
Healthier Construction: Conceptualising Transformation of Mental Health Outcomes through an Integrated Supply Chain Model




Abstract
:1. Introduction
2. Literature Review Critique
2.1. Mental Health
2.2. Workplace Stressors
2.3. Project and Industry and Project Context
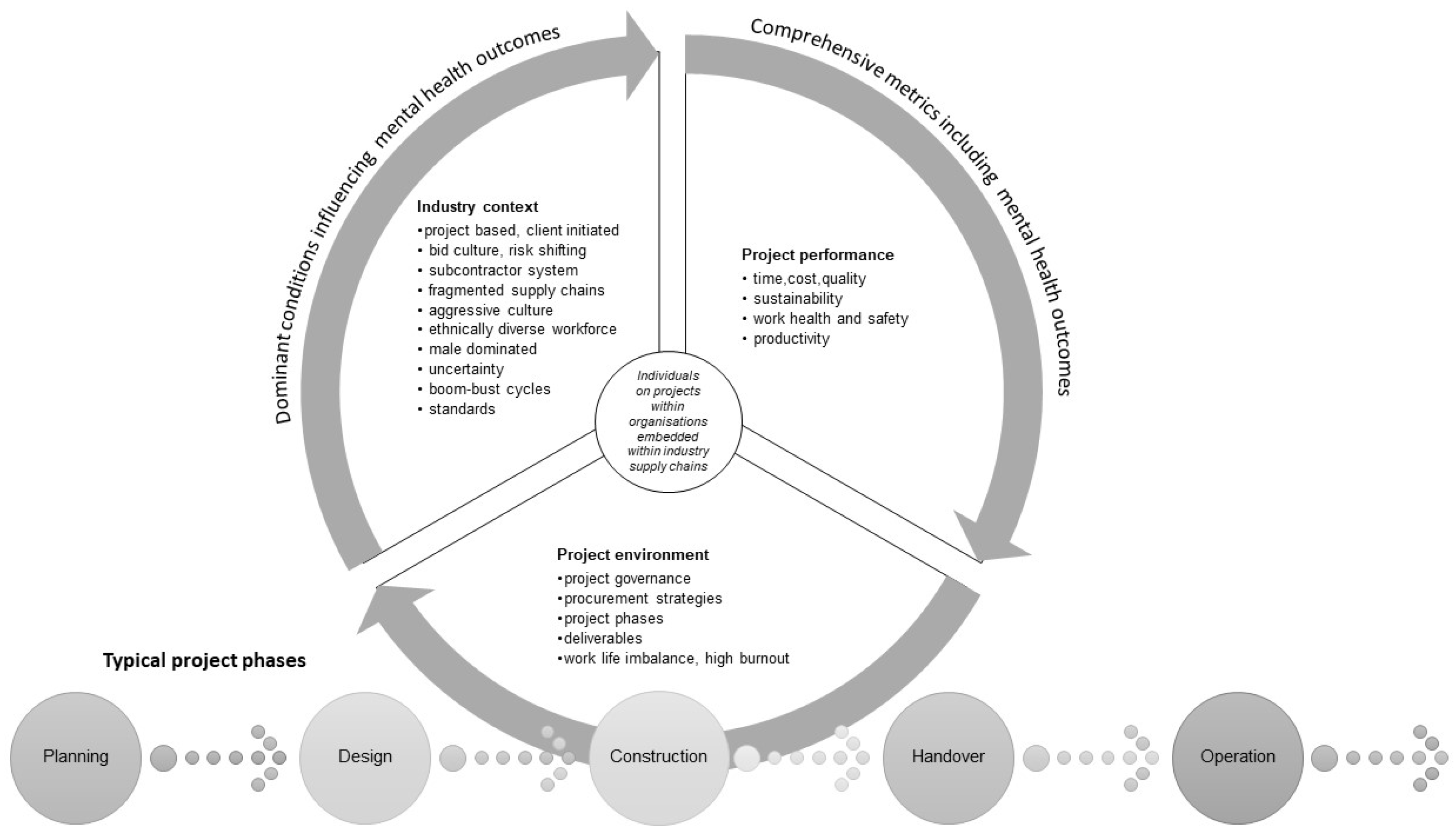
3. Conceptual Model and Discussion
4. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Pradhan, P.; Costa, L.; Rybski, D.; Lucht, W.; Kropp, J.P. A Systematic Study of Sustainable Development Goal (SDG) Interactions. Earth’s Future 2017, 5, 1169–1179. [Google Scholar] [CrossRef] [Green Version]
- Costanza, R.; Fioramonti, L.; Kubiszewski, I. The UN Sustainable Development Goals and the Dynamics of Well-Being. Front. Ecol. Environ. 2016, 14, 59. [Google Scholar] [CrossRef] [Green Version]
- Scharlemann, J.P.W.; Brock, R.C.; Balfour, N.; Brown, C.; Burgess, N.D.; Guth, M.K.; Ingram, D.J.; Lane, R.; Martin, J.G.C.; Wicander, S.; et al. Towards Understanding Interactions between Sustainable Development Goals: The Role of Environment-Human Linkages. Sustain. Sci. 2020, 15, 1573–1584. [Google Scholar] [CrossRef] [Green Version]
- Sompolska-Rzechuła, A.; Kurdyś-Kujawska, A. Towards Understanding Interactions between Sustainable Development Goals: The Role of Climate-Well-Being Linkages. Experiences of EU Countries. Energies 2021, 14, 2025. [Google Scholar] [CrossRef]
- Campbell, B.M.; Hansen, J.; Rioux, J.; Stirling, C.M.; Twomlow, S.; Wollenberg, E. Urgent Action to Combat Climate Change and Its Impacts (SDG 13): Transforming Agriculture and Food Systems. Curr. Opin. Environ. Sustain. 2018, 34, 13–20. [Google Scholar] [CrossRef]
- Ortiz, A.M.D.; Outhwaite, C.L.; Dalin, C.; Newbold, T. A Review of the Interactions between Biodiversity, Agriculture, Climate Change, and International Trade: Research and Policy Priorities. One Earth 2021, 4, 88–101. [Google Scholar] [CrossRef]
- Nunes, A.R.; Lee, K.; O’Riordan, T. The Importance of an Integrating Framework for Achieving the Sustainable Development Goals: The Example of Health and Well-Being. BMJ Glob. Health 2016, 1, e000068. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dybdahl, R.; Lien, L. Mental Health Is an Integral Part of the Sustainable Development Goals. Prev. Med. Community Health 2018, 1. [Google Scholar] [CrossRef] [Green Version]
- Yip, P.S.F.; Zheng, Y.; Wong, C. Demographic and Epidemiological Decomposition Analysis of Global Changes in Suicide Rates and Numbers over the Period 1990–2019. Inj. Prev. 2021, 28, 117–124. [Google Scholar] [CrossRef]
- Naghavi, M. Global, Regional, and National Burden of Suicide Mortality 1990 to 2016: Systematic Analysis for the Global Burden of Disease Study 2016. BMJ 2019, 364, l94. [Google Scholar] [CrossRef] [Green Version]
- Jones, P.B. Adult Mental Health Disorders and Their Age at Onset. Br. J. Psychiatry 2013, 202, s5–s10. [Google Scholar] [CrossRef] [PubMed]
- Vigo, D.; Thornicroft, G.; Atun, R. Estimating the True Global Burden of Mental Illness. Lancet Psychiatry 2016, 3, 171–178. [Google Scholar] [CrossRef] [Green Version]
