1. Introduction
The burden of disease linked with exposure to poor AQ is significant and rising, and this is especially the case in middle and low-income countries [
1]. The World Health Organization (WHO) has reported that ambient poor AQ is responsible for about 4.2 million global deaths annually, with 99% of the global population breathing air that exceeds the organisation’s guideline limits [
2]. Poor AQ also has several important adverse impacts on climate change and may directly affect natural ecosystems and biodiversity [
3]. Nitrogen oxides (NO
X), nitrogen monoxide (NO), and ammonia (NH
3) emissions alter terrestrial and aquatic ecosystems and Tropospheric Ozone (O
3), while black carbon and Particulate Matter (PM) are short-lived climate forcers that lead directly to global warming. Poor AQ also damages materials, buildings and artwork through corrosion, biodegradation, and weathering and fading of colours. A report by [
3] also stated that the market costs of Poor AQ include reduction in productivity of labour, extra health expenses, and loss in yield of crops and forests. Indeed, despite urbanisation being one of the fundamental features of economic development, concerns about AQ have led to a wide-ranging discussion about the meaning of urban sustainability [
4]. An important consideration here is the need to define what is meant by AQ. A common approach taken by agencies charged with monitoring and managing AQ is to define it in terms of concentrations of pollutants, be they gasses or particles in the air (please see for example [
5]).
Appropriate means of assessing pollutant levels are needed as the basis for AQ management [
6], and many instruments such as passive air pollutant samplers, air quality sensors, reference instruments [
7], and Earth Observation (EO) satellites have been employed, with data from such instruments often used as the basis for predictive models [
8,
9,
10]. According to [
11], nearly all urban areas in Europe and North America have networks of AQ monitoring instruments at a density of about 1 per 100,000 to 600,000 residents, while in developing regions, such as Africa, it is estimated to be around 1 per 4,200,000 residents. Although there has been some improvement in recent years, there are still huge challenges in monitoring AQ, especially in urban areas of developing countries [
12]. For instance, ref. [
11] reported that in the United States of America (USA), federal, state, and tribal agencies constructed the existing AQ monitoring systems over five decades at a cost of millions of dollars for the hardware, human resources, and institutional frameworks to install and maintain monitoring stations and process, analyse, and report the information. Additionally, in developed countries such as the USA, there is a steady electricity supply system, telecommunications, and other structures to ensure uninterrupted collection/processing of data as well as maintenance of hardware.
Conversely, many cities in developing countries have an unstable electricity supply, inadequate or no laboratories or air quality monitoring stations, little or no financial and human resources, and weak telecommunications systems, resulting in a dearth of reliable and timely information on AQ [
13,
14]. Finding and using the best monitoring equipment may be unique to each context and may also depend on levels of precision required, standards and regulatory framework. For example, ref. [
7,
15] note that a sensor’s ability to measure accurately can be compromised by chemical and physical interference, and improvements designed to tackle the abnormalities need to be validated against reference measurements. Low-cost alternative sensors have been developed, but the measurements can fluctuate depending upon factors such as temperature, humidity, pressure, and signal instability [
15].
A different approach to assessing and managing AQ is to seek the views and perceptions of those people directly experiencing it. For example, an investigation by [
16] found that people perceived AQ to be very poor and the major environmental problem in Ljubljana, Slovenia, while [
17] found that urban residents, especially those suffering from asthma, are more concerned about and tend to check the AQ in their vicinity. In their study at Richards Bay and its surroundings in uMhlathuze Municipality, KwaZulu, South Africa, ref. [
18] found that residents were concerned about AQ, and most perceive it to be fair or poor, with industrial emissions regarded by them as the major cause of poor AQ. According to [
19], residents in Accra, Ghana, were aware that their AQ is poor and does influence their health, although they also found that some demographic groups, such as the less educated and the elderly, were less aware of poor AQ in the city. Similar work was conducted in Nigeria among people living near a cement manufacturing area of Ewokoro and Reno-North Local Government Areas of Ogun State by [
20] and noted that people are aware of poor AQ and its adverse health effects. Recently, ref. [
21] using an online survey of residents’ perception of AQ in Abuja and Enugu cities, Nigeria, stated that a variety of ‘perceptual’ indicators of poor AQ were employed, and these varied in terms of their relative importance (
Table 1). Respondents were aware of their exposure to poor AQ, and they used smoke, dust, and odour as the main perceptual indicators of poor AQ. However, while the use of perceptual indicators of poor AQ has value, according to [
16], the use of such tools should be seen as providing a “supplementary” approach alongside data from monitoring instruments.
