

Satisfactions on Self-Perceived Health of Urban Residents in Chengdu, China: Gender, Age and the Built Environment

 ,
, 
Abstract
1. Introduction
2. Literature Review
2.1. Social Demography, Lifestyle and Health Awareness, and Indoor Environment Factors
2.2. Neighborhood Characteristics and Sub-Group Analysis
2.3. Determinants of Resident’s Health Perception in the Chinese Context
2.4. Research Gap
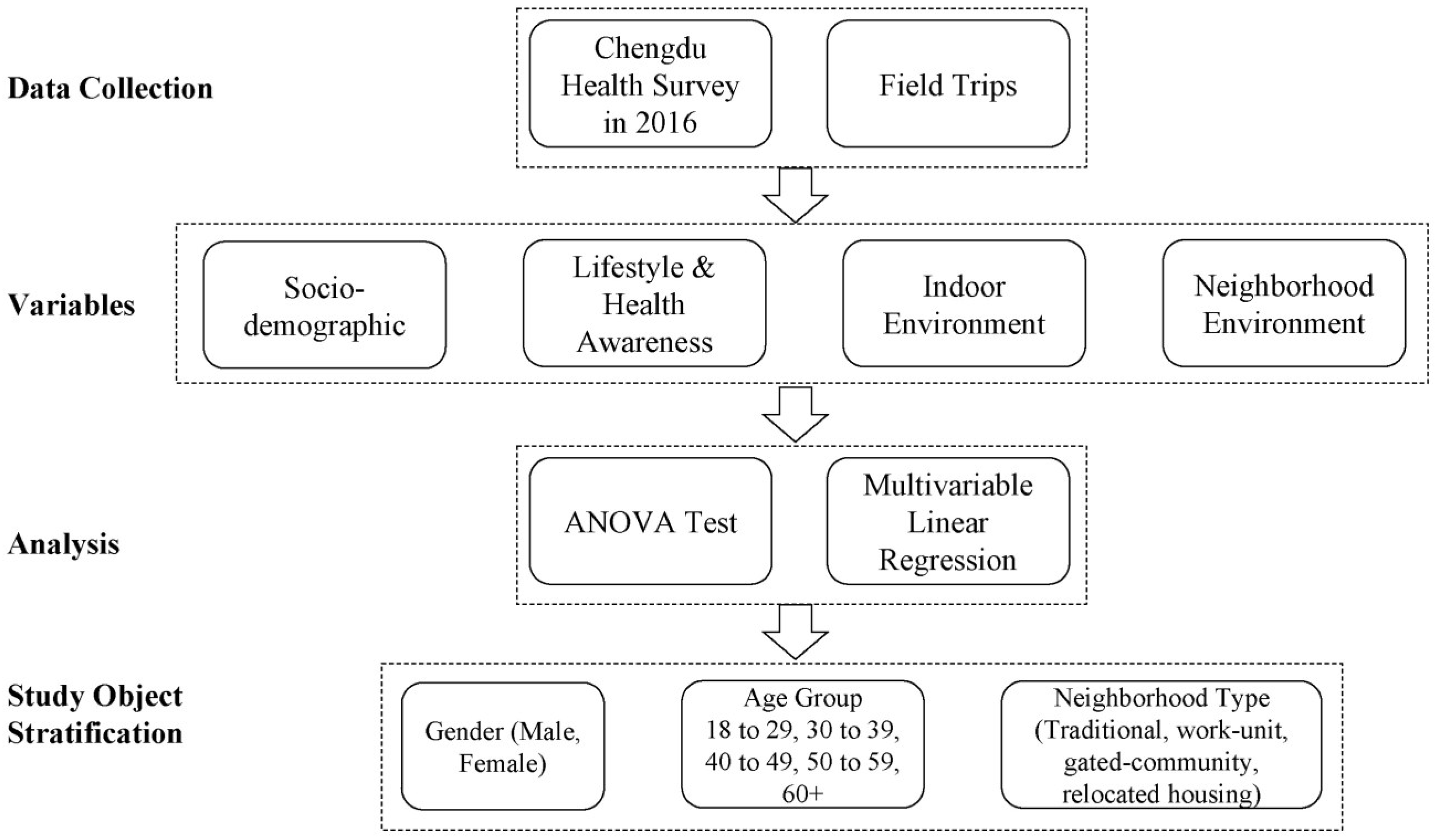
3. Methodology
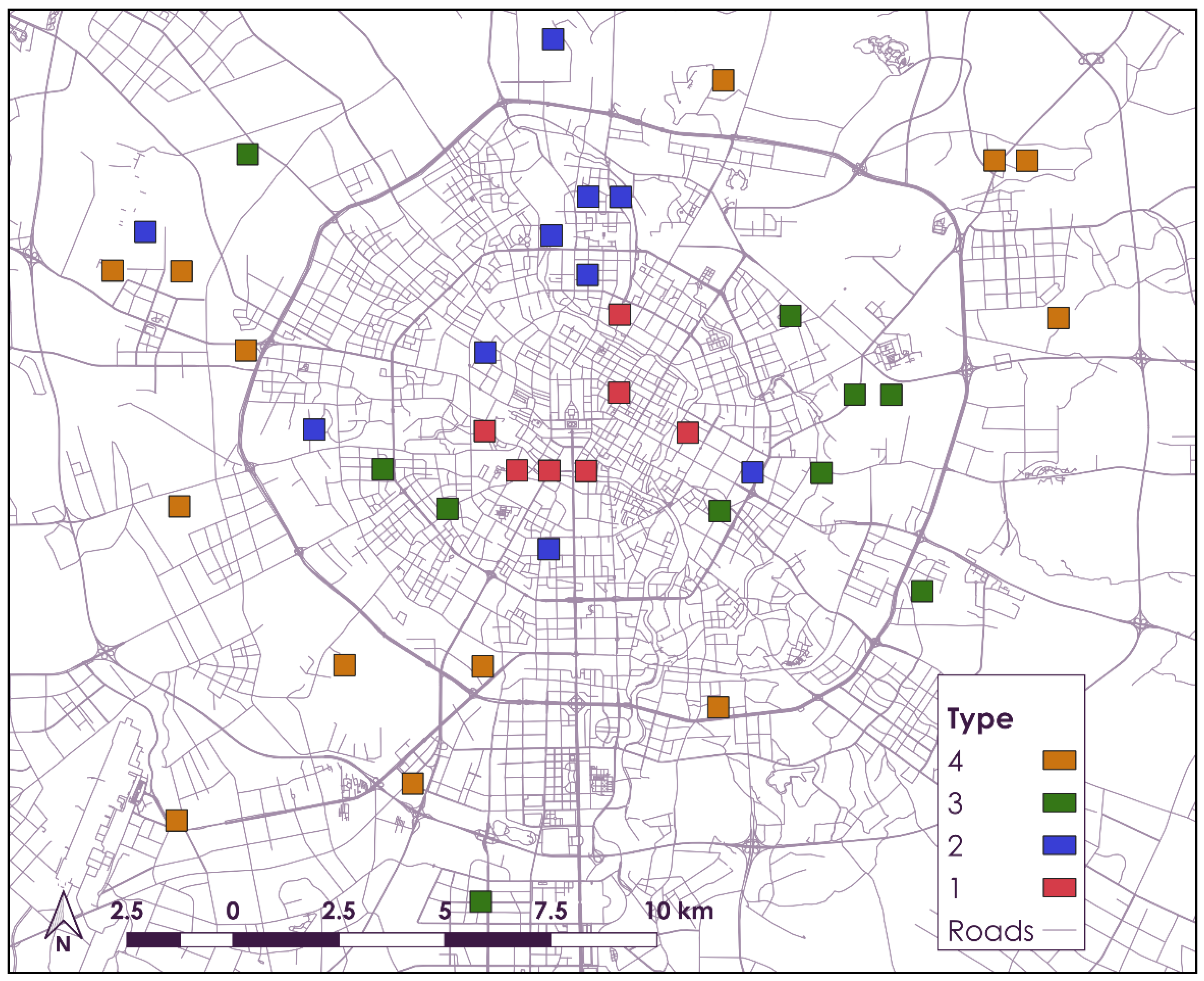
3.1. Study Area and Data Collection
3.2. Statistical Analysis
4. Results
4.1. Statistical Summary of Variables
4.2. Self-Perceived Health Conditions by Gender and Age
4.3. Self Perceived Health Conditions by Neighborhood Type
5. Discussion
5.1. Health Perception and Gender
5.2. Health Perception and Age
5.3. Health Perception and Neighborhood Type
6. Limitations and Future Study
7. Contribution and Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Dipeolu, A.; Ibem, E.; Fadamiro, J.; Omoniyi, S.; Aluko, R. Influence of green infrastructure on residents' self-perceived health benefits in Lagos metropolis, Nigeria. Cities 2021, 118, 103378. [Google Scholar] [CrossRef]
- Su, Y.; D’Arcy, C.; Li, M.; Meng, X. Determinants of Life Satisfaction and Self-Perceived Health in Nationally Representative Population-Based Samples, Canada, 2009 to 2018. Appl. Res. Qual. Life. 2022, 21, 1–26. [Google Scholar] [CrossRef]
- Benyamini, Y.; Leventhal, E.A.; Leventhal, H. Gender Differences in Processing Information for Making Self-assessments of Health. Psychosom. Med. 2000, 62, 354–364. [Google Scholar] [CrossRef] [PubMed]
- Boerstra, A.; Beuker, T.; Loomans, M.; Hensen, J. Impact of Available and Perceived Control on Comfort and Health in European Offices. Archit. Sci. Rev. 2013, 56, 30–41. [Google Scholar] [CrossRef]
- Jarvis, I.; Koehoorn, M.; Gergel, S.; Bosch, M. Different types of urban natural environments influence various dimensions of self-reported health. Environ. Res. 2020, 186, 109614. [Google Scholar] [CrossRef] [PubMed]
- Mousavinia, S.; Pourdeihimi, S.; Madani, R. Housing layout, perceived density and social interactions in gated communities: Mediational role of territoriality. Sustain. Cities Soc. 2009, 51, 101699. [Google Scholar] [CrossRef]
- Pasanen, T.P.; Tyrväinen, L.; Korpela, K.M. The Relationship between Perceived Health and Physical Activity Indoors, Outdoors in Built Environments, and Outdoors in Nature. Appl. Psychol. Health Well-Being 2014, 6, 324–346. [Google Scholar] [CrossRef]