- Patel, V.; Saxena, S.; Frankish, H.; Boyce, N. Sustainable Development and Global Mental Health—A Lancet Commission. Lancet 2016, 387, 1143–1145. [Google Scholar] [CrossRef] [Green Version]
- Doran, C.M.; Kinchin, I. A Review of the Economic Impact of Mental Illness. Aust. Health Rev. 2019, 43, 43–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chernyak-Hai, L.; Rabenu, E. The New Era Workplace Relationships: Is Social Exchange Theory Still Relevant? Ind. Organ. Psychol. 2018, 11, 456–481. [Google Scholar] [CrossRef] [Green Version]
- Stepanek, M.; Jahanshahi, K.; Millard, F. Individual, Workplace, and Combined Effects Modeling of Employee Productivity Loss. J. Occup. Environ. 2019, 61, 469–478. [Google Scholar] [CrossRef] [PubMed]
- Nikmehr, B.; Hosseini, M.R.; Martek, I.; Zavadskas, E.K.; Antucheviciene, J. Digitalization as a Strategic Means of Achieving Sustainable Efficiencies in Construction Management: A Critical Review. Sustainability 2021, 13, 5040. [Google Scholar] [CrossRef]
- Goubran, S. On the Role of Construction in Achieving the SDGs. J. Sustain. Res. 2019, 1, e190020. [Google Scholar] [CrossRef]
- Fei, W.; Opoku, A.; Agyekum, K.; Oppon, J.A.; Ahmed, V.; Chen, C.; Lok, K.L. The Critical Role of the Construction Industry in Achieving the Sustainable Development Goals (SDGs): Delivering Projects for the Common Good. Sustainability 2021, 13, 9112. [Google Scholar] [CrossRef]
- Opoku, D.-G.J.; Perera, S.; Osei-Kyei, R.; Rashidi, M. Digital Twin Application in the Construction Industry: A Literature Review. J. Build. Eng. 2021, 40, 102726. [Google Scholar] [CrossRef]
- Neis, B.; Neil, K. Mental Health in the Construction Industry: An Interview with Australia’s MATES in Construction CEO, Jorgen Gullestrup. Labour Ind. A J. Soc. Econ. Relat. Work 2020, 30, 413–429. [Google Scholar] [CrossRef]
- MATES—Industry Based Suicide Prevention. Available online: http://mates.org.au (accessed on 22 May 2022).
- The Australian Building and Construction Industry. Available online: https://www.constructionblueprint.com.au/wp-content/uploads/Blueprint-for-Better-Mental-Health-Report.pdf (accessed on 22 May 2022).
- The Cost of Doing Nothing Report or to View More Information about the Draft Culture Standard. Available online: www.cultureconstruction.com.au.2022 (accessed on 22 May 2022).
- Sun, C.; Hon, C.K.H.; Way, K.A.; Jimmieson, N.L.; Xia, B. The Relationship between Psychosocial Hazards and Mental Health in the Construction Industry: A Meta-Analysis. Saf. Sci. 2022, 145, 105485. [Google Scholar] [CrossRef]
- Lingard, H.; Turner, M.; Charlesworth, S. Growing Pains: Work-Life Impacts in Small-To-Medium Sized Construction Firms. Eng. Constr. Archit. Manag. 2015, 22, 312–326. [Google Scholar] [CrossRef] [Green Version]
- Turner, M.; Lingard, H. Examining the Interaction between Bodily Pain and Mental Health of Construction Workers. Constr. Manag. Econ. 2020, 38, 1009–1023. [Google Scholar] [CrossRef]
- Tijani, B.; Nwaeze, J.F.; Jin, X.; Osei-Kyei, R. Suicide in the Construction Industry: Literature Review. Int. J. Constr. Manag. 2021; in press. [Google Scholar] [CrossRef]
