
Current Trends in Interprofessional Shared Decision-Making Programmes in Health Professions Education: A Scoping Review


Abstract
1. Introduction
2. Methods
2.1. Research Questions
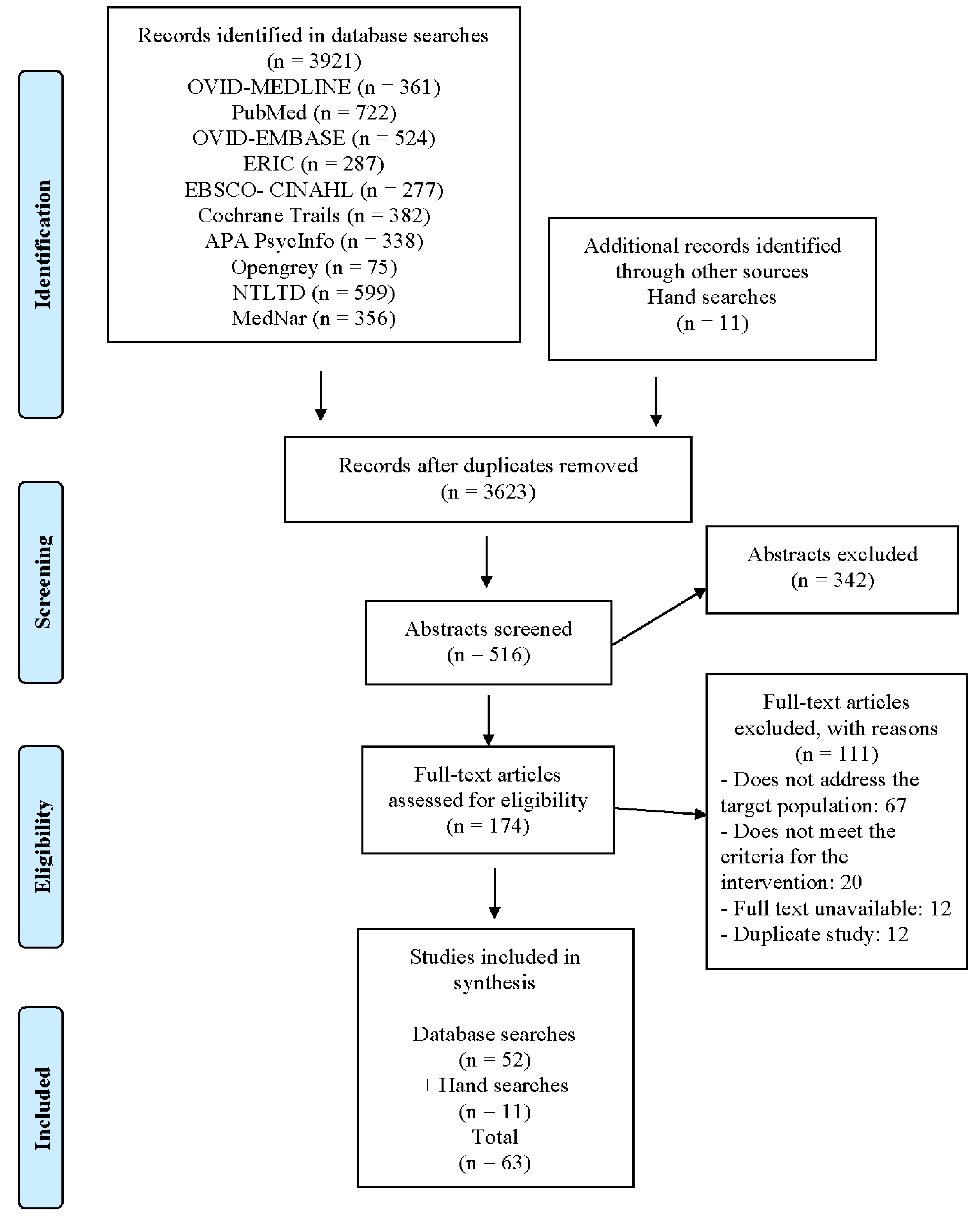
2.2. Search Strategy
2.3. Article Selection
2.3.1. Eligibility Criteria
2.3.2. Quality Assessment
2.4. Charting the Data
2.5. Collecting, Summarizing, and Reporting the Data
3. Results
3.1. Study Characteristics
3.2. Theoretical Frameworks for IP-SDM Educational Interventions
3.2.1. Educational Frameworks and Learning Theories
3.2.2. SDM Models and Their Components
3.3. IP-SDM Educational Applications and Delivery Methods
3.3.1. Population Characteristics
3.3.2. Intervention Characteristics
3.4. Assessed Outcomes in IP-SDM Educational Interventions
3.4.1. Evaluation Frameworks
3.4.2. SDM Measures and Instruments
3.4.3. Type of Outcomes
3.4.4. Summative and Formative Assessments
4. Discussion
5. Limitations of This Scoping Review
6. Conclusions
7. Practice Implications
8. Lessons for Practice
- More than half of the studies did not report using an educational framework or learning theory or SDM models. The one who did had various components and different steps. The studies that reported using SDM models are focused on communication and collaboration or decision aids.
- The current delivery methods of IP-SDM educational intervention included workshops, interactive learning sessions, case-based learning, videos, role play, observation, simulation, and online courses.
- The outcomes of IP-SDM educational interventions included collaboration and communication, clinical practice and outcome, patients’ value and preferences, and clinical decision-making skills.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dang, S. Shared decision making-the pinnacle of patient-centered care. J. Indian Acad. Geriatr. 2018, 14, 184. [Google Scholar]
- Elwyn, G.; Laitner, S.; Coulter, A.; Walker, E.; Watson, P.; Thomson, R. Implementing shared decision making in the NHS. BMJ 2010, 341, c5146. [Google Scholar] [CrossRef] [PubMed]
- Reimer, T.; Russell, T.; Roland, C. Decision-Making in Medical Teams. In Organizations, Communication, and Health, 1st ed.; Routledge: London, UK, 2015. [Google Scholar]
- World Health Organization. Improving the Quality and Use of Birth, Death and Cause-of-Death Information: Guidance for a Standards-Based Review of Country Practices; World Health Organization: Geneva, Switzerland; School of Population Health, University of Queensland: Herston, QLD, Australia, 2010. [Google Scholar]
- Reinke, L.; Hammer, B. The role of interprofessional collaboration in creating and supporting health care reform. Am. J. Respir. Crit. Care Med. 2011, 184, 863–864. [Google Scholar] [CrossRef] [PubMed]
- Shay, L.A.; Lafata, J.E. Where is the evidence? A systematic review of shared decision making and patient outcomes. Med. Decis. Mak. 2015, 35, 114–131. [Google Scholar] [CrossRef] [PubMed]
- Steffensen, K.; Vinter, M.; Crüger, D.; Dankl, K.; Coulter, A.; Stuart, B.; Berry, L.L. Lessons in integrating shared decision-making into cancer care. J. Oncol. Pract. 2018, 14, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.O.; Emanuel, E.J. Shared decision making to improve care and reduce costs. N. Engl. J. Med. 2013, 368, 6–8. [Google Scholar]
- Veroff, D.; Marr, A.; Wennberg, D.E. Enhanced support for shared decision making reduced costs of care for patients with preference-sensitive conditions. Health Aff. 2013, 32, 285–293. [Google Scholar] [CrossRef]
- Gravel, K.; Légaré, F.; Graham, I.D. Barriers and facilitators to implementing shared decision-making in clinical practice: A systematic review of health professionals’ perceptions. Implement. Sci. 2006, 1, 16. [Google Scholar] [CrossRef]
- Liberatore, M.; Nydick, R. The analytic hierarchy process in medical and health care decision making: A literature review. Eur. J. Oper. Res. 2008, 189, 194–207. [Google Scholar] [CrossRef]
- Légaré, F.; Stacey, D.; Graham, I.; Elwyn, G.; Pluye, P.; Gagnon, M.P.; Frosch, D.; Harrison, M.B.; Kryworuchko, J.; Pouliot, S.; et al. Advancing theories, models and measurement for an interprofessional approach to shared decision making in primary care: A study protocol. BMC Health Serv. Res. 2008, 8, 2. [Google Scholar] [CrossRef]
- Müller, E.; Strukava, A.; Scholl, I.; Härter, M.; Diouf, N.T.; Légaré, F.; Buchholz, A. Strategies to evaluate healthcare provider trainings in shared decision-making (SDM): A systematic review of evaluation studies. BMJ Open 2019, 9, e026488. [Google Scholar] [CrossRef]
- Siyam, T.; Shahid, A.; Perram, M.; Zuna, I.; Haque, F.; Archundia-Herrera, M.C.; Vohra, S.; Olson, K. A scoping review of interventions to promote the adoption of shared decision-making (SDM) among health care professionals in clinical practice. Patient Educ. Couns. 2019, 102, 1057–1066. [Google Scholar] [CrossRef]
- World Health Organization. Framework for Action on Interprofessional Education and Collaborative Practice. 2010. Available online: https://apps.who.int/iris/handle/10665/70185 (accessed on 11 September 2022).
- Reeves, S.; Fletcher, S.; Barr, H.; Birch, I.; Boet, S.; Davies, N.; McFadyen, A.; Rivera, J.; Kitto, S. A BEME systematic review of the effects of interprofessional education: BEME Guide No. 39. Med. Teach. 2016, 38, 656–668. [Google Scholar] [CrossRef]
- Cox, M.; Cuff, P.; Brandt, B.; Reeves, S.; Zierler, B. Measuring the impact of interprofessional education on collaborative practice and patient outcomes. J. Interprof. Care 2016, 30, 1–3. [Google Scholar] [CrossRef]
- Col, N.; Bozzuto, L.; Kirkegaard, P.; Loon, M.K.; Majeed, H.; Ng, C.J.; Pacheco-Huergo, V. Interprofessional education about shared decision making for patients in primary care settings. J. Interprof. Care 2011, 25, 409–415. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Buckley, S.; Coleman, J.; Davison, I.; Khan, K.S.; Zamora, J.; Malick, S.; Ashcroft, T.; Popovic, C.; Sayers, J. The educational effects of portfolios on undergraduate student learning: A Best Evidence Medical Education (BEME) systematic review. BEME Guide No. 11. Med. Teach. 2009, 31, 282–298. [Google Scholar] [CrossRef]
- Kryworuchko, J.; Hill, E.; Murray, M.A.; Stacey, D.; Fergusson, D.A. Interventions for shared decision-making about life support in the intensive care unit: A systematic review. Worldviews Evid.-Based Nurs. 2013, 10, 3–16. [Google Scholar] [CrossRef]
- Orchard, C.A.; King, G.A.; Khalili, H.; Bezzina, M.B. Assessment of interprofessional team collaboration scale (AITCS): Development and testing of the instrument. J. Contin. Educ. Health Prof. 2012, 32, 58–67. [Google Scholar] [CrossRef]
- Thomson, C.L.; Maskrey, N.; Vlaev, I. Making Decisions Better: An evaluation of an educational intervention. J. Eval. Clin. Pract. 2017, 23, 251–256. [Google Scholar] [CrossRef]
- Waldron, N.; Johnson, C.E.; Saul, P.; Waldron, H.; Chong, J.C.; Hill, A.-M.; Hayes, B. Development of a video-based education and process change intervention to improve advance cardiopulmonary resuscitation decision-making. BMC Health Serv. Res. 2016, 16, 555. [Google Scholar] [CrossRef] [PubMed]
- Sangaleti, C.; Schveitzer, M.C.; Peduzzi, M.; Zoboli, E.L.; Soares, C.B. Experiences and shared meaning of teamwork and interprofessional collaboration among health care professionals in primary health care settings: A systematic review. JBI Evid. Synth. 2017, 15, 2723–2788. [Google Scholar] [CrossRef]
- Nguyen, J.; Smith, L.; Hunter, J.; Harnett, J.E. Conventional and complementary medicine health care practitioners’ perspectives on interprofessional communication: A qualitative rapid review. Medicina 2019, 55, 650. [Google Scholar] [CrossRef]
- Shiao, T.H.; Yang, Y.Y.; Wu, C.Y.; Yang, L.-Y.; Hwang, S.-J.; Huang, C.-C.; Liang, J.-F.; Kao, S.-Y.; Lee, F.-Y. Creation of nurse-specific integrated interprofessional collaboration and team-efficiency scenario/video improves trainees’ attitudes and performances. J. Chin. Med. Assoc. 2019, 82, 546–553. [Google Scholar] [CrossRef]
- Voogdt-Pruis, H.R.; Ras, T.; Van Der Dussen, L.; Benjaminsen, S.; Goossens, P.H.; Raats, I.; Boss, G.; Van Hoef, E.F.M.; Lindhout, M.; Tjon-A-Tsien, M.R.S.; et al. Improvement of shared decision making in integrated stroke care: A before and after evaluation using a questionnaire survey. BMC Health Serv. Res. 2019, 19, 936. [Google Scholar] [CrossRef]
- Légaré, F.; Stacey, D.; Pouliot, S.; Gauvin, F.-P.; Desroches, S.; Kryworuchko, J.; Dunn, S.; Elwyn, G.; Frosch, D.; Gagnon, M.-P.; et al. Interprofessionalism and shared decision-making in primary care: A stepwise approach towards a new model. J. Interprof. Care 2011, 25, 18–25. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, J.E.; Cox, W.C.; Williams, C.R.; Shepherd, G. Rational and experiential decision-making preferences of third-year student pharmacists. Am. J. Pharm. Educ. 2014, 78, 120. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.O.; Oczkowski, S.J.; Hanvey, L.; Mbuagbaw, L.; You, J.J. Educational interventions to train healthcare professionals in end-of-life communication: A systematic review and meta-analysis. BMC Med. Educ. 2016, 16, 131. [Google Scholar] [CrossRef] [PubMed]
- Diouf, N.T.; Menear, M.; Robitaille, H.; Guérard, G.P.; Légaré, F. Training health professionals in shared decision making: Update of an international environmental scan. Patient Educ. Couns. 2016, 99, 1753–1758. [Google Scholar] [CrossRef]
- Johnsen, H.M.; Fossum, M.; Vivekananda-Schmidt, P.; Fruhling, A.; Slettebø, Å. Teaching clinical reasoning and decision-making skills to nursing students: Design, development, and usability evaluation of a serious game. Int. J. Med. Inform. 2016, 94, 39–48. [Google Scholar] [CrossRef]
- Kryworuchko, J.; Strachan, P.H.; Nouvet, E.; Downar, J.; You, J.J. Factors influencing communication and decision-making about life-sustaining technology during serious illness: A qualitative study. BMJ Open 2016, 6, e010451. [Google Scholar] [CrossRef]
- Lestari, E.; Stalmeijer, R.E.; Widyandana, D.; Scherpbier, A. Understanding students’ readiness for interprofessional learning in an Asian context: A mixed-methods study. BMC Med. Educ. 2016, 16, 179. [Google Scholar] [CrossRef]
- Lütgendorf-Caucig, C.; Kaiser, P.A.; Machacek, A.; Waldstein, C.; Pötter, R.; Löffler-Stastka, H. Vienna summer school on oncology: How to teach clinical decision making in a multidisciplinary environment. BMC Med. Educ. 2017, 17, 100. [Google Scholar] [CrossRef]
- Légaré, F.; Adekpedjou, R.; Stacey, D.; Turcotte, S.; Kryworuchko, J.; Graham, I.D.; Lyddiat, A.; Politi, M.C.; Thompson, R.; Elwyn, G.; et al. Interventions for increasing the use of shared decision making by healthcare professionals. Cochrane Database Syst. Rev. 2018, 7, CD006732. [Google Scholar] [CrossRef]
- Diendéré, G.; Dansokho, S.C.; Rocque, R.; Julien, A.-S.; Légaré, F.; Côté, L.; Mahmoudi, S.; Jacob, P.; Casais, N.A.; Pilote, L.; et al. How often do both core competencies of shared decision making occur in family medicine teaching clinics? Can. Fam. Physician 2019, 65, e64–e75. [Google Scholar]
