
A Study on Model of Psychotherapy Narration Focused on Mental Well-Being for Stress Management in the Elderly


Abstract
1. Introduction
- RQ1.
- What is the psychotherapy-narration model focusing on mental well-being for stress management in the elderly?
- RQ2.
- What is the level of satisfaction (by specific situation and emotion) with the psychotherapy-narration model focusing on mental well-being for stress management in the elderly?
2. Psychotherapy Narration
2.1. Person-Centered-Theory
2.2. Positive Psychology
2.3. Cognitive Behavioral Therapy
2.4. Acceptance and Commitment Therapy
2.5. Mindfulness-Based Stress Reduction
3. Methods
3.1. Study Design (Proposed Psychological Narrative)
3.2. Study Subjects
3.3. Study Instrument and Data Collection
3.4. Data Analysis
3.4.1. Frequency Analysis
3.4.2. Chi-Square Test
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- The Encyclopedia of Doosan. The Problem of the Aged. Available online: http://www.doopedia.co.kr/ (accessed on 12 December 2022).
- Rowe, J.W.; Kahn, R.L. Successful Ageing. Gerontologist 1997, 37, 433–440. [Google Scholar] [CrossRef] [PubMed]
- Barer, B.M.; Johnson, C.L. Problems and problem solving among aging White and Black Americans. J. Aging Stud. 2003, 17, 323–340. [Google Scholar] [CrossRef]
- Statistics Korea. Senior Citizen Statistics. Available online: http://kosis.kr/ (accessed on 9 September 2022).
- Hooyman, N.; Kawamoto, K.; Kiyak, H.A. Aging Matters: An Introduction to Social Gerontology; Pearson Higher Ed.: San Francisco, CA, USA, 2014. [Google Scholar]
- Yang, S.M.; Oh, Y.J. Effect of related-variables on stress of the rural elderly. J. Welf. Aged 2005, 30, 123–140. [Google Scholar]
- Bae, M.J. The Effects of Integrated Group Art Therapy Program for Enhancing Self-Compassion among the Depressed Elderly Living Alone. Ph.D. Thesis, Hanyang University, Seoul, Republic of Korea, 2018. [Google Scholar]
- Kim, D.J. Social difficulties of the aged people who live alone and alternative welfare solutions. Korean Acad. Soc. Welf. Support 2012, 7, 217–239. [Google Scholar]
- Shin, C.H. The study on effects of objective life attributes on depression of elderly mediated by life-satisfaction. J. Korean Gerontol. Soc. 2010, 30, 453–469. [Google Scholar]