- Guan, C.; Srinivasan, S.; Zhang, B.; Da, L.; Liu, J.; Nielsen, C. The Influence of Neighborhood Types on Active Transport in China’s Growing Cities. Transp. Res. Part D Transp. Environ. 2020, 80, 102273. [Google Scholar] [CrossRef]
- Wu, J.; Xu, Z.; Jin, Y.; Chai, Y.; Newell, J.; Ta, N. Gender disparities in exposure to green space: An empirical study of suburban Beijing. Landsc. Urban Plan. 2022, 222, 104381. [Google Scholar] [CrossRef]
- Ho, H.; Wong, P.; Guo, C. Impacts of social and environmental perceptions on preparedness and knowledge of air pollution risk: A study of adolescent males in an urbanized, high-density city. Sustain. Cities Soc. 2021, 66, 102678. [Google Scholar] [CrossRef]
- Srinivasan, S.; Guan, C.; Nielsen, C. Built environment, income and travel behavior: Change in the city of Chengdu, China 2005–2016. Int. J. Sustain. Transp. 2020, 14, 749–760. [Google Scholar] [CrossRef]
- Shields, M.; Shooshtari, S. Determinants of Self-perceived Health. Health Rep. 2001, 13, 35–52. [Google Scholar] [PubMed]
- Wang, J.; Rao, C.; Goh, M.; Xiao, X. Risk assessment of coronary heart disease based on cloud-random forest. Artif. Intell. Rev. 2022, 1–26. [Google Scholar] [CrossRef]
- Berglund, E.; Westerling, R.; Lytsy, P. Housing Type and Neighbourhood Safety Behaviour Predicts Self-rated Health, Psychological Well-being and Frequency of recent Unhealthy Days: A Comparative Cross-sectional Study of the General Population in Sweden. Plan. Pract. Res. 2013, 32, 444–465. [Google Scholar] [CrossRef]
- Nummela, O.P.; Sulander, T.T.; Heinonen, H.S.; Uutela, A.K. Self-rated Health and Indicators of SES among the Ageing in three Types of Communities. Scand. J. Public Health 2007, 35, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Dong, R.; Wang, X. Plants with health risks undermine residents’ perceived health status, evaluations and expectations of residential greenery. Landsc. Urban Plan. 2021, 216, 104236. [Google Scholar] [CrossRef]
- Wong, M.; Yu, R.; Woo, J. Effects of Perceived Neighbourhood Environments on Self-rated Health among Community-dwelling Older Chinese. Int. J. Environ. Res. Public Health 2017, 14, 614. [Google Scholar] [CrossRef] [PubMed]
- Cai, J.; Coyte, P.C.; Zhao, H. Determinants of and Socio-Economic Disparities in Self-rated Health in China. Int. J. Equity Health 2017, 16, 7. [Google Scholar] [CrossRef] [PubMed]
- Xie, Z.; Poon, A.N.; Wu, Z.; Jian, W.; Chan, K.Y. Is Occupation a Good Predictor of Self-rated Health in China? PLoS ONE 2015, 10, e0125274. [Google Scholar] [CrossRef]