- Martin, G.; Swannell, S.; Milner, A. Mates in Construction Suicide Prevention Program: A Five-Year Review. J. Community Med. Health Educ. 2016, 6, 2161–2711. [Google Scholar] [CrossRef] [Green Version]
- Milner, A.; Niven, H.; LaMontagne, A. Suicide by Occupational Skill Level in the Australian Construction Industry: Data from 2001 to 2010. Aust. N. Z. J. Public Health 2014, 38, 281–285. [Google Scholar] [CrossRef] [PubMed]
- Langdon, R.R.; Sawang, S. Construction Workers’ Well-Being: What Leads to Depression, Anxiety, and Stress? J. Constr. Eng. Manag. 2018, 144, 04017100. [Google Scholar] [CrossRef] [Green Version]
- King, T.L.; Batterham, P.J.; Lingard, H.; Gullestrup, J.; Lockwood, C.; Harvey, S.B.; Kelly, B.; LaMontagne, A.D.; Milner, A. Are Young Men Getting the Message? Age Differences in Suicide Prevention Literacy among Male Construction Workers. Int. J. Environ. Res. Public Health 2019, 16, 475. [Google Scholar] [CrossRef] [Green Version]
- Eyllon, M.; Vallas, S.P.; Dennerlein, J.T.; Garverich, S.; Weinstein, D.; Owens, K.; Lincoln, A.K. Mental Health Stigma and Wellbeing among Commercial Construction Workers: A Mixed Methods Study. J. Occup. Environ. Med. 2020, 62, e423. [Google Scholar] [CrossRef]
- Battams, S.; Roche, A.M.; Fischer, J.A.; Lee, N.K.; Cameron, J.; Kostadinov, V. Workplace Risk Factors for Anxiety and Depression in Male-Dominated Industries: A Systematic Review. Health Psychol. Behav. Med. 2014, 2, 983–1008. [Google Scholar] [CrossRef]
- Chapman, J.; Roche, A.M.; Duraisingam, V.; Ledner, B.; Finnane, J.; Pidd, K. Exploring the Relationship between Psychological Distress and Likelihood of Help Seeking in Construction Workers: The Role of Talking to Workmates and Knowing How to Get Help. Work 2020, 67, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Holden, S.; Sunindijo, R.Y. Technology, Long Work Hours, and Stress Worsen Work-Life Balance in the Construction Industry. Int. J. Integr. Eng. 2018, 10, 13–18. [Google Scholar] [CrossRef]
- Chan, A.P.C.; Nwaogu, J.M.; Naslund, J.A. Mental Ill-Health Risk Factors in the Construction Industry: Systematic Review. J. Constr. Eng. Manag. 2020, 146, 04020004. [Google Scholar] [CrossRef]
- Tijani, B.; Jin, X.; Osei-kyei, R. A Systematic Review of Mental Stressors in the Construction Industry. Int. J. Build. Pathol. 2020, 39, 433–460. [Google Scholar] [CrossRef]
- Tijani, B.; Osei-Kyei, R.; Feng, Y. A Review of Work-Life Balance in the Construction Industry. Int. J. Constr. Manag. 2020. [Google Scholar] [CrossRef]
- Tijani, B.; Xiaohua, J.; Osei-Kyei, R. Critical Analysis of Mental Health Research among Construction Project Professionals. J. Eng. Des. Technol. 2020, 19, 467–496. [Google Scholar] [CrossRef]
- Sundquist, V.; Gadde, L.-E.; Hulthén, K. Reorganizing Construction Logistics for Improved Performance. J. Constr. Manag. Econ. 2017, 36, 49–65. [Google Scholar] [CrossRef]
- London, K. Construction and Supply Chain Economics; Routledge: London, UK, 2014. [Google Scholar]

{kind=link}
| INDUSTRY CONTEXT: Dominant Structural and Behavioural Characteristics of a Project-Based Sector | CATALYSTS: Dominant Timeframe and Actions Effectively Impact Systemic Change | FUTURE STATE: Directions for Policy and Practice Influencers | PERFORMANCE: Initial and Future State Measures of Likely Systemic Failure |