- Lim, E.J. The relationship between depression, cognitive function and the instrumental activities of daily living of elderly women living alone. J. Korea Acad. Ind. Coop. Soc. 2013, 14, 1849–1856. [Google Scholar]
- Kim, S.E.; Lee, M.H. What are the problems(difficulties) experienced by the elderly in Korea? Korea Assoc. Policy Anal. Eval. 2015, 25, 1–22. [Google Scholar]
- Kim, M.H.; Min, K.H. Emotional experience and emotion regulation in old age. Korean J. Psychol. Gen. 2004, 23, 1–21. [Google Scholar]
- Kim, A.; Kim, Y.; Rhee, J.; Lee, S.; Jeong, Y.; Lee, J.; Yoo, Y.; Kim, H.; So, H.; Park, J. A Study on Emotions to Improve the Quality of Life of South Korean Senior Patients Residing in Convalescent Hospitals. Int. J. Environ. Res. Public Health 2022, 19, 14480. [Google Scholar] [CrossRef]
- Ryff, C.D.; Singer, B. The contours of positive human health. Psychol. Inq. 1998, 9, 1–28. [Google Scholar] [CrossRef]
- Fava, G.A.; Rafanelli, C.; Grandi, S.; Conti, S.; Belluardo, P. Prevention of recurrent depression with cognitive behavioral therapy: Preliminary findings. Arch. Gen. Psychiatry 1998, 55, 816–820. [Google Scholar] [CrossRef]
- Erica, K. Treatment of social anxiety disorder using online virtual environments in second life. Behav. Ther. 2013, 44, 51–61. [Google Scholar]
- Kim, J.Y.; Lee, Y.H. The Trend and Issues on Untact Counseling and Psychotherapy: Focusing on Journal Papers (2010–2020.6). J. Learn. Cent. Curric. Instr. 2021, 21, 775–805. [Google Scholar] [CrossRef]
- Chung, A.R. A phenomenological study on the experience of non-face-to-face videoconferencing counseling of college students. J. Educ. Innov. Res. 2022, 32, 331–355. [Google Scholar]
- Kim, M.J.; Ha, C.S.; Shim, H.W. Comparative study of Lee Whang’s SimHak and Adler, Roser’s psychology-On the human nature and way of self-realization. Stud. Philos. East West 2008, 50, 339–363. [Google Scholar]
- Hwang, Y.M.; Jang, S.H. Theory comparison study of Carl R. Rogers’s Person Centered Therapy and Narrative Therapy. Korean J. Couns. Psychother. 2012, 3, 13–29. [Google Scholar]
- Corey, G. Theory and Practice of Counseling and Psychotherapy; Cengage Learning: Belmont, CA, USA, 2011. [Google Scholar]
