
Impact of the COVID-19 Pandemic on Routine Immunization Programs in Northern Nigeria


Abstract
1. Introduction
1.1. Background
1.2. Study Rationale
1.3. Objectives
- To determine the effects of the pandemic on RI programs, focusing on L&G, M&E (SS), CE, the VSC, HFM, and SD in six northern Nigerian states;
- To explore the perception of key stakeholders at different implementation levels (state, local government areas (LGAs), healthcare facilities (HFs), and the community) on the impact of COVID-19 on RI systems and services in six northern Nigerian states;
- To discuss the implications of the findings for RI and PHC program policies and implementation.
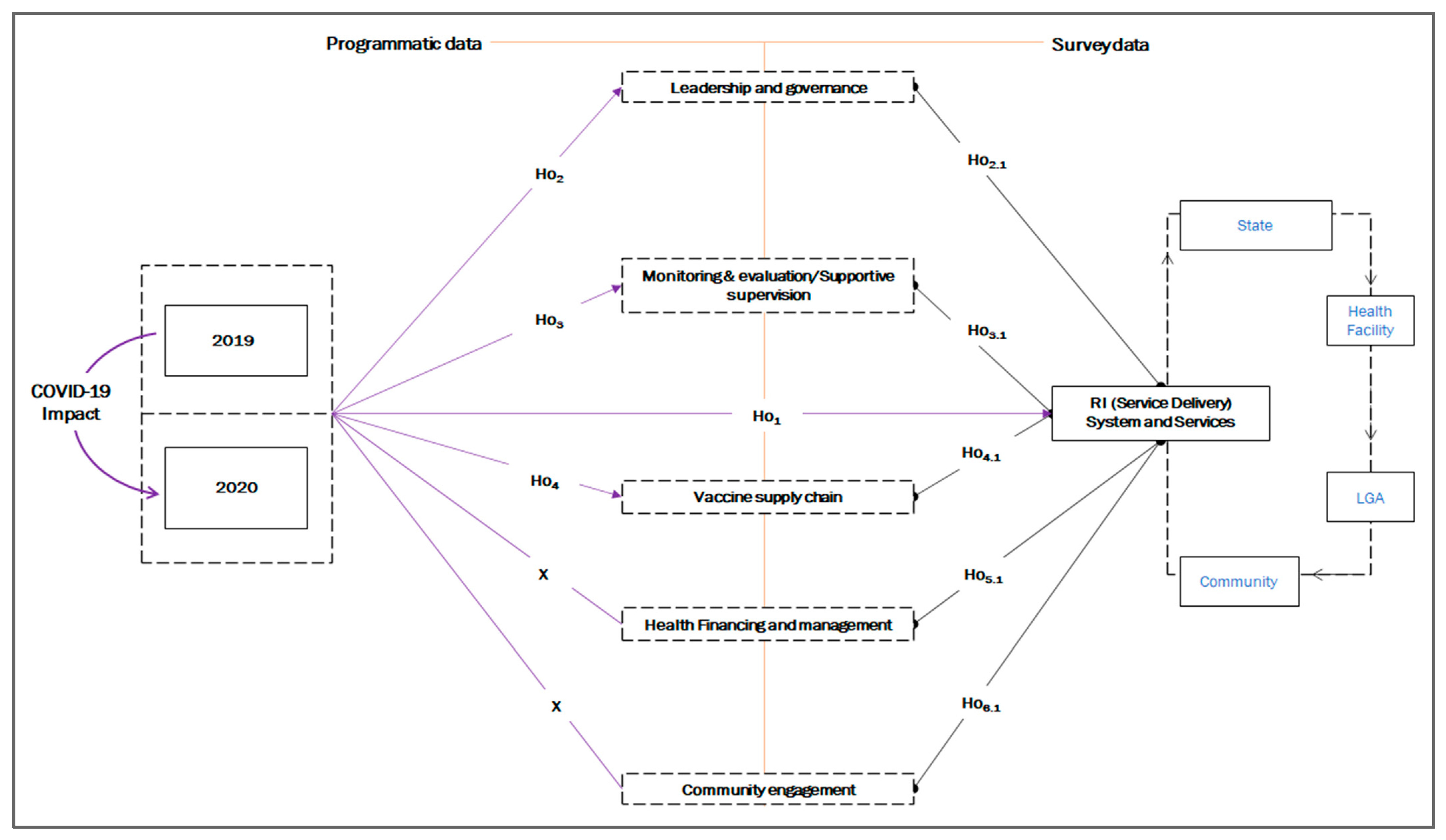
1.4. Analysis Framework and Research Hypothesis
1.5. Programmatic Themes
- Ho1: There was a change in SD due to the COVID-19 pandemic;
- Ho2: COVID-19 affected different L&G activities;
- Ho3: M&E (SS) were affected by the COVID-19 pandemic;
- Ho4: COVID-19 affected the VSC.
1.6. Survey Themes
- Ho2.1: The impact of COVID-19 on L&G directly affected RI SD;
- Ho3.1: The impact of COVID-19 on M&E (SS) directly affected RI SD;
- Ho5.1: The impact of the COVID-19 pandemic on the VSC directly affected RI SD;
- Ho6.1: The impact of the COVID-19 pandemic on HFM systems directly affected RI SD;
- Ho2.1: The impact of COVID-19 on CE directly affected RI SD.