- Noguera, A.; Arantzamendi, M.; López-Fidalgo, J.; Gea, A.; Acitores, A.; Arbea, L.; Centeno, C. Student’s inventory of professionalism (Sip): A tool to assess attitudes towards professional development based on palliative care undergraduate education. Int. J. Environ. Res. Public Health 2019, 16, 4925. [Google Scholar] [CrossRef]
- Rajendran, D.; Beazley, J.; Bright, P. Shared decision making by United Kingdom osteopathic students: An observational study using the OPTION-12 instrument. Chiropr. Man. Ther. 2019, 27, 42. [Google Scholar] [CrossRef]
- Allaire, A.S.; Labrecque, M.; Giguere, A.; Gagnon, M.P.; Légaré, F. What motivates family physicians to participate in training programs in shared decision making? J. Contin. Educ. Health Prof. 2012, 32, 98–107. [Google Scholar] [CrossRef]
- Beitinger, R.; Kissling, W.; Hamann, J. Trends and perspectives of shared decision-making in schizophrenia and related disorders. Curr. Opin. Psychiatry 2014, 27, 222–229. [Google Scholar] [CrossRef]
- Allen, K.A.; Dittmann, K.R.; Hutter, J.A.; Chuang, C.; Donald, M.L.; Enns, A.L.; Havonec, N.; Hunt, A.W.; Kellowan, R.S.; Linkewich, E.A.; et al. Implementing a shared decision-making and cognitive strategy-based intervention: Knowledge user perspectives and recommendations. J. Eval. Clin. Pract. 2020, 26, 575–581. [Google Scholar] [CrossRef]
- Kienlin, S.; Nytrøen, K.; Stacey, D.; Kasper, J. Ready for shared decision making: Pretesting a training module for health professionals on sharing decisions with their patients. J. Eval. Clin. Pract. 2020, 26, 610–621. [Google Scholar] [CrossRef]
- Keshmiri, F.; Rezai, M.; Tavakoli, N. The effect of interprofessional education on healthcare providers’ intentions to engage in interprofessional shared decision-making: Perspectives from the theory of planned behaviour. J. Eval. Clin. Pract. 2020, 26, 1153–1161. [Google Scholar] [CrossRef]
- Reed, C.R.; Garcia, L.I.; Slusser, M.; Konowitz, S.; Yep, J. Linking essential learning outcomes and interprofessional collaborative practice competency in health science undergraduates. J. Scholarsh. Teach. Learn. 2017, 17, 15–23. [Google Scholar] [CrossRef][Green Version]
- Wainwright, S.F.; Shepard, K.F.; Harman, L.B.; Stephens, J. Factors that influence the clinical decision making of novice and experienced physical therapists. Phys Ther. 2011, 91, 87–101. [Google Scholar] [CrossRef]
- Hansen, L.; Press, N.; Rosenkranz, S.J.; Baggs, J.G.; Kendall, J.; Kerber, A.; Williamson, A.; Chesnutt, M.S. Life-sustaining treatment decisions in the ICU for patients with ESLD: A prospective investigation. Res. Nurs. Health 2012, 35, 518–532. [Google Scholar] [CrossRef]
- Thompson, C.; Aitken, L.; Doran, D.; Dowding, D. An agenda for clinical decision making and judgement in nursing research and education. Int. J. Nurs. Stud. 2013, 50, 1720–1726. [Google Scholar] [CrossRef]
- Giguère, A.; Labrecque, M.; Njoya, M.; Thivierge, R.; Legare, F. Development of PRIDe: A tool to assess physicians’ preference of role in clinical decision making. Patient Educ. Couns. 2012, 88, 277–283. [Google Scholar] [CrossRef]
- Körner, M.; Ehrhardt, H.; Steger, A.K.; Bengel, J. Interprofessional SDM train-the-trainer program “Fit for SDM”: Provider satisfaction and impact on participation. Patient Educ. Couns. 2012, 89, 122–128. [Google Scholar] [CrossRef]
- Sheridan, S.L.; Golin, C.; Bunton, A.; Lykes, J.B.; Schwartz, B.; McCormack, L.; Driscoll, D.; Bangdiwala, S.I.; Harris, R.P. Shared decision making for prostate cancer screening: The results of a combined analysis of two practice-based randomized controlled trials. BMC Med. Inform. Decis. Mak. 2012, 12, 130. [Google Scholar] [CrossRef]
- Yu, C.H.; Ivers, N.M.; Stacey, D.; Rezmovitz, J.; Telner, D.; Thorpe, K.; Hall, S.; Settino, M.; Kaplan, D.M.; Coons, M.; et al. Impact of an interprofessional shared decision-making and goal-setting decision aid for patients with diabetes on decisional conflict–study protocol for a randomized controlled trial. Trials 2015, 16, 286. [Google Scholar] [CrossRef]
- Giguere, A.; Lawani, M.A.; Fortier-Brochu, É.; Carmichael, P.-H.; Légaré, F.; Kröger, E.; Witteman, H.O.; Voyer, P.; Caron, D.; Rodríguez, C. Tailoring and evaluating an intervention to improve shared decision-making among seniors with dementia, their caregivers, and healthcare providers: Study protocol for a randomized controlled trial. Trials 2018, 19, 332. [Google Scholar] [CrossRef] [PubMed]
- Hendricks-Ferguson, V.L.; Ruebling, I.; Sargeant, D.M.; Kienstra, K.; Eliot, K.A.; Howell, T.G.; Sebelski, C.A.; Moore, K.S.; Armstrong, K. Undergraduate students’ perspectives of healthcare professionals’ use of shared decision-making skills. J. Interprof. Care 2018, 32, 481–489. [Google Scholar] [CrossRef] [PubMed]
- Arenth, J.; Pituch, K.; Turnbull, J. Teaching the Skill of Shared Decision Making Utilizing a Novel Online Curriculum: A Blinded Randomized Controlled Pilot Study (S803). J. Pain Symptom Manag. 2019, 57, 481–482. [Google Scholar] [CrossRef]
- Hagoel, L.; Volz, S.; Palileo, L.M.; Eldar-Lissai, A.; Kamath, C.C.; Cox, E.D. Interprofessional education about decision support for patients across cultures. J. Interprof. Care 2011, 25, 431–433. [Google Scholar] [CrossRef] [PubMed]
- Lown, B.A.; Kryworuchko, J.; Bieber, C.; Lillie, D.M.; Kelly, C.; Berger, B.; Loh, A. Continuing professional development for interprofessional teams supporting patients in healthcare decision making. J. Interprof. Care 2011, 25, 401–408. [Google Scholar] [CrossRef]
- Neville, C.C.; Petro, R.; Mitchell, G.K.; Brady, S. Team decision making: Design, implementation and evaluation of an interprofessional education activity for undergraduate health science students. J. Interprof. Care 2013, 27, 523–525. [Google Scholar] [CrossRef]
- Thistlethwaite, J.; Dallest, K.; Moran, M.; Dunston, R.; Roberts, C.; Eley, D.; Bogossian, F.; Forman, D.; Bainbridge, L.; Drynan, D.; et al. Introducing the individual Teamwork Observation and Feedback Tool (iTOFT): Development and description of a new interprofessional teamwork measure. J. Interprof. Care 2016, 30, 526–528. [Google Scholar] [CrossRef]
- Elwyn, G.; Durand, M.A.; Song, J.; Aarts, J.; Barr, P.J.; Berger, Z.; Cochran, N.; Frosch, D.; Galasiński, D.; Gulbrandsen, P.; et al. A three-talk model for shared decision making: Multistage consultation process. BMJ 2017, 359, j4891. [Google Scholar] [CrossRef]
- Grey, C.; Constantine, L.; Baugh, G.M.; Lindenberger, E. Advance care planning and shared decision-making: An interprofessional role-playing workshop for medical and nursing students. MedEdPORTAL 2017, 13, 10644. [Google Scholar] [CrossRef]
- Green, M.J.; Levi, B.H. Teaching advance care planning to medical students with a computer-based decision aid. J. Cancer Educ. 2011, 26, 82–91. [Google Scholar] [CrossRef]
- Thompson, C.; Stapley, S. Do educational interventions improve nurses’ clinical decision making and judgement? A systematic review. Int. J. Nurs. Stud. 2011, 48, 881–893. [Google Scholar] [CrossRef]
- Légaré, F.; Politi, M.C.; Drolet, R.; Desroches, S.; Stacey, D.; Bekker, H. Training health professionals in shared decision-making: An international environmental scan. Patient Educ. Couns. 2012, 88, 159–169. [Google Scholar] [CrossRef]
- Légaré, F.; Labrecque, M.; Cauchon, M.; Castel, J.; Turcotte, S.; Grimshaw, J. Training family physicians in shared decision-making to reduce the overuse of antibiotics in acute respiratory infections: A cluster randomized trial. Can. Med. Assoc. J. 2012, 184, 726–734. [Google Scholar] [CrossRef]
- Körner, M.; Ehrhardt, H.; Steger, A.K. Designing an interprofessional training program for shared decision making. J. Interprof. Care 2013, 27, 146–154. [Google Scholar] [CrossRef]
- Schell, J.O.; Green, J.A.; Tulsky, J.A.; Arnold, R.M. Communication skills training for dialysis decision-making and end-of-life care in nephrology. Clin. J. Am. Soc. Nephrol. 2013, 8, 675–680. [Google Scholar] [CrossRef]
- Liaw, S.Y.; Zhou, W.T.; Lau, T.C.; Siau, C.; Chan, S.W. An interprofessional communication training using simulation to enhance safe care for a deteriorating patient. Nurse Educ. Today 2014, 34, 259–264. [Google Scholar] [CrossRef]
- Jo, K.H.; An, G.J. Effects of an educational programme on shared decision-making among korean nurses. Int. J. Nurs. Pract. 2015, 21, 839–846. [Google Scholar] [CrossRef]
- Simmons, L.; Leavitt, L.; Ray, A.; Fosburgh, B.; Sepucha, K. Shared decision making in common chronic conditions: Impact of a resident training workshop. Teach. Learn. Med. 2016, 28, 202–209. [Google Scholar] [CrossRef]
- Légaré, F.; Stacey, D.; Gagnon, S.; Dunn, S.; Pluye, P.; Frosch, D.; Kryworuchko, J.; Elwyn, G.; Gagnon, M.; Graham, I.D. Validating a conceptual model for an inter-professional approach to shared decision making: A mixed methods study. J. Eval. Clin. Pract. 2011, 17, 554–564. [Google Scholar] [CrossRef]
- Hales, B.M.; Hawryluck, L. An interactive educational workshop to improve end of life communication skills. J. Contin. Educ. Health Prof. 2008, 28, 241–255. [Google Scholar] [CrossRef]
- Wainwright, S.F.; Shepard, K.F.; Harman, L.B.; Stephens, J. Novice and experienced physical therapist clinicians: A comparison of how reflection is used to inform the clinical decision-making process. Phys. Ther. 2010, 90, 75–88. [Google Scholar] [CrossRef]
- Keefe, C.W.; Thompson, M.E.; Noel, M.M. Medical students, clinical preventive services, and shared decision-making. Acad. Med. 2002, 77, 1160–1161. [Google Scholar] [CrossRef]
- Stephenson, R.; Richardson, B. Building an interprofessional curriculum framework for health: A paradigm for health function. Adv. Health Sci. Educ. 2008, 13, 547–557. [Google Scholar] [CrossRef]
- Edwards, A.; Elwyn, G.; Wood, F.; Atwell, C.; Prior, L.; Houston, H. Shared decision making and risk communication in practice: A qualitative study of GPs’ experiences. Br. J. Gen. Pract. 2005, 55, 6–13. [Google Scholar]
- Elwyn, G.; Edwards, A.; Hood, K.; Robling, M.; Atwell, C.; Russell, I.; Wensing, M.; Grol, R. Achieving involvement: Process outcomes from a cluster randomized trial of shared decision-making skill development and use of risk communication aids in general practice. Fam. Pract. 2004, 21, 337–346. [Google Scholar] [CrossRef]
- Stacey, D.; Légaré, F.; Pouliot, S.; Kryworuchko, J.; Dunn, S. Shared decision-making models to inform an interprofessional perspective on decision making: A theory analysis. Patient Educ. Couns. 2010, 80, 164–172. [Google Scholar] [CrossRef]
- Curran, V. Interprofessional Education for Collaborative Patient-Centred Practice: Research Synthesis Paper. 2004. Unpublished Work. Available online: https://research.library.mun.ca/154/1/Interprofessional_Education_for_collaborative_patient_centred_practice.pdf (accessed on 1 October 2022).