- Gómez-Costilla, P.; García-Prieto, C.; Somarriba-Arechavala, N. Aging and Gender Health Gap: A Multilevel Analysis for 17 European Countries. Soc. Indic. Res. 2022, 160, 1051–1069. [Google Scholar] [CrossRef]
- Liu, Q.; Luo, S.; Shen, Y.; Zhu, Z.; Yao, X.; Li, Q.; Tarin, M.W.K.; Zheng, J.; Zhuo, Z. Relationships between students’ demographic characteristics, perceived naturalness and patterns of use associated with campus green space, and self-rated restoration and health. Urban For. Urban Green. 2022, 68, 127474. [Google Scholar] [CrossRef]
- Fan, Y.; He, D. Self-rated health, socioeconomic status and all-cause mortality in Chinese middle-aged and elderly adults. Sci. Rep. 2021, 12, 9309. [Google Scholar] [CrossRef] [PubMed]
- Qi, Y.; Niu, J. Health Selection Effects in China’s Internal Migration. Asian Popul. Stud. 2013, 9, 142–155. [Google Scholar] [CrossRef]
- Ou, H.T.; Su, C.T.; Luh, W.M.; Lin, C.Y. Knowing is Half the Battle: The Association between Leisure-time Physical Activity and Quality of Life among Four Groups with Different Self-perceived Health Status in Taiwan. Appl. Res. Qual. Life 2017, 12, 799–812. [Google Scholar] [CrossRef]
- Dhingra, S.S.; Zack, M.M.; Strine, T.W.; Druss, B.G.; Simoes, E. Change in Health Insurance Coverage in Massachusetts and Other New England States by Perceived Health Status: Potential Impact of Health Reform. Am. J. Public Health 2013, 103, 107–144. [Google Scholar] [CrossRef]
- Lu, C.; Deng, Q.; Li, Y.; Sundell, J.; Norbäck, D. Outdoor Air Pollution, Meteorological Conditions and Indoor Factors in Dwellings in Relation to Sick Building Syndrome (SBS) among Adults in China. Sci. Total Environ. 2016, 560, 186–196. [Google Scholar] [CrossRef]
- Wen, M.; Hawkley, L.C.; Cacioppo, J.T. Objective and Perceived Neighborhood Environment, Individual SES and Psychosocial Factors, and Self-rated Health: An Analysis of Older Adults in Cook County, Illinois. Soc. Sci. Med. 2006, 63, 2575–2590. [Google Scholar] [CrossRef]
- Lawder, R.; Walsh, D.; Kearns, A.; Livingston, M. Healthy Mixing? Investigating the Associations between Neighbourhood Housing Tenure Mix and Health Outcomes for Urban Residents. Urban Stud. 2014, 51, 264–283. [Google Scholar] [CrossRef]
- Ichida, Y.; Kondo, K.; Hirai, H.; Hanibuchi, T.; Yoshikawa, G.; Murata, C. Social Capital, Income Inequality and Self-rated Health in Chita Peninsula, Japan: A Multilevel Analysis of Older People in 25 Communities. Soc. Sci. Med. 2009, 69, 489–499. [Google Scholar] [CrossRef]