2. Materials and Methods
2.1. Study Design
2.2. Study Setting
2.3. Study Sampling
2.3.1. Sample Size
2.3.2. Sampling Technique
2.3.3. Selection Criteria
2.4. Instrument Design
2.5. Data Collection
2.6. Data Sources and Variables
2.6.1. Secondary (Programmatic) Data
2.6.2. Primary (Survey) Data
2.6.3. Variables
2.7. Data Management and Analysis
2.7.1. Statistical Analysis
2.7.2. Thematic Analysis
3. Results
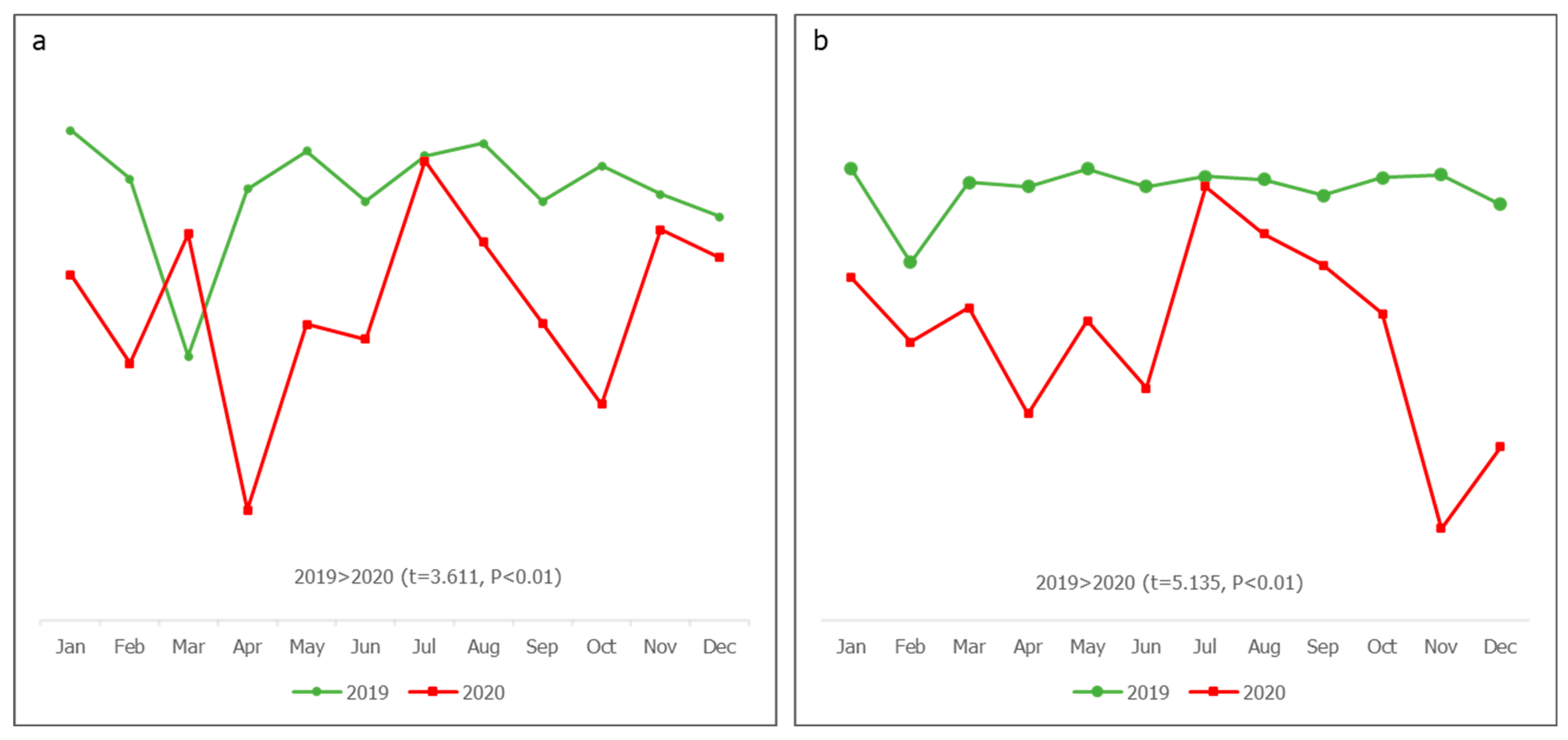
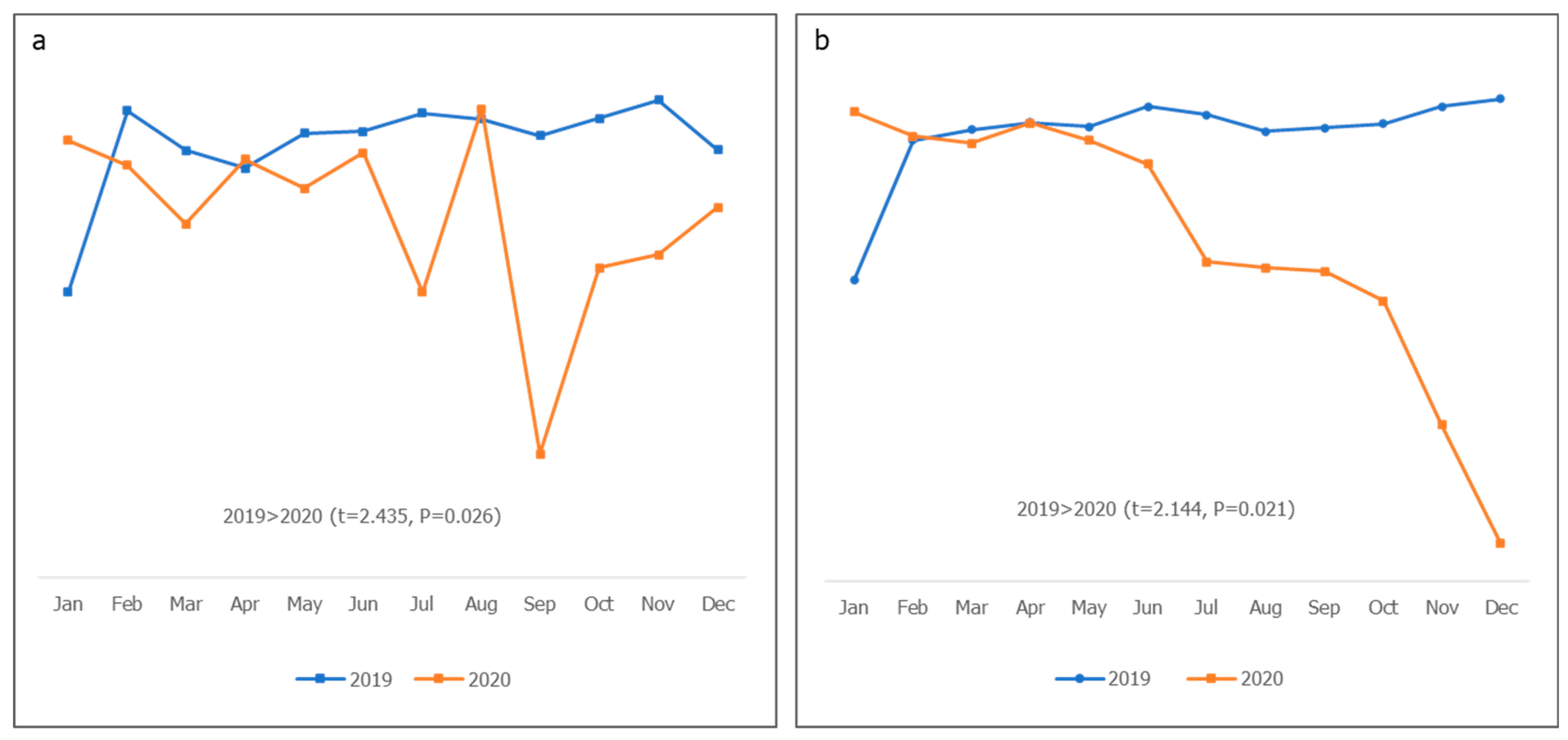
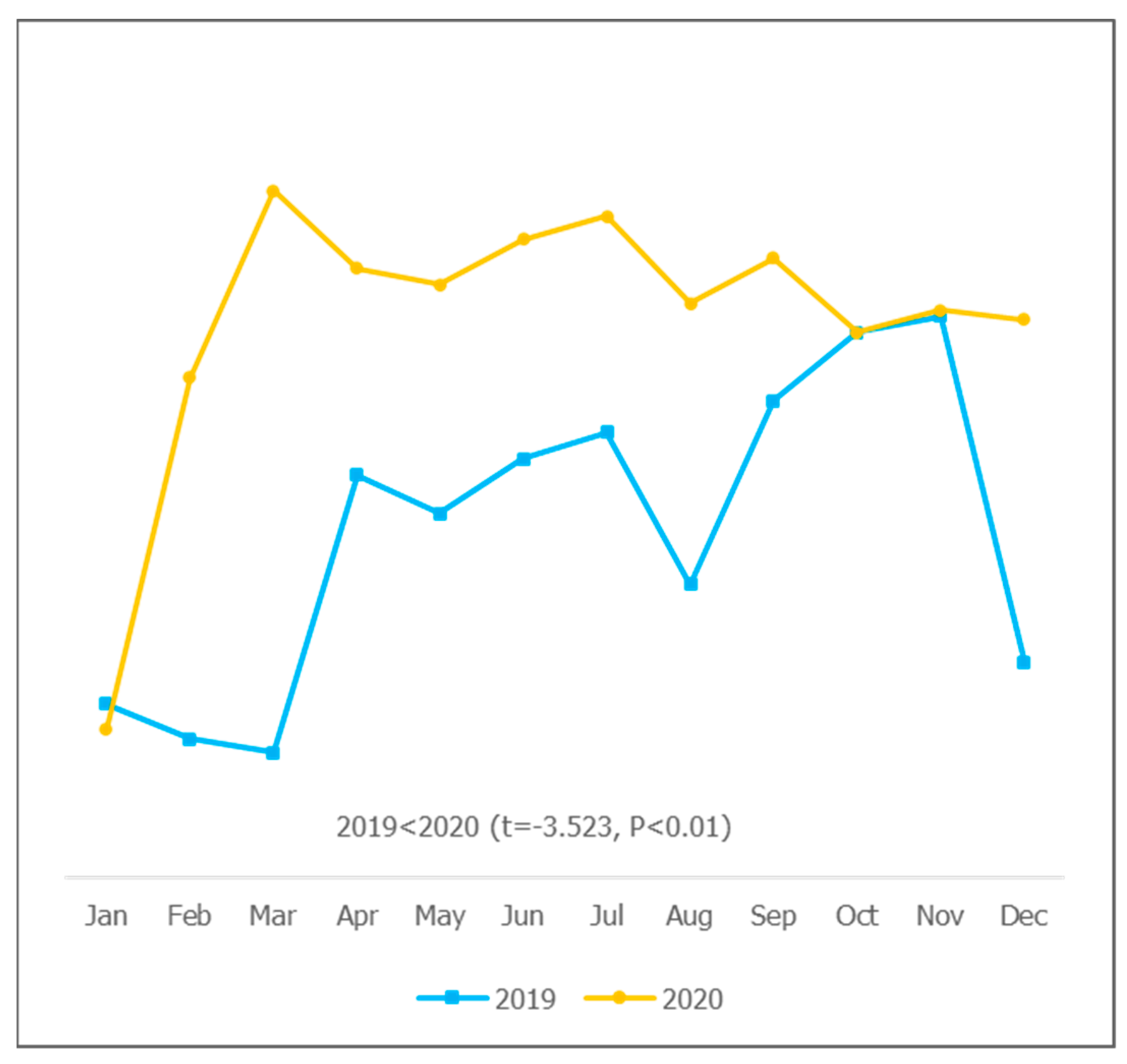
3.1. Programmatic Data Analysis
3.2. Survey Data Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CB | capacity building |
| CE | community engagement |
| CFI | comparative fit index |
| DVD | digital vaccine delivery |
| DPT | diphtheria, tetanus, and pertussis |
| EOC | emergency operation center |
| FGD | focused group discussion |
| GLS | generalized least square |
| GFI | goodness-of-fit index |
| HCD | human-centered design |
| HF | health facility |
| HFM | health financing and management |
| IFRC | International Federation of Red Cross and Red Crescent Societies |
| IMOP | integrated medical outreach program |
| ISS | integrated supportive supervision |
| KMO | Kaiser–Meyer–Olkin |
| LGA | local government area |
| L&G | leadership and governance |
| M&E/SS | monitoring and evaluation/supportive supervision |
| NCDC | Nigeria Centers for Disease Control |
| NPI | national provider identifier |
| OECD | Organization for Economic Cooperation and Development |
| PIRI | periodic intensification of routine immunization |
| PCA | principal component analysis |
| PHC | primary health care |
| PPE | personal protective equipment |
| RI | routine immunization |
| SD | service delivery |
| SEM | structural equation modeling |
| SPSS | Statistics Package for Social Science |
| TWG | technical working group |
| UNICEF | United Nations Children Funds |
| USAID | United States Agency for International Development |
| VSCL | vaccine supply chain logistics |
| WG | working group |
| WHO | World Health Organization |
Appendix A
- To what extent has the COVID-19 pandemic affected the performance of RI programs in the six northern Nigerian states in terms of:
- a.
- Leadership and governance;
- b.