|---|---|---|---|
| Multi Project Supply Chain Environment | |||
| High workloads | Planning Phase: Initial starting conditions of projects for each firm | Development of tools to monitor Development of benchmarking databases | Project and organisational capacity to deliver Monitoring of project multiplicity |
| Industry structural conditions of project bid and work uncertainty exacerbating job insecurity | Pre-planning Phase: Annual development of pipeline presented to industry by major private and public sector clients | National database of projects mapped to mental health metrics (absences, productivity, hours worked) | Volume of projects across a sector in a region |
| Uncertain economic environment resulting in poor decision making on project true cost resulting in multiple projects that are economically unviable exerting pressure on firms’ staff & supply chains | Pre-construction and tendering phase | Analysis of case studies of low bids and poor mental health outcomes | Establish comparison between poor health outcomes through metrics and relate to costs projected in tenders |
| Uncertain economic environment may lead to bankruptcies resulting in redundancies | Tendering: Bid analysis by clients. Project completion: post construction & handover cross project assessments and performance evaluations of key supply chain actors | Analysis of case studies of bankrupt companies and impact on poor mental health outcomes | At the firm level significant numbers of project submissions with highly significant reduced fee/tender value in comparison to market bidders |
| Emerging significant infrastructure workload as a peak arising from COVID pandemic as governments seek to re-energise the economy | Pre-planning Phase: Annual development of pipeline presented to industry by major private and public sector clients | Inter-state comparison of workload and workforce capacity | State by state analysis of workforce capacity |
| Construction Project Supply Chain Organisational Environment Level | |||
| Project specific demands with peaks and troughs of pressure points within strict budget and quality regimes | All project phases | Recommendations on project portfolio planning and management and scheduling supported by case study evidence | Examples of system capacity |
| Project specific contracts with high performance metrics of timely completions | Planning and Tendering | Guidance on various national and international approaches to limits and ranges to project timeframes | Metrics on limits and ranges to project timeframes within Australian context |
| Cascading pressure down fragmented subcontract contractual supply chain | Tendering, Interim Milestones Handover and Completion | Project by project benchmarking on construction supply chain workforce cohesiveness and capacity to deliver on project | Integration supply chain metric |