One of the issues with using perceptual indicators is that much is likely to depend on the biological ability of humans to detect pollutants. For the particulate matter (PM)-based indicators, such as smoke and dust, the detection may be relatively straightforward as people can see smoke as well as dirt on skin, clothes and surfaces, and indeed this may well explain their relatively high ranking in
Table 1. Gaseous pollutants such as SO
2 and NO
2 are typically detected by people through odour and taste. The colourless gas SO
2 can be detected by taste at concentrations of 0.35 to 1.05 ppm and has an irritating odour with a threshold in the range of 0.67–4.75 ppm, depending upon the individual [
22]. An odour threshold range of 0.1 to 0.4 ppm for NO
2 is cited by [
23]. On the other hand, CO is both a colourless and odourless gas that humans cannot so readily detect. Hence, while odour and even taste are important perceptual indicators, as noted in
Table 1, some pollutants may not be detectable if concentrations are below a threshold, while others may not be detectable unless levels are so high that they cause effects such as difficulty in breathing. It is also conceivable that the ability to detect pollutants may vary depending on factors such as age, health and education, and there is also the possibility that experience of exposure to poor AQ could be important. Finally, it is also likely that people’s perceptions of poor AQ may be framed by assumptions based on the prevalence of causes such as traffic or indeed influenced by the views of others. Therefore, while public perceptions of AQ have been explored by researchers, albeit to a much lesser extent in urban areas of the developing than the developed world, there are important questions to ask about how well such perceptions match results obtained using instruments.