- Service delivery;
- c.
- Monitoring and evaluation/supportive supervision;
- d.
- Community engagement;
- e.
- The caccine supply chain;
- f.
- Funding and financial management;
- g.
- Capacity building.
- What was the performance of the RI program during pre-pandemic periods and how has this changed?
- What adaptive measures were utilized and how did they influence the RI program during the COVID-19 pandemic?
- Which stakeholders, processes, and factors were responsible for/have contributed to the resilience of the RI program amidst the pandemic strains?
- What are the persisting challenges?
- What policy and program changes can be made to bolster the existing RI program and support the integration of COVID-19 interventions?
References
- Liu, J.; Liao, X.; Qian, S.; Yuan, J.; Wang, F.; Liu, Y.; Wang, Z.; Wang, F.-S.; Liu, L.; Zhang, Z. Community transmission of severe acute respiratory syndrome Coronavirus 2, Shenzhen, China, 2020. Emerg. Infect. Dis. 2020, 26, 1320–1323. [Google Scholar] [CrossRef] [PubMed]
- Li, Q. An Outbreak of NCIP (2019-nCoV) Infection in China—Wuhan, Hubei Province, 2019−2020. China CDC Wkly. 2020, 2, 79–80. [Google Scholar] [CrossRef]
- NHS. Landmark Moment as First NHS Patient Receives COVID-19 Vaccination. 2020. Available online: https://www.england.nhs.uk/2020/12/landmark-moment-as-first-nhs-patient-receives-covid-19-vaccination/ (accessed on 19 October 2022).
- OCHA Services. First Case of Coronavirus Disease Confirmed in Nigeria—Nigeria. Available online: https://reliefweb.int/report/nigeria/first-case-coronavirus-disease-confirmed-nigeria (accessed on 19 October 2022).
- NCDC. NCDC Coronavirus COVID-19 Microsite. 2022. Available online: https://covid19.ncdc.gov.ng/advisory/ (accessed on 19 October 2022).
- GAVI. Combining COVID-19 and Routine Vaccination: Nigeria Implements a ‘Whole Family’ Approach. Available online: https://www.gavi.org/vaccineswork/combining-covid-19-and-routine-vaccination-nigeria-implements-whole-family-approach?gclid=Cj0KCQjw6pOTBhCTARIsAHF23fI2oGsW8VwCEdYfjFrVquJm6PPpW0NOMp_3rq0ZjMbFusJ1L4zyGyAaApeOEALw_wcB (accessed on 10 September 2022).
- Mader, S.; Rüttenauer, T. The Effects of Non-pharmaceutical Interventions on COVID-19 Mortality: A Generalized Synthetic Control Approach Across 169 Countries. Front. Public Health 2022, 10, 820642. [Google Scholar] [CrossRef] [PubMed]
- Watson, O.J.; Barnsley, G.; Toor, J.; Hogan, A.B.; Winskill, P.; Ghani, A.C. Global impact of the first year of COVID-19 vaccination: A mathematical modelling study. Lancet Infect. Dis. 2022, 22, 1293–1302. [Google Scholar] [CrossRef] [PubMed]
- Dan-Nwafor, C.; Ochu, C.L.; Elimian, K.; Oladejo, J.; Ilori, E.; Umeokonkwo, C.; Steinhardt, L.; Igumbor, E.; Wagai, J.; Okwor, T.; et al. Nigeria’s public health response to the COVID-19 pandemic: January to May 2020. J. Glob. Health 2020, 10, 020399. [Google Scholar] [CrossRef] [PubMed]
- Owhonda, G.; Onyekwere, N.; Kanee, R.B.; Maduka, O.; Nwadiuto, I.; Okafor, C.; Chibianotu, O.; Aigbogun, E.O. Community awareness, perceptions, enablers and potential barriers to non-pharmaceutical interventions (npis) in the COVID-19 pandemic in Rivers State, Nigeria. Biomed. J. Sci. Tech. Res. 2021, 36, 28984–28995. [Google Scholar] [CrossRef]
- Abubakar, I.; Dalglish, S.L.; Angell, B.; Sanuade, O.; Abimbola, S.; Adamu, A.L.; Adetifa, I.M.O.; Colbourn, T.; Ogunlesi, A.O.; Onwujekwe, O.; et al. The Lancet Nigeria Commission: Investing in health and the future of the nation. Lancet 2022, 399, 1155–1200. [Google Scholar] [CrossRef]
- Mbaeyi, C.; Kamawal, N.S.; Porter, K.A.; Azizi, A.K.; Sadaat, I.; Hadler, S.; Ehrhardt, D. Routine Immunization Service Delivery Through the Basic Package of Health Services Program in Afghanistan: Gaps, Challenges, and Opportunities. J. Infect. Dis. 2017, 216, S273–S279. [Google Scholar] [CrossRef]
- Oku, A.; Oyo-Ita, A.; Glenton, C.; Fretheim, A.; Eteng, G.; Ames, H.; Muloliwa, A.; Kaufman, J.; Hill, S.; Cliff, J.; et al. Factors affecting the implementation of childhood vaccination communication strategies in Nigeria: A qualitative study. BMC Public Health 2017, 17, 200. [Google Scholar] [CrossRef]
- OECD. The Territorial Impact of COVID-19: Managing The Crisis Across Levels of Government. Organ. fo Econ. Coop. Dev. 2020, 2–44. Available online: https://www.oecd.org/coronavirus/policy-responses/the-territorial-impact-of-covid-19-managing-the-crisis-across-levels-of-government-d3e314e1/ (accessed on 19 October 2022).
- Bello, I.M.; Lebo, E.; Shibeshi, M.E.; Akpan, G.U.; Chakauya, J.; Masresha, B.G.; Daniel, F. Implementation of integrated supportive supervision in the context of coronavirus 19 pandemic: Its effects on routine immunization and vaccine preventable surveillance diseases indicators in the East and Southern African countries. Pan Afr. Med. J. 2021, 38, 164. [Google Scholar] [CrossRef] [PubMed]
- Faiva, E.; Hashim, H.T.; Ramadhan, M.A.; Musa, S.K.; Bchara, J.; Tuama, Y.D.; Adebisi, Y.A.; Kadhim, M.H.; Essar, M.Y.; Ahmad, S.; et al. Drug supply shortage in Nigeria during COVID-19: Efforts and challenges. J. Pharm. Policy Pr. 2021, 14, 17. [Google Scholar] [CrossRef] [PubMed]
- Olutuase, V.O.; Iwu-Jaja, C.J.; Akuoko, C.P.; Adewuyi, E.O.; Khanal, V. Medicines and vaccines supply chains challenges in Nigeria: A scoping review. BMC Public Health 2022, 22, 11. [Google Scholar] [CrossRef] [PubMed]
- WHO and UNICEF. Maintaining Routine Immunization Services Vital during the COVID-19 Pandemic. 2020. Available online: https://www.unicef.org/tajikistan/press-releases/maintaining-routine-immunization-services-vital-during-covid-19-pandemic-who-and (accessed on 19 October 2022).