- Myers, D.G.; Diener, E. Who is happy? Psychol. Sci. 1995, 6, 10–19. [Google Scholar] [CrossRef]
- Kwon, S.M. Positive Psychology; Hakjisa: Seoul, Republic of Korea, 2008. [Google Scholar]
- Seligman, M.E. Positive psychology, positive prevention, and positive therapy. Handb. Posit. Psychol. 2002, 2, 3–12. [Google Scholar]
- Kim, M.A.; Jung, M.J. The effects on an education program based on positive psychology for the depressed elderly living alone. J. Korean Home Manag. Assoc. 2020, 38, 125–141. [Google Scholar] [CrossRef]
- Luthans, F. The need for and meaning of positive organizational behavior. J. Organ. Behav. Int. J. Ind. Occup. Organ. Psychol. Behav. 2002, 23, 695–706. [Google Scholar] [CrossRef]
- Frisch, M.B. Quality of life therapy and assessment in health care. Clin. Psychol. Sci. Pract. 1998, 5, 19. [Google Scholar] [CrossRef]
- Frisch, M.B. Evidence-based well-being/positive psychology assessment and intervention with quality of life therapy and coaching and the Quality of Life Inventory (QOLI). Soc. Indic. Res. 2013, 114, 193–227. [Google Scholar] [CrossRef]
- Rodrigue, J.R.; Baz, M.A.; Widows, M.R.; Ehlers, S.L. A randomized evaluation of quality-of-life therapy with patients awaiting lung transplantation. Am. J. Transplant. 2005, 5, 2425–2432. [Google Scholar] [CrossRef] [PubMed]
- Fava, G.A.; Ruini, C. Development and characteristics of a well-being enhancing psychotherapeutic strategy: Well-being therapy. J. Behav. Ther. Exp. Psychiatry 2003, 34, 45–63. [Google Scholar] [CrossRef] [PubMed]
- Ellis, A. Reason and Emotion in Psychotherapy; Lyle Stuart: New York, NY, USA, 1962. [Google Scholar]
- Beck, A.T. Cognitive Therapy and the Emotional Disorders; Penguin: New York, NY, USA, 1979. [Google Scholar]
- Engels, G.I.; Vermey, M. Efficacy of nonmedical treatments of depression in elders: A quantitative analysis. J. Clin. Geropsychol. 1997, 3, 17–35. [Google Scholar]
- Laidlaw, K. An empirical review of cognitive therapy for late life depression: Does research evidence suggest adaptations are necessary for cognitive therapy with older adults? Clin. Psychol. Psychother. Int. J. Theory Pract. 2001, 8, 1–14. [Google Scholar] [CrossRef]
- Kim, J.H.; Kim, S.J. Understanding and Managing Stress; Sigma Press: Seoul, Republic of Korea, 2002. [Google Scholar]