Some studies have suggested that perceived AQ can match well with instrument-measured and model-based results, although many of these have been conducted in urban contexts in the developed world [
24]. A study by [
25] noted that smells reported by individuals were significantly associated with modelled NO
2 and SO
2 concentrations, and in their study of public perceptions of AQ in Chinese cities, ref. [
26] noted that perceptions can match results based on reference equipment. However, others have noted that perceptual indicators of poor AQ may not necessarily tally with instrument-based measurements [
27,
28,
29]. For example, ref. [
30] found an insignificant relationship between perceived and measured AQ in Seoul, South Korea, and in their work in the USA [
31] found perceived AQ to be getting worse while instrumentally obtained information showed there had been an improvement. In Texas, United States of America, ref. [
32] found only a weak relationship between perceived AQ made by locals and that measured via instruments.
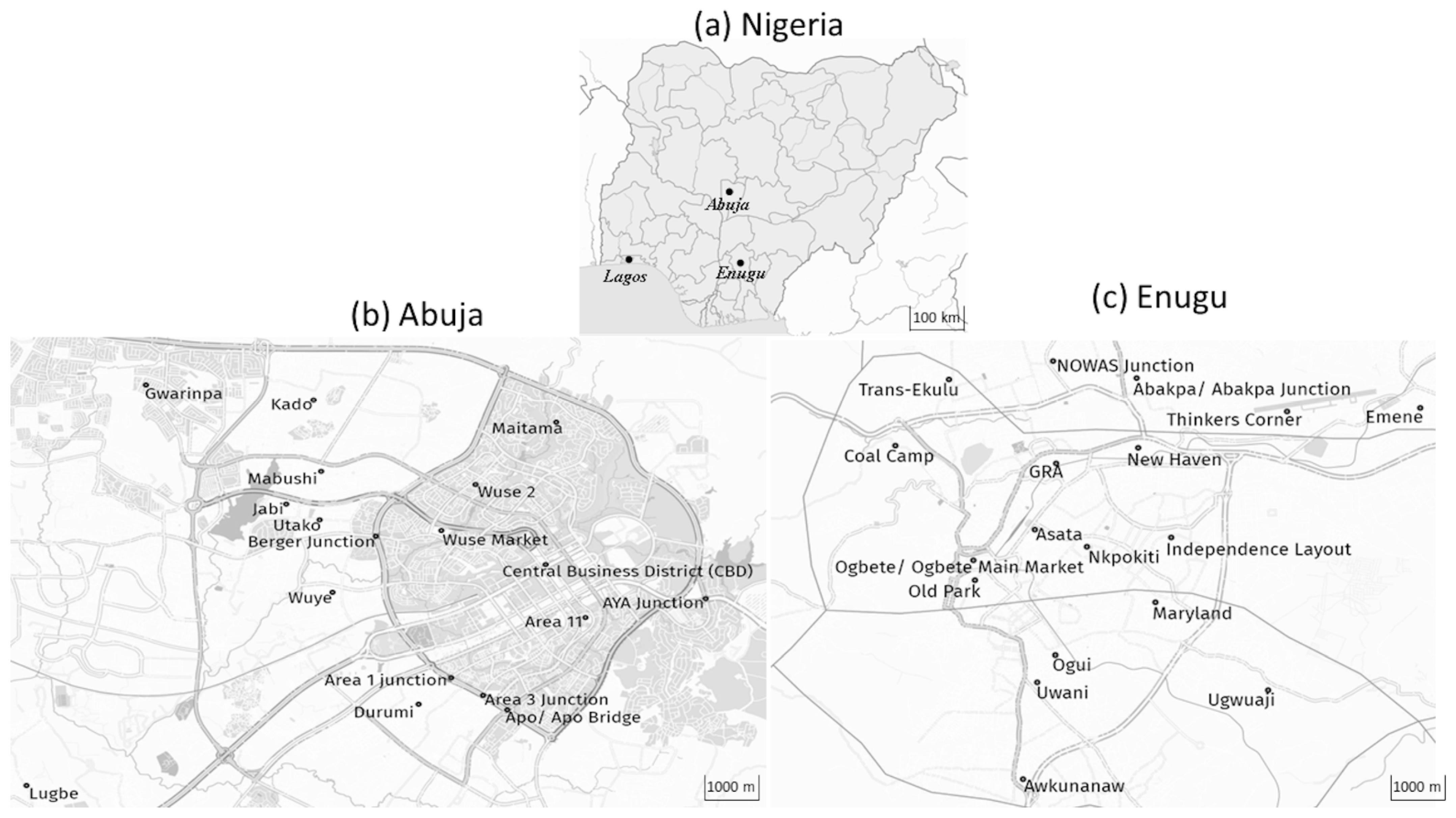
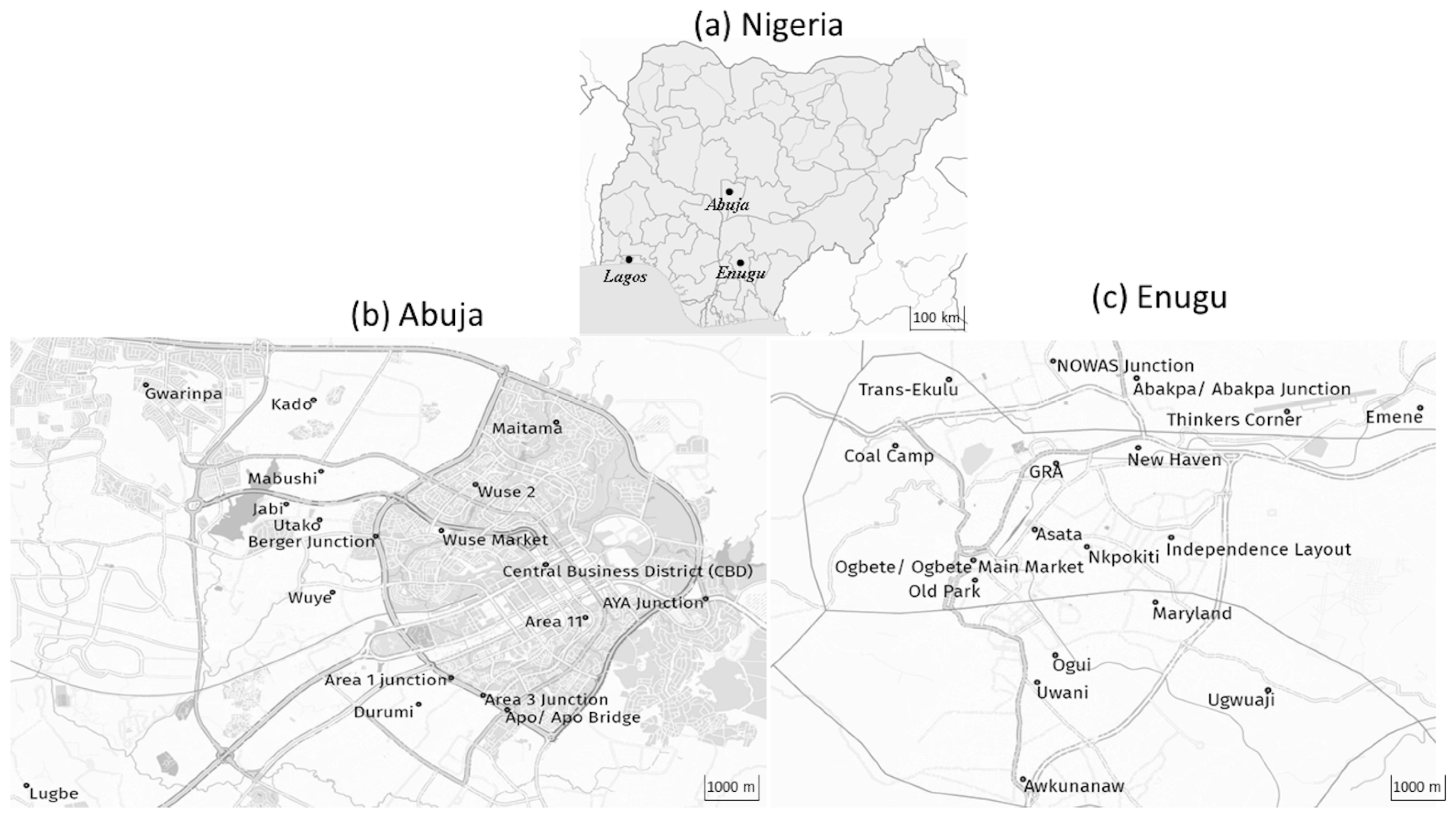
However, there remains a dearth of such comparative studies from urban areas of the developing world. Hence, the aim of the research set out in this paper was to explore the link between perceptual indicators of AQ and measurements from instruments in various locations within two cities in Nigeria (Abuja and Enugu) along with whether various demographic factors influenced perceptions of AQ in those locations. The two cities were chosen for their contrasting geographical and socio-economic situations (summarised below), although the intention was not to compare the two cities per se. Instead, the choice of such contrasting urban contexts was intended to provide the basis for a robust comparison between perceptual and instrument-based analysis of AQ.