- The Impact of COVID-19 on Digital Financial Inclusion. Available online: https://www.gpfi.org/sites/gpfi/files/sites/default/files/5_WB%20Report_The%20impact%20of%20COVID-19%20on%20digital%20financial%20inclusion.pdf (accessed on 25 April 2022).
- Uba, B.V.; Waziri, N.E.; Akerele, A.; Biya, O.; Adegoke, O.J.; Gidado, S.; Ugbenyo, G.; Simple, E.; Usifoh, N.; Sule, A.; et al. Strengthening facility-based immunization service delivery in local government areas at high risk for polio in Northern Nigeria, 2014–2015. Pan. Afr. Med. J. 2021, 40 (Suppl. 1), 6. [Google Scholar] [PubMed]
- Shet, A.; Carr, K.; Danovaro-Holliday, M.C.; Sodha, S.V.; Prosperi, C.; Wunderlich, J.; Wonodi, C.; Reynolds, H.W.; Mirza, I.; Gacic-Dobo, M.; et al. Impact of the SARS-CoV-2 pandemic on routine immunisation services: Evidence of disruption and recovery from 170 countries and territories. Lancet Glob. Health 2022, 10, e186–e194. [Google Scholar] [CrossRef]
- Causey, K.; Fullman, N.; Sorensen, R.J.D.; Galles, N.C.; Zheng, P.; Aravkin, A.; Danovaro-Holliday, M.C.; Martinez-Piedra, R.; Sodha, S.V.; Velandia-González, M.P.; et al. Estimating global and regional disruptions to routine childhood vaccine coverage during the COVID-19 pandemic in 2020: A modelling study. Lancet 2021, 398, 522–534. [Google Scholar] [CrossRef]
- Hirabayashi, K. The Impact of COVID-19 on Routine Vaccinations|UNICEF East Asia and Pacific. Unicef. 2020. Available online: https://www.unicef.org/eap/stories/impact-covid-19-routine-vaccinations (accessed on 18 October 2022).
- World Health Organization. COVID-19 Pandemic Fuels Largest Continued Backslide in Vaccinations in Three Decades, pp. 1–5. 2022. Available online: https://www.who.int/news/item/15-07-2022-covid-19-pandemic-fuels-largest-continued-backslide-in-vaccinations-in-three-decades (accessed on 18 October 2022).
- GAVI. At least 80 Million Children at Risk of Disease as COVID-19 Disrupts Vaccination Efforts, Warn Gavi, WHO and UNICEF. Gavi, the Vaccine Alliance. 2020. Available online: https://www.gavi.org/news/media-room/least-80-million-children-risk-disease-covid-19-disrupts-vaccination-efforts (accessed on 18 October 2022).
- SeyedAlinaghi, S.; Karimi, A.; Mojdeganlou, H.; Alilou, S.; Mirghaderi, S.P.; Noori, T.; Shamsabadi, A.; Dadras, O.; Vahedi, F.; Mohammadi, P.; et al. Impact of COVID-19 pandemic on routine vaccination coverage of children and adolescents: A systematic review. Health Sci. Rep. 2022, 5, e00516. [Google Scholar] [CrossRef]
- Sharma, L.; Sharma, M.; Singh, S.; Dwiwedi, M.; Agarwal, D.; Gupta, G.; Dhiman, R. Magnitude and causes of routine immunization disruptions during COVID-19 pandemic in developing countries. J. Fam. Med. Prim. Care 2021, 10, 3991–3997. [Google Scholar] [CrossRef]
- Bosch-Capblanch, X.; Liaqat, S.; Garner, P. Managerial supervision to improve primary health care in low- and middle-income countries. Cochrane Database Syst. Rev. 2011, 2011, CD006413. [Google Scholar] [CrossRef]
- Bradley, S.; Kamwendo, F.; Masanja, H.; de Pinho, H.; Waxman, R.; Boostrom, C.; McAuliffe, E. An in-depth exploration of health worker supervision in Malawi and Tanzania. Hum. Resour. Heal. 2013, 11, 43. [Google Scholar] [CrossRef]
- Madede, T.; Sidat, M.; McAuliffe, E.; Patricio, S.R.; Uduma, O.; Galligan, M.; Bradley, S.; Cambe, I. The impact of a supportive supervision intervention on health workers in Niassa, Mozambique: A cluster-controlled trial. Hum. Resour. Health 2017, 15, 58. [Google Scholar] [CrossRef] [PubMed]
- Onyango, R.O. Designing an M&E System during a Pandemic: Successes and Failures at a Project’S Inception Phase. Indep. Dev. Eval. (IDEV)—Afr. Dev. Bank. 2021. Available online: http://idev.afdb.org/en/content/designing-me-system-during-pandemic-successes-and-failures-projects-inception-phase (accessed on 19 October 2022).
- UNICEF. The Critical Role of UNICEF in Accelerating COVID-19 Vaccine Rollout through National Logistics Work. Supply Div. 2021. Available online: https://www.unicef.org/supply/stories/critical-role-unicef-accelerating-covid-19-vaccine-rollout-through-national-logistics-work (accessed on 8 January 2023).
- Essoh, T.-A.; Adeyanju, G.C.; Adamu, A.A.; Ahawo, A.K.; Aka, D.; Tall, H.; Aplogan, A.; Wiysonge, C.S. Early Impact of SARS-CoV-2 Pandemic on Immunization Services in Nigeria. Vaccines 2022, 10, 1107. [Google Scholar] [CrossRef] [PubMed]
- GAVI. Routine Vaccinations during a Pandemic—Benefit or Risk? 2020. Available online: https://www.gavi.org/vaccineswork/routine-vaccinations-during-pandemic-benefit-or-risk?gclid=Cj0KCQiAzeSdBhC4ARIsACj36uGt_uOFfiMwXitGM_dO30qknvxXbswogi3cOo7YW1X0hO9Ay--0Bu0aAmaIEALw_wcB (accessed on 8 January 2023).