- Neenan, M.; Dryden, W. Cognitive Behaviour Therapy: 100 Key Points and Techniques; Routledge: London, UK, 2014. [Google Scholar]
- Palmer, S.; Szymanska, K. Cognitive Behavioural Coaching: An Integrative Approach. In Handbook of Coaching Psychology; Routledge: London, UK, 2018. [Google Scholar]
- Salkovskis, P.M.; Wahl, K. Treating obsessional problems using cognitive-behavioural therapy. Cogn. Ther. Across Lifesp. Theory Res. Pract. 2003, 1, 138–171. [Google Scholar]
- Konnert, C.; Dobson, K.; Stelmach, L. The prevention of depression in nursing home residents: A randomized clinical trial of cognitive-behavioral therapy. Aging Ment. Health 2009, 13, 288–299. [Google Scholar] [CrossRef]
- Hayes, S.C.; Strosahl, K.; Wilson, K.G.; Bissett, R.T.; Pistorello, J.; Toarmino, D.; Polusny, M.A.; Dykstra, T.A.; Batten, S.V.; Bergan, J.; et al. Measuring experiential avoidance: A preliminary test of a working model. Psychol. Rec. 2004, 54, 553–578. [Google Scholar] [CrossRef]
- Moon, H.M. The Third wave of cognitive-behavioral therapy. Korean J. Couns. Psychother. 2005, 17, 15. [Google Scholar]
- Song, J.H. Development of ACT Group Counseling Program and Its Effect on Parenting Variable. Doctoral Dissertation, Hanyang University, Seoul, Republic of Korea, 2019. [Google Scholar]
- Shin, J.S.; Lee, B.K.; Lee, H.K. The effects of acceptance and mindfulness on catastrophizing, depression, and pain in chronic pain patients: The moderating effects of acceptance and mindfulness. Stressresearch 2014, 22, 11–21. [Google Scholar] [CrossRef]
- Kim, E.H.; Bae, J.E. Development and Effects of Elderly Depression Management Program Applying Acceptance and Commitment Therapy. Korean Assoc. Crisis Emerg. Manag. 2020, 1, 100–101. [Google Scholar]
- Kim, G.R.; Kim, I.S. The meta-analysis of the effects of meditation programs of the elderly. J. Korea Gerontol. Soc. 2018, 38, 47–63. [Google Scholar]
- Lee, S.G. A Study on the Effects of Mindfulness Meditation on the Reduction of Stress in Contemporary; Ningin Graduate Schoole of Buddhist: Gyeonggi, Republic of Korea, 2018. [Google Scholar]
- Kabat-Zinn, J. Wherever You Go, There You Are: Mindfulness Meditation in Everyday Life; Hachette Books: New York, NY, USA, 2009. [Google Scholar]