4. Discussion
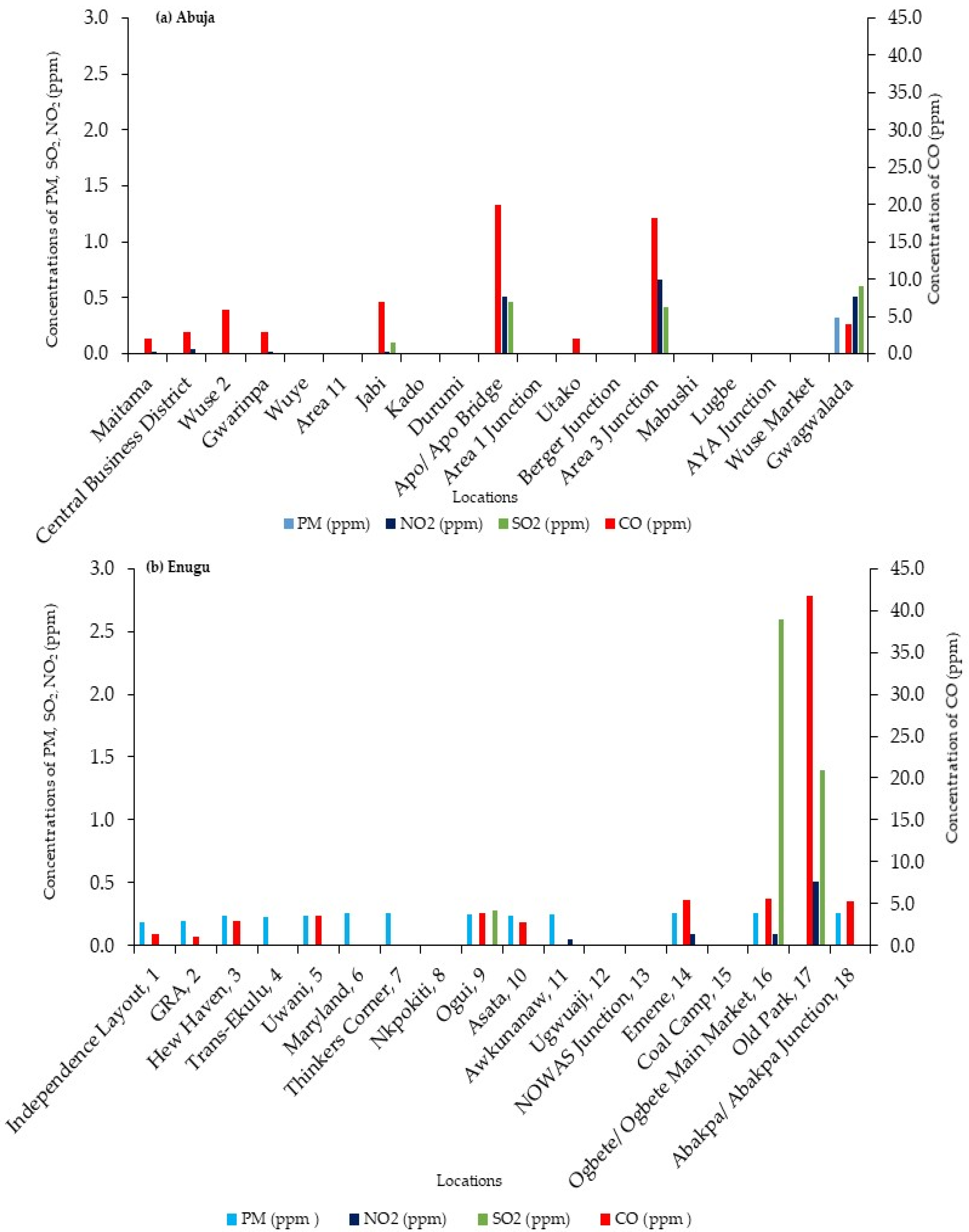
The research described in this paper was designed to explore whether the perceptions of AQ align with those provided by instruments. Based on published results in the literature, it does indeed appear to be the case that the locations in both cities vary significantly in terms of the concentration of some pollutants in the air. However, it does need to be noted that comparisons between the two cities are challenging, as much depends on the choice of location within them as well as differences in methods adopted by the researchers to measure pollutant concentrations. Nonetheless, the findings suggest that perceptions of AQ do appear to be associated with instrument-based measurements as those locations in Abuja and Enugu that people perceive to have the worst AQ are those that instrument-based studies have shown to have the highest concentrations of pollutants such as PM, SO2, NO2, and CO. This intriguing and important finding, however, does have some important caveats.