- Xu, X.; Bos, N.; Wu, H. The relationship between medical student engagement in the provision of the school’s education programme and learning outcomes. Med. Teach. 2022, 4, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Cuff, N.; Particia, A. The Behavioral and Social Sciences in Medical School Curricula. In Improving Medical Education: Enhancing the Behavioral and Social Science Content of Medical School Curricula; National Academies Press: Washington, DC, USA, 2004. [Google Scholar]
- Carman, K.L.; Dardess, P.; Maurer, M.; Sofaer, S.; Adams, K.; Bechtel, C.; Sweeney, J. Patient and family engagement: A framework for understanding the elements and developing interventions and policies. Health Aff. 2013, 32, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Jha, V.; Quinton, N.; Bekker, H.; Roberts, T. Strategies and interventions for the involvement of real patients in medical education: A systematic review. Med. Educ. 2009, 43, 10–20. [Google Scholar] [CrossRef] [PubMed]
- Smeets, H.; Moser, A.; Sluijsmans, D.; Janssen-Brandt, X.; Van Merrienboer, J. The Design of Interprofessional Performance Assessments in Undergraduate Healthcare & Social Work Education: A Scoping Review. Health Interprof. Pract. Educ. 2021, 4, eP2144. [Google Scholar]
- Steinert, Y.; Mann, K.; Anderson, B.; Barnett, B.M.; Centeno, A.; Naismith, L.; Prideaux, D.; Spencer, J.; Tullo, E.; Viggiano, T.; et al. A systematic review of faculty development initiatives designed to enhance teaching effectiveness: A 10-year update: BEME Guide No. 40. Med. Teach. 2016, 38, 769–786. [Google Scholar] [CrossRef]


{kind=link}
| Ref No. | Author (s), Year of Publication | Title | Study Period | Country | Study Population and Sample Size (If Applicable) | Study Design | Methods/Methodology | SDM Definition | Data Collection Methods | Conclusion | Recommendations |
|---|---|---|---|---|---|---|---|---|---|---|---|
| [12] | Légaré et al., 2008 | Advancing theories, models and measurement for an interprofessional approach to shared decision-making in primary care: a study protocol | Not reported | Canada | (n = 70) experts in the field | Systematic review | Based on conceptual model and a set of measurement tools used to enhance an interprofessional approach to SDM in primary healthcare and pilot-tested with key stakeholders and primary healthcare teams. | A process by which a healthcare choice is made by practitioners together with the patient. | Face-to-face team meeting, interviews, and focus groups | This study protocol is informative for researchers interested in designing and/or conducting future studies and educating health professionals to improve how primary healthcare teams foster active participation of patients in making health decisions. | The need to foster a more coordinated interprofessional effort for implementing SDM in clinical practice. |
| [13] | Müller et al., 2019 | Strategies to evaluate healthcare provider trainings in shared decision-making (SDM): a systematic review of evaluation studies | Not reported | Germany | Not reported | Systematic review | Systematic review of studies evaluating healthcare provider trainings in SDM to analyse their evaluation strategies. | The patient and at least one clinician share information and values, deliberate the next step, and arrive at a jointly made decision. | Not reported | Strategies to evaluate HCP trainings in SDM varied largely. | The proposed evaluation framework maybe useful to structure future evaluation studies, but international agreement on a core set of outcomes is needed to improve evidence. |
| [18] | Col et al., 2011 | Interprofessional education about shared decision-making for patients in primary care settings | Not reported | United Kingdom | Not reported | Framework development | A two-part review highlights key elements for consideration in planning and implementing interprofessional educational interventions. | Decision making in preventive care. | Not reported | A framework for educators to construct their own teaching models following adult learning. | Understanding the concept of SDM; acquiring relevant communication skills to facilitate SDM; understanding professional values/sensitivities; understanding the roles of different professions within the relevant primary care group; and acquiring relevant skills to implement SDM. |
| [21] | Kryworuchko et al., 2013 | Interventions for Shared Decision-Making About Life Support in the Intensive Care Unit: A Systematic Review | Not reported | Canada | Not reported | Systematic review | A systematic review of randomized controlled trials of SDM interventions for the decision about using life support, limiting the use of life support, or withdrawing life support for hospitalized patients. | A process where healthcare professionals engage the patient and their family or surrogate decision-maker in the essential elements of the SDM process. | Not reported | Emerging evidence to guide clinical practice suggests that having someone on the interprofessional team assigned to the role of facilitating communication of the essential elements of SDM improves health outcomes. | Interventions that include essential elements of SDM need to be more thoroughly evaluated in order to determine their effectiveness and health impact and to guide clinical practice. |
| [22] | Orchard et al., 2012 | Assessment of Interprofessional Team Collaboration Scale (AITCS): Development and Testing of the Instrument | Not reported | Canada | (n = 125) practitioners from 7 healthcare teams and (n = 24) IPE experts | Diagnostic study | The characteristics of collaboration used to generate items related to each element. Scale items represent the 4 elements that are considered key to collaborative practice. | A process in which the patient and providers consider outcome probabilities and patients’ preferences and reach a healthcare decision based on mutual agreement. | Survey | The AITCS can be applied to continuing professional education interventions to determine change over time. | Further test and retest reliability and longitudinal study application are needed. |
| [23] | Thomson et al., 2017 | Making Decisions Better: an evaluation of an educational Intervention | Not reported | United Kingdom | (n = 85) primary care health professionals | Pre-intervention and post-intervention. | Three groups of primary care health professionals completed questionnaires using Likert scales to assess strength of agreement with decision-making statements. | Multiple complex skills, including information mastery, numeracy, communication of risks and benefits using a variety of techniques, and the interplay of two peoples’ cognitive and affective biases. | Questionnaire | Participation in the learning sessions significantly improved self-reported understanding of decision-making processes and application to clinical practice. | Further research should be undertaken to continue to build the evidence base for the explicit impact of decision-making teaching on evidence-based and individualized care. |
| [24] | Waldron et al., 2016 | Development of a video-based education and process change intervention to improve advance cardiopulmonary resuscitation decision-making | 13 months | Australia | 2 focus groups, (n = 8) consultants and (n = 10) junior doctors | Literature review | Utilize a framework to develop an intervention to improve advance CPR decision making. | A discussion with the patient that should be used to reach a common understanding about the medical treatment plan. | Focus groups | Approaches were developed to address physician and systemic barriers to advance CPR decision making and documentation. | Implementation and evaluation across hospital settings is required to examine utility and determine effect on quality of care. |
| [25] | Sangaleti et al., 2017 | Experiences and shared meaning of teamwork and interprofessional collaboration among health care professionals in primary health care settings: a systematic review | Not reported | Brazil | Not reported | Systematic review | A three-step search strategy was utilized. Ten databases were searched for papers published from 1980 to June 2015. | Not reported | Not reported | This review has identified possible actions that could improve implementation of teamwork and IPC in primary healthcare. | Not reported |
| [26] | Nguyen et al., 2019 | Conventional and Complementary Medicine Health Care Practitioners’ Perspectives on Interprofessional Communication: A Qualitative Rapid Review | 3 months | Australia | Not reported | Qualitative rapid literature review | Six databases were searched to identify original research and systematic reviews published since 2009. | “Sharing a philosophy of care and a common understanding pertaining to scope of practice and area of expertise” “Agreement among the practitioners of a shared vision, open-minded culture, credible supporters, suitable facilities and confidence in the clinical competency of the other practitioners” | Surveys, questionnaires, semi-structured interviews | IPC within and between conventional and complementary HCP is impacted by inter-related factors. | A diverse range of initiatives that facilitate interprofessional learning and collaboration are required to facilitate IPC and help overcome medical dominance and interprofessional cultural divides. |
| [27] | Shiao et al., 2019 | Creation of nurse-specific integrated interprofessional collaboration and team efficiency scenario/video improves trainees’ attitudes and performances | Not reported | Taiwan | (n = 36) nursing trainees, (n = 24) standardized partners | Prospective study | Mock simulation with two scenarios was held as pre-intervention IPC-TE assessment. Basic and advanced workshops were arranged for teams of intervention groups for creation of discipline-specific scenario and video. | Not reported | Survey | The implementation of a scenario creation-based training resulted in additional improvement in trainee IPC and TE behaviours and attitudes. | Future research can explore the impacts of this interventional program on clinical practice and long-lasting dynamics among nursing teams and other professional teams. |
| [28] | Voogdt-Pruis et al., 2019 | Improvement of shared decision-making in integrated stroke care: a before and after evaluation using a questionnaire survey | 7 months | Netherlands | (n = 25) healthcare professionals | Before and after evaluation study | The SDM implementation programme consisted of training for healthcare professional, tailored support, development of decision aids, and a social map of local stroke care. | An approach where clinicians and patients share the best available evidence when faced with the task of making decisions, and where patients are supported to consider options, to achieve informed preferences. | Questionnaire and in-depth interviews | The study indicated its feasibility to implement SDM in integrated stroke care. | Special attention should be given to the following activities: (1) the appointment of knowledge brokers, (2) agreements between HCPs on roles and responsibilities, (3) the timely investigation of patient’s preferences in the care process through discussions in a multidisciplinary meeting. |
| [29] | Légaré et al., 2011 | Interprofessionalism and shared decision-making in primary care: a stepwise approach towards a new model | 7 months | Canada | (n = 4) nurses, (n = 3) physicians, (n = 1) dietician, (n = 1) psychologist, (n = 1) anthropologist, and (n = 1) community health specialist | Model development | Participants were divided into 3 small interdisciplinary groups and were charged with using the blocks to develop and draw the figure of a new conceptual model in primary care. | A process by which a healthcare choice is made by a practitioner together with the patient and is said to be the crux of patient-centred care. | Questionnaire | The new IP-SDM model for primary care has the potential to unify the process of SDM in different healthcare system settings and with different health professionals. | It is important to identify factors that could affect the model’s implementation in primary healthcare practice, education, and applied health services research. |
| [30] | McLaughlin et al., 2014 | Rational and Experiential Decision-Making Preferences of Third-Year Student Pharmacists | Not reported | United States of America | (n = 114) pharmacist students | Mixed-method study | To collect data about student pharmacist decision-making styles. | A complex process that can vary based on individual, social, and context-specific influences. | Electronic survey | Student pharmacists favoured rational decision making over experiential decision making, which was similar to results of studies performed of other health professions. | This study suggested that there are 2 independent modes of processing that operate simultaneously and sequentially during decision making. |
| [31] | Chung et al., 2016 | Educational interventions to train healthcare professionals in end-of-life communication: a systematic review and meta-analysis | Not reported | Canada | Not reported | Systematic review | MEDLINE, Embase, CINAHL, ERIC, and the Cochrane Central Register of Controlled Trials were searched. | Interventions designed solely for information-sharing. | Not reported | Very-low- to low-quality evidence suggests that end-of-life communication training may improve healthcare professionals’ self-efficacy, knowledge, and EoL communication scores compared to usual teaching. | Further studies comparing two active educational interventions are recommended with a continued focus on contextually relevant high-level outcomes. |
| [32] | Diouf et al., 2016 | Training health professionals in shared decision-making: Update of an international environmental scan | 24 months | Canada | Not reported | Systematic review | Two systematic reviews were shared for SDM training programs targeting health professionals produced from 2011 to 2015. | A decision-making process jointly shared by patients and their healthcare providers. | Not reported | SDM training programs still vary widely. Most still focus on the single provider/patient dyad and few are evaluated. | Integration of SDM training into the mandatory academic curricula of health professionals to ensure a better dissemination of interprofessional SDM. |
| [33] | Johnsen et al., 2016 | Teaching clinical reasoning and decision-making skills to nursing students: Design, development, and usability evaluation of a serious game | Not reported | United Kingdom | (n = 6) nursing students and faculty members | Prototype development | Unified framework of usability called TURF (Task, User, Representation, and Function) and SG theory were employed to ensure a user-centred design. | Not reported | Questionnaire and individual interviews | The SG was perceived as being useful, usable, and satisfying. | The achievement of the desired functionality and the minimization of user–computer interface issues emphasize the importance of conducting a usability evaluation during the SG development process. |
| [34] | Kryworuchko et al., 2016 | Factors influencing communication and decision-making about life-sustaining technology during serious illness: a qualitative study | 12 months | Canada | (n = 30) healthcare professionals | Qualitative study | Used Flanagan’s critical incident technique (CIT) and interpretive description of open-ended interviews. | The integration of information about options with the patient’s values and preferences. | Open-ended in-depth individual interviews | A focus on more meaningful and productive dialogue with patients and families may improve decisions about life-sustaining technology. | Work is needed to acknowledge and support the non-curative role of healthcare and build capacity for the interprofessional team to engage in effective decision-making discussions. |
| [35] | Lestari et al., 2016 | Understanding students’ readiness for interprofessional learning in an Asian context: a mixed-methods study | Not reported | Indonesia | (n = 470) students from (medicine, nursing, midwifery, and dentistry) | Explanatory, sequential mixed-methods design | Collected quantitative data and the results of the questionnaire were then used as input for the qualitative data collection consisting of mono-professional focus group discussions. | Not reported | Mono-professional focus group discussions | Students were generally favourable to IPE opportunity that offered to them interprofessional leadership, collaboration, and communication skills. | The present study revealed several important reasons underlying students’ positive and negative perceptions of IPE implementation which may be addressed during the interprofessional learning process. |
| [36] | Lütgendorf-Caucig et al., 2017 | Vienna Summer School on Oncology: how to teach clinical decision-making in a multidisciplinary environment | 7 days | Austria | (n = 30) medical students | Educational approach | The program is comprised of two parts: clinical (T1) and research (T2). | Clinical decision making | Questionnaire | Clinical decision making should proceed based on the results of prototypic case-based-derived knowledge supporting associative and procedural learning processes. | Students should be prepared for multidisciplinary teaching in under- and postgraduate cancer education. |
| [37] | Légaré et al., 2018 | Interventions for increasing the use of shared decision-making by healthcare professionals (Review) | Not reported | Canada | Not reported | Review | CENTRAL, MEDLINE, Embase, and five other databases were searched on 15 June 2017 and two clinical trials registries and proceedings of relevant conferences. | A process by which a healthcare choice is made by the patient, significant others, or both with one or more healthcare professionals. | Not reported | Studies in this field of research are no different from those in other fields in that their methods may be inadequate; they may be too small; many fail to deal adequately with bias; and most are not replicated. | More and better research is required to strengthen the certainty of the evidence. |