- Jung, J.Y.; Park, S.H. Sati in early Buddhism and mindfulness in current psychology: A proposal for establishing the construct of mindfulness. Korean J. Couns. Psychother. 2010, 22, 1–32. [Google Scholar]
- Lee, S.S.; Lee, K.J. The stress, social support and psychological well-being of the elderly. J. Korean Gerontol. Soc. 2002, 22, 1–20. [Google Scholar]
- Kil, T.Y. Study on the quality of life in the elderly in Korea using qualitative interpretive Meta-Synthesis. Korea Glob. Aff. 2021, 5, 5–36. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
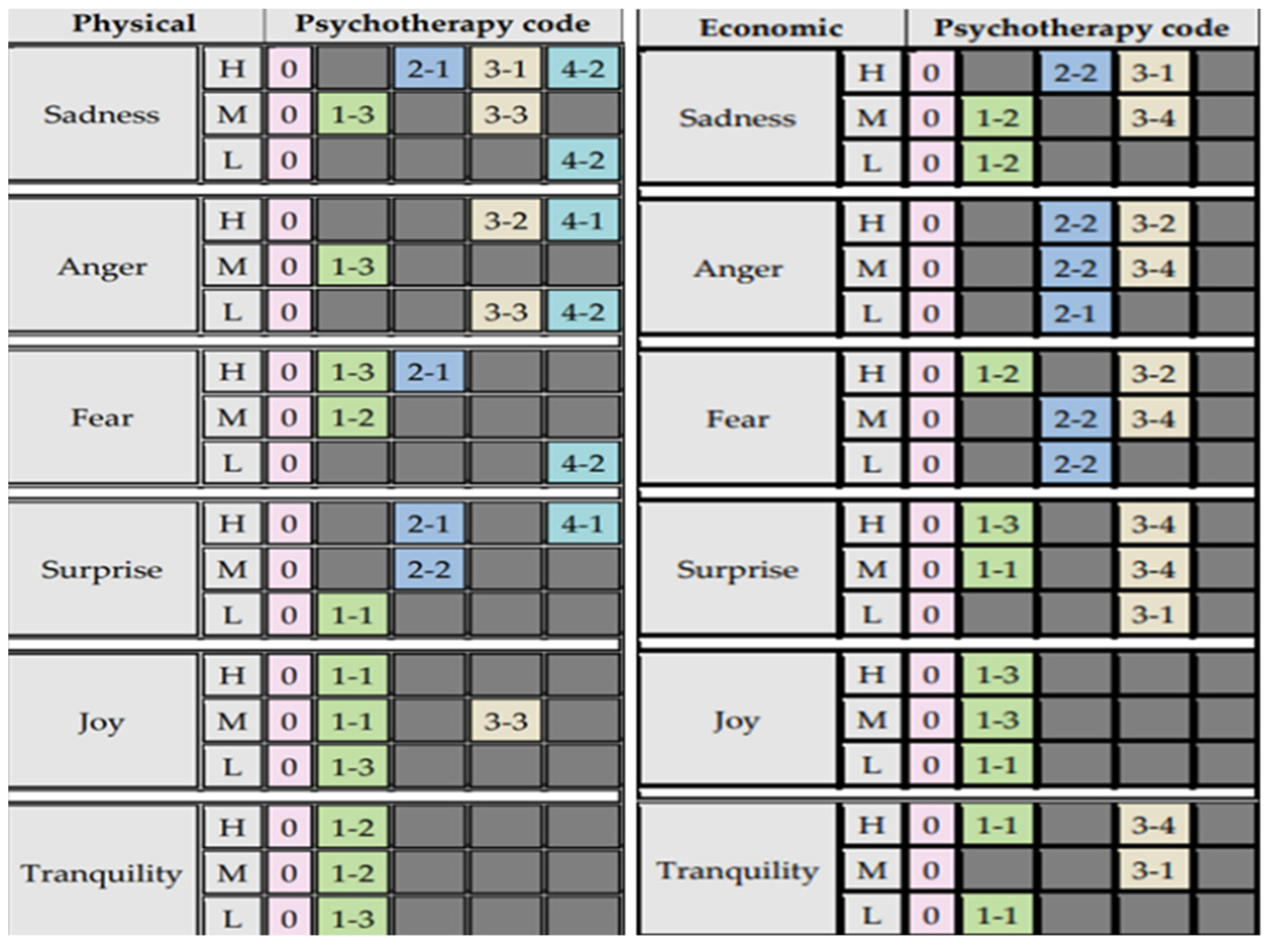
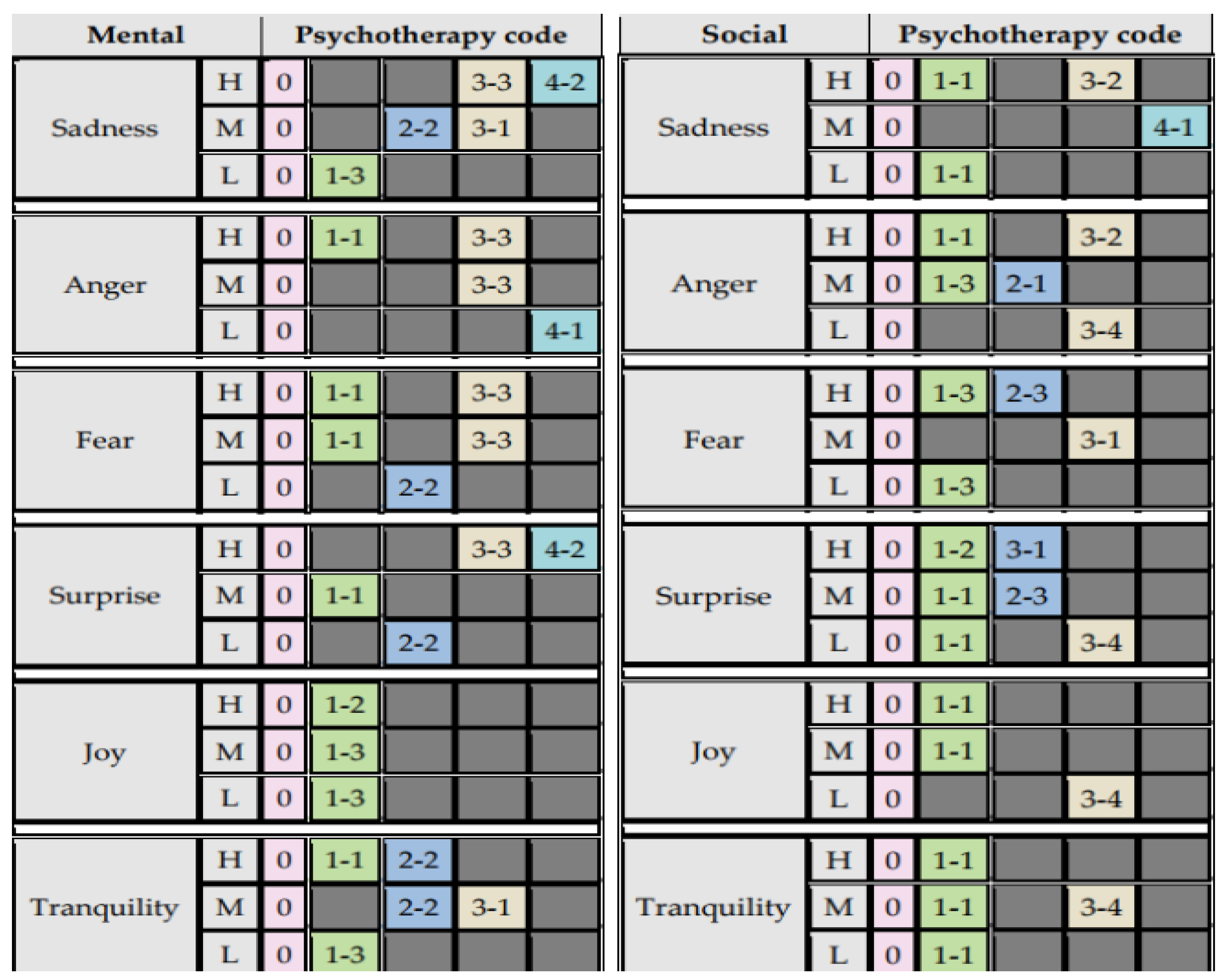
| Psychotherapy Type | Code | Treatments | |
|---|---|---|---|
| Person-centered theory (PCT) | 0 | Narrator attitude | |
| Positive psychology | 1 | 1 | Positive-psychological capital |
| 2 | Quality of life coaching | ||
| 3 | Well-being therapy (WBT) | ||
| Cognitive behavioral therapy (CBT) | 2 | 1 | Relaxation techniques |
| 2 | Cognitive behavior coaching | ||
| 3 | Exposure therapy | ||
| Acceptance and commitment therapy (ACT) | 3 | 1 | Acceptance |
| 2 | Cognitive defusion | ||
| 3 | Contact with the present moment | ||
| 4 | Values | ||
| Mindfulness-based stress reduction program (MBSR) | 4 | 1 | Watching the breath |
| 2 | Body scan | ||
| n | Proportion (%) | ||
|---|---|---|---|
| Gender | Male | 34 | 34.0 |
| Female | 66 | 66.0 | |
| Age group | >80 | 4 | 4.0 |
| 70–79 | 4 | 4.0 | |
| 65–69 | 92 | 92.0 | |
| Highest academic level | Elementary | 5 | 5.0 |
| Middle school | 3 | 3.0 | |
| High school | 32 | 32.0 | |
| University | 53 | 53.0 | |
| Graduate school | 7 | 7.0 | |
| Major income source | Self-employed | 7 | 7.0 |
| Real estate | 15 | 15.0 | |
| Pension | 39 | 39.0 | |
| Family members (e.g., children) | 35 | 35.0 | |
| Other | 4 | 4.0 | |
| Preferred Mechanism to Deal with Stress [Respondent Count and Proportion (%)] | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Walking | Eating | Drinking or Smoking | Reading | TV | Conversation | Shopping | Religion | Other | |
| Male | 15 (44.1) | - | 4 (11.8) | - | 5 (14.7) | 7 (20.6) | 1 (2.9) | 1 (2.9) | 1 (2.9) |