Firstly, there were significant differences between demographic groups in how they perceived AQ. Gender was not important in either city, but there were differences in terms of the income-education demographics in Abuja (but not Enugu) and age in Enugu (but not Abuja). In both cases, the differences between demographic groups were most marked for locations that had poorer AQ (i.e., locations in the lower parts of
Table 5 and
Table 6). Why should this be so? The differences between age groups in Enugu were noted in previous research [
21], where the younger demographic (18–34 years old) was more positive about measures to control AQ and the need for action by agencies such as state and local government. This may be associated with youth identity and activism in the Igbo (the dominant ethnic group in Enugu) compared with the much more multi-ethnic and multi-cultural nature of the Abuja respondents from Tiv, Yoruba, Igbo, Hausa, Fulani, Edo, Idoma, Igala, Efik, Ibibio, Gbagyi, Ijaw, Eggon, and Berom [
21]. However, the importance of the income-education demographics in Abuja (but not Enugu) is intriguing. One possibility may be linked to the greater wealth and income levels of respondents in the Abuja sample; 58% of Abuja respondents had annual incomes of about 51,000 compared with 46% for Enugu. Differences in income levels can generate segregation between rich and poor neighbourhoods, as seen, in the most extreme cases, with “gated” communities that have been on the rise throughout Sub-Saharan Africa and which are known to generate spatial fragmentation and urban segregation [
59]. Their popularity is partly driven by a desire for better security, and they exist in Abuja and Enugu. Segregation between richer and poorer neighbourhoods, with the former tending to be more distant from causes of pollution [
60], may engender a more polarised view of AQ. A further factor is that people living in low-income neighbourhoods tend to have more negative views of their environment than do those from wealthier neighbourhoods [