- Hamplova, D.; Klusacek, J.; Mracek, T. Assessment of self-rated health: The relative importance of physiological, mental, and socioeconomic factors. PLoS ONE 2022, 17, e0267115. [Google Scholar] [CrossRef]
- Awang, M.; Alfitri, A.; Ahmad, A.; Careemdeen, J.; Ahmad, J. Socio-Ecological Support and Physical Facilities Satisfaction: How They Link to Social Participation and Well-Being among Urban Residents in Malaysia. Sustainability 2022, 14, 1184. [Google Scholar] [CrossRef]
- Woo, J.; Ho, S.C.; Yu, A.L.M. Lifestyle Factors and Health Outcomes in Elderly Hong Kong Chinese aged 70 years and over. Gerontology 2022, 48, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Luo, Y.; Haller, W.; Vander Mey, B.; Granberg, E. Neighborhood Environments and Self-rated Health in Mainland China, Japan and South Korea. PLoS ONE 2018, 13, 0204910. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y. Negotiating Authenticity in China’s Urban Historic Preservations–the Case of the Kuan and Zhai Alleys in Chengdu. Herit. Soc. 2018, 11, 79–104. [Google Scholar] [CrossRef]
- Rowe, P.G.; Forsyth, A.; Kan, H.Y. China’s Urban Communities: Concepts, Contexts, and Well-being; Birkhäuser: Basel, Switzerland, 2016. [Google Scholar]
- Kan, H.Y.; Forsyth, A.; Rowe, P. Redesigning China’s Superblock Neighbourhoods: Policies, Opportunities and Challenges. J. Urban Des. 2017, 22, 757–777. [Google Scholar] [CrossRef]
- Li, X.; Kleinhans, R.; van Ham, M. Ambivalence in Place Attachment: The Lived Experiences of Residents in Danwei Communities Facing Demolition in Shenyang, China. Hous. Stud. 2019, 34, 997–1020. [Google Scholar] [CrossRef]
- Yang, Q.; Ley, D. Residential Relocation and the Remaking of Socialist Workers through State-facilitated Urban Redevelopment in Chengdu, China. Urban Stud. 2019, 56, 2480–2498. [Google Scholar] [CrossRef]
- Breitung, W. Enclave Urbanism in China: Attitudes towards Gated Communities in Guangzhou. Urban Geogr. 2012, 33, 278–294. [Google Scholar] [CrossRef]
- Yip, N.M. Walled without gates: Gated communities in Shanghai. Urban Geogr. 2012, 33, 221–236. [Google Scholar] [CrossRef]
- Shih, M. The Evolving Law of Disputed Relocation: Constructing Inner-city Renewal Practices in Shanghai, 1990–2005. Int. J. Urban Reg. Res. 2010, 34, 350–364. [Google Scholar] [CrossRef]
- Guan, C.; Forsyth, A. The influence of urban form and socio-demographics on active transport: A 40-neighborhoods study in Chengdu, China. J. Transp. Land Use 2020, 13, 367–388. [Google Scholar] [CrossRef]