| Female | 34 (51.5) | 3 (4.5) | - | 1 (1.5) | 4 (6.1) | 16 (24.2) | 5 (7.6) | 2 (3.0) | 1 (1.5) |
| Total | 46 (46.0) | 3 (3.0) | 4 (4.0) | 1 (1.0) | 9 (9.0) | 23 (23.0) | 6 (6.0) | 3 (3.0) | 2 (2.0) |
| Chi-square = 13.102, p-value = 0.108 | |||||||||
| Stress Situations [Respondent Count and Proportion (%)] | |||||
|---|---|---|---|---|---|
| Health | Social | Mental | Economy | Total | |
| Male | 19 (55.9) | 6 (17.6) | 4 (11.8) | 5 (14.7) | 34 (100.0) |
| Female | 39 (59.1) | 10 (15.2) | 8 (12.1) | 9 (13.6) | 66 (100.0) |
| Total | 58 (58.0) | 16 (16.0) | 12 (12.0) | 14 (14.0) | 100 (100.0) |
| Chi-square = 0.148, p-value = 0.986 | |||||
| Emotions under Stress Situations [Respondent Count and Proportion (%)] | |||||
|---|---|---|---|---|---|
| Sadness | Anger | Fear | Surprise | Tranquility | Total |
| 8 (23.5) | 5 (14.7) | 15 (44.1) | 6 (17.6) | - | 34 (100.0) |
| 28 (42.4) | 3 (4.5) | 25 (37.9) | 9 (13.6) | 1 (1.5) | 66 (100.0) |
| 36 (36.0) | 8 (8.0) | 40 (40.0) | 15 (15.0) | 1 (1.0) | 100 (100.0) |
| Chi-Square: 6.095, p-value: 0.192 | |||||
| n (%) | Intensity [Respondent Count and Proportion (%)] | ||||||
|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | |||
| Health | Sadness | 18 (31.0) | - | 1 (5.6) | 7 (38.9) | 6 (33.3) | 4 (22.2) |
| Anger | 2 (3.4) | - | - | - | 1 (50.0) | 1 (50.0) | |
| Fear | 26 (44.8) | - | 4 (15.4) | 8 (30.8) | 11 (42.3) | 3 (11.5) | |
| Surprise | 11 (19.0) | - | - | 6 (54.5) | 3 (27.3) | 2 (18.2) | |
| Tranquility | 1 (1.7) | - | - | 1 (100.0) | - | - | |
| Social | Sadness | 9 (56.3) | - | - | 4 (44.4) | 4 (44.4) | 1 (11.1) |
| Anger | 3 (18.8) | - | - | 1 (33.3) | 2 (66.7) | - | |
| Fear | 1 (6.3) | - | - | - | 1 (100.0) | - | |
| Surprise | 3 (18.8) | - | 1 (33.3) | 2 (66.7) | - | - | |
| Tranquility | - | - | - | - | - | - | |
| Mental | Sadness | 7 (58.3) | - | - | 4 (57.1) | 3 (42.9) | - |
| Anger | 2 (16.7) | - | - | - | 1 (50.0) | 1 (50.0) | |
| Fear | 3 (25.0) | - | - | 1 (33.3) | 2 (66.7) | - | |
| Surprise | - | - | - | - | - | - | |
| Tranquility | - | - | - | - | - | - | |
| Economic | Sadness | 2 (14.3) | - | - | 1 (50.0) | 1 (50.0) | - |
| Anger | 1 (7.1) | - | - | - | 1 (100.0) | - | |
| Fear | 10 (71.4) | 1 (10.0) | 1 (10.0) | 4 (40.0) | 2 (20.0) | 2 (20.0) | |