| Organisations balancing multiple projects simultaneously with competing work deadlines | New bids (design and construction) and periodic monitoring | Recommendations on project portfolio planning and management and scheduling supported by case study evidence | Examples of system capacity |
| Government as a significant influencer as a client through procurement of major public sector infrastructure projects | Design and Construction pre-bid and tendering | Case studies of best practice in relation to procurement directions aligned to mental health outcomes across entire client portfolio of capital works | Inter-state metrics and benchmarking on public sector performance in relation to mental health outcomes related back to procurement methods |
| Construction Supply Chain Procurement Environment | |||
| ‘Silence’ in tendering criteria of psychological work health and safety outcomes | Design and Construction pre- bid and tendering | Best practice examples of procurement and tendering directions aligned to mental health outcomes | Examples of project tendering metrics |
| Frequent changing work specifications during all phases of the project to meet uncertain and complex project conditions | Design and Construction reporting and monitoring | Guidelines on impact of decision-making flow on effect including quantitative and qualitative evidence | Metrics on change work orders and stress impact on workforce to deliver |
| Lack of leadership with incentives for workplace well-being and a ‘complete the job’ at all cost mentality | All phases but particularly project delivery milestones | Guidance for senior/middle management supervisors of project directors/managers within consultancies/contracting companies | Leadership performance indicators inclusive of project and staff mental health outcomes |
| Extensive long work hours during the work week with little downtime | Design and construction phases exacerbated at organisational milestone delivery submission times | Case studies of projects with varying work hours aligned to productivity analysis | Recommendations for companies and clients on feasibility of reduced working week and associated impacts on completion time and costs |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
London, K.A.; Meade, T.; McLachlan, C. Healthier Construction: Conceptualising Transformation of Mental Health Outcomes through an Integrated Supply Chain Model. Sustainability 2022, 14, 9460. https://doi.org/10.3390/su14159460
London KA, Meade T, McLachlan C. Healthier Construction: Conceptualising Transformation of Mental Health Outcomes through an Integrated Supply Chain Model. Sustainability. 2022; 14(15):9460. https://doi.org/10.3390/su14159460
Chicago/Turabian StyleLondon, Kerry Anne, Tanya Meade, and Craig McLachlan. 2022. "Healthier Construction: Conceptualising Transformation of Mental Health Outcomes through an Integrated Supply Chain Model" Sustainability 14, no. 15: 9460. https://doi.org/10.3390/su14159460
APA StyleLondon, K. A., Meade, T., & McLachlan, C. (2022). Healthier Construction: Conceptualising Transformation of Mental Health Outcomes through an Integrated Supply Chain Model. Sustainability, 14(15), 9460. https://doi.org/10.3390/su14159460