61].
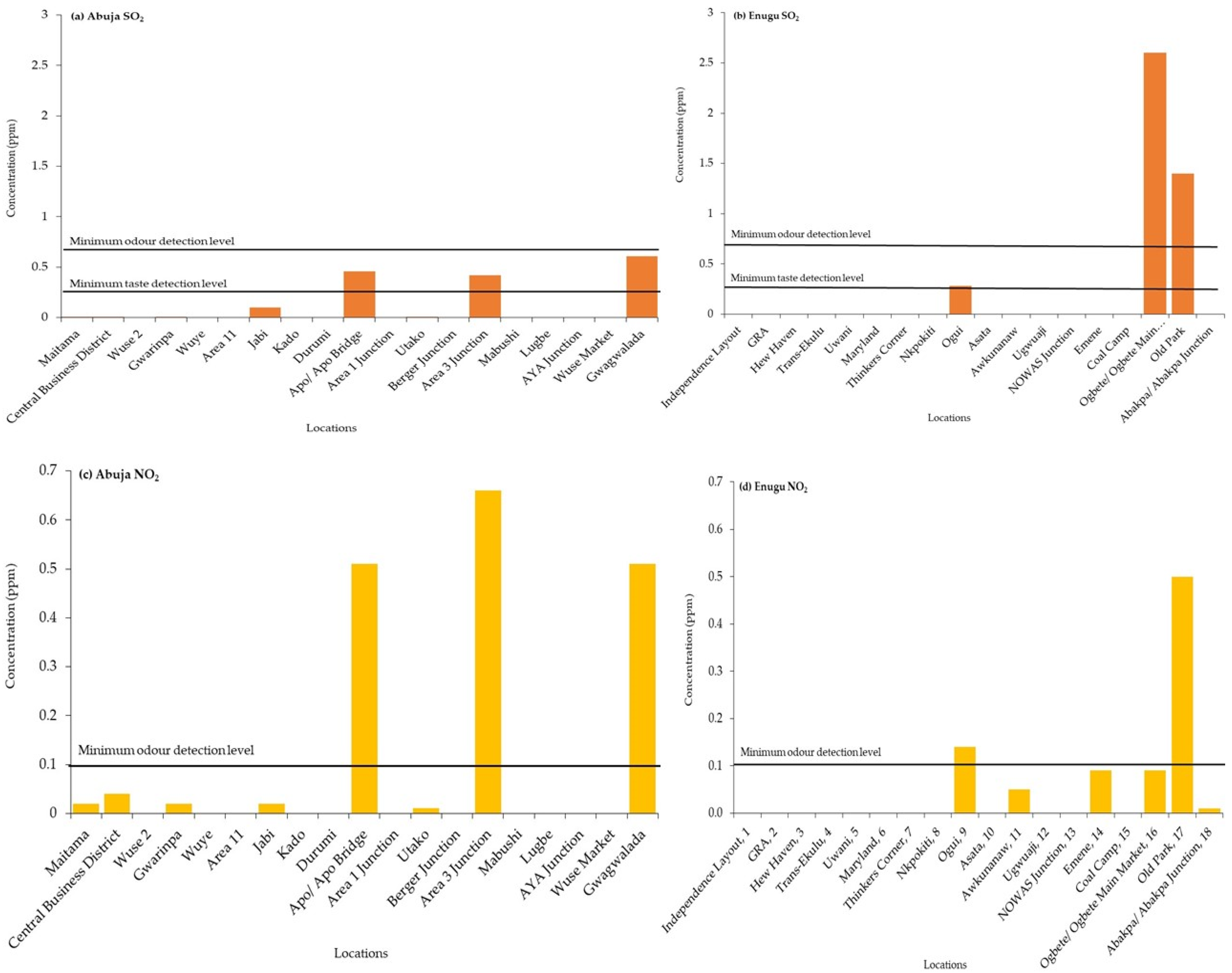
Secondly, while there is an apparent link between perceptions of AQ and measurements of pollutant concentrations in both cities, this may not necessarily mean that people can detect the pollutants directly. For SO
2 in Abuja and NO
2 in Enugu, the concentrations were indeed higher in locations perceived to have the worst AQ, but these concentrations were below the thresholds at which the pollutants could be detected via the senses of smell and taste. It would appear more likely that respondents were basing their views of AQ on the presence of more visible “clues”, such as smoke and dust, and while the odour is an important indicator (
Table 1), it may be that it reflects a “cocktail” of pollutants in the air including hydrocarbons. These clues may well be positively correlated with concentrations of SO
2 and NO
2. In addition, respondents may also have framed their scoring of locations, at least in part, on the presence of causes of poor AQ. This possibility resonates with the work of [
62], who analysed data from the Third European Quality of Life Survey undertaken between 2011 and 2012. They concluded that perceived exposure to air pollution is formed based on sensory awareness as well as what they refer to as a “cognitive component”, which is framed using knowledge of exposure to sources of air pollution (e.g., presence of traffic), perceived ability to cope with that exposure, and the perception of health risks. Moreover, an earlier study by [
63] shows that odour annoyance is more perceived to exist in locations that have higher levels of traffic. This study and the study of [
64] illustrated that the detection of air quality by people could be because of the extent or duration of the situation which causes poor air quality. The work of [
64] also found that people perceive traffic as one of the main sources of poor AQ. Social discourse such as views from people via online social sites can also influence perceptions of environmental issues including AQ [
65].