- Qin, B.; Yang, J. Access of Low-income Residents to Urban Services for Inclusive Development: The Case of Chengdu, China. In Governance for Urban Services; Springer: Singapore, 2020; pp. 209–236. [Google Scholar]
- Zhang, S.; Song, X.; Wei, Y.; Deng, W. Spatial Equity of Multilevel Healthcare in the Metropolis of Chengdu, China: A new Assessment Approach. Int. J. Environ. Res. Public Health 2019, 16, 493. [Google Scholar] [CrossRef] [PubMed]
- Qiao, X.; Jaffe, D.; Tang, Y.; Bresnahan, M.; Song, J. Evaluation of Air Quality in Chengdu, Sichuan Basin, China: Are China’s Air Quality Standards Sufficient yet? Environ. Monit. Assess. 2015, 187, 250. [Google Scholar] [CrossRef] [PubMed]
- Xiao, K.; Wang, Y.; Wu, G.; Fu, B.; Zhu, Y. Spatiotemporal Characteristics of Air Pollutants (PM10, PM2. 5, SO2, NO2, O3, and CO) in the Inland Basin City of Chengdu, Southwest China. Atmosphere 2018, 9, 74. [Google Scholar] [CrossRef]
- Chengdu Survey. The Research Center for Contemporary China (RCCC) at Peking University in collaboration with Harvard China Project at Harvard University. 2016. Available online: https://chinaproject.harvard.edu/urban%20 (accessed on 1 March 2017).
- Liang, J.; Bennett, J.; Gu, S. Self-reported Physical Health among the Aged in Wuhan, China. J. Cross-Cult. Gerontol. 1993, 8, 225–251. [Google Scholar] [CrossRef]
- Harris, C.R.; Jenkins, M.; Glaser, D. Why do Men Take More Risks than Women? Judgm. Decis. Mak. 2006, 1, 48–63. [Google Scholar]
- Alarcão, V.; Madeira, T.; Peixoto-Plácido, C.; Sousa-Santos, N.; Fernandes, E.; Nicola, P.; Santos, O.; Gorjão-Clara, J. Gender Differences in Psychosocial Determinants of Self-perceived Health among Portuguese Older Adults in Nursing Homes. Aging Ment. Health 2019, 23, 1049–1056. [Google Scholar] [CrossRef]
- Golley, J.; Zhou, Y.; Wang, M. Inequality of Opportunity in China’s Labor Earnings: The Gender Dimension. China World Econ. 2019, 27, 28–50. [Google Scholar] [CrossRef]
- Hu, L.C. Marital Status and Self-Rated Health in China: A Longitudinal Analysis. Popul. Res. Policy Rev. 2021, 40, 499–531. [Google Scholar] [CrossRef]
- He, G.; Wu, X. Marketization, Occupational Segregation, and Gender Earnings Inequality in Urban China. Soc. Sci. Res. 2017, 65, 96–111. [Google Scholar] [CrossRef]
- Deng, W.J.; Hoekstra, J.S.; Elsinga, M.G. Why Women own less Housing Assets in China? The Role of Intergenerational Transfers. J. Hous. Built Environ. 2019, 34, 1–22. [Google Scholar] [CrossRef]
- Institute of Ali Research. Report of Chinese Women’s Asset Management, 2016. Available online: http://www.199it.com/archives/516719.html (accessed on 1 March 2017).