| [38] | Diendéré et al., 2019 | How often do both core competencies of shared decision-making occur in family medicine teaching clinics? | 12 months | Canada | (n = 71) health professionals and (n = 238) patients | Qualitative and quantitative cross-sectional study | Collected a convenience sample of 250 visits in primary care, approximately 50 visits per site, considering both the need for a range of primary care consultations and the feasibility of the study. | The collaborative process by which health professionals and patients partner to make evidence-informed health decisions that reflect what matters to patients and their families. | Questionnaire | Health professionals in family medicine are making an effort to engage patients in shared decision making in routine daily practice. | The greatest potential for improvement might lie in value clarification; that is, discussing what matters to patients and families. |
| [39] | Noguera et al., 2019 | Student’s Inventory of Professionalism (SIP): A Tool to Assess Attitudes towards Professional Development Based on Palliative Care Undergraduate Education | Not reported | Spain | (n = 300) medical students | Sequential exploratory strategy mixed method | The inventory is built based on the themes that emerged from the analysis of four qualitative studies about nursing and medical students’ perceptions related to palliative care teaching interventions. | Helps medical students address several competencies related to being patient-centred and empathic. | Survey | This new inventory is grounded on students’ palliative care teaching experiences and seems to be valid to assess students’ professional development. | Including sociodemographic variables in future studies would allow to study which other personal and cultural factors influence professionalism learning. |
| [40] | Rajendran et al., 2019 | Shared decision-making by United Kingdom osteopathic students: an observational study using the OPTION-12 Instrument | Not reported | United Kingdom | (n = 30) medical students | Instrument validation | The use of reliable and validated OPTION-12 (O12) instrument to calculate a score that reflected the degree of SDM utility. | An approach where clinicians and patients make decisions together using the best available evidence. | Interviews | Students in this study did not practice competent SDM behaviours. | Effective educational strategies are required to ensure SDM behaviours reach competent levels. |
| [41] | Allaire et al., 2012 | What Motivates Family Physicians to Participate in Training Programs in Shared Decision-Making? | Not reported | Canada | (n = 39) family physicians | Pilot randomized trial | Small, interactive group workshops at each family medicine group. | The physician and the patient make a decision together based on the best available evidence and on the patient’s values and preferences, without discounting those of the physician. | Questionnaire and focus groups | Findings from this study cannot be generalized to the larger population of physicians, and additional research is needed to refine the understanding of factors influencing FPs’ participation in CPD programs in SDM. | CPD developers should make the program interesting, enjoyable, and professionally stimulating. |
| [42] | Beitinger et al., 2014 | Trends and perspectives of shared decision-making in schizophrenia and related disorders | Not reported | Germany | Not reported | Narrative review, systematic review | Narrative review of important studies on SDM in the years before 2012 and a systematic review for the time period May 2012–October 2013. | A model of how doctors and patients make medical decisions, which is seen as very applicable to mental health. | Questionnaire and interviews | SDM in mental health is complex, takes time, and involves more than just two participants; patients’ lack of decisional capacity is seen as the major barrier. | Healthcare professionals need more training in how to deal with difficult decisional situations. |
| [43] | Allen et al., 2020 | Implementing a shared decision-making and cognitive strategy-based intervention: Knowledge user perspectives and recommendations | Not reported | Canada | (n = 10) clinicians | Exploratory qualitative research design | Cognitive strategy-based intervention approach. | A person-centred process in which clinicians and patients collaborate to make decisions about assessments, treatment goals, and subsequent evidence-based treatment plans. | Semi-structured focus group | This study is based on a real-world implementation of an SDM-based intervention from the perspective of individual allied health professionals and interprofessional stroke rehabilitation teams. | Facilitators should lay out a framework for training, communication, and implementation that is structured but still provides flexibility for iterative learning and active problem-solving within the relevant practice context. |
| [44] | Kienlin et al., 2020 | Ready for shared decision-making: Pretesting a training module for health professionals on sharing decisions with their patients | 5 months | Norway | (n = 429) nurses, physicians, and health professional students | Descriptive mixed-methods study | The training was provided as two different applications (module AB (introduction and SDM-basics) and module ABC (introduction, SDM-basics, and interactive training)) with differing learning objectives, extent of interactivity, and duration (1 vs. 2 h). | A best practice approach for decision-making communication about health-related issues. | Questionnaires and focus group | The two SDM training modules met the basic requirements for use in a broader SDM implementation strategy and can even improve knowledge. | Findings to improve the education suggest higher emphasis on interprofessional teaching methods. |
| [45] | Keshmiri et al., 2020 | The effect of interprofessional education on healthcare providers’ intentions to engage in interprofessional shared decision-making: Perspectives from the theory of planned behaviour | Not reported | Iran | (n = 113) ED residents and nurses | Sequential explanatory mixed method | The intervention group was exposed to case-based learning sessions conducted by applying interprofessional strategies. Then, they were assessed before and 2 weeks after the intervention by a questionnaire designed based on the theory of planned behaviour. | Collaboration to make decisions about assessments and treatment goals. | Questionnaire, semi-structured individual interviews | The major findings of the current study indicated that IPE could significantly improve the learners’ intentions to engage in IP-SDM. | There is a need to develop the infrastructure of IP-SDM at different elements such as providers, administers, consumers, and contextual factors. |
| [46] | Reed et al., 2017 | Linking Essential Learning Outcomes and Interprofessional Collaborative Practice Competency in Health Science Undergraduates | 4 months | United States of America | (n = 94) medical students | Mixed methods | Several ethical decision-making models were presented, and student groups were required to use one to work through the ethical issues and come to a decision. | Articulate the impact of personal values and professional ethics in healthcare decision making. | Group presentation, individual scholarly paper | Results were as expected given students’ level of progression in the program and the university. | The strategy has potential for use in assessing a variety of Student Learning Outcomes if closely linked with course, program, and college outcomes. |
| [47] | Wainwright et al., 2011 | Factors That Influence the Clinical Decision-Making of Novice and Experienced Physical Therapists | Not reported | United States of America | (n = 3) clinicians | Qualitative research methods using grounded theory | Three participant pairs (each pair consisting of one novice and one experienced physical therapist). Case summaries of each participant provided the basis for within- and cross-case analysis. | A process including skills such as critical thinking and problem solving, which are essential to making appropriate decisions and taking action for the effective care of patients. | Interview | The results of the study may be used by educators and employers to develop and structure learning experiences and mentoring opportunities for students and novice learners. | The results of the present study may be used by academic and clinical educators to develop and structure learning experiences to facilitate CDM and reflection for novice clinicians or students. |
| [48] | Hansen et al., 2012 | Life-Sustaining Treatment Decisions in the ICU for Patients with ESLD: A Prospective Investigation | 14 months | United States of America | (n = 6) patients, (n = 19) family members, and (n = 122) health professionals | Prospective, multiple case design | Case studies began within 24–48 h of ICU admission and ended when LSTs were withheld or withdrawn, or when a patient died or was transferred out of the ICU. | Process by providing information about minor decisions and assessing families’ understanding of treatments. | Bedside observation, semi-structured interviews, medical record reviews, quantitative survey. | Sub themes described why patients and family members may not fully understand or comprehend the LST decision-making process. | Further research is needed to develop interventions that target patients, family members, and healthcare professionals. |
| [49] | Thompson et al., 2013 | An agenda for clinical decision-making and judgement in nursing research and education | Not reported | United Kingdom | Not reported | Review | The paper presents nine unanswered questions that researchers and educators might like to consider as a potential agenda for the future of research into this important area of nursing practice, training, and development. | The act of choosing between alternatives. | Not reported | The paper highlights the role of decisions and judgements made by nurses in improving quality in healthcare systems. | The real methodological, theoretical, and empirical advances will come from researchers and educators grappling with answering these questions. |
| [50] | Gigue’re et al., 2012 | Development of PRIDe: A tool to assess physicians’ preference of role in clinical decision-making | 6 months | Canada | (n = 39) family physicians | Pilot clustered randomized clinical trial | Evaluated the effectiveness of DECISION+. | When a doctor and a patient engage in a joint decisional process that is informed by the best scientific evidence on the harms and benefits of the relevant interventions and by the patient’s values and preferences. | Questionnaire | SDM training shows promising results, and the next step is to develop more clinical vignettes followed by questions inspired from this analysis. | The PRIDe instrument can be used in the assessment of health professionals’ attitude towards SDM after training in SDM. Additional research is needed to evaluate its validity before it can be recommended for use. |
| [51] | Körner et al., 2012 | Interprofessional SDM train-the-trainer programme “Fit for SDM”: provider satisfaction and impact on participation | Not reported | Germany | (n = 15) patients | Not reported | In step 1 the university project team trained the providers in executive positions in the clinics as trainers, who then in step 2 trained their staff in the healthcare team. | Not reported | Questionnaire | This is the first interprofessional SDM train-the-trainer program in Germany to bridge interprofessionalism and SDM. It was implemented successfully and evaluated positively. | Establishing IP- SDM training programs should be encouraged for all healthcare professionals. |
| [52] | Sheridan et al., 2012 | Shared decision-making for prostate cancer screening: the results of a combined analysis of 2 practice-based randomized controlled trials | 13 months | United States of America | (n = 36) physicians | Two separate randomized controlled trials | Two separate randomized controlled trials of the same prostate cancer intervention. | A process in which patients are involved as active partners in clinical decisions. | Survey | SDM interventions can increase men’s knowledge, alter their perceptions of prostate cancer screening, and reduce actual screening. However, they may not guarantee an increase in shared decisions. | More work is needed to determine the added value of a shared decision. |
| [53] | Yu et al., 2015 | Impact of an interprofessional shared decision-making and goal-setting decision aid for patients with diabetes on decisional conflict—study protocol for a randomized controlled trial | 12 months | Canada | (n = 40) patients with physician 1:1 ratio | Randomized controlled trial | The first step is a provider-directed implementation only; the second (after a 6-month delay) involves both provider- and patient-directed implementation. | Is the process whereby two or more healthcare professionals are involved in making the decision with the patient. | Individual semi structured interview | An individualized approach to patients with multiple chronic conditions using SDM and goal setting is a desirable strategy for achieving guideline-concordant treatment in a patient-centred fashion. | This trial will provide insights regarding strategies for the routine implementation of such interventions in clinical practice, and it will offer an assessment of the impact of this approach. |
| [54] | Giguère et al., 2018 | Tailoring and evaluating an intervention to improve shared decision-making among seniors with dementia, their caregivers, and healthcare providers: study protocol for a randomized controlled trial | Not reported | Canada | (n = 49) clinicians and (n = 27) caregivers | Two-armed, clustered randomized trial | Two phases: (1) design and tailor the intervention; and (2) implement and evaluate. | Proposes that clinicians and patients collaborate to make joint decisions based on the best evidence. | Interview approaches, questionnaires and audio-recorded discussions | The intervention empowered patients and their caregivers in their healthcare by fostering their participation as partners during the decision-making process. | Not reported |
| [55] | Hendricks-Ferguson et al., 2018 | Undergraduate students’ perspectives of healthcare professionals’ use of shared decision-making skills | Not reported | United States of America | (n = 42) students | Exploratory qualitative approach | Data consisted of student responses in a course reflection assignment that captured their perspectives about recommended SDM responses by HCPs. | Small-group discussions | Student reflection assignments | IPE and healthcare students can develop an understanding of SDM and ethical principles related to PCC. | Not reported |
| [56] | Arenth et al., 2019 | Teaching the Skill of Shared Decision-Making Utilizing a Novel Online Curriculum: a Blinded Randomized Controlled Pilot Study (S803) | Not reported | United States of America | Not reported | Not reported | The intervention group received a brief online curriculum aimed at teaching the skill of shared decision making. Participants from both groups then repeated the same simulation and were reassessed. | Conversations | Video recorded | An easily accessible educational intervention in the form of an online module format is an effective way of teaching these behaviours. | SDM behaviours in non-palliative care paediatric providers can be significantly improved by access to online educational modules. |
| [57] | Hagoel et al., 2011 | Interprofessional education about decision support for patients across cultures | Not reported | United States of America | Not reported | Curricula design | The literature on cultural competency and DS offers guidance on the objectives, competencies, and teaching strategies for an IP cross-cultural DS curriculum. | The potential to create misunderstandings and barriers among providers and between them and patients. | Videos of simulated cross-cultural, self-reflection, cross-cultural interactions with simulated patients, role play, observation | The literature on cultural competency and DS offers guidance on the objectives, competencies, and teaching strategies for an IP cross-cultural DS curriculum. | These topics are fertile ground for future research efforts in both education and healthcare, with findings that would support the refinement of decision aids and the movement of culturally competent DS into IP curricula and practice. |
| [58] | Lown et al., 2011 | Continuing professional development for interprofessional teams supporting patients in healthcare decision-making | Not reported | United States of America | Not reported | Curriculum development | Modification of the six-step approach to curriculum development advocated by Kern et al. to develop the model. | A complex process in which mutual influence, context, preferences, values, and information are shared in both the process and decision outcomes. | Questionnaire, open-ended questions, and semi-structured interviews | This model aligns curricular goals, objectives, educational strategies, and evaluation instrument strategies with desired learning and organizational outcomes. | Educational leaders and researchers can institutionalize such a model. |
| [59] | Neville et al., 2013 | Team decision-making: design, implementation and evaluation of an interprofessional education activity for undergraduate health science students | 6 months | Australia | (n = 33) nursing students, (n = 10), midwifery students, (n = 18) medical students | Cross-sectional study | All students were informed about this IPE program during an introductory lecture, which provided the evidence for the value of team decision making. The following week, students were allocated to an interprofessional mixed group that assessed the key issues. | Not reported | Questionnaire | Design, implementation, and evaluation of an IPE, team decision-making activity were reported. | This study contributed to the development of an innovative curriculum activity, which provided the opportunity for health science students to participate effectively in team decision making with the purpose of achieving better health outcomes. |
| [60] | Thistlethwaite et al., 2016 | Introducing the individual Teamwork Observation and Feedback Tool (iTOFT): Development and description of a new interprofessional teamwork measure | Not reported | Australia | Not reported | Not reported | Not reported | Not reported | Not reported | The advanced version is for senior students and junior health professionals and has 10 observable behaviours under four headings: “shared decision making”, “working in a team”, “leadership”, and “patient safety”. | Further testing is required to focus on its validity and educational impact. |