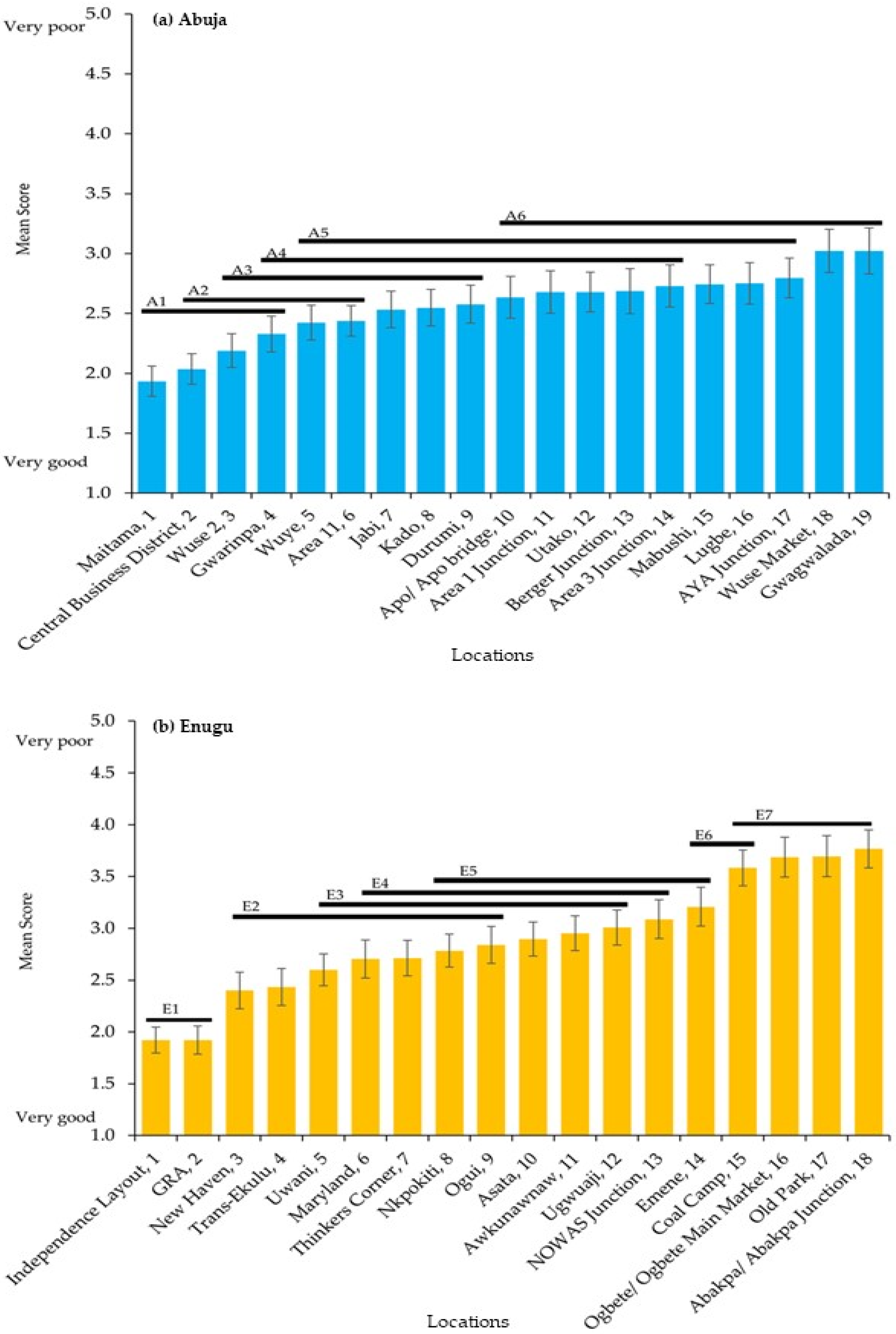
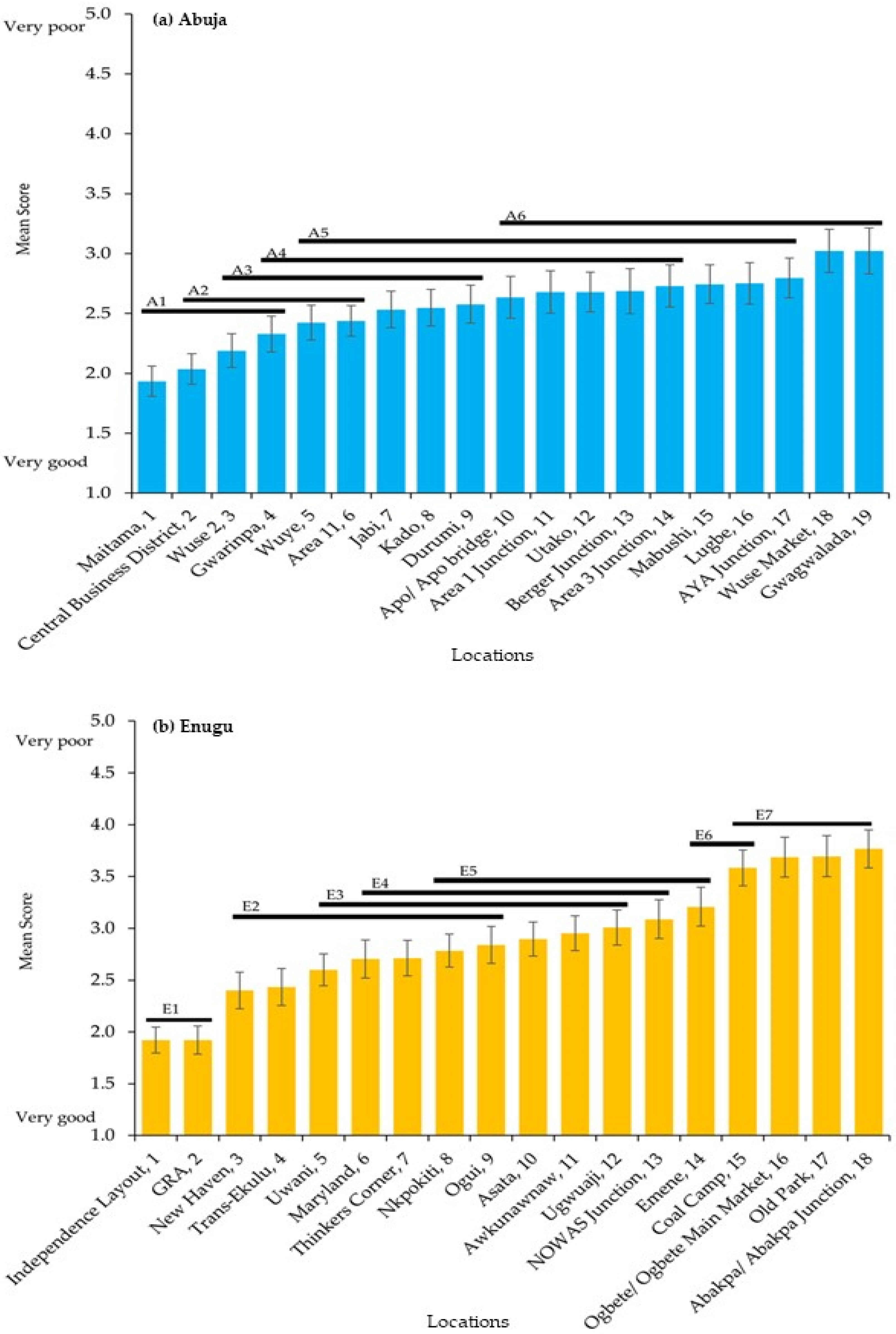
The results, both perceptions and measurements, do indeed point to differences between the AQ of locations in the two cities. The locations for comparison in the survey were selected using the advice provided by key informants, and some locations were known to have issues with AQ. In general, the AQ in government reserved areas (GRA or areas resided by higher-income earners) and administrative locations were better than market locations, busy junctions, and lower-income earners’ residential locations, which are mainly mixed with other functions such as manufacturing and retailing with a high density of inhabitants (
Table 4). In Abuja, Maitama is perceived to be the cleanest among the selected locations, and this location is mainly inhabited by prominent people and political office holders, while the AQ at Wuse Market and Gwagwalada is scored more poorly. This result is similar to the work of [
54], where they found that locations with major vehicular traffic junctions, such as AYA Junction, Area 1 Junction, Area 3 Junction, Gwagwalada, Wuse Market, and Mabushi Roundabout, have poorer AQ compared with locations with lower vehicular traffic. For Enugu, the results show that Independence Layout and GRA (mainly higher-income earners residential areas) are jointly ranked as those having the best AQ, while seven locations (Ugwuaji, NOWAS Junction, Emene, Coal Camp, Ogbete/Ogbete Main Market, Old Park, and Abakpa/Abakpa Junction) (mixed-use, commercial and transportation locations) that are rated above neutral are the locations with the worst AQ.
The assessment of AQ, especially within the developing world, has, to date, mainly been achieved using monitoring equipment and models, but issues including inadequate funds and technical know-how have been limiting their use. These limitations could be alleviated by using a participatory approach, such as the one used in the present research to draw upon people’s perceptions of AQ. While perceptions of AQ are framed by perceptual indicators, such as odour and dust, there may well be other factors at play such as the “cognitive component” identified by [
62] and framing via social discourse [
65]. Hence, while the research reported here has shown a link between the perceived AQ of locations in Abuja and Enugu and the measured levels of pollutants, it is perhaps understandable that this may not always be the case as reflected in the spectrum of published evidence that falls in both camps [
25,
26,
30,
31,
32]. More research is certainly needed in this important field, especially for urban centres in the developing world. Nonetheless, we suggest that the use of perception in monitoring AQ should be globally accepted as a complementary approach to the use of instruments. Perceptual-based approaches cannot substitute for instrument-based approaches, but the authors are very much in agreement with [
16] that perceptual-based approaches can be a useful supplement. Perceptual indicators and monitoring not only serve as a form of assessment but also as a form of awareness-raising of AQ and related environmental phenomena.






{kind=link}
{kind=link}
{kind=link}
{kind=link}