- World Health Organisation. Guiding Principles for Immunization Activities during the COVID-19 Pandemic. WHO/2019-nCoV/immunization_services/2020.1, no. March, pp. 17–20. 2020. Available online: https://apps.who.int/iris/bitstream/handle/10665/331590/WHO-2019-nCoV-immunization_services-2020.1-eng.pdf (accessed on 15 August 2022).
- World Health Organization. COVID-19 Global Risk Communication and Community Engagement Strategy—Interim Guidance. 2020, 20–21. Available online: https://www.who.int/publications/i/item/covid-19-global-risk-communication-and-community-engagement-strategy (accessed on 15 August 2022).
- Musa, E. The Impact of the COVID-19 Pandemic on Immunization Programs in Kaduna State Nigeria. Sabin Vaccine Inst. 2020. Available online: https://www.sabin.org/resources/the-impact-of-the-covid-19-pandemic-on-immunization-programs-in-kaduna-state-nigeria/ (accessed on 19 October 2022).
- G20 Italian Presidency. The Impact of COVID-19 on Digital Financial Inclusion. In Glob. Partnersh. Financ. Incl. By World Bank; 2021; pp. 1–29. Available online: https://www.mef.gov.it/inevidenza/2021/article_00064/Annex-II-Reports-and-Documents-Received-Fourth-G20-FMCBGs-13-Octob....pdf (accessed on 19 October 2022).
- Alagboso, C. Overcoming the Challenges of Financing Routine Immunisation Beyond COVID-19. Nigeria Health Watch 2022. Available online: https://nigeriahealthwatch.com/overcoming-the-challenges-of-financing-routine-immunisation-beyond-covid-19/ (accessed on 19 October 2022).
- Aregbeshola, B.S.; Folayan, M.O. Nigeria’s financing of health care during the COVID-19 pandemic: Challenges and recommendations. World Med. Health Policy 2022, 14, 195–204. [Google Scholar] [CrossRef] [PubMed]
- Abbas, K.; Procter, S.R.; van Zandvoort, K.; Clark, A.; Funk, S.; Mengistu, T.; Hogan, D.; Dansereau, E.; Jit, M.; Flasche, S.; et al. Routine childhood immunisation during the COVID-19 pandemic in Africa: A benefit–risk analysis of health benefits versus excess risk of SARS-CoV-2 infection. Lancet Glob. Health 2020, 8, e1264–e1272. [Google Scholar] [CrossRef]
- Ranganathan, R.; Khan, A.M. Routine immunization services during the coronavirus (COVID-19) pandemic. Indian J. Community Health 2020, 32, 236–239. [Google Scholar] [CrossRef]
- USAID. The Power of Partnerships for Improved Routine Immunization in Nigeria. 2019. Available online: https://mcsprogram.org/the-power-of-partnerships-for-improved-routine-immunization-in-nigeria/ (accessed on 26 September 2022).
- Sharma, S.; Mudgal, S.; Thakur, K.; Gaur, R. How to calculate sample size for observational and experiential nursing research studies? Natl. J. Physiol. Pharm. Pharmacol. 2020, 10, 1. [Google Scholar] [CrossRef]
- Fox, N.; Hunn, A.; Mathers, N. Sampling and Sample Size Calculation. NIHR RDS East Midl. 2022, 1, 1–4. Available online: https://www.bdct.nhs.uk/wp-content/uploads/2019/04/Sampling-and-Sample-Size-Calculation.pdf (accessed on 14 May 2022).
- Lakens, D. Sample size justification. Collabra Psychol. 2022, 8, 33267. [Google Scholar] [CrossRef]
- Aliyu, A.; Amadu, L. Urbanization, cities and health: The challenges to Nigeria—A review. Ann. Afr. Med. 2017, 16, 149–158 . [Google Scholar] [CrossRef] [PubMed]
- Farrell, K. An Inquiry into the Nature and Causes of Nigeria’s Rapid Urban Transition. Urban Forum 2018, 29, 277–298. [Google Scholar] [CrossRef]
- IA2030. Monitoring and Monitoring & Evaluation (M&E) Framework. Immun. Agenda 2020, 2030, 1–34. [Google Scholar]
- Khatiwada, A.P.; Maskey, S.; Shrestha, N.; Shrestha, S.; Khanal, S.; Kc, B.; Paudyal, V. Impact of the first phase of COVID-19 pandemic on childhood routine immunisation services in Nepal: A qualitative study on the perspectives of service providers and users. J. Pharm. Policy Pract. 2021, 14, 79. [Google Scholar] [CrossRef]
- Turner, A.G.; Angels, G.; Tsui, A.O.; Wilkinson, M.; Magnani, R. Sampling Manual For Facility Surveys, 3rd ed.; MEASURE Evaluation Manual Series; 2001; Available online: https://www.measureevaluation.org/resources/publications/ms-01-03/at_download/document (accessed on 14 April 2022).