| Surprise | 1 (7.1) | - | - | - | 1 (100.0) | - | |
| Tranquility | - | - | - | - | - | - | |
| Situation Type | Emotion Intensity [Respondent Count] | ||||||
|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | Summary | ||
| Health | score | - | 3.0 | 3.68 | 4.05 | 4.0 | 3.81 |
| n | - | 5 | 22 | 21 | 10 | 58 | |
| Social | score | - | 4.0 | 3.57 | 3.43 | 5.0 | 3.63 |
| n | - | 1 | 7 | 7 | 1 | 16 | |
| Mental | score | - | - | 2.8 | 4.17 | 3.0 | 3.5 |
| n | - | - | 5 | 6 | 1 | 12 | |
| Economic | score | 4.0 | 5.0 | 3.4 | 3.6 | 3.0 | 3.57 |
| n | 1 | 1 | 5 | 5 | 2 | 14 | |
| Summary | score | 4.0 | 3.43 | 3.51 | 3.90 | 3.86 | 3.71 |
| n | 1 | 7 | 39 | 39 | 14 | 100 | |
| Situation Type | Emotion Intensity | ||||||
|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | Summary | ||
| Sadness | score | - | 4.0 | 3.31 | 4.21 | 4.4 | 3.83 |
| n | - | 1 | 16 | 14 | 5 | 36 | |
| Anger | score | - | - | 3.0 | 3.2 | 2.5 | 3.0 |
| n | - | - | 1 | 5 | 2 | 8 | |
| Fear | score | 4.0 | 3.2 | 3.62 | 3.81 | 3.6 | 3.65 |
| n | 1 | 5 | 13 | 16 | 5 | 40 | |
| Surprise | score | - | 4.0 | 3.75 | 4.0 | 4.5 | 3.93 |
| n | - | 1 | 8 | 4 | 2 | 15 | |
| Tranquility | score | - | - | 4.0 | - | - | 4.0 |
| n | - | - | 1 | - | - | 1 | |
| Summary | score | 4.0 | 3.43 | 3.51 | 3.90 | 3.86 | 3.71 |
| n | 1 | 7 | 39 | 39 | 14 | 100 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, E.; Kim, S.; Rhee, J. A Study on Model of Psychotherapy Narration Focused on Mental Well-Being for Stress Management in the Elderly. Sustainability 2023, 15, 2656. https://doi.org/10.3390/su15032656
Kim E, Kim S, Rhee J. A Study on Model of Psychotherapy Narration Focused on Mental Well-Being for Stress Management in the Elderly. Sustainability. 2023; 15(3):2656. https://doi.org/10.3390/su15032656
Chicago/Turabian StyleKim, Eunyoung, Seongjoon Kim, and Jongtae Rhee. 2023. "A Study on Model of Psychotherapy Narration Focused on Mental Well-Being for Stress Management in the Elderly" Sustainability 15, no. 3: 2656. https://doi.org/10.3390/su15032656
APA StyleKim, E., Kim, S., & Rhee, J. (2023). A Study on Model of Psychotherapy Narration Focused on Mental Well-Being for Stress Management in the Elderly. Sustainability, 15(3), 2656. https://doi.org/10.3390/su15032656