
Longitudinal Associations of Children’s Hyperactivity/Inattention, Peer Relationship Problems and Mobile Device Use


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Materials
2.2.1. Digital Kids Questionnaire
2.2.2. Strength and Difficulties Questionnaire
2.3. Procedure
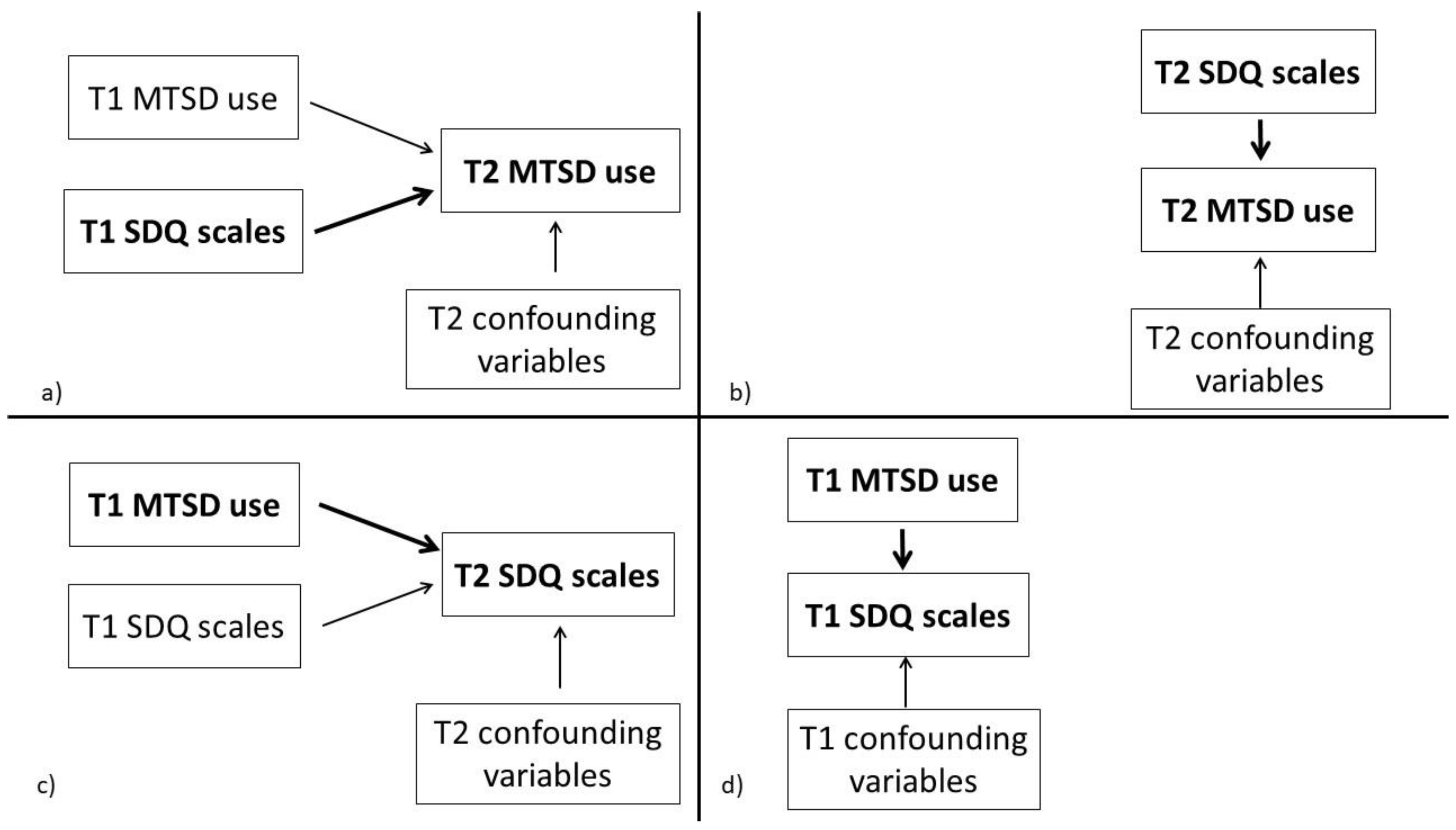
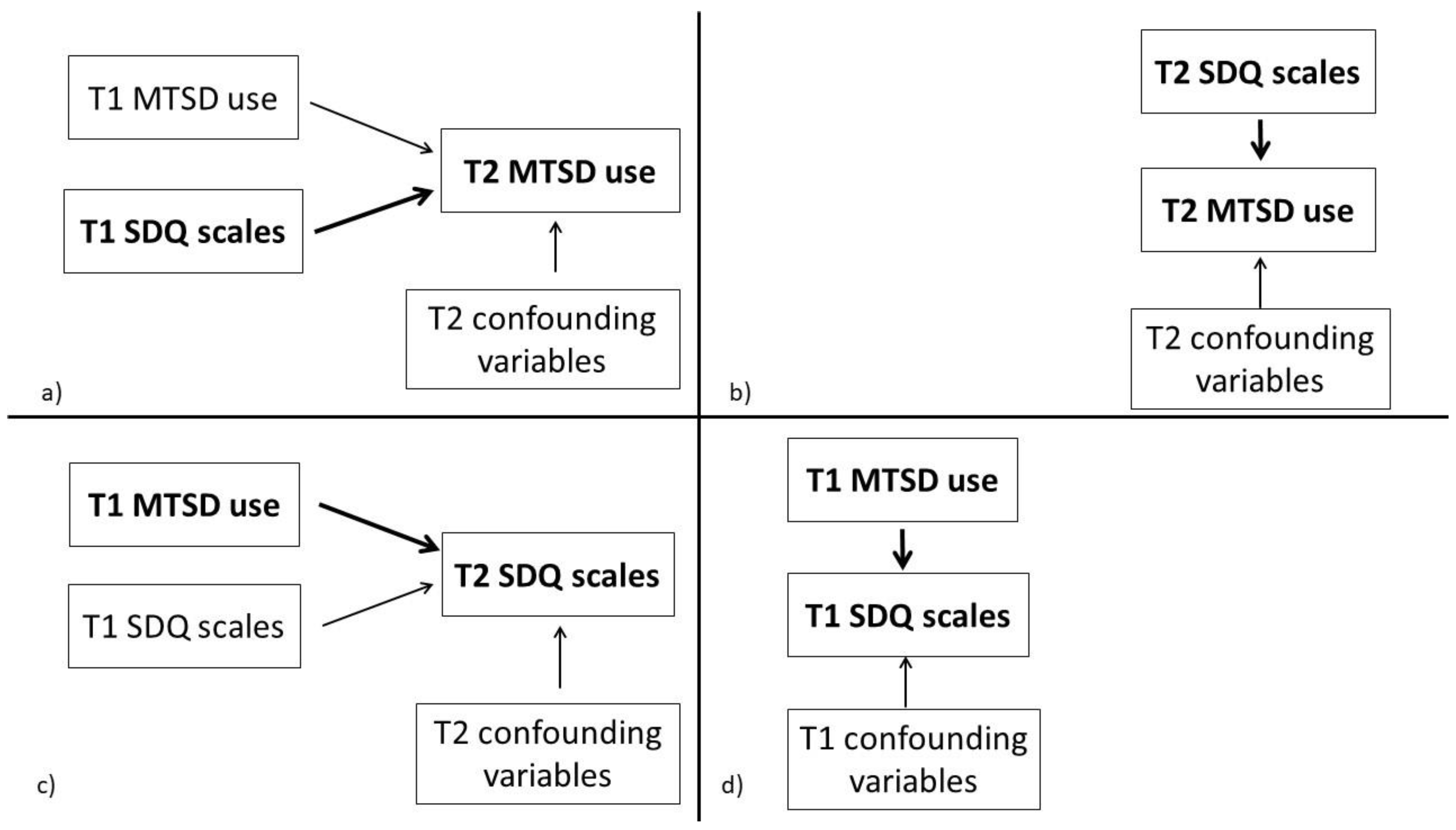
2.4. Statistical Analysis
3. Results
3.1. Comparison of the Dropout and Retested Participants
3.2. T2 MTSD Use and T1 Behaviour Problems
3.3. T2 MTSD Use and T2 Behaviour Problems
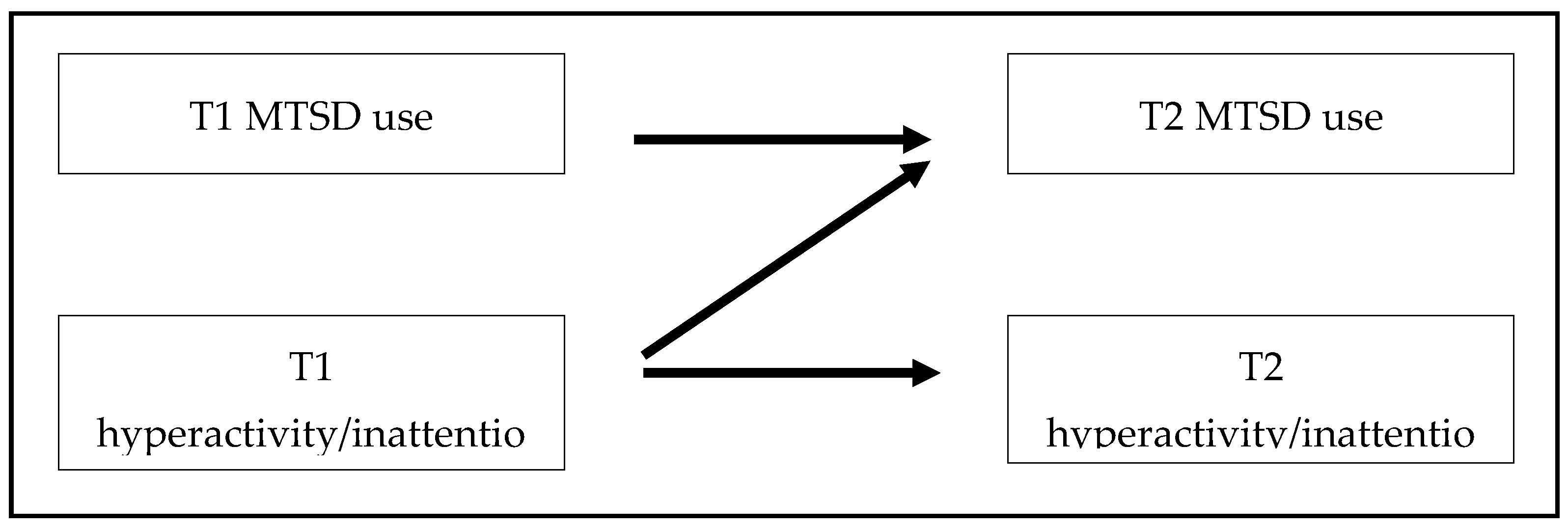
3.4. T1 MTSD Use and T2 Behaviour Problems
3.5. T1 MTSD Use and T1 Behaviour Problems
3.6. Change in SDQ Scores and MTSD Use over Time
4. Discussion
4.1. Higher Hyperactivity/Inattention Leads to Higher MTSD Use
4.2. Higher MTSD Use Does Not Lead to Higher Hyperactivity/Inattention
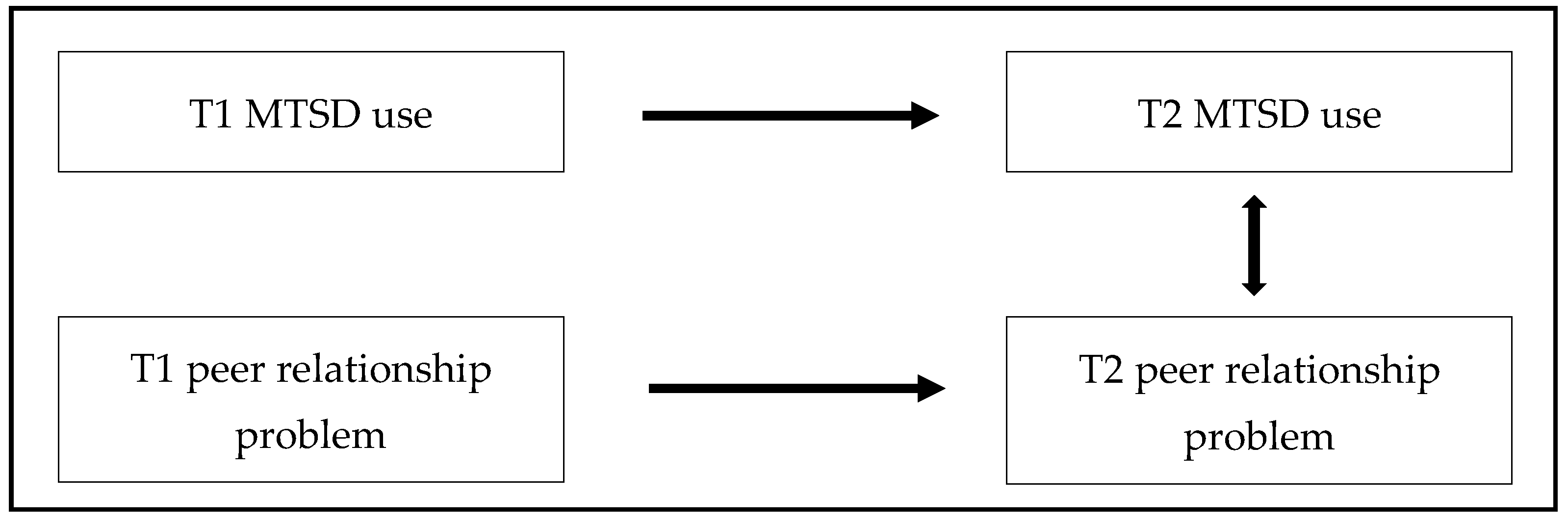
4.3. Association between Concurrent Peer Relationship Problems and MTSD Use in Early School Years
4.4. Other SDQ Scales and MTSD Use
4.5. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Digital Kids Questionnaire (Short Form)
- Q1. Your age:
- Q2. Your gender:
- Man
- Woman
- Q3. Your highest level of education:
- Elementary school
- Technical school
- High school
- College BA Bs(c)
- University MA MS(c)
- Postgraduate PhD
- Q4. Child’s date of birth:
- Q5. Child’s gender:
- Boy
- Girl
- Q6. Number of siblings: ____
- Q7. Husband’s partner’s highest level of education:
- Elementary school
- Technical school
- High school
- College BA Bs(c)
- University MA MS(c)
- Postgraduate PhD
- Q8. With regard to your knowledge, which statement is true about your child’s relationship with the smartphone?
- Has never seen or held a smartphone in his/her hand
- Has never held a smartphone in his/her hand, but has seen one
- Has already held/used a smartphone, but only on a few occasions
- Uses/holds a smartphone in his/her hand regularly (but does not have his/her own)
- Has his/her own smartphone (which he/she regularly uses)
- Q9. How frequently does he/she use a smartphone?
- Several times daily
- Daily
- Every 2–3 days
- Every 4–5 days
- Weekly
- Every 2–3 weeks
- Monthly
- Less often than monthly
- Q10. When he/she uses smartphone, how long does he/she typically use it for?
- More than 3 h
- 2–3 h
- 1–2 h
- 30–60 min
- 10–30 min
- 5–10 min
- A few min (5 min maximum)
- Q11. With regard to your knowledge, which statement is true about your child’s relationship with the tablet?
- Has never seen or held a tablet in his/her hand
- Has never held a tablet in his/her hand, but has seen one
- Has already held/used a tablet, but only on a few occasions
- Uses/holds a tablet in his/her hand regularly (but does not have his/her own)
- Has his/her own tablet (which he/she regularly uses)
- Q12. How frequently does he/she use a tablet?
- Several times daily
- Daily
- Every 2–3 days
- Every 4–5 days
- Weekly
- Every 2–3 weeks
- Monthly
- Less often than monthly
- Q13. When he/she uses tablet, how long does he/she typically use it for?
- More than 3 h
- 2–3 h
- 1–2 h
- 30–60 min
- 10–30 min
- 5–10 min
- A few min (5 min maximum)
- Q14. Please rate the following statements according to how much they describe you. (not at all characteristic–––absolutely characteristic)
- If I feel uneasy/tense in company, I take out my phone.
- I am nervous/tense when I leave my phone at home.
- If my phone is in my hand, I feel more confident.
- If I do not have my phone on me, I do not feel safe.
References
- Green, C.S.; Bavelier, D. Exercising your brain: A review of human brain plasticity and training-induced learning. Psychol. Aging 2008, 23, 692–701. [Google Scholar] [CrossRef] [Green Version]
- Tromholt, M. The Facebook Experiment: Quitting Facebook Leads to Higher Levels of Well-Being. Cyberpsychol. Behav. Soc. Netw. 2016, 19, 661–666. [Google Scholar] [CrossRef]