| [61] | Elwyn et al., 2017 | A three-talk model for shared decision-making: multistage consultation process | 12 months | United States of America | (n = 488) clinicians from 6 specialties | Multistage consultation process | Step 1: key informant commentary on revised model, Step 2: distribution of online survey to wider communities of interest, Step 3: review by medically qualified clinicians in six clinical specialties. | A process in which decisions are made in a collaborative way, where trustworthy information is provided in accessible formats about a set of options. | Survey | The revised model conveys the core principles of shared decision making by proposing easy-to-remember conversational steps to facilitate the use in teaching contexts. | Research will be encouraged in different countries to know whether the model can be translated, adapted, and used in different context and cultures. |
| [62] | Grey et al., 2017 | Advance Care Planning and Shared Decision-Making: An Interprofessional Role-Playing Workshop for Medical and Nursing Students | 24 months | United States of America | (n = 85) medical and nursing students | Flipped classroom workshop | During the 2 h workshop, students complete four role-play ACP scenarios with the following roles: patient, family member, nurse, and physician. | Not reported | Survey | This role-play activity allows students to practice ACP and SDM, both with patient and family presence, and in premeeting rounds with the healthcare team. | The workshop can be utilized in many other levels of education. |
| [63] | Green and Levi, 2011 | Teaching advance care planning to medical students with a computer-based decision aid | Not reported | United States of America | (n = 133) medical students | Prospective, randomized controlled design | The multimedia decision aid helps prepare users to engage in advance care planning discussions by providing education material and exercises designed. | End-of-life decision making | Questionnaire | Use of a computer-based decision aid may be an effective way to teach medical students how to discuss advance care planning with cancer patients. | Look for a national study comparing this intervention with existing teaching modalities for advance care planning, and also invite other medical educators to examine the program. |
| [64] | Thompson and Stapley, 2011 | Do educational interventions improve nurses’ clinical decision-making and judgement? A systematic review | Not reported | United Kingdom | Not reported | Systematic review | Studies published since 1960 reporting any educational intervention that aimed to improve nurses’ clinical judgements or decision making were included. | Clinical or diagnostic reasoning | Not reported | Educational interventions to improve nurses’ judgements and decisions are complex and the evidence from comparative studies does little to reduce the uncertainty about “what works”. | Study design and reporting requires improvement to maximize the information contained in reports of educational interventions. |
| [65] | Légaré et al., 2012 | Training health professionals in shared decision-making: an international environmental scan | Not reported | Canada | Not reported | Review | Environmental scan looking for programs that train health professionals in SDM | An interactive process in which patients and health professionals collaborate to choose healthcare. | Not reported | Health professional training programs in SDM vary widely in how and what they deliver, and evidence of their effectiveness is sparse. | The study suggests there is a need for international consensus on ways to address the variability in SDM training programs. |
| [66] | Légaré et al., 2012 | Training family physicians in shared decision-making to reduce the overuse of antibiotics in acute respiratory infections: a cluster randomized trial | 9 months | France | (n = 162) family physicians | Randomized trial | Twp study arms: DECISION+ 2 and control | Is recognized as an effective strategy for reducing the overuse of treatment options not clearly associated with benefits for all patients. | Questionnaire | The shared decision-making program DECISION+2 enhanced patient participation in decision making and led to fewer patients deciding to use antibiotics for acute respiratory infections. | Future studies should assess the effectiveness of SDM in other clinical areas. |
| [67] | Körner et al., 2013 | Designing an interprofessional training programme for shared decision-making | Not reported | Germany | (n = 36) patients and (n = 34) senior healthcare professionals | Cross-sectional mixed method | Two phases: focus groups of patients in the rehabilitation clinic and a second phase for the expert survey of senior healthcare professionals. | Is increasingly advocated as the ideal interaction model of external participation in patient–physician interaction. | Focus groups with patients and a survey of experts | The results of both assessments have been used to develop an interprofessional SDM training program for implementing internal and external participation in interprofessional teams in medical rehabilitation. | The approach ensures consideration of the important issues of internal and external participation and enhances acceptance of the implementation of training in these rehabilitation clinics. |
| [68] | Schell et al., 2013 | Communication skills training for dialysis decision-making and end-of-life care in nephrology | 1 month | United States of America | Not reported | Workshop design | NephroTalk was designed as a half-day workshop. | Helping patients define care goals, including end-of-life preferences. | Survey | NephroTalk is successful in improving preparedness among nephrology fellows for having difficult conversations about dialysis decision making and end-of-life care. | Disseminating NephroTalk to interested nephrology programs and encouraging education and awareness among nephrology educators. |
| [69] | Liaw et al., 2014 | An interprofessional communication training using simulation to enhance safe care for a deteriorating patient | Not reported | Singapore | (n = 127) medical and nursing students | Pre-test and post-test design | The program was conducted using full-scale simulation and communication strategies adapted from Team Strategies and Tools to Enhance Performance and Patient Safety (TeamSTEPPS). | Important factor in enhancing the students’ confidence to communicate. | Questionnaire | The Sim-IPE has better prepared the medical and nursing students in communicating with one another in providing safe care for deteriorating patients. | Future studies could conduct a more rigorous research methodology such as randomized controlled trial. |
| [70] | Jo and An, 2015 | Effects of an educational programme on shared decision-making among Korean nurses | 1 month | Korea | (n = 41) nurses | Quasi-experimental study | Twenty nurses in the control group received no intervention, and twenty-one nurses in the experimental group received the educational programme on SDM. | Is a comprehensive concept of sharing information about treatment choices and decision methods based on the values and autonomy of the patients, families, doctors, and nurses. | Questionnaire | This study suggests that the educational programme on SDM was effective in increasing the moral sensitivity and attitude towards SDM among Korean nurses. | Future studies should investigate the effects of implementing similar programmers for longer periods. |
| [71] | Simmons et al., 2016 | Shared decision-making in common chronic conditions: impact of a resident training workshop | 4 months | United States of America | (n = 130) internal medicine and paediatric medicine residents | Curriculum development | Workshop curriculum for internal medicine residents to promote SDM in treatment decisions. | An interactive process that involves the clinician, the patient, and the best available clinical evidence to select the right medical test or treatment for each patient. | Written course evaluations and direct observation | Internal medicine residents had considerable gaps in SDM skills as measured in a baseline written exercise. | Additional studies are warranted to examine whether the workshop was successful in increasing residents’ ability to implement skills in practice. |
| [72] | Légaré et al., 2011 | Validating a conceptual model for an interprofessional approach to shared decision-making: a mixed methods study | 3 months | Canada | (n = 79) stakeholders | Mixed Method | The participants were asked about the following: (1) propose changes to the IP-SDM model; (2) identify barriers and facilitators to the model’s implementation in clinical practice; and (3) assess the model using a theory appraisal questionnaire. | An approach whereby practitioners and patients communicate around decisions, referring to the best available evidence and deliberating upon the consequences of each option. | Group interviews and individual interviews | Stakeholders validated the new IP-SDM model for primary care settings and proposed few modifications. | Future research should assess if the model helps implement SDM in IP clinical practice. |
| [73] | Hales and Hawryluck, 2008 | An interactive educational workshop to improve end-of-life communication skills | Not reported | Canada | (n = 6) members of varying disciplines | Pre-test and post-test design | A one-day interactive continuing education workshop. | A difficult and complex process as a result of differing perspectives among healthcare providers, patients, and families regarding ethics, benefits of treatment, culture, and religious beliefs. | Questionnaire | An interactive workshop can be a valuable educational intervention for building capacity and confidence in end-of-life communication skills and ethical and legal knowledge for HCPs. | Further research in this area should focus on evaluation of the lasting impact of this intervention on clinical practice. |
| [74] | Wainwright et al., 2010 | Novice and Experienced Physical Therapist Clinicians: A Comparison of How Reflection Is Used to Inform the Clinical Decision-Making Process | Not reported | United States of America | (n = 3) clinicians | Qualitative research | Three participant pairs (each pair consisting of one novice and one experienced physical therapist). Case summaries of each participant provided the basis for within- and across-case analysis. | Reasoning that results in action. | Interview | The research provides information to educators, novice clinicians, and the clinicians who mentor these novices that may facilitate the development of mature clinical decision-making abilities. | The results of this study may be used by educators and employers to develop and structure learning experiences and mentoring opportunities to facilitate clinical decision-making abilities. |
| [75] | Keefe et al., 2002 | Medical Students, Clinical Preventive Services, and Shared Decision-Making | Not reported | United States of America | Not reported | Educational module | Not reported | Not reported | Videotaped discussion with a simulated patient | Medical students appear quite willing to accept SDM as a skill that they should have in working with patients, and this was the primary focus of the newly implemented module. | It would be helpful to provide students with more formative feedback and to develop faculty development programs around SDM. |
| [76] | Stephenson and Richardson, 2008 | Building an Interprofessional Curriculum Framework for Health: A Paradigm for Health Function | Not reported | United Kingdom | Not reported | Quasi-experimental | Adaption of ICF as a foundation for defining health status and for conceptualizing and formulating health-related client-focused problems. | Iterative process of reflection and reflexivity which takes into account wide evidence base relevant to the specific task of healthcare with the individual client and which can be developed in dialogue with other professionals. | Not reported | Client-focused practice and an iterative process of clinical reasoning based on a broad evidence base that conceptualizes healthcare as the maintenance, and promotion of health across the lifespan requires a re-conceptualizing of health. | The orientation of the curriculum needs to foster the development of collaboration and synergies of understanding between health professionals and between health professionals and clients of healthcare. |
| [77] | Edwards et al., 2005 | Shared decision-making and risk communication in practice A qualitative study of GPs’ experiences | 4 months | United Kingdom | (n = 20) GPs | Qualitative study | The trial interventions comprised training in SDM skills and the use of risk communication materials. | Not reported | Exit interviews and questionnaire evaluations | The promotion of “patient involvement” appears likely to continue. | All the study findings require corroboration with a wider sample of practicing professionals. |
| [78] | Elwyn et al., 2005 | Achieving involvement: process outcomes from a cluster randomized trial of shared decision-making skill development and use of risk communication aids in general practice | Not reported | United Kingdom | (n = 352) patients and (n = 20) GPs | Cluster randomized design | Separate interventions to enhance clinician skills in either SDM or the use of risk communication aids were devised and piloted; they were provided to the clinicians before each active trial phase. | Process of involving patients in clinical decisions. | Questionnaires, audio taping, and patient interviews | The clinicians were able to acquire the skills to implement SDM competences and to use risk communication aids. | Progress towards greater patient involvement in healthcare decision making is possible, and skill development in this area should be incorporated into postgraduate professional development programmes. |
| [79] | Stacey et al., 2010 | Shared decision-making models to inform an interprofessional perspective on decision-making: A theory analysis | Not reported | Canada | Not reported | Theory analysis | Model of SDM; described concepts with relational statements. Two independently appraised models. | Not reported | Not reported | Most SDM models failed to encompass an interprofessional approach. Those that included at least two professionals met few of the elements of interprofessional collaboration and had limited description of SDM processes. | Appraisal of SDM models highlights the need for a model that is more inclusive of an interprofessional approach. |
| [80] | Curran, 2004 | Interprofessional Education for Collaborative Patient-Centred Practice Research Synthesis Paper | 13 months | Canada | Not reported | Research synthesis paper | Literature review and environmental scan undertaken by a multidisciplinary group of researchers. | Enables the separate and shared knowledge and skills of healthcare providers to synergistically influence the client/patient care provided. | Online survey and in-depth interviews | The purpose of this paper is to summarize the main themes emerging from the research report and discussion papers. | Readers are advised to consult the specific report or discussion paper for further elaboration and description. |
| Ref No. | Author (s), Year of Publication | Title | Disease/Medical Specialties | Settings/Clinical Area | Health Professionals’ Involvement | Undergraduate or Postgraduate | Patient/Family Member Involvement | Type of Application | Educational Framework Learning Theory/ | Teaching Method/Activity/Strategy/Delivery | Focuses on Knowledge, Attitudes, and/or Skills | Intervention Duration | SDM Model/SDM Tool/SDM Design | DM Components |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| [12] | Légaré et al., 2008 | Advancing theories, models and measurement for an interprofessional approach to shared decision-making in primary care: a study protocol | Chronic disease | Primary healthcare | Nurses and physicians | Not reported | Patients | Quality of patient decision | Not reported | Not reported | Skills and attitude | Not reported | Transactional and descriptive models | Essential elements and ideal elements |
| [13] | Müller et al., 2019 | Strategies to evaluate healthcare provider trainings in shared decision-making (SDM): a systematic review of evaluation studies | Not reported | Healthcare settings | Healthcare providers | Not reported | Not reported | Not reported | Not reported | Lectures, case studies, role play, and group discussion | Knowledge, skills and attitude | Not reported | Not reported | Not reported |
| [18] | Col et al., 2011 | Interprofessional education about shared decision-making for patients in primary care settings | Not reported | Primary healthcare | Not reported | Not reported | Patients and family members | Cross-cultural issues | Adult learning | Practical, interactive, and problem-based learning | Knowledge and skills | Not reported | Not reported | Not reported |
| [21] | Kryworuchko et al., 2013 | Interventions for Shared Decision-Making About Life Support in the Intensive Care Unit: A Systematic Review | End-of-life care | Intensive care unit | Healthcare team members | Not reported | Patients and family members | Intervention for end-of-life care | Not reported | Conference and brochure | Knowledge, skills, and attitudes | Not reported | SDM framework | 9 elements |
| [22] | Orchard et al., 2012 | Assessment of Interprofessional Team Collaboration Scale (AITCS): Development and Testing of the Instrument | Orthopaedic general surgery, acute mental health, and palliative care | Long-term care | Clinical psychologist, speech–language pathologist, nurse practitioner, child and youth worker, ward clerk, recreation therapist, therapy assistant, and orderly. | Undergraduate and postgraduate | Patients and family members | Collaboration in teams | Not reported | Not reported | Knowledge, skills, and attitudes | Not reported | Not reported | 19 items |
| [23] | Thomson et al., 2017 | Making Decisions Better: an evaluation of an educational Intervention | Not reported | Clinical settings | GP registrars and nurses | Undergraduate | Patients | Understanding of decision-making processes | Reflecting on learning | Interactive learning sessions | Skills | Not reported | Not reported | Not reported |
| [24] | Waldron et al., 2016 | Development of a video-based education and process change intervention to improve advance cardiopulmonary resuscitation decision-making | End-of-life care | Inpatient hospital | Junior doctors and consultants | Undergraduate | Patients and family members | Advance CPR decision making and communication | Adult educational theory | Education videos | Knowledge and skills | Not reported | CPR decision-making practices | (i) Knowing what to say; (ii) knowing how to say it; (iii) wanting to say it. |