- Hughes, J.; Maurer-Fazio, M. Effects of Marriage, Education and Cccupation on the Female/Male Wage Gap in China. Pac. Econ. Rev. 2002, 7, 137–156. [Google Scholar] [CrossRef]
- Condello, G.; Capranica, L.; Stager, J.; Forte, R.; Falbo, S.; Di Baldassarre, A.; Segura-Garcia, C.; Pesce, C. Physical Activity and Health Perception in Aging: Do Body Mass and Satisfaction Matter? A Three-path Mediated Link. PLoS ONE 2016, 11, e0160805. [Google Scholar] [CrossRef]
- Korpela, K.M.; Ylén, M.; Tyrväinen, L.; Silvennoinen, H. Favorite Green, Waterside and Urban Environments, Restorative Experiences and Perceived Health in Finland. Health Promot. Int. 2010, 25, 200–209. [Google Scholar] [CrossRef] [PubMed]
- Ross, A.; Cloutier, S.; Searle, M. The Association between Leisure-time Physical Activity and Happiness: Testing the Indirect Role of Health Perception. J. Community Psychol. 2019, 47, 1169–1183. [Google Scholar] [CrossRef]
- Chen, J. Perceived Discrimination and Subjective Well-being among Rural-to-Urban Migrants in China. J. Soc. Soc. Welf. 2013, 40, 131. [Google Scholar]
- Lynch, S.M. Explaining Life Course and Cohort Variation in the Relationship between Education and Health: The Role of Income. J. Health Soc. Behav. 2006, 47, 324–338. [Google Scholar] [CrossRef]
- Dai, H.; Jing, S.; Wang, H.; Ma, Y.; Li, L.; Song, W.; Kan, H. VOC Characteristics and Inhalation Health Risks in Newly Renovated Residences in Shanghai, China. Sci. Total Environ. 2017, 577, 73–83. [Google Scholar] [CrossRef] [PubMed]
- He, S.; Webster, C.; Wu, F.; Liu, Y. Profiling Urban Poverty in a Chinese City, the Case of Nanjing. Appl. Spat. Anal. Policy 2008, 1, 193–214. [Google Scholar] [CrossRef]
- Feng, J.; Tang, S.; Chuai, X. The Impact of Neighbourhood Environments on Quality of Life of Elderly People: Evidence from Nanjing, China. Urban Stud. 2018, 55, 2020–2039. [Google Scholar] [CrossRef]
- Day, J.; Cervero, R. Effects of Residential Relocation on Household and Commuting Expenditures in Shanghai, China. Int. J. Urban Reg. Res. 2010, 34, 762–788. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Jv, Y. A smooth difference-in-differences model for assessing gradual policy effects: Revisiting the impact of banking deregulation on income distribution. Financ. Res. Lett. 2022, 50, 103319. [Google Scholar] [CrossRef]
- Gao, M.; Yang, H.; Xiao, Q.; Goh, M. COVID-19 lockdowns and air quality: Evidence from grey spatiotemporal forecasts. Socio-Econ. Plan. Sci. 2022, 83, 101228. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| All | Male | Female | |||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | 2.50% | 97.50% | OR | 2.50% | 97.50% | OR | 2.50% | 97.50% | |
| Demography | |||||||||
| Gender | 1.228 ** | 1.061 | 1.421 | ||||||
| Age | 1.023 *** | 1.015 | 1.032 | 1.022 ** | 1.008 | 1.035 | 1.026 *** | 1.014 | 1.038 |
| Years living in Chengdu | 1.005 * | 1.000 | 1.009 | 1.010 ** | 1.004 | 1.017 | 1.001 | 0.995 | 1.007 |
| Years of education | 0.988 | 0.975 | 1.001 | 0.990 | 0.976 | 1.005 | 0.977 | 0.951 | 1.004 |
| Rural hukou | 1.047 | 0.890 | 1.232 | 1.102 | 0.872 | 1.392 | 0.988 | 0.782 | 1.247 |
| Chengdu hukou | 0.856 | 0.724 | 1.013 | 0.769 * | 0.604 | 0.980 | 0.934 | 0.735 | 1.188 |
| Household income level | 0.927 | 0.823 | 1.044 | 1.050 | 0.894 | 1.234 | 0.796 * | 0.661 | 0.950 |
| Chance of getting injured at work | 1.007 | 0.983 | 1.030 | 0.994 | 0.962 | 1.026 | 1.027 | 0.991 | 1.064 |