- Green, S.B.; Yan, Y. Evaluation of Dimensionality in the Assessment of Internal Consistency Reliability: Coefficient Alpha and Omega Coefficients. Educ. Meas. Issues Pract. 2015, 34, 14–20. [Google Scholar] [CrossRef]
- Davenport, E.C.; Davison, M.L.; Liou, P.Y.; Love, Q.U. Reliability, Dimensionality, and Internal Consistency as Defined by Cronbach: Distinct Albeit Related Concepts. Educ. Meas. Issues Pract. 2015, 34, 4–9. [Google Scholar] [CrossRef]
- Collins, L.M. Research Design and Methods. Encycl. Gerontol. 2007, 433–442. [Google Scholar] [CrossRef]
- Yu, C.H. Test-Retest Reliability. Encycl. Soc. Meas. 2005, 777–784. [Google Scholar] [CrossRef]
- Wood, P. Confirmatory Factor Analysis for Applied Research. Am. Stat. 2008, 62, 91–92. [Google Scholar] [CrossRef]
- Pavlov, G.; Maydeu-Olivares, A.; Shi, D. Using the Standardized Root Mean Squared Residual (SRMR) to Assess Exact Fit in Structural Equation Models. Educ. Psychol. Meas. 2020, 81, 110–130. [Google Scholar] [CrossRef] [PubMed]
- Bentler, P.M. Comparative fit indexes in structural models. Psychol. Bull. 1990, 107, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Kumar, K. A Beginner’s Guide to Structural Equation Modeling, 3rd ed.; Psychology Press: London, UK, 2012; pp. 828–829. [Google Scholar] [CrossRef]
- Parry, S. Fit Indices commonly reported for CFA and SEM. Cornell Univ. Cornell Stat. Consult. Unit. 2020, 1, 2021. [Google Scholar]
- Tanaka, J.S.; Huba, G.J. A fit index for covariance structure models under arbitrary GLS estimation. Br. J. Math. Stat. Psychol. 1985, 38, 197–201. [Google Scholar] [CrossRef]
- Stone, B.M. The Ethical Use of Fit Indices in Structural Equation Modeling: Recommendations for Psychologists. Front. Psychol. 2021, 12, 5221. [Google Scholar] [CrossRef] [PubMed]
- Creswell, J.W. Qualitative Inquiry & Research Design: Choosing among Five Approaches, vol. 2. 2007. Available online: https://www.scirp.org/(S(351jmbntvnsjt1aadkposzje))/reference/ReferencesPapers.aspx?ReferenceID=1807302 (accessed on 16 September 2022).
- Khan, S.N. Qualitative Research Method: Grounded Theory. Int. J. Bus. Manag. 2014, 9, p224. [Google Scholar] [CrossRef]
- Cohen, L.; Manion, L.; Morrison, K. Research Methods in Education; Routledge: London, UK, 2007. [Google Scholar] [CrossRef]
- World Health Organization. COVID-19 Pandemic Leads to Major Backsliding on Childhood Vaccinations, New WHO, UNICEF Data Shows. News Release 2021. Available online: https://www.unicef.org/press-releases/covid-19-pandemic-leads-major-backsliding-childhood-vaccinations-new-who-unicef-data (accessed on 8 January 2023).
- Save the Children. SCALING UP ROUTINE IMMUNISATION COVERAGE IN NIGERIA. 2022. Available online: https://www.savethechildren.org.uk/blogs/2022/scaling-up-routine-immunisation-coverage-in-nigeria (accessed on 8 January 2023).
- NPHCDA. Community Engagement Strategy for Strengthening Routine immunization in northern nigeria. pp. 1–20. 2022. Available online: https://publications.jsi.com/JSIInternet/Inc/Common/_download_pub.cfm?id=22337&lid=3 (accessed on 22 June 2022).
- Oyo-Ita, A.; Bosch-Capblanch, X.; Ross, A.; Oku, A.; Esu, E.; Ameh, S.; Oduwole, O.; Arikpo, D.; Meremikwu, M. Effects of engaging communities in decision-making and action through traditional and religious leaders on vaccination coverage in Cross River State, Nigeria: A cluster-randomised control trial. PLoS ONE 2021, 16, e0248236. [Google Scholar] [CrossRef] [PubMed]
- Gooding, E.; Spiliotopoulou, E.; Yadav, P. Impact of vaccine stockouts on immunization coverage in Nigeria. Vaccine 2019, 37, 5104–5110. [Google Scholar] [CrossRef]
- Molemodile, S.; Wotogbe, M.; Abimbola, S. Evaluation of a pilot intervention to redesign the decentralised vaccine supply chain system in Nigeria. Glob. Public Health 2017, 12, 601–616. [Google Scholar] [CrossRef] [PubMed]
- UNICEF. Lessons Learned and Good Practices: Country-Specific Case Studies on Immunization Activities during the COVID-19 Pandemic. 2021. Available online: https://www.unicef.org/media/115221/file/Lessons-Learned-and-Good-Practices-Immunization-Activities-During-the-COVID-19-Pandemic-2021.pdf (accessed on 19 October 2022).
- Aina, M.; Igbokwe, U.; Jegede, L.; Fagge, R.; Thompson, A.; Mahmoud, N. Preliminary results from direct-to-facility vaccine deliveries in Kano, Nigeria. Vaccine 2017, 35, 2175–2182. [Google Scholar] [CrossRef] [PubMed]
- Uchenna, A.A.; Saleh, J.-E.; Saddiq; Eze, O.L.; Ogbonna, P.E.; Calista, U.N.; Abonyi, I.; Isaac, E.; Obianuju, I.C.; Ugochukwu, E.N.; et al. Intensified Routine Immunization (RI) Activities as A Strategy for Improving Routine Immunization and Acute Flaccid Paralysis (AFP) Surveillance outcomes; Lessons from Intensified Activities Conducted in 2 LGAs in Abia State Nigeria. J. Community Med. Public Health 2018, 2, 100032. [Google Scholar] [CrossRef][Green Version]
- allAfrica.com. Nigeria: Rising Cost of Healthcare in Nigeria Amid COVID-19. 2020. Available online: https://allafrica.com/stories/202103070279.html (accessed on 8 January 2023).