| [25] | Sangaleti et al., 2017 | Experiences and shared meaning of teamwork and interprofessional collaboration among health care professionals in primary health care settings: a systematic review | Integrative medicine, family medicine | Primary healthcare | Not reported | Not reported | Not reported | Not reported | Not reported | Not reported | Not reported | Not reported | Not reported | Not reported |
| [26] | Nguyen et al., 2019 | Conventional and Complementary Medicine Health Care Practitioners’ Perspectives on Interprofessional Communication: A Qualitative Rapid Review | Traditional and complementary medicine | Primary healthcare | Medical doctors, nurses, pharmacists, and other HCPs such as allied HCPs | Undergraduate and postgraduate | Patients and family members | Patient satisfaction, health literacy, treatment compliance, and quality of life | Not reported | Not reported | Knowledge, skills, and attitudes | Not reported | Not reported | Not reported |
| [27] | Shiao et al., 2019 | Creation of nurse-specific integrated interprofessional collaboration and team efficiency scenario/video improves trainees’ attitudes and performances | Internal medicine | Simulation | Nurses, medical students, and other professions | Undergraduate | Simulated patients | Team efficiency | Experiential learning theory | Role play, videos, and discussion | Knowledge and skills | 4 weeks | Not reported | Not reported |
| [28] | Voogdt-Pruis et al., 2019 | Improvement of shared decision-making in integrated stroke care: a before and after evaluation using a questionnaire survey | Stroke | Outpatient rehabilitation and primary healthcare | Rehabilitation nurse, occupational therapist, physiotherapist, speech therapist, psychologist, rehabilitation specialist, and care manager | Postgraduate | Patients and family members | Stroke care | Not reported | Role play | Knowledge and skills | 1 year | Not reported | Not reported |
| [29] | Légaré et al., 2011 | Interprofessionalism and shared decision-making in primary care:a stepwise approach towards a new model | Not reported | Primary healthcare | Nurses, physicians, dietician, psychologist, anthropologist, and community health specialist | Undergraduate and postgraduate | Patients and family members | Patient’s choices | Not reported | Workshop, presentations, and group discussion | Knowledge, skills, and attitudes | Not reported | IP-SDM model | 3 levels (micro, meso, macro) |
| [30] | McLaughlin et al., 2014 | Rational and Experiential Decision-Making Preferences of Third-Year Student Pharmacists | Not reported | University | Pharmacist students | Undergraduate | Not reported | Direct patient care and mitigation of medication errors | Not reported | Experiential decision-making activities | Knowledge and skills | Not reported | Not reported | Not reported |
| [31] | Chung et al., 2016 | Educational interventions to train healthcare professionals in end-of-life communication: a systematic review and meta-analysis | Palliative care | Not reported | Medical and nursing students | Undergraduate and postgraduate | Patients and family members | End-of-life communication | Not reported | Didactic lectures, small group discussions, role-play, direct observation, and feedback | Knowledge, skills, and attitudes | Not reported | Not reported | Not reported |
| [32] | Diouf et al., 2016 | Training health professionals in shared decision-making: Update of an international environmental scan | Generic, cancer, other chronic diseases | Primary healthcare | Physicians/residents, multiple professionals, and nurses | Not reported | Patients | Not reported | Not reported | Online course and traditional course | Knowledge, skills, and attitudes | Not reported | Not reported | Not reported |
| [33] | Johnsen et al., 2016 | Teaching clinical reasoning and decision-making skills to nursing students: Design, development, and usability evaluation of a serious game | Chronic obstructive pulmonary disease. | Home healthcare | Nursing students | Undergraduate | Simulated Patients | Clinical reasoning and decision-making skills | Clinical decision-making model and Bloom’s taxonomy | Simulation technology | Skills | Not reported | TURF (Task, User, Representation, and Function) | Not reported |
| [34] | Kryworuchko et al., 2016 | Factors influencing communication and decision-making about life-sustaining technology during serious illness: a qualitative study | End-of-life care | Hospital | Staff physicians, residents, and nurses | Postgraduate | Patients and family members | Use of life-sustaining technology | Not reported | Not reported | Skills and attitudes | 47 min | Not reported | Not reported |
| [35] | Lestari et al., 2016 | Understanding students’ readiness for interprofessional learning in an Asian context: a mixed-methods study | Not reported | University | Medical, nursing, midwifery, and dentistry students | Undergraduate | Simulated patients | Collaborative role | Not reported | Lectures | Knowledge, skills, and attitudes | Not reported | Not reported | Not reported |
| [36] | Lütgendorf-Caucig et al., 2017 | Vienna Summer School on Oncology: how to teach clinical decision-making in a multidisciplinary environment | Oncology | Hospital | Undergraduate medical students | Undergraduate | Not reported | Clinical decision-making in oncology | Kahneman model | Pre-module, presentations, classical lectures, workshops, and blended learning | Knowledge | 7 days | Not reported | Not reported |
| [37] | Légaré et al., 2018 | Interventions for increasing the use of shared decision-making by healthcare professionals (Review) | Cancer, cardiovascular diseases, psychiatric conditions | Primary and specialized care | Healthcare professionals (e.g., physicians, nurses, pharmacists, social workers) | Postgraduate | Patients and simulated patients | Not reported | Not reported | Not reported | Knowledge and skills | Not reported | Not reported | Not reported |
| [38] | Diendéré et al., 2019 | How often do both core competencies of shared decision-making occur in family medicine teaching clinics? | Family medicine | University teaching clinics | Family physicians, residents, nurses, and allied health professionals | Postgraduate | Patients | Chronic conditions, preventive care, and lifestyle issues | Not reported | Not reported | Skills | 4 to 6 days | Not reported | Not reported |
| [39] | Noguera et al., 2019 | Student’s Inventory of Professionalism (SIP): A Tool to Assess Attitudes towards Professional Development Based on Palliative Care Undergraduate Education | Palliative care | University | Medical students | Undergraduate | Patients | Not reported | Not reported | Workshop | Knowledge and attitudes | Not reported | Wilkinson’s framework | Not reported |
| [40] | Rajendran et al., 2019 | Shared decision-making by United Kingdom osteopathic students: an observational study using the OPTION-12 Instrument | Osteopathic | Teaching clinics | Fourth- and third-year students in the Osteopathic Educational Institute | Undergraduate | Patients | Long-term care management | Not reported | Not reported | Knowledge and skills | 7-week period | Not reported | Not reported |
| [41] | Allaire et al., 2012 | What Motivates Family Physicians to Participate in Training Programs in Shared Decision-Making? | Acute respiratory tract infections | Primary healthcare | Family physicians | Postgraduate | Patients | Level of agreement between the patient and the providers | Not reported | Workshops, videos, reflective exercises, and group discussion | Knowledge and skills | Workshops of 3 h each, for a total of 9 h over 4–6 months | DECISION+ | Major and minor components |
| [42] | Beitinger et al., 2014 | Trends and perspectives of shared decision-making in schizophrenia and related disorders | Mental Health | Clinics | Healthcare providers | Postgraduate | Patients and caregivers | Physicians’ communication skills | Not reported | Not reported | Skills | Not reported | Decision aids | Not reported |
| [43] | Allen et al., 2020 | Implementing a shared decision-making and cognitive strategy-based intervention: Knowledge user perspectives and recommendations | Stroke | Rehabilitation hospitals | Occupational therapists, physical therapists, and speech language pathologists | Postgraduate | Patients | Knowledge and capacity among interprofessional team member and outcomes for patients discharged from inpatient stroke rehabilitation | Constructivist learning theory | Workshops | Knowledge and skills | 4 months | Not reported | Not reported |
| [44] | Kienlin et al., 2020 | Ready for shared decision-making: Pretesting a training module for health professionals on sharing decisions with their patients | Not reported | University/college and hospital | Nurses, physicians, and health professional students | Undergraduate and postgraduate | Patients | Apply SDM in clinical practice | Not reported | Lecture | Knowledge and skills | 1 h vs. 2 h | Ready for SDM | Not reported |
| [45] | Keshmiri et al., 2020 | The effect of interprofessional education on healthcare providers’ intentions to engage in interprofessional shared decision-making: Perspectives from the theory of planned behaviour | Emergency medicine | University hospitals | ED residents and nurses | Postgraduate | Patients | Communication, teamwork, and recognizing the roles of team members | Not reported | Case-based learning sessions | Skills and attitudes | Not reported | IP-SDM model | Not reported |
| [46] | Reed et al., 2017 | Linking Essential Learning Outcomes and Interprofessional Collaborative Practice Competency in Health Science Undergraduates | Not reported | University | Health profession students | Not reported | Patients | Perform skills and express emotional responses | Not reported | Situated activities | Skills and attitudes | Not reported | Not reported | Not reported |
| [47] | Wainwright et al., 2011 | Factors That Influence the Clinical Decision-Making of Novice and Experienced Physical Therapists | Cerebrovascular accident | Rehabilitation settings | Three clinician pairs, consisting of one novice and one experienced physical therapist | Undergraduate and postgraduate | Patients | Reasoning skills | Reflection in Clinical Decision-Making Revised Model | Observation and interview | Knowledge, skills and attitudes | Not reported | Schön’s model | Informative factors and directive factors |
| [48] | Hansen et al., 2012 | Life-Sustaining Treatment Decisions in the ICU for Patients with ESLD: A Prospective Investigation | End-stage liver disease | Intensive care unit | Physicians, nurses, respiratory therapists, social workers, gastroenterology technician, and chaplain | Undergraduate and postgraduate | Patients and family members | Comfort care decisions | Not reported | Observation | Knowledge | 4–10 h each day, 3–6 morning hours and 1–4 h | Not reported | Not reported |
| [49] | Thompson et al., 2013 | An agenda for clinical decision-making and judgement in nursing research and education | Not reported | Not reported | Nurses | Not reported | Not reported | Nurse’s decision making | Not reported | Not reported | Knowledge and skills | Not reported | Computerized decision support systems | Not reported |
| [50] | Giguere et al., 2012 | Development of PRIDe: A tool to assess physicians’ preference of role in clinical decision-making | Acute respiratory infections | Not reported | Family physicians | Postgraduate | Patients | Decisional comfort | Not reported | Workshops, videos, reflective exercises, and group discussion | Knowledge, skills and attitudes | Not reported | Not reported | Not reported |
| [51] | Körner et al., 2012 | Interprofessional SDM train-the-trainer programme “Fit for SDM”: provider satisfaction and impact on participation | Not reported | Medical rehabilitation clinic | Not reported | Postgraduate | Not reported | Not reported | Not reported | Not reported | Knowledge | Not reported | Not reported | Not reported |
| [52] | Sheridan et al., 2012 | Shared decision-making for prostate cancer screening: the results of a combined analysis of 2 practice-based randomized controlled trials | Prostate cancer | Not reported | Physicians | Postgraduate | Patients | Patients’ participation | Not reported | Discussion and videos | Knowledge and attitudes | 1 h | O’Connor’s Decisional Conflict Scale | 53 items |
| [53] | Yu et al., 2015 | Impact of an interprofessional shared decision-making and goal-setting decision aid for patients with diabetes on decisional conflict—study protocol for a randomized controlled trial | Diabetes | Primary healthcare | Physicians, nurses, dietitians, and pharmacists | Postgraduate | Patients and family members | Decisional conflict, diabetes distress | Knowledge-to-Action Framework | Training videos and patient education pamphlet | Knowledge, skills | Not reported | IP-SDM framework | 7 steps |
| [54] | Giguère et al., 2018 | Tailoring and evaluating an intervention to improve shared decision-making among seniors with dementia, their caregivers, and healthcare providers: study protocol for a randomized controlled trial | Dementia | Medicine unit | Physicians and residents; nurses and other health or social services professionals | Postgraduate | Patients and caregivers | Patient involvement, decisional comfort, patient quality of life, caregiver burden, and decisional regret | Not reported | e-learning | Attitudes | Not reported | Not reported | Not reported |
| [55] | Hendricks-Ferguson et al., 2018 | Undergraduate students’ perspectives of healthcare professionals’ use of shared decision-making skills | Not reported | University | Medical students | Undergraduate | Not reported | SDM responses | Not reported | Discussion | Knowledge | Not reported | Not reported | Not reported |
| [56] | Arenth et al., 2019 | Teaching the Skill of Shared Decision-Making Utilizing a Novel Online Curriculum: a Blinded Randomized Controlled Pilot Study (S803) | Palliative care | Children’s hospital | Not reported | Postgraduate | Family members | Comfort care | Not reported | Video recorded in a simulated patient | Skills | Not reported | Not reported | Not reported |
| [57] | Hagoel et al., 2011 | Interprofessional education about decision support for patients across cultures | Not reported | Not reported | Not reported | Not reported | Patients | Cross-cultural issues | Adult learning | Scenarios, role playing, and videos | Knowledge, skills, and attitudes | Not reported | Explanatory models of illness or decision making | Not reported |
| [58] | Lown et al., 2011 | Continuing professional development for interprofessional teams supporting patients in healthcare decision-making | Not reported | University | Healthcare professionals | Undergraduate and postgraduate | Patients and family members | Decision support during the process of shared decision making | Six-step approach to curriculum development by Kern | Lectures, web-based targeted readings and other audiovisual resources, large and small group discussion, and problem-based learning | Knowledge, skills, and attitudes | Not reported | Not reported | 6 steps |
| [60] | Thistlethwaite et al., 2016 | Introducing the individual Teamwork Observation and Feedback Tool (iTOFT): Development and description of a new interprofessional teamwork measure | Not reported | University | Not reported | Not reported | Not reported | Not reported | Not reported | Not reported | Not reported | Not reported | Not reported | Not reported |
| [61] | Elwyn et al., 2017 | A three-talk model for shared decision-making: multistage consultation process | Internal medicine, family medicine, paediatrics | Not reported | Internal medicine, family medicine, and paediatric physicians | Postgraduate | Not reported | Patient’s choices | Not reported | Web-based cases and simulations | Skills and attitudes | 12 months | Three-talk model | Not reported |
| [62] | Grey et al., 2017 | Advance Care Planning and Shared Decision-Making: An Interprofessional Role-Playing Workshop for Medical and Nursing Students | Nephrology | University | Medical students and undergraduate nursing students | Undergraduate | Patients and family members | Quality conversations between the provider and the patient | Not reported | Role-playing workshop | Knowledge, skills, and attitudes | 135 min flipped classroom for 2 years | Not reported | Not reported |
| [63] | Green and Levi, 2011 | Teaching advance care planning to medical students with a computer-based decision aid | Cancer, amyotrophic lateral sclerosis | University | Medical students | Undergraduate | Patients | Advance care planning and directive | Not reported | Question–answer format, clinical vignettes, video clips, lectures, and small group discussion | Knowledge and skills | Not reported | Not reported | Not reported |
| [64] | Thompson and Stapley, 2011 | Do educational interventions improve nurses’ clinical decision-making and judgement? A systematic review | Not reported | Not reported | Not reported | Undergraduate and postgraduate | Patients | Decisional conflict | Social cognitive learning theory, decision analysis, and cognitive moral development theory | Critical thinking and problem-based learning | Skills | Not reported | The Outcome Present State model | Not reported |
| [65] | Légaré et al., 2012 | Training health professionals in shared decision-making: an international environmental scan | Palliative care, cardiovascular disease, prenatal screening, chronic pain, paediatrics, urology | Not reported | Any healthcare professions | Undergraduate and postgraduate | Patients and family members | Patient outcomes and organizational level | Not reported | Case-based discussion, small group educational session, role play, printed educational material, and feedback | Knowledge, skills and attitudes | Not reported | Ottawa Decision Support Framework | Not reported |
| [66] | Légaré et al., 2012 | Training family physicians in shared decision-making to reduce the overuse of antibiotics in acute respiratory infections: a cluster randomized trial | Acute respiratory infections | Practice teaching units | All family physicians, including physician teachers and residents | Postgraduate | Patients and family members | Decision to take antibiotics | Not reported | Online tutorial and workshop | Knowledge and attitudes | 2 h online tutorial followed by a 2 h interactive seminar | DECISION+2 | Not reported |