| Years of working | 0.999 | 0.991 | 1.008 | 0.998 | 0.985 | 1.012 | 0.995 | 0.985 | 1.006 |
| Martial status | 0.888 | 0.765 | 1.030 | 0.973 | 0.788 | 1.201 | 0.797 * | 0.641 | 0.991 |
| Household size | 1.011 | 0.966 | 1.059 | 0.980 | 0.916 | 1.050 | 1.038 | 0.974 | 1.106 |
| Lifestyle and Health Awareness | |||||||||
| Air quality perception | 1.168 *** | 1.097 | 1.244 | 1.191 *** | 1.091 | 1.301 | 1.149 ** | 1.047 | 1.260 |
| Smoking | 0.921 | 0.769 | 1.105 | 0.880 | 0.643 | 1.204 | 0.913 | 0.639 | 1.306 |
| Hours of weekly exercise | 0.993 | 0.985 | 1.001 | 0.997 | 0.986 | 1.008 | 0.990 | 0.977 | 1.002 |
| Health insurance | 1.181 * | 1.006 | 1.387 | 1.135 | 0.902 | 1.429 | 1.259 | 1.000 | 1.586 |
| Familiarity to asthma | 1.048 | 0.981 | 1.120 | 1.033 | 0.943 | 1.130 | 1.048 | 0.947 | 1.160 |
| Willing to pay for asthma treatment | 1.006 | 0.897 | 1.127 | 0.996 | 0.847 | 1.172 | 1.065 | 0.903 | 1.256 |
| Daily cooking time in family | 0.998 | 0.946 | 1.054 | 0.984 | 0.910 | 1.065 | 0.984 | 0.911 | 1.064 |
| Indoor Environment | |||||||||
| Fuel use—LPG | 0.875 | 0.685 | 1.118 | 1.014 | 0.711 | 1.445 | 0.788 | 0.553 | 1.124 |
| Fuel use—natural gas | 1.117 | 0.906 | 1.376 | 1.323 | 0.986 | 1.776 | 0.984 | 0.716 | 1.353 |
| Fuel use—electricity | 0.939 | 0.825 | 1.068 | 0.923 | 0.767 | 1.112 | 0.938 | 0.780 | 1.128 |
| Fuel use—coal | 1.077 | 0.729 | 1.593 | 0.774 | 0.410 | 1.461 | 1.263 | 0.762 | 2.092 |
| Hours of daily natural ventilation | 1.013 *** | 1.005 | 1.020 | 1.018 ** | 1.007 | 1.029 | 1.008 | 0.998 | 1.019 |
| Air conditioner | 0.844 * | 0.740 | 0.962 | 0.830 | 0.687 | 1.002 | 0.892 | 0.738 | 1.078 |
| Smoking in household | 1.223 * | 1.053 | 1.421 | 1.299 | 0.933 | 1.808 | 1.228 ** | 1.022 | 1.474 |
| Neighborhood Environment | |||||||||
| Sidewalk in front of building | 0.894 | 0.699 | 1.142 | 0.862 | 0.621 | 1.198 | 0.991 | 0.676 | 1.453 |
| Building condition | 0.973 | 0.908 | 1.042 | 0.986 | 0.895 | 1.087 | 0.973 | 0.878 | 1.079 |
| OR | Age 18–29 | Age 30–39 | Age 40–49 | Age 50–59 | Age 60+ |
|---|---|---|---|---|---|
| Demography | |||||
| Gender | 1.351 * | 1.032 | 1.142 | 1.366 | 1.173 |
| Years living in Chengdu | 1.006 | 1.003 | 1.003 | 1.01 | 1.004 |
| Years of education | 1.012 | 1.004 | 0.950 * | 0.96 | 0.973 |
| Rural hukou | 0.945 | 1.11 | 0.722 | 1.467 | 1.137 |
| Chengdu hukou | 0.852 | 0.932 | 0.757 | 1.151 | 0.685 |
| Household income level | 1.101 | 1.076 | 1.017 | 0.706 | 0.928 |
| Chance of getting injured at work | 0.994 | 1.019 | 1.004 | 1.023 | 1.016 |
| Years of working | 1.005 | 1.004 | 0.985 | 0.995 | 1.01 |
| Martial status | 0.992 | 1.162 | 0.6 | 0.75 | 0.86 |
| Household size | 1.015 | 0.941 | 0.965 | 1.09 | 0.989 |
| Lifestyle and Health Awareness | |||||
| Air quality perception | 0.98 | 1.154 | 1.139 | 1.134 | 1.401 *** |
| Smoking | 0.692 * | 0.777 | 0.991 | 1.295 | 1.005 |
| Hours of weekly exercise | 0.991 | 0.984 | 0.99 | 1.017 | 0.977 * |
| Health insurance | 1.268 | 1.099 | 1.136 | 1.206 | 0.965 |
| Familiarity to asthma | 1.111 | 1.004 | 1.074 | 1.035 | 0.95 |
| Willing to pay for asthma treatment | 1.004 | 0.965 | 0.905 | 1.066 | 1.131 |
| Daily cooking time in family | 1.025 | 1.018 | 1.035 | 0.872 * | 1 |
| Indoor environment | |||||
| Fuel use—LPG | 0.661 | 1.251 | 0.68 | 0.849 | 1.085 |
| Fuel use—natural gas | 0.912 | 1.632 | 0.615 | 1.696 | 1.505 |
| Fuel use—electricity | 0.685 *** | 0.905 | 0.908 | 0.995 | 1.470 * |