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Theme | Variables | Year | Bauchi (n = 12) | Borno (n = 12) | Kaduna (n = 12) | Kano (n = 12) | Sokoto (n = 12) | Yobe (n = 12) |
|---|---|---|---|---|---|---|---|---|
| Leadership and governance | WG meeting conducted | 2019 | 0.87 ± 0.09 ** | 0.85 ± 0.09 | 0.85 ± 0.08 | 0.72 ± 0.21 | 0.88 ± 0.10 ** | 0.80 ± 0.26 * |
| 2020 | 0.58 ± 0.27 | 0.74 ± 0.29 | 0.76 ± 0.24 | 0.66 ± 0.28 | 0.63 ± 0.24 | 0.54 ± 0.30 | ||
| Action-point completion rate | 2019 | 0.76 ± 0.05 | 0.78 ± 0.09 | 0.85 ± 0.05 | 0.63 ± 0.23 | 0.79 ± 0.05 ** | 0.71 ± 0.24 * | |
| 2020 | 0.66 ± 0.22 | 0.66 ± 0.32 | 0.66 ± 0.32 | 0.45 ± 0.45 | 0.41 ± 0.36 | 0.43 ± 0.38 | ||
| Service delivery | Planned fixed sessions conducted | 2019 | 1.00 ± 0.33 * | 0.91 ± 0.21 | 0.98 ± 0.33 | 1.00 ± 0.01 * | 0.99 ± 0.02 * | 1.02 ± 0.06 * |
| 2020 | 0.75 ± 0.36 | 0.74 ± 0.29 | 0.79 ± 0.37 | 0.88 ± 0.19 | 0.94 ± 0.07 | 0.86 ± 0.23 | ||
| Planned outreach sessions conducted | 2019 | 0.97 ± 0.02 * | 0.98 ± 0.03 ** | 0.99 ± 0.02 | 1.00 ± 0.02 ** | 0.98 ± 0.01 * | 1.00 ± 0.16 * | |
| 2020 | 0.70 ± 0.34 | 0.66 ± 0.32 | 0.78 ± 0.37 | 0.85 ± 0.16 | 0.92 ± 0.09 | 0.83 ± 0.20 | ||
| Monitoring and evaluation/ supportive supervision | Planned RISS visits conducted (LGA to HF) | 2019 | 0.83 ± 0.90 | 0.61 ± 0.17 | 0.75 ± 0.24 | 0.32 ± 0.47 | 0.72 ± 0.15 | 0.84 ± 0.10 |
| 2020 | 0.90 ± 0.03 ** | 0.64 ± 0.07 | 0.77 ± 0.11 | 0.90 ± 0.28 ** | 0.61 ± 0.19 | 0.92 ± 0.07 * | ||
| Vaccine supply chain and logistics | Apex facilities that received vaccines on time | 2019 | 0.95 ± 0.03 | 0.82 ± 0.10 | 0.89 ± 0.06 | 0.94 ± 0.04 | 0.92 ± 0.04 | 0.98 ± 0.02 |
| 2020 | 0.98 ± 0.02 ** | 1.00 ± 0.00 ** | 1.00 ± 0.00 ** | 1.00 ± 0.00 ** | 1.00 ± 0.00 ** | 1.00 ± 0.00 ** | ||
| Vaccine stockout | 2019 | 0.05 ± 0.02 | 0.13 ± 0.06 ** | 0.15 ± 0.05 | 0.06 ± 0.02 | 0.06 ± 0.02 ** | 0.17 ± 0.04 ** | |
| 2020 | 0.07 ± 0.04 | 0.12 ± 0.01 | 0.12 ± 0.03 | 0.06 ± 0.02 | 0.01 ± 0.05 | 0.06 ± 0.08 |
| Demographic Factors | Bauchi (n = 37) | Borno (n = 23) | Kaduna (n = 54) | Kano (n = 50) | Sokoto (n = 47) | Yobe (n = 56) | Mean ± S.D | Total (n = 267) |
|---|---|---|---|---|---|---|---|---|
| Highest Education Qualification | ||||||||
| Primary (%) | 2 (5.4) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | N/A | 2 (0.7) |
| Secondary (%) | 0 (0) | 0 (0) | 2 (3.7%) | 0 (0) | 0 (0) | 7 (12.5) | 9 (3.4) | |
| Tertiary (%) | 35 (94.6) | 23 (100) | 52 (96.3) | 50 (100) | 47 (100) | 49 (87.5) | 256 (95.9) | |
| Years of Practice | ||||||||
| 0–5 years (%) | 2 (5.4) | 0 (0) | 4 (7.4) | 5 (10.5) | 3 (6.4) | 6 (10.7) | 17.34 ± 8.32 | 20 (7.5) |
| 6–15 years (%) | 4 (10.8) | 4 (17.4) | 8 (14.8) | 6 (12.0) | 24 (51.1) | 10 (17.9) | 56 (21.0) | |
| ≥16 years (%) | 31 (83.8) | 19 (82.6) | 42 (77.8) | 39 (78.0) | 20 (42.6) | 40 (71.4) | 191 (71.5) | |
| Years in Present Job | ||||||||
| 0–5 years (%) | 23 (62.3) | 10 (43.5) | 29 (53.7) | 29 (58.0) | 25 (53.2) | 23 (41.1) | 7.67 ± 6.61 | 139 (52.1) |
| 6–10 years (%) | 11 (29.7) | 4 (17.4) | 13 (26.0) | 13 (27.7) | 13 (28.6) | 16 (28.6) | 70 (26.2) | |
| ≥11 years (%) | 3 (8.1) | 9 (39.1) | 12 (22.2) | 8 (16.0) | 9 (19.1) | 17 (30.4) | 58 (21.7) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aigbogun, E.O., Jr.; Ibrahim, R.; Yusufari, Y.; Igbokwe, U.; Okongwu, C.; Abdulkarim, A.; Tijanni, H.; Modu, M.; Fagge, R.M.; Aina, M. Impact of the COVID-19 Pandemic on Routine Immunization Programs in Northern Nigeria. Sustainability 2023, 15, 12966. https://doi.org/10.3390/su151712966
Aigbogun EO Jr., Ibrahim R, Yusufari Y, Igbokwe U, Okongwu C, Abdulkarim A, Tijanni H, Modu M, Fagge RM, Aina M. Impact of the COVID-19 Pandemic on Routine Immunization Programs in Northern Nigeria. Sustainability. 2023; 15(17):12966. https://doi.org/10.3390/su151712966
Chicago/Turabian StyleAigbogun, Eric Osamudiamwen, Jr., Raihanah Ibrahim, Yusuf Yusufari, Uchenna Igbokwe, Chimelu Okongwu, Amina Abdulkarim, Hussaini Tijanni, Maina Modu, Rabiu Muhammad Fagge, and Muyi Aina. 2023. "Impact of the COVID-19 Pandemic on Routine Immunization Programs in Northern Nigeria" Sustainability 15, no. 17: 12966. https://doi.org/10.3390/su151712966
APA StyleAigbogun, E. O., Jr., Ibrahim, R., Yusufari, Y., Igbokwe, U., Okongwu, C., Abdulkarim, A., Tijanni, H., Modu, M., Fagge, R. M., & Aina, M. (2023). Impact of the COVID-19 Pandemic on Routine Immunization Programs in Northern Nigeria. Sustainability, 15(17), 12966. https://doi.org/10.3390/su151712966