| [67] | Körner et al., 2013 | Designing an interprofessional training programme for shared decision-making | Not reported | Rehabilitation clinics | Medicine, psychotherapy, physical therapy, and nursing | Postgraduate | Patients | Management of feedback, talking with difficult team members, and moderate conflict discussion | Not reported | Focus group | Knowledge, skills, attitudes | Not reported | Model of integrated patient-centeredness and expanded model of SDM | Not reported |
| [68] | Schell et al., 2013 | Communication skills training for dialysis decision-making and end-of-life care in nephrology | Nephrology | University | Nephrology fellows | Postgraduate | Patients and family members | Delivering bad news and helping patients define care goals | The OncoTalk teaching model | Workshops | Knowledge and skills | 4 h workshop | NephroTalk | Specific skills demonstration and fellows’ skills practice |
| [69] | Liaw et al., 2014 | An interprofessional communication training using simulation to enhance safe care for a deteriorating patient | End-of-life care | Simulation | Medical and nursing students | Undergraduate | Not reported | Communication skills between medical and nursing students | Presage–process–product (3P) model | Simulation and small group interprofessional learning | Skills | 3 h small group interprofessional learning | Not reported | Not reported |
| [70] | Jo and An, 2015 | Effects of an educational programme on shared decision-making among Korean nurses | End-of-life care | University hospitals | Nurses | Postgraduate | Patients and family members | End-of-life care performance, moral sensitivity, and attitude towards shared decision | Not reported | Education programmer | Knowledge and attitudes | 4 weeks | Not reported | Not reported |
| [71] | Simmons et al., 2016 | Shared decision-making in common chronic conditions: impact of a resident training workshop | Diabetes, depression, hypertension, and hyperlipidaemia | Clinics | Internal medicine residents | Postgraduate | Patients | Practice in shared decision-making skills | Not reported | Written case exercise, a short didactic presentation, and role-playing exercises | Skills | 1 h for PGY-1 residents and 2 h for PGY 2–4 residents | 6 Steps to Shared Decision-Making framework | 6 steps |
| [72] | Légaré et al., 2011 | Validating a conceptual model for an interprofessional approach to shared decision-making: a mixed methods study | Down syndrome | Primary healthcare | Health professionals, medical education, and the healthcare policy environment clinicians from primary healthcare teams | Not reported | Patients | Making a decision regarding prenatal screening for Down syndrome | Not reported | Short video illustrating an IP-SDM approach | Knowledge, skills, and attitudes | Not reported | Revised IP-SDM model | Various phases |
| [73] | Hales and Hawryluck, 2008 | An interactive educational workshop to improve end-of-life communication skills | End-of-life care | Hospital | Critical care providers of varying disciplines | Undergraduate | Patients and family members | Delivery of sensitive news | Experiential learning | Interactive workshops | Knowledge and skills | 45 min stations | Not reported | Not reported |
| [74] | Wainwright et al., 2010 | Novice and Experienced Physical Therapist Clinicians: A Comparison of How Reflection Is Used to Inform the Clinical Decision-Making Process | Cerebrovascular accident | Clinics | Three clinician pairs, consisting of one novice and one experienced physical therapist | Undergraduate and postgraduate | Patients | Reasoning skills | Reflection in Clinical Decision-Making Revised Model | Observation and interview | Knowledge and skills | Not reported | Schön’s model | Attributes and behaviours of the participants |
| [75] | Keefe et al., 2002 | Medical Students, Clinical Preventive Services, and Shared Decision-Making | Cardiovascular disease and cancer | Simulation | Medical students | Undergraduate | Patients | Screening cancer and lipid profile | Model adapted from Braddock and colleagues | Not reported | Knowledge and skills | Not reported | Not reported | Not reported |
| [76] | Stephenson and Richardson, 2008 | Building an Interprofessional Curriculum Framework for Health: A Paradigm for Health Function | Chronic disease | University | Physicians, nurses, and occupational therapists | Undergraduate | Family members | Ethical decision | Not reported | Case study | Attitudes and knowledge | 3 of 5 sections taught in a course semester | Not reported | Not reported |
| [77] | Edwards et al., 2005 | Shared decision-making and risk communication in practice A qualitative study of GPs’ experiences | Surgery | Health authority | General practitioners (GPs) | Postgraduate | Patients | Patient involvement | Work-based experiential learning | Workshops | Skills | Not reported | Not reported | Not reported |
| [78] | Elwyn et al., 2005 | Achieving involvement: process outcomes from a cluster randomized trial of shared decision-making skill development and use of risk communication aids in general practice | Patients with known atrial fibrillation, prostatitis, menorrhagia, or menopausal symptoms | Urban and rural general practices | Recently qualified GPs | Postgraduate | Patients | Risk communication | Not reported | Workshops | Skills | Not reported | Simple risk communication aids | Not reported |
| [79] | Stacey et al., 2010 | Shared decision-making models to inform an interprofessional perspective on decision-making: A theory analysis | Not reported | Not reported | Not reported | Not reported | Not reported | Not reported | Not reported | Not reported | Knowledge and skills | Not reported | Not reported | Not reported |
| [80] | Curran, 2004 | Interprofessional Education for Collaborative Patient-Centred Practice Research Synthesis Paper | Not reported | Not reported | Not reported | Undergraduate | Patients and family members | Patient and provider satisfaction, patient outcomes | Experiential learning strategy and adult learning theory | Cooperative learning, small group learning, case-based learning, and problem-based learning | Knowledge, skills, and attitudes | Not reported | IECPCP Synthesis Framework | Separate components within the framework |
| Ref No. | Author (s), Year of Publication | Title | Evaluation Framework | Type of Outcome | SDM Measures/Instruments | Summative and/or Formative Assessment | Results |
|---|---|---|---|---|---|---|---|
| [12] | Légaré et al., 2008 | Advancing theories, models and measurement for an interprofessional approach to shared decision-making in primary care: a study protocol | Evaluation by McDowell and Newell and by Tremblay and collaborators | Impact on health systems and organizations | Measurement tools for enhancing an interprofessional approach to SDM in primary healthcare | Not reported | The authors of this systematic review concluded that it was important to study communication and decision making in relatively mundane contexts such as suggesting that SDM in primary healthcare contexts had been satisfactorily addressed. |
| [13] | Müller et al., 2019 | Strategies to evaluate healthcare provider trainings in shared decision-making (SDM): a systematic review of evaluation studies | Kirkpatrick’s evaluation levels and Quadruple Aim framework | Students’ professional development | Not reported | Summative and formative | Identified evaluation outcomes covered all categories of the proposed framework. |
| [18] | Col et al., 2011 | Interprofessional education about shared decision-making for patients in primary care settings | Not reported | Patient care | Patient decision aids | Not reported | A series of teaching methods using principles from adult learning. |
| [21] | Kryworuchko et al., 2013 | Interventions for Shared Decision-Making About Life Support in the Intensive Care Unit: A Systematic Review | Not reported | Patient’s value and preferences | Not reported | Not reported | The interventions were not harmful; they decreased family member anxiety and distress, shortened intensive care unit stay, but did not affect patient mortality. |
| [22] | Orchard et al., 2012 | Assessment of Interprofessional Team Collaboration Scale (AITCS): Development and Testing of the Instrument | Not reported | Team collaboration | Assessment of Interprofessional Team Collaboration Scale (AITCS) | Not reported | The AITCS can help healthcare teams enhance their development as teams by focusing attention on areas their members view as not being collaborative. |
| [23] | Thomson et al., 2017 | Making Decisions Better: an evaluation of an educational Intervention | Not reported | Understanding of decision-making processes and application to clinical practice | Joint Practice—PRE and POST | Formative | Participation in the learning sessions significantly improved self-reported understanding of decision-making processes and application to clinical practice. The extended learning sessions did not provide additional benefits over and above 2 half days or 1 whole day learning sessions. |
| [24] | Waldron et al., 2016 | Development of a video-based education and process change intervention to improve advance cardiopulmonary resuscitation decision-making | Not reported | Patients’ preferences | “Goals of Patient Care” (GOPC) form and Supportive and Palliative Care Indicators Tool (SPICT) tool | Not reported | CPR decision-making analysis: (i) knowing what to say; (ii) knowing how to say it; (iii) wanting to say it. |
| [25] | Sangaleti et al., 2017 | Experiences and shared meaning of teamwork and interprofessional collaboration among health care professionals in primary health care settings: a systematic review | Not reported | Team collaboration | Not reported | Not reported | Not reported |
| [26] | Nguyen et al., 2019 | Conventional and Complementary Medicine Health Care Practitioners’ Perspectives on Interprofessional Communication: A Qualitative Rapid Review | Not reported | Not reported | Not reported | Not reported | Four key themes were identified that impact IPC: medical dominance, clarity of HCP roles, a shared vision, and education and training. |
| [27] | Shiao et al., 2019 | Creation of nurse-specific integrated interprofessional collaboration and team efficiency scenario/video improves trainees’ attitudes and performances | Kirkpatrick’s Model | Team performance | Assessment of Interprofessional Team Collaboration Scale (AITCS) Attitudes Toward Interprofessional Health Care Teams Scale (ATHCTS) | Formative | Nursing trainees in intervention group gave high satisfaction score to this IIT intervention and increase in instructor-assessed team performance in the “partnership,” “cooperation,” and “shared decision making”. |
| [28] | Voogdt-Pruis et al., 2019 | Improvement of shared decision-making in integrated stroke care: a before and after evaluation using a questionnaire survey | Not reported | Patients’ preferences | Not reported | Formative | Healthcare professionals provided 8 recommendations for adoption of SDM in integrated stroke care. |
| [29] | Légaré et al., 2011 | Interprofessionalism and shared decision-making in primary care: a stepwise approach towards a new model | Not reported | Patients’ value and preferences | Nine theory appraisal criteria | Not reported | The model has the potential to improve traditional decision-making processes and working practices currently exercised in many industrialized healthcare systems. |
| [30] | McLaughlin et al., 2014 | Rational and Experiential Decision-Making Preferences of Third-Year Student Pharmacists | Not reported | Clinical problem-solving skills | The Rational-Experiential Inventory (REI-40) | Not reported | All correlations between REI-40 scores and incoming grade point average (GPA) and Pharmacy College Admission Test (PCAT) scores were weak. |
| [31] | Chung et al., 2016 | Educational interventions to train healthcare professionals in end-of-life communication: a systematic review and meta-analysis | Kirkpatrick’s Model | Students’ self-efficacy, knowledge, improvements in communication | Not reported | Not reported | Twenty were studies of educational interventions and were reviewed in this paper. |
| [32] | Diouf et al., 2016 | Training health professionals in shared decision-making: Update of an international environmental scan | Not reported | Training satisfaction | Not reported | Not reported | A total of 94 new eligible programs in 4 new countries and 2 new languages, for a total of 148 programs produced from 1996 to 2015. |
| [33] | Johnsen et al., 2016 | Teaching clinical reasoning and decision-making skills to nursing students: Design, development, and usability evaluation of a serious game | Not reported | Not reported | Cognitive walkthrough evaluations | Not reported | The SG was perceived as being realistic, clinically relevant, and at an adequate level of complexity for the intended users. |
| [34] | Kryworuchko et al., 2016 | Factors influencing communication and decision-making about life-sustaining technology during serious illness: a qualitative study | Flanagan’s critical incident technique | Healthcare professionals, patient and family engagement | DECIDE quantitative | Not reported | Several key factors that influenced communication and decision making about life-sustaining technology. |
| [35] | Lestari et al., 2016 | Understanding students’ readiness for interprofessional learning in an Asian context: a mixed-methods study | Not reported | Not reported | Readiness for Interprofessional Learning Scale (RIPLS) | Not reported | Medical students seemed to be the most prepared for IPE. |
| [36] | Lütgendorf-Caucig et al., 2017 | Vienna Summer School on Oncology: how to teach clinical decision-making in a multidisciplinary environment | Not reported | Students’ knowledge acquisition | Compulsory pre-VSSO and post-VSSO single choice questionnaire | Formative | Most students’ comments about the VSSO were very positive. |
| [37] | Légaré et al., 2018 | Interventions for increasing the use of shared decision-making by healthcare professionals (Review) | Not reported | Primary and secondary outcomes | Not reported | Not reported | There was insufficient information to determine the effects on decision regret, physical- or mental-health-related quality of life, or consultation length or costs. |
| [38] | Diendéré et al., 2019 | How often do both core competencies of shared decision-making occur in family medicine teaching clinics? | Not reported | Patients’ values clarification | The OPTION 5 (observing patient involvement in decision-making) | Formative | The core elements of SDM occurred together in nearly two-thirds of visits without any active intervention. |
| [39] | Noguera et al., 2019 | Student’s Inventory of Professionalism (SIP): A Tool to Assess Attitudes towards Professional Development Based on Palliative Care Undergraduate Education | Not reported | Students’ performance in educational activities | Student’s Inventory of Professionalism (SIP) | Not reported | “Student’s Inventory on Professionalism” to indicate with the name the construct explored and that it is grounded in students’ perceptions. |
| [40] | Rajendran et al., 2019 | Shared decision-making by United Kingdom osteopathic students: an observational study using the OPTION-12 Instrument | Not reported | SDM behaviours | Validated OPTION-12 (O12) instrument (observing patient involvement) scale | Formative | No significant differences between O12 score of the third- and fourth-year students, which implies that the extra year of clinical teaching and supervision does not result in a higher engagement of SDM within the undergraduate teaching clinic. |
| [41] | Allaire et al., 2012 | What Motivates Family Physicians to Participate in Training Programs in Shared Decision-Making? | Not reported | Decision conflict level | DECISION+ and decision conflict scale | Not reported | CPD developers should promote their programs as interesting, enjoyable, and professionally stimulating. |
| [42] | Beitinger et al., 2014 | Trends and perspectives of shared decision-making in schizophrenia and related disorders | Not reported | Patients’ self-advocacy | 9-item SDM Questionnaire (SDM-Q-9), SDM scale sum score, sum score of the decision-making subscale of the API, physician ratings of patient behaviour, OPTION scale, 28-item Empowerment Scale, adapted version of “Elements of Informed Decision-Making Scale”, COMRADE, patient rated | Not reported | There are only a few interventional studies measuring the outcome of SDM; existing research constantly shows positive, but small effects. |
| [43] | Allen et al., 2020 | Implementing a shared decision-making and cognitive strategy-based intervention: Knowledge user perspectives and recommendations | Integrated promoting action on research implementation in health services (iPARIHS) framework | Enhanced knowledge and capacity among interprofessional team members | Cognitive Orientation to daily Occupational Performance (CO-OP) | Not reported | Participants suggested there needs to be specific training and a familiarity with the language across professions and among patients to ensure consistency in documentation, verbal communication, and person-centred care. |
| [44] | Kienlin et al., 2020 | Ready for shared decision-making: Pretesting a training module for health professionals on sharing decisions with their patients | The Medical Research Council Complex Interventions Framework, Kirkpatrick’s model | Improve communication and patient involvement | Not reported | Summative and formative | Participants gained knowledge of SDM relevant for improved communication. This study has only evaluated the first two levels of the Kirkpatrick’s model, but the intention is to make changes based on these findings and evaluate the other levels involvement. |
| [45] | Keshmiri et al., 2020 | The effect of interprofessional education on healthcare providers’ intentions to engage in interprofessional shared decision-making: Perspectives from the theory of planned behaviour | Not reported | Team collaboration | TPB-based questionnaire | Not reported | The qualitative data analysis showed two main categories of “team-based facilitators” and “contextual challenges” as the main affecting factors in the engagement of participant in IP-SDM. |
| [46] | Reed et al., 2017 | Linking Essential Learning Outcomes and Interprofessional Collaborative Practice Competency in Health Science Undergraduates | Not reported | Students’ ethical reasoning decision | Interprofessional Collaborative Practice (IPCEP) Core Competency of Values/Ethics | Not reported | Most students demonstrated adequate achievement of the Interprofessional Collaborative Practice (IPCEP) Core Competency of Values/Ethics. |