| Fuel use—coal | 2.582 * | 0.479 | 0.727 | 0.89 | 1.113 |
| Hours of daily natural ventilation | 1.023 *** | 1.013 | 1.009 | 1.031 ** | 0.981 |
| Air conditioner | 0.821 | 0.944 | 1.007 | 0.906 | 0.969 |
| Smoking in household | 1.316 * | 1.404 | 1.086 | 0.876 | 1.449 |
| Neighborhood environment | |||||
| Sidewalk in front of building | 0.691 | 0.500 * | 1.256 | 1.263 | 0.68 |
| Building condition | 1.057 | 0.997 | 0.968 | 0.932 | 1.057 |
| OR | Type 1 (Traditional) | Type 2 (Work-Unit) | Type 3 (Gated-Community) | Type 4 (Relocated Housing) |
|---|---|---|---|---|
| Demography | ||||
| Gender | 0.924 | 1.188 | 1.119 | 1.452 ** |
| Age | 0.999 | 1.023 * | 1.025 * | 1.024 ** |
| Years living in Chengdu | 1.01 | 0.998 | 1.006 | 1.008 * |
| Years of education | 0.917 *** | 0.992 | 0.998 | 0.992 |
| Rural hukou | 0.611 * | 0.746 | 1.313 | 1.475 ** |
| Chengdu hukou | 0.442 *** | 0.844 | 1.236 | 0.962 |
| Household income level | 1.174 | 0.750 * | 1.068 | 0.974 |
| Chance of getting injured at work | 0.976 | 1.02 | 1.018 | 1.004 |
| Years of working | 1.012 | 1.018 * | 0.989 | 0.994 |
| Martial status | 0.785 | 1.041 | 0.742 | 0.987 |
| Household size | 1.067 | 0.923 | 1.071 | 0.99 |
| Lifestyle and Health Awareness | ||||
| Air quality perception | 1.09 | 1.295 *** | 1.218 * | 1.058 |
| Smoking | 0.885 | 1.054 | 0.723 | 0.987 |
| Hours of weekly exercise | 1.004 | 0.975 * | 0.99 | 0.999 |
| Health insurance | 0.927 | 0.96 | 1.2 | 1.358 * |
| Familiarity to asthma | 1.09 | 0.934 | 1.135 | 1.005 |
| Willing to pay for asthma treatment | 1.008 | 1.205 | 0.87 | 0.925 |
| Daily cooking time in family | 1.076 | 1.025 | 0.934 | 1.013 |
| Indoor environment | ||||
| Fuel use—LPG | 1.316 | 1.041 | 0.448 * | 0.949 |
| Fuel use—natural gas | 1.228 | 1.14 | 0.733 | 1.297 |
| Fuel use—electricity | 0.94 | 1.155 | 1.169 | 0.798 |
| Fuel use—coal | 0.432 | 1.572 | 0.569 | 0.858 |
| Hours of daily natural ventilation | 0.983 | 1.011 | 1.021 * | 1.016 * |
| Air conditioner | 0.670 * | 0.905 | 0.889 | 0.904 |
| Smoking in household | 1.216 | 1.037 | 1.426 * | 1.068 |
| Neighborhood environment | ||||
| Sidewalk in front of building | 0.631 | 0.584 | 0.927 | 1.372 |
| Building condition | 0.824 * | 0.973 | 1.03 | 1.056 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cai, Z.; Guan, C.; Trinh, A.; Zhang, B.; Chen, Z.; Srinivasan, S.; Nielsen, C. Satisfactions on Self-Perceived Health of Urban Residents in Chengdu, China: Gender, Age and the Built Environment. Sustainability 2022, 14, 13389. https://doi.org/10.3390/su142013389
Cai Z, Guan C, Trinh A, Zhang B, Chen Z, Srinivasan S, Nielsen C. Satisfactions on Self-Perceived Health of Urban Residents in Chengdu, China: Gender, Age and the Built Environment. Sustainability. 2022; 14(20):13389. https://doi.org/10.3390/su142013389
Chicago/Turabian StyleCai, Zhichang, ChengHe Guan, An Trinh, Bo Zhang, Zhibin Chen, Sumeeta Srinivasan, and Chris Nielsen. 2022. "Satisfactions on Self-Perceived Health of Urban Residents in Chengdu, China: Gender, Age and the Built Environment" Sustainability 14, no. 20: 13389. https://doi.org/10.3390/su142013389
APA StyleCai, Z., Guan, C., Trinh, A., Zhang, B., Chen, Z., Srinivasan, S., & Nielsen, C. (2022). Satisfactions on Self-Perceived Health of Urban Residents in Chengdu, China: Gender, Age and the Built Environment. Sustainability, 14(20), 13389. https://doi.org/10.3390/su142013389