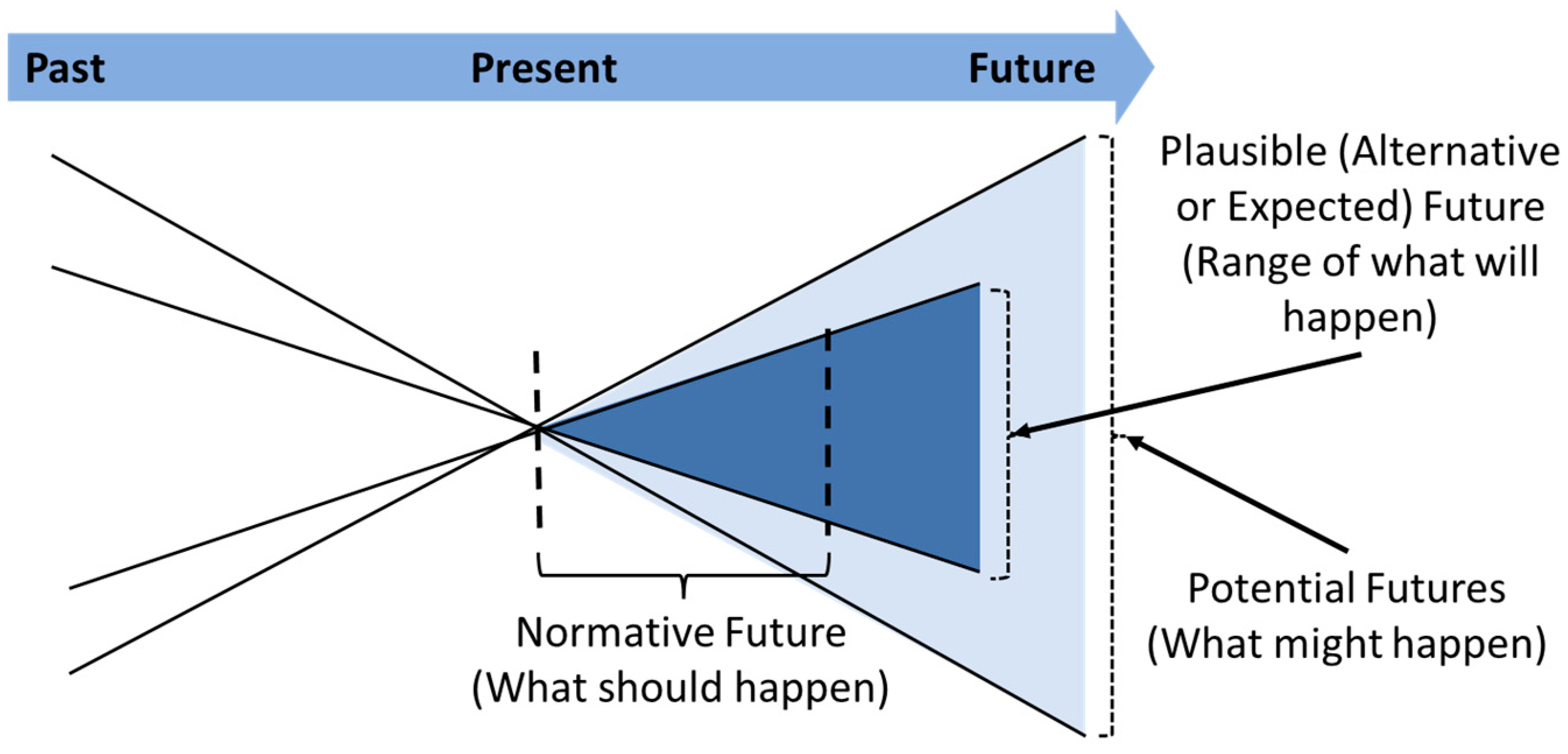
| Future Type | Description |
|---|---|
| Possible futures | Possible futures are future societal states that may occur, and not eventual societal states that do occur. A future state is never certain until it occurs, and there are many possible futures. |
| Plausible futures | Evidence or theory based future states that are likely if policymakers do not intervene to redirect the course of events. The future that is expected if events, as they are, run their course. |
| Normative futures | Societal futures that are consistent with future values, dictated by what ought to be done for the future to be realized. Normative futures narrow the range of potential and plausible futures by linking forecasts to the achievement of objectives and values. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rees, G.H.; James, R.; Samadashvili, L.; Scotter, C. Are Sustainable Health Workforces Possible? Issues and a Possible Remedy. Sustainability 2023, 15, 3596. https://doi.org/10.3390/su15043596
Rees GH, James R, Samadashvili L, Scotter C. Are Sustainable Health Workforces Possible? Issues and a Possible Remedy. Sustainability. 2023; 15(4):3596. https://doi.org/10.3390/su15043596
Chicago/Turabian StyleRees, Gareth H, Rosemary James, Levan Samadashvili, and Cris Scotter. 2023. "Are Sustainable Health Workforces Possible? Issues and a Possible Remedy" Sustainability 15, no. 4: 3596. https://doi.org/10.3390/su15043596
APA StyleRees, G. H., James, R., Samadashvili, L., & Scotter, C. (2023). Are Sustainable Health Workforces Possible? Issues and a Possible Remedy. Sustainability, 15(4), 3596. https://doi.org/10.3390/su15043596