| [47] | Wainwright et al., 2011 | Factors That Influence the Clinical Decision-Making of Novice and Experienced Physical Therapists | Reflection-on- action (ROA) | Clinical decision-making abilities | Semi-Structured Interview Question Guide: Think-Aloud Videotape Analysis Interviews | Not reported | The factors that influenced clinical decision making were categorized as informative or directive. Novice participants relied more on informative factors, whereas experienced participants were more likely to rely on directive factors. |
| [48] | Hansen et al., 2012 | Life-Sustaining Treatment Decisions in the ICU for Patients with ESLD: A Prospective Investigation | Signal detection theory, judgement analysis | Comfort care decisions | Not reported | Not reported | Findings suggest that including patients and family members in non-immediate lifesaving decisions and verifying early their understanding may help to improve the decision-making process. |
| [49] | Thompson et al., 2013 | An agenda for clinical decision-making and judgement in nursing research and education | Not reported | Improve quality in healthcare systems | Not reported | Not reported | CDSS can help improve practice but is limited. |
| [50] | Gigue’re et al., 2012 | Development of PRIDe: A tool to assess physicians’ preference of role in clinical decision-making | Not reported | Health professionals’ attitude towards SDM | Theory of Planned Behaviour-based questionnaire | Formative | Five items for potential inclusion in PRIDe. The results of these items were pooled, and their reliability and validity explored. |
| [51] | Körner et al., 2012 | Interprofessional SDM train-the-trainer programme “Fit for SDM”: provider satisfaction and impact on participation | Not reported | SDM skills and satisfaction | Not reported | Not reported | Not reported |
| [52] | Sheridan et al., 2012 | Shared decision-making for prostate cancer screening: the results of a combined analysis of 2 practice-based randomized controlled trials | “PSA is a Decision” | Patients’ knowledge | 3-item uncertainty subscale from O’Connor’s Decisional Conflict Scale | Not reported | Participants in the control group were additionally slightly less likely to consider prostate cancer screening a decision and slightly more likely to have key knowledge about prostate cancer screening. |
| [53] | Yu et al., 2015 | Impact of an interprofessional shared decision-making and goal-setting decision aid for patients with diabetes on decisional conflict—study protocol for a randomized controlled trial | Not reported | Improve clinical outcomes | Patient questionnaires of validated scales—SPIRIT checklist | Not reported | The development of an evidence-based SDM intervention for patients with diabetes and other conditions that was framed by the IP-SDM model and followed a user-centred approach. |
| [54] | Giguère et al., 2018 | Tailoring and evaluating an intervention to improve shared decision-making among seniors with dementia, their caregivers, and healthcare providers: study protocol for a randomized controlled trial | CollaboRATE instrument | Healthcare empowerment, caregiver burden, patient quality of life, and decisional regret | QoL-AD questionnaire | Not reported | Not reported |
| [55] | Hendricks-Ferguson et al., 2018 | Undergraduate students’ perspectives of healthcare professionals’ use of shared decision-making skills | Not reported | Understanding of SDM and ethical principles | Student reflection assignments | Not reported | Not reported |
| [56] | Arenth et al., 2019 | Teaching the Skill of Shared Decision-Making Utilizing a Novel Online Curriculum: a Blinded Randomized Controlled Pilot Study (S803) | Not reported | Comfort care decisions | Validated scoring tool for the degree of shared decision making | Not reported | Regression analysis demonstrated the odds of improved performance in mean total score for intervention groups was 39.78 times greater than that of the control group. |
| [57] | Hagoel et al., 2011 | Interprofessional education about decision support for patients across cultures | Not reported | Not reported | Not reported | Not reported | Not reported |
| [58] | Lown et al., 2011 | Continuing professional development for interprofessional teams supporting patients in healthcare decision-making | Kirkpatrick’s Model | Interpersonal and communication skills | OPTION instrument COMRADE instrument Team Dimensions Rating Form Collaboration and Satisfaction About Care Decisions | Summative and formative | The study describes a model that can be used to design, implement, and evaluate continuing education curricula in IP-SDM and decision support. |
| [59] | Neville et al., 2013 | Team decision-making: design, implementation and evaluation of an interprofessional education activity for undergraduate health science students | Not reported | Team effectiveness | Readiness for Interprofessional Learning Scale, Interdisciplinary Education Perception Scale, and the Role Perception Questionnaires | Not reported | Students were willing to share their knowledge and skills as a way of understanding clinical problems in the workplace and had professionally oriented perceptions and related affective domains. |
| [60] | Thistlethwaite et al., 2016 | Introducing the individual Teamwork Observation and Feedback Tool (iTOFT): Development and description of a new interprofessional teamwork measure | Not reported | Clinical teamwork experience | Individual Teamwork Observation and Feedback Tool (iTOFT) | Formative | Not reported |
| [61] | Elwyn et al., 2017 | A three-talk model for shared decision-making: multistage consultation process | SHARE (Seek participation, Help comparison, Assess values, Reach decision, Evaluate decision) | Patients’ preferences | Not reported | Not reported | A new three-talk model of SDM is proposed, based on “team talk”, “option talk”, and “decision talk”, to depict a process of collaboration and deliberation. |
| [62] | Grey et al., 2017 | Advance Care Planning and Shared Decision-Making: An Interprofessional Role-Playing Workshop for Medical and Nursing Students | Not reported | Teaching effectiveness | Not reported | Formative | Advance care planning (ACP) exposure during student training helps trainees recognize the impact of high-quality interprofessional conversations on the care patients want and ultimately receive. |
| [63] | Green and Levi, 2011 | Teaching advance care planning to medical students with a computer-based decision aid | Not reported | Students’ knowledge, skill, and satisfaction | Pre-intervention and post-intervention evaluations and evaluation of student performance by patients, 17-item true/false and multiple-choice test, self-assessment instrument, 12-item instrument that addressed students’ communication skills | Formative | Patients in the decision aid group were more satisfied with the advance care planning method and with several aspects of student performance. |
| [64] | Thompson and Stapley, 2011 | Do educational interventions improve nurses’ clinical decision-making and judgement? A systematic review | Outcome Present State model | Patient outcomes | Not reported | Formative | From 5262 initial citations 24 studies were included in the review. The effectiveness and efficacy of interventions was mixed. |
| [65] | Légaré et al., 2012 | Training health professionals in shared decision-making: an international environmental scan | Kirkpatrick’s Model | Patient outcomes and organizational level | Not reported | Not reported | A total of 54 programs conducted between 1996 and 2011 in 14 countries and 10 languages. |
| [66] | Légaré et al., 2012 | Training family physicians in shared decision-making to reduce the overuse of antibiotics in acute respiratory infections: a cluster randomized trial | Not reported | Patients’ adherence to the decision | Decisional Conflict Scale | Not reported | The percentage of patients who decided to use antibiotics after consultation was 52.2% in the control group and 27.2% in the DECISION+2 group. |
| [67] | Körner et al., 2013 | Designing an interprofessional training programme for shared decision-making | Not reported | External participation (interaction between patient and healthcare professionals) and internal participation (communication, coordination, and cooperation in the interprofessional team) | Not reported | Not reported | The results indicate the importance of internal and external participation in interprofessional settings. |
| [68] | Schell et al., 2013 | Communication skills training for dialysis decision-making and end-of-life care in nephrology | Not reported | End-of-life preferences | Not reported | Not reported | The results presented highlight the need for structured communication education in nephrology programs. |
| [69] | Liaw et al., 2014 | An interprofessional communication training using simulation to enhance safe care for a deteriorating patient | Not reported | Students’ self-confidence | The C-scale with 10-point scales | Formative | Both medicine and nursing groups demonstrated a significant improvement on post-test score from pre-test score for self-confidence and perception. The participants were highly satisfied with their simulation learning. |
| [70] | Jo and An, 2015 | Effects of an educational programme on shared decision-making among Korean nurses | Not reported | End-of-life care performance, moral sensitivity, and attitude towards SDM | End-of-life care performance scale, Moral Sensitivity Questionnaire, attitude towards shared decision-making scale | Not reported | The experimental group showed significantly higher scores in moral sensitivity and attitude towards SDM after the intervention compared with the control group. |
| [71] | Simmons et al., 2016 | Shared decision-making in common chronic conditions: impact of a resident training workshop | Not reported | Health behaviours, adherence, health outcomes | Not reported | Formative | Residents were involved in the development of the workshop and helped identify key content, suggested framing for difficult topics, and confirmed the need for the skills workshop. |
| [72] | Légaré et al., 2011 | Validating a conceptual model for an interprofessional approach to shared decision-making: a mixed methods study | Not reported | Interprofessional collaboration | Theory appraisal questionnaire scale | Not reported | Stakeholders suggested placing the patient at its centre; extending the concept of family to include significant others; clarifying outcomes; highlighting the concept of time; merging the micro, meso, and macro levels in one figure. |
| [73] | Hales and Hawryluck, 2008 | An interactive educational workshop to improve end-of-life communication skills | Not reported | End of life communication, ethical and legal knowledge for clinicians | Preworkshop and postworkshop evaluations | Formative | High overall perception of success and achievement of educational objectives. |
| [74] | Wainwright et al., 2010 | Novice and Experienced Physical Therapist Clinicians: A Comparison of How Reflection Is Used to Inform the Clinical Decision-Making Process | Reflection on- action (ROA) | Clinical decision-making abilities | Semi-Structured Interview Question Guide: Think-Aloud Videotape Analysis Interviews | Formative | The data illustrate the theme of reflection as it is used to inform the clinical decision-making process. |
| [75] | Keefe et al., 2002 | Medical Students, Clinical Preventive Services, and Shared Decision-Making | Not reported | Skills development | Checklist on the elements of SDM | Summative and formative | Explicit model that allows students to demonstrate a process for SDM is a good introductory tool. |
| [76] | Stephenson and Richardson, 2008 | Building an Interprofessional Curriculum Framework for Health: A Paradigm for Health Function | Not reported | Client function | Not reported | Not reported | The framework can promulgate a paradigm of practice within an interprofessional dialogue of healthcare. |
| [77] | Edwards et al., 2005 | Shared decision-making and risk communication in practice A qualitative study of GPs’ experiences | Not reported | SDM skills | Not reported | Not reported | The GPs indicated positive attitudes towards involving patients and described positive effects on their consultations. |
| [78] | Elwyn et al., 2005 | Achieving involvement: process outcomes from a cluster randomized trial of shared decision-making skill development and use of risk communication aids in general practice | OPTION: observing patients, multilevel modelling involvement | SDM skills | OPTION scale | Formative | Clinicians increased the proportion of consultations in which they used several categories of risk information after the risk communication training intervention. |
| [79] | Stacey et al., 2010 | Shared decision-making models to inform an interprofessional perspective on decision-making: A theory analysis | Medical Research Council framework | Interprofessional collaboration | Not reported | Not reported | The 15 unique models included 18 core concepts. Of two models that included more than one health professional collaborating with the patient, one included 3 of 10 elements of interprofessional collaboration and the other included 1 element. |
| [80] | Curran, 2004 | Interprofessional Education for Collaborative Patient-Centred Practice Research Synthesis Paper | Not reported | Patient and provider satisfaction, patient outcomes | Team Oral Structured Clinical Examination or (TOSCE) | Not reported | Main factors determinants and elements as they relate to the micro, meso, and macro levels. |
| A. Study Characteristics/General Information | |
| Country | |
| Canada | 19 (30%) |
| USA | 16 (24%) |
| UK | 9 (14%) |
| Australia | 4 (7%) |
| Germany | 4 (7%) |
| Other * | 11 (18%) |
| Study design | |
| Review | 14 (22%) |
| Before and after evaluation study Pre-intervention and post-intervention | 5 (8%) |
| Explanatory, qualitative study | 6 (10%) |
| Instrument design, instrument validation, curriculum development, curriculum design | 15 (24%) |
| Mixed-method design | 9 (14%) |
| Cross-sectional design | 1 (2%) |
| Randomized controlled trial | 9 (14%) |
| Quasi-experimental, survey, action research | 1 (2%) |
| N/A | 3 (4%) |
| B. SDM interventions | |
| Disease(s)/medical specialties | |
| Down syndrome | 1 (2%) |
| Family medicine/internal medicine/chronic diseases, including diabetes, stroke, liver diseases, lung diseases, cardiovascular diseases | 22 (34%) |
| End-of-life/palliative care/oncology | 14 (21%) |
| Orthopaedic/osteopathic/surgery | 3 (5%) |
| Integrative medicine/traditional and complementary medicine | 2 (3%) |
| Mental health | 1 (2%) |
| Emergency medicine | 1 (2%) |
| Not reported | 19 (31%) |
| Settings/clinical area | |
| Primary healthcare | 9 (14%) |
| Intensive care unit | 2 (4%) |
| Long-term care/home healthcare | 2 (4%) |
| Hospital | 10 (15%) |
| Simulation | 3 (5%) |
| Outpatient clinic | 7 (11%) |
| University teaching clinic | 17 (26%) |
| Health authority | 1 (2%) |
| Urban and rural general practices | 1 (2%) |
| Not reported | 11 (17%) |
| Undergraduate and/or postgraduate | |
| Undergraduate | 18 (29%) |
| Postgraduate | 22 (35%) |
| Both | 11 (17%) |
| Not reported | 12 (19%) |
| Patient/family member involvement | |
| Patient | 28 (44%) |
| Family member | 2 (4%) |
| Both | 21 (32%) |
| None | 12 (20%) |
| Type of decisions/applications | |
| Decision quality | 6 (9%) |
| Communication and collaboration | 18 (28%) |
| Patient care, satisfaction | 10 (16%) |
| Healthcare choice | 8 (13%) |
| Application in clinical practice | 2 (3%) |
| SDM processes | 4 (6%) |
| Clinical reasoning | 3 (5%) |
| Use of technology | 1 (2%) |
| Ethical decision | 1 (2%) |
| Cultural issue | 2 (3%) |
| Not reported | 8 (13%) |
| Teaching method/activity/strategy/delivery | |
| Video | 4 (6%) |
| Role play | 4 (6%) |
| Observation | 3 (5%) |
| Interactive learning sessions, discussion | 9 (15%) |
| Case-based learning | 5 (8%) |
| Lectures | 5 (8%) |
| Online course | 3 (5%) |
| Blended learning | 1 (2%) |
| Simulation | 3 (5%) |
| Workshop | 11 (17%) |
| Not reported | 15 (23%) |
| Focuses on knowledge, attitudes, skills | |
| Knowledge | 4 (6%) |
| Attitudes | 1 (2%) |
| Skills | 10 (16%) |
| All | 17 (27%) |
| Knowledge and attitudes | 5 (8%) |
| Knowledge and skills | 19 (30%) |
| Attitudes and skills | 5 (8%) |
| N/A | 2 (3%) |
| Intervention duration | |
| Less than 2 h | 5 (8%) |
| 3–4 h | 3 (5%) |
| 1–7 days | 3 (5%) |
| 1–8 weeks | 3 (5%) |
| 2–12 months | 5 (8%) |
| Longer than 12 months | 1 (2%) |
| Not reported | 43 (67%) |
| C. Outcomes | |
| Summative and/or formative assessment | |
| Summative only | 0 (0%) |
| Formative only | 16 (25%) |
| Summative and formative | 4 (7%) |
| None | 43 (68%) |
| Types of outcomes | |
| Health system and organization | 3 (5%) |
| Collaboration and communication | 13 (21%) |
| Patients’ value and preferences | 8 (13%) |
| Clinical practice and outcome | 9 (14%) |
| Problem-solving skills | 2 (3%) |
| Students’ knowledge acquisition | 2 (3%) |
| Satisfaction | 3 (5%) |
| Students’ professional development | 3 (5%) |
| SDM behaviours | 1 (2%) |
| Students’ ethical reasoning decision | 2 (3%) |
| Clinical decision-making skills | 7 (10%) |
| End-of-life care | 5 (8%) |
| Health professionals’ attitude towards SDM | 1 (2%) |
| Not reported | 4 (6%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sultan, L.; Alsaywid, B.; De Jong, N.; De Nooijer, J. Current Trends in Interprofessional Shared Decision-Making Programmes in Health Professions Education: A Scoping Review. Sustainability 2022, 14, 13157. https://doi.org/10.3390/su142013157
Sultan L, Alsaywid B, De Jong N, De Nooijer J. Current Trends in Interprofessional Shared Decision-Making Programmes in Health Professions Education: A Scoping Review. Sustainability. 2022; 14(20):13157. https://doi.org/10.3390/su142013157
Chicago/Turabian StyleSultan, Lama, Basim Alsaywid, Nynke De Jong, and Jascha De Nooijer. 2022. "Current Trends in Interprofessional Shared Decision-Making Programmes in Health Professions Education: A Scoping Review" Sustainability 14, no. 20: 13157. https://doi.org/10.3390/su142013157
APA StyleSultan, L., Alsaywid, B., De Jong, N., & De Nooijer, J. (2022). Current Trends in Interprofessional Shared Decision-Making Programmes in Health Professions Education: A Scoping Review. Sustainability, 14(20), 13157. https://doi.org/10.3390/su142013157