- Hubel, D.H.; Wiesel, T.N. Shape and arrangement of columns in cat’s striate cortex. J. Physiol. 1963, 165, 559–568. [Google Scholar] [CrossRef] [Green Version]
- Schoenmaker, C.; Juffer, F.; van Ijzendoorn, M.H.; Dries, L.V.D.; Linting, M.; van der Voort, A.; Bakermans-Kranenburg, M.J. Cognitive and health-related outcomes after exposure to early malnutrition: The Leiden longitudinal study of international adoptees. Child. Youth Serv. Rev. 2015, 48, 80–86. [Google Scholar] [CrossRef]
- Konok, V.; Bunford, N.; Miklósi, Á. Associations between child mobile use and digital parenting style in Hungarian families. J. Child. Media 2020, 14, 91–109. [Google Scholar] [CrossRef]
- Rideout, V. The Common Sense Census: Media Use by Kids Age Zero to Eight; Common Sense Media: San Francisco, CA, USA, 2017. [Google Scholar]
- Kabali, H.K.; Irigoyen, M.M.; Nunez-Davis, R.; Budacki, J.G.; Mohanty, S.H.; Leister, K.P.; Bonner, R.L., Jr. Exposure and use of mobile media devices by young children. Pediatrics 2015, 136, 1044–1050. [Google Scholar] [CrossRef] [Green Version]
- Connell, S.L.; Lauricella, A.R.; Wartella, E. Parental co-use of media technology with their young children in the USA. J. Child. Media 2015, 9, 5–21. [Google Scholar] [CrossRef]
- Rocha, B.; Nunes, C. Benefits and damages of the use of touchscreen devices for the development and behavior of children under 5 years old—A systematic review. Psicol. Reflex. Crítica 2020, 33, 24. [Google Scholar] [CrossRef]
- Odgers, C.L.; Jensen, M.R. Annual research review: Adolescent mental health in the digital age: Facts, fears, and future directions. J. Child Psychol. Psychiatry 2020, 61, 336–348. [Google Scholar] [CrossRef]
- Beyens, I.; Valkenburg, P.M.; Piotrowski, J.T. Screen media use and ADHD-related behaviors: Four decades of research. Proc. Natl. Acad. Sci. USA 2018, 115, 9875–9881. [Google Scholar] [CrossRef] [Green Version]
- LeBlanc, A.G.; Spence, J.C.; Carson, V.; Gorber, S.C.; Dillman, C.; Janssen, I.; Kho, M.E.; Stearns, J.A.; Timmons, B.W.; Tremblay, M.S. Systematic review of sedentary behaviour and health indicators in the early years (aged 0–4 years). Appl. Physiol. Nutr. Metab. 2012, 37, 753–772. [Google Scholar] [CrossRef] [Green Version]
- Stiglic, N.; Viner, R.M. Effects of screentime on the health and well-being of children and adolescents: A systematic review of reviews. BMJ Open 2019, 9, e023191. [Google Scholar] [CrossRef] [Green Version]
- Suchert, V.; Hanewinkel, R.; Isensee, B. Sedentary behavior and indicators of mental health in school-aged children and adolescents: A systematic review. Prev. Med. 2015, 76, 48–57. [Google Scholar] [CrossRef]
- Tremblay, M.S.; LeBlanc, A.G.; Kho, M.E.; Saunders, T.J.; Larouche, R.; Colley, R.C.; Goldfield, G.; Gorber, S.C. Systematic review of sedentary behaviour and health indicators in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 98. [Google Scholar] [CrossRef] [Green Version]
- Boneberger, A.; Bolte, G.; von Kries, R.; GME-Studiengruppe, N.F.D. Exzessiver Medienkonsum und Verhaltensauffälligkeiten–eine Querschnittstudie bei Vorschulkindern. Gesundheitswesen 2011, 73, 280–285. [Google Scholar] [CrossRef]
- Pagani, L.S.; Fitzpatrick, C.; Barnett, T.A.; Dubow, E. Prospective Associations between Early Childhood Television Exposure and Academic, Psychosocial, and Physical Well-being by Middle Childhood. Arch. Pediatr. Adolesc. Med. 2010, 164, 425–431. [Google Scholar] [CrossRef] [Green Version]
- Zimmerman, F.J.; Glew, G.M.; Christakis, D.A.; Katon, W. Early Cognitive Stimulation, Emotional Support, and Television Watching as Predictors of Subsequent Bullying among Grade-School Children. Arch. Pediatr. Adolesc. Med. 2005, 159, 384–388. [Google Scholar] [CrossRef]
- Zimmerman, F.J.; Christakis, D.A. Associations between Content Types of Early Media Exposure and Subsequent Attentional Problems. Pediatrics 2007, 120, 986–992. [Google Scholar] [CrossRef] [Green Version]
- Tamana, S.K.; Ezeugwu, V.; Chikuma, J.; Lefebvre, D.L.; Azad, M.B.; Moraes, T.J.; Subbarao, P.; Becker, A.B.; Turvey, S.E.; Sears, M.R.; et al. Screen-time is associated with inattention problems in preschoolers: Results from the CHILD birth cohort study. PLoS ONE 2019, 14, e0213995. [Google Scholar] [CrossRef]
- Homer, B.D.; Plass, J.L.; Raffaele, C.; Ober, T.M.; Ali, A. Improving high school students’ executive functions through digital game play. Comput. Educ. 2018, 117, 50–58. [Google Scholar] [CrossRef]
- Rasmussen, E.E.; Strouse, G.; Colwell, M.J.; Johnson, C.R.; Holiday, S.; Brady, K.; Flores, I.; Troseth, G.; Wright, H.D.; Densley, R.L.; et al. Promoting Preschoolers’ Emotional Competence through Prosocial TV and Mobile App Use. Media Psychol. 2019, 22, 1–22. [Google Scholar] [CrossRef]
- Gentile, D.A.; Swing, E.L.; Lim, C.G.; Khoo, A. Video game playing, attention problems, and impulsiveness: Evidence of bidirectional causality. Psychol. PoMedia Cult. 2012, 1, 62–70. [Google Scholar] [CrossRef] [Green Version]
- Cliff, D.P.; Howard, S.J.; Radesky, J.S.; McNeill, J.; Vella, S.A. Early Childhood Media Exposure and Self-Regulation: Bidirectional Longitudinal Associations. Acad. Pediatr. 2018, 18, 813–819. [Google Scholar] [CrossRef] [Green Version]
- McHarg, G.; Ribner, A.D.; Devine, R.T.; Hughes, C. Screen time and executive function in toddlerhood: A longitudinal study. Front. Psychol. 2020, 11, 2846. [Google Scholar] [CrossRef]
- McHarg, G.; Ribner, A.D.; Devine, R.T.; Hughes, C.; NewFAMS Study Team. Infant screen exposure links to toddlers’ inhibition, but not other EF constructs: A propensity score study. Infancy 2020, 25, 205–222. [Google Scholar] [CrossRef] [Green Version]
- McNeill, J.; Howard, S.J.; Vella, S.A.; Cliff, D.P. Longitudinal Associations of Electronic Application Use and Media Program Viewing with Cognitive and Psychosocial Development in Preschoolers. Acad. Pediatr. 2019, 19, 520–528. [Google Scholar] [CrossRef]
- Poulain, T.; Vogel, M.; Neef, M.; Abicht, F.; Hilbert, A.; Genuneit, J.; Körner, A.; Kiess, W. Reciprocal associations between electronic media use and behavioral difficulties in preschoolers. Int. J. Environ. Res. Public. Health 2018, 15, 814. [Google Scholar] [CrossRef] [Green Version]
- Swing, E.L.; Gentile, D.A.; Anderson, C.A.; Walsh, D.A. Television and Video Game Exposure and the Development of Attention Problems. Pediatrics 2010, 126, 214–221. [Google Scholar] [CrossRef] [Green Version]
- Hinkley, T.; Verbestel, V.; Ahrens, W.; Lissner, L.; Molnar, D.; Moreno, L.A.; Pigeot, I.; Pohlabeln, H.; Reisch, L.; Russo, P.; et al. Early Childhood Electronic Media Use as a Predictor of Poorer Well-being: A Prospective Cohort Study. JAMA Pediatr. 2014, 168, 485. [Google Scholar] [CrossRef]
- Lobel, A.; Engels, R.; Stone, L.L.; Burk, W.J.; Granic, I. Video Gaming and Children’s Psychosocial Wellbeing: A Longitudinal Study. J. Youth Adolesc. 2017, 46, 884–897. [Google Scholar] [CrossRef] [Green Version]
- Hinkley, T.; Timperio, A.; Salmon, J.; Hesketh, K. Does Preschool Physical Activity and Electronic Media Use Predict Later Social and Emotional Skills at 6 to 8 Years? A Cohort Study. J. Phys. Act. Health 2017, 14, 308–316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Konok, V.; Liszkai-Peres, K.; Bunford, N.; Ferdinandy, B.; Jurányi, Z.; Ujfalussy, D.J.; Réti, Z.; Pogány, Á.; Kampis, G.; Miklósi, Á. Mobile use induces local attentional precedence and is associated with limited socio-cognitive skills in preschoolers. Comput. Hum. Behav. 2021, 120, 106758. [Google Scholar] [CrossRef]
- Christakis, D.A.; Ramirez, J.S.B.; Ferguson, S.M.; Ravinder, S.; Ramirez, J.-M. How early media exposure may affect cognitive function: A review of results from observations in humans and experiments in mice. Proc. Natl. Acad. Sci. USA 2018, 115, 9851–9858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christakis, D.A.; Ramirez, J.S.B.; Ramirez, J.M. Overstimulation of newborn mice leads to behavioral differences and deficits in cognitive performance. Sci. Rep. 2012, 2, 546. [Google Scholar] [CrossRef] [PubMed]
- Lissak, G. Adverse physiological and psychological effects of screen time on children and adolescents: Literature review and case study. Environ. Res. 2018, 164, 149–157. [Google Scholar] [CrossRef]
- Nikkelen, S.W.C.; Valkenburg, P.M.; Huizinga, M.; Bushman, B.J. Media use and ADHD-related behaviors in children and adolescents: A meta-analysis. Dev. Psychol. 2014, 50, 2228–2241. [Google Scholar] [CrossRef]
- Jensen, P.S.; Mrazek, D.; Knapp, P.K.; Steinberg, L.; Pfeffer, C.; Schowalter, J.; Shapiro, T. Evolution and Revolution in Child Psychiatry: ADHD as a Disorder of Adaptation. J. Am. Acad. Child Adolesc. Psychiatry 1997, 36, 1672–1681. [Google Scholar] [CrossRef] [Green Version]
- Bender, P.K.; Plante, C.; Gentile, D.A. The effects of violent media content on aggression. Curr. Opin. Psychol. 2018, 19, 104–108. [Google Scholar] [CrossRef]
- Bushman, B.J.; Huesmann, L.R. Short-term and Long-term Effects of Violent Media on Aggression in Children and Adults. Arch. Pediatr. Adolesc. Med. 2006, 160, 348–352. [Google Scholar] [CrossRef] [Green Version]
- Vandewater, E.A.; Bickham, D.S.; Lee, J.H. Time Well Spent? Relating Television Use to Children’s Free-Time Activities. Pediatrics 2006, 117, e181–e191. [Google Scholar] [CrossRef] [Green Version]
- Ashiabi, G.S. Play in the preschool classroom: Its socioemotional significance and the teacher’s role in play. Early Child. Educ. J. 2007, 35, 199–207. [Google Scholar] [CrossRef]
- Ranson, K.E.; Urichuk, L.J. The effect of parent–child attachment relationships on child biopsychosocial outcomes: A review. Early Child Dev. Care 2008, 178, 129–152. [Google Scholar] [CrossRef]
- Viner, R.M.; Gireesh, A.; Stiglic, N.; Hudson, L.D.; Goddings, A.-L.; Ward, J.L.; Nicholls, D. Roles of cyberbullying, sleep, and physical activity in mediating the effects of social media use on mental health and wellbeing among young people in England: A secondary analysis of longitudinal data. Lancet Child Adolesc. Health 2019, 3, 685–696. [Google Scholar] [CrossRef]
- Mazurek, M.O.; Engelhardt, C.R. Video Game Use in Boys with Autism Spectrum Disorder, ADHD, or Typical Development. Pediatrics 2013, 132, 260–266. [Google Scholar] [CrossRef] [Green Version]
- Mazurek, M.O.; Wenstrup, C. Television, Video Game and Social Media Use among Children with ASD and Typically Developing Siblings. J. Autism Dev. Disord. 2013, 43, 1258–1271. [Google Scholar] [CrossRef]
- Demetrovics, Z.; Urbán, R.; Nagygyörgy, K.; Farkas, J.; Zilahy, D.; Mervo, B.F.; Reindl, A.; Ágoston, C.; Kertész, A.; Harmath, E. Why do you play? The development of the motives for online gaming questionnaire (MOGQ). Behav. Res. Methods 2011, 43, 814–825. [Google Scholar] [PubMed]
- Weber, S.; Mast, F.W.; Weibel, D. Experiencing Presence in a Gaming Activity Improves Mood After a Negative Mood Induction. Int. J. Gaming Comput. Simul. 2020, 12, 22. [Google Scholar] [CrossRef]
- Purper-Ouakil, D.; Cortese, S.; Wohl, M.; Aubron, V.; Orejarena, S.; Michel, G.; Asch, M.; Mouren, M.-C.; Gorwood, P. Temperament and character dimensions associated with clinical characteristics and treatment outcome in attention-deficit/hyperactivity disorder boys. Compr. Psychiatry 2010, 51, 286–292. [Google Scholar] [CrossRef]
- Wang, P.; Lei, L.; Wang, X.; Nie, J.; Chu, X.; Jin, S. The exacerbating role of perceived social support and the ‘buffering’ role of depression in the relation between sensation seeking and adolescent smartphone addiction. Personal. Individ. Differ. 2018, 130, 129–134. [Google Scholar] [CrossRef]
- Konok, V.; Gigler, D.; Bereczky, B.M.; Miklósi, Á. Humans’ attachment to their mobile phones and its relationship with interpersonal attachment style. Comput. Hum. Behav. 2016, 61, 537–547. [Google Scholar] [CrossRef]
- Selfhout, M.H.W.; Branje, S.J.T.; Delsing, M.; Bogt, T.F.M.t.; Meeus, W.H.J. Different types of Internet use, depression, and social anxiety: The role of perceived friendship quality. J. Adolesc. 2009, 32, 819–833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Radesky, J.S.; Peacock-Chambers, E.; Zuckerman, B.; Silverstein, M. Use of Mobile Technology to Calm Upset Children: Associations with Social-Emotional Development. JAMA Pediatr. 2016, 170, 397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirkorian, H.L. When and how do interactive digital media help children connect what they see on and off the screen? Child Dev. Perspect. 2018, 12, 210–214. [Google Scholar] [CrossRef]
- Radesky, J.; Miller, A.L.; Rosenblum, K.L.; Appugliese, D.; Kaciroti, N.; Lumeng, J.C. Maternal Mobile Device Use during a Structured Parent–Child Interaction Task. Acad. Pediatr. 2015, 15, 238–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hosokawa, R.; Katsura, T. Association between mobile technology use and child adjustment in early elementary school age. PLoS ONE 2018, 13, e0199959. [Google Scholar] [CrossRef]
- Schneider, H.; Eisenberg, D. Who receives a diagnosis of attention-deficit/hyperactivity disorder in the United States elementary school population? Pediatrics 2006, 117, e601–e609. [Google Scholar] [CrossRef] [Green Version]
- Ofcom, U. Children and Parents: Media Use and Attitudes Report 2018; Ofcom Website: London, UK, 2019. [Google Scholar]
- Elo, S.; Kyngäs, H. The qualitative content analysis process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef]
- Konok, V.; Pogány, Á.; Miklósi, Á. Mobile attachment: Separation from the mobile phone induces physiological and behavioural stress and attentional bias to separation-related stimuli. Comput. Hum. Behav. 2017, 71, 228–239. [Google Scholar] [CrossRef]
- Turi, E.; Tóth, I.; Gervai, J. Further examination of the Strengths and Difficulties Questionnaire (SDQ-Magy) in a community sample of young adolescents. Psychiatr. Hung. 2011, 26, 415–426. [Google Scholar]
- Goodman, R. Psychometric Properties of the Strengths and Difficulties Questionnaire. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 1337–1345. [Google Scholar] [CrossRef]
- Giannakopoulos, G.; Tzavara, C.; Dimitrakaki, C.; Kolaitis, G.; Rotsika, V.; Tountas, Y. The factor structure of the Strengths and Difficulties Questionnaire (SDQ) in Greek adolescents. Ann. Gen. Psychiatry 2009, 8, 20. [Google Scholar] [CrossRef] [Green Version]
- Maurice-Stam, H.; Haverman, L.; Splinter, A.; van Oers, H.A.; Schepers, S.A.; Grootenhuis, M.A. Dutch norms for the Strengths and Difficulties Questionnaire (SDQ)–parent form for children aged 2–18 years. Health Qual. Life Outcomes 2018, 16, 123. [Google Scholar] [CrossRef] [Green Version]
- Riso, D.D.; Salcuni, S.; Chessa, D.; Raudino, A.; Lis, A.; Altoè, G. The Strengths and Difficulties Questionnaire (SDQ). Early evidence of its reliability and validity in a community sample of Italian children. Personal. Individ. Differ. 2010, 49, 570–575. [Google Scholar] [CrossRef]
- Bunford, N.; Evans, S.W.; Langberg, J.M. Emotion Dysregulation Is Associated with Social Impairment among Young Adolescents with ADHD. J. Atten. Disord. 2018, 22, 66–82. [Google Scholar] [CrossRef]
- Graziano, P.A.; Garcia, A. Attention-deficit hyperactivity disorder and children’s emotion dysregulation: A meta-analysis. Clin. Psychol. Rev. 2016, 46, 106–123. [Google Scholar] [CrossRef]
- Di Blasi, M.; Giardina, A.; Giordano, C.; Coco, G.L.; Tosto, C.; Billieux, J.; Schimmenti, A. Problematic video game use as an emotional coping strategy: Evidence from a sample of MMORPG gamers. J. Behav. Addict. 2019, 8, 25–34. [Google Scholar] [CrossRef]
- Wadley, G.; Smith, W.; Koval, P.; Gross, J.J. Digital Emotion Regulation. Curr. Dir. Psychol. Sci. 2020, 29, 412–418. [Google Scholar] [CrossRef]
- Villani, D.; Carissoli, C.; Triberti, S.; Marchetti, A.; Gilli, G.; Riva, G. Videogames for Emotion Regulation: A Systematic Review. Games Health J. 2018, 7, 85–99. [Google Scholar] [CrossRef] [Green Version]
- Coyne, S.M.; Shawcroft, J.; Gale, M.; Gentile, D.A.; Etherington, J.T.; Holmgren, H.; Stockdale, L. Tantrums, toddlers and technology: Temperament, media emotion regulation, and problematic media use in early childhood. Comput. Hum. Behav. 2021, 120, 106762. [Google Scholar] [CrossRef]
- Gueron-Sela, N.; Gordon-Hacker, A. Longitudinal Links between Media Use and Focused Attention through Toddlerhood: A Cumulative Risk Approach. Front. Psychol. 2020, 11, 569222. [Google Scholar] [CrossRef]
- Ballon, N.; Brunault, P.; Cortese, S. Sensation Seeking and Cocaine Dependence in Adults with Reported Childhood ADHD. J. Atten. Disord. 2015, 19, 335–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geissler, J.; Romanos, M.; Hegerl, U.; Hensch, T. Hyperactivity and sensation seeking as autoregulatory attempts to stabilize brain arousal in ADHD and mania? ADHD Atten. Deficit Hyperact. Disord. 2014, 6, 159–173. [Google Scholar] [CrossRef] [PubMed]
- Goodrich, S.A.; Pempek, T.A.; Calvert, S.L. Formal Production Features of Infant and Toddler DVDs. Arch. Pediatr. Adolesc. Med. 2009, 163, 1151–1156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cain, M.S.; Leonard, J.A.; Gabrieli, J.D.E.; Finn, A.S. Media multitasking in adolescence. Psychon. Bull. Rev. 2016, 23, 1932–1941. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garrote, G.P.d.; Rubio, L.; Gómez, B.M.; Buedo-Guirado, C. Smartphone Abuse amongst Adolescents: The Role of Impulsivity and Sensation Seeking. Front. Psychol. 2021, 12, 746626. [Google Scholar] [CrossRef] [PubMed]
- Mehroof, M.; Griffiths, M.D. Online gaming addiction: The role of sensation seeking, self-control, neuroticism, aggression, state anxiety, and trait anxiety. Cyberpsychol. Behav. Soc. Netw. 2010, 13, 313–316. [Google Scholar] [CrossRef]
- Jensen, J.D.; Weaver, A.J.; Ivic, R.; Imboden, K. Developing a Brief Sensation Seeking Scale for Children: Establishing Concurrent Validity with Video Game Use and Rule-Breaking Behavior. Media Psychol. 2011, 14, 71–95. [Google Scholar] [CrossRef]
- Nabi, R.L.; Krcmar, M. It takes two: The effect of child characteristics on US parents’ motivations for allowing electronic media use. J. Child. Media 2016, 10, 285–303. [Google Scholar] [CrossRef]
- Nikken, P. Parents’ Instrumental use of Media in Childrearing: Relationships with Confidence in Parenting, and Health and Conduct Problems in Children. J. Child Fam. Stud. 2019, 28, 531–546. [Google Scholar] [CrossRef] [Green Version]
- Hoza, B. Peer Functioning in Children with ADHD. J. Pediatr. Psychol. 2007, 32, 655–663. [Google Scholar] [CrossRef] [Green Version]
- DuPaul, G.J.; McGoey, K.E.; Eckert, T.L.; VanBrakle, J. Preschool children with attention-deficit/hyperactivity disorder: Impairments in behavioral, social, and school functioning. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 508–515. [Google Scholar] [CrossRef]
- Pimentel, M.J.; Vieira-Santos, S.; Santos, V.; Vale, M.C. Mothers of children with attention deficit/hyperactivity disorder: Relationship among parenting stress, parental practices and child behaviour. Atten. Deficit Hyperact. Disord. 2011, 3, 61–68. [Google Scholar] [CrossRef]
- Faraone, S.V.; Biederman, J.; Mick, E. The age-dependent decline of attention deficit hyperactivity disorder: A meta-analysis of follow-up studies. Psychol. Med. 2006, 36, 159–165. [Google Scholar] [CrossRef]
- Sweetser, P.; Johnson, D.; Ozdowska, A.; Wyeth, P. Active versus Passive Screen Time for Young Children. Australas. J. Early Child. 2012, 37, 94–98. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Perry, A.C. Metabolic and physiologic responses to video game play in 7-to 10-year-old boys. Arch. Pediatr. Adolesc. Med. 2006, 160, 411–415. [Google Scholar] [CrossRef] [Green Version]
- Hu, B.Y.; Johnson, G.K.; Teo, T.; Wu, Z. Relationship between Screen Time and Chinese Children’s Cognitive and Social Development. J. Res. Child. Educ. 2020, 34, 183–207. [Google Scholar] [CrossRef]
- Huber, B.; Yeates, M.; Meyer, D.; Fleckhammer, L.; Kaufman, J. The effects of screen media content on young children’s executive functioning. J. ExChild Psychol. 2018, 170, 72–85. [Google Scholar] [CrossRef]
- Veraksa, N.; Veraksa, A.; Gavrilova, M.; Bukhalenkova, D.; Oshchepkova, E.; Chursina, A. Short- and Long-Term Effects of Passive and Active Screen Time on Young Children’s Phonological Memory. Front. Educ. 2021, 6, 600687. [Google Scholar] [CrossRef]
- Parkes, A.; Sweeting, H.; Wight, D.; Henderson, M. Do television and electronic games predict children’s psychosocial adjustment? Longitudinal research using the UK Millennium Cohort Study. Arch. Dis. Child. 2013, 98, 341–348. [Google Scholar] [CrossRef] [Green Version]
- McCollum, J.F., Jr.; Bryant, J. Pacing in Children’s Television Programming. Mass Commun. Soc. 2003, 6, 115–136. [Google Scholar] [CrossRef]
- Crescenzi-Lanna, L. The developmental appropriateness of digital games and its impact on young children’s enjoyment and playtime. Int. J. Child-Comput. Interact. 2022, 33, 100480. [Google Scholar] [CrossRef]
- Dunn, J.; Brown, J.; Beardsall, L. Family talk about feeling states and children’s later understanding of others’ emotions. Dev. Psychol. 1991, 27, 448–455. [Google Scholar] [CrossRef]
- Fonagy, P.; Redfern, S.; Charman, T. The relationship between belief-desire reasoning and a projective measure of attachment security (SAT). Br. J. Dev. Psychol. 1997, 15, 51–61. [Google Scholar] [CrossRef]
- Sarti, D.; Bettoni, R.; Offredi, I.; Tironi, M.; Lombardi, E.; Traficante, D.; Lorusso, M.L. Tell Me a Story: Socio-Emotional Functioning, Well-Being and Problematic Smartphone Use in Adolescents with Specific Learning Disabilities. Front. Psychol. 2019, 10, 2369. Available online: https://www.frontiersin.org/article/10.3389/fpsyg.2019.02369 (accessed on 29 April 2022). [CrossRef] [Green Version]
- Uhls, Y.T.; Michikyan, M.; Morris, J.; Garcia, D.; Small, G.W.; Zgourou, E.; Greenfield, P.M. Five days at outdoor education camp without screens improves preteen skills with nonverbal emotion cues. Comput. Hum. Behav. 2014, 39, 387–392. [Google Scholar] [CrossRef] [Green Version]
- Nathanson, E. Television and Postfeminist Housekeeping: No Time for Mother; Routledge: London, UK, 2013. [Google Scholar]
- Hinkley, T.; Brown, H.; Carson, V.; Teychenne, M. Cross sectional associations of screen time and outdoor play with social skills in preschool children. PLoS ONE 2018, 13, e0193700. [Google Scholar] [CrossRef]
- Raman, S.; Guerrero-Duby, S.; McCullough, J.L.; Brown, M.; Ostrowski-Delahanty, S.; Langkamp, D.; Duby, J.C. Screen Exposure during Daily Routines and a Young Child’s Risk for Having Social-Emotional Delay. Clin. Pediatr. 2017, 56, 1244–1253. [Google Scholar] [CrossRef]
- Kovess-Masfety, V.; Keyes, K.; Hamilton, A.; Hanson, G.; Bitfoi, A.; Golitz, D.; Koç, C.; Kuijpers, R.; Lesinskiene, S.; Mihova, Z.; et al. Is time spent playing video games associated with mental health, cognitive and social skills in young children? Soc. Psychiatry Psychiatr. Epidemiol. 2016, 51, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Danet, M. Parental Concerns about their School-aged Children’s Use of Digital Devices. J. Child Fam. Stud. 2020, 29, 2890–2904. [Google Scholar] [CrossRef]
- Sivrikova, N.V.; Ptashko, T.G.; Perebeynos, A.E.; Chernikova, E.G.; Gilyazeva, N.V.; Vasilyeva, V.S. Parental reports on digital devices use in infancy and early childhood. Educ. Inf. Technol. 2020, 25, 3957–3973. [Google Scholar] [CrossRef]
- Okada, S.; Doi, S.; Isumi, A.; Fujiwara, T. The association between mobile devices use and behavior problems among fourth grade children in Japan. Psychiatry Clin. Neurosci. 2021, 75, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Limone, P.; Toto, G.A. Psychological and Emotional Effects of Digital Technology on Children in COVID-19 Pandemic. Brain Sci. 2021, 11, 1126. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Tao, S.; Rutayisire, E.; Chen, Y.; Huang, K.; Tao, F. The relationship between screen time, nighttime sleep duration, and behavioural problems in preschool children in China. Eur. Child Adolesc. Psychiatry 2017, 26, 541–548. [Google Scholar] [CrossRef]
- Sundqvist, A.; Heimann, M.; Koch, F.-S. Relationship between Family Technoference and Behavior Problems in Children Aged 4–5 Years. Cyberpsychol. Behav. Soc. Netw. 2020, 23, 371–376. [Google Scholar] [CrossRef]
- Przybylski, A.K. Electronic Gaming and Psychosocial Adjustment. Pediatrics 2014, 134, e716–e722. [Google Scholar] [CrossRef] [Green Version]
- Radesky, J.S.; Weeks, H.M.; Ball, R.; Schaller, A.; Yeo, S.; Durnez, J.; Tamayo-Rios, M.; Epstein, M.; Kirkorian, H.; Coyne, S.; et al. Young children’s use of smartphones and tablets. Pediatrics 2020, 146, e20193518. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variable | Measure | Min | Max | M | SD | Median | IQR |
|---|---|---|---|---|---|---|---|
| Child age T1 | In years | 3.842 | 6.064 | 4.913 | 0.596 | ||
| Child age T2 | 7.264 | 9.542 | 8.270 | 0.556 | |||
| Child gender | (girl/boy) | N boys = 54 N girls = 44 | |||||
| Siblings T1 | Count | 0 | 6 | 0.827 | 0.964 | 1 | 1 |
| Siblings T2 | 0 | 6 | 0.944 | 0.975 | 1 | 1 | |
| Parent age T1 | In years | 23 | 47 | 37.459 | 4.445 | ||
| Parent age T2 | 26 | 50 | 40.888 | 4.479 | |||
| Parental education | Mean score from the two parents’ 6-leveled education. | 2 | 6 | 4.296 | 0.858 | ||
| Parental mobile attachment T1 | Mean score from the four 5-graded items. | 1 | 4.75 | 2.288 | 0.918 | ||
| Parental mobile attachment T2 | 1 | 5 | 2.503 | 1.012 | |||
| MTSD use T1 | In minutes/day | 0 | 110 | 18.157 | 27.090 | 6.965 | 20.750 |
| MTSD use T2 | 0 | 900 | 65.355 | 134.392 | 18 | 54 | |
| SDQ Emotional symptoms T1 | 0 | 6 | 1.888 | 1.698 | 1 | 2 | |
| SDQ Emotional symptoms T2 | 0 | 7 | 1.837 | 1.648 | 1 | 2.250 | |
| SDQ Conduct problems T1 | 0 | 7 | 1.908 | 1.547 | 2 | 2 | |
| SDQ Conduct problems T2 | 0 | 6 | 1.388 | 1.397 | 1 | 2 | |
| SDQ Hyperactivity/inattention T1 | 0 | 10 | 3.837 | 2.469 | 3 | 4 | |
| SDQ Hyperactivity/inattention T2 | 0 | 10 | 2.98 | 2.573 | 3 | 3.250 | |
| SDQ Peer relationship problems T1 | 0 | 8 | 1.684 | 1.870 | 1 | 2 | |
| SDQ Peer relationship problems T2 | 0 | 7 | 1.602 | 1.679 | 1 | 2 | |
| SDQ Prosocial behavior T1 | 2 | 10 | 7.949 | 1.830 | 8 | 2 | |
| SDQ Prosocial behavior T2 | 3 | 10 | 8.214 | 1.607 | 9 | 3 | |
| Cronbach’s Alpha in T1 | Cronbach’s Alpha in T2 | |
|---|---|---|
| Emotional symptoms | 0.485 | 0.528 |
| Conduct problems | 0.554 | 0.487 |
| Hyperactivity/inattention | 0.744 | 0.797 |
| Peer relationship problems | 0.612 | 0.571 |
| Prosocial behavior | 0.656 | 0.549 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Konok, V.; Szőke, R. Longitudinal Associations of Children’s Hyperactivity/Inattention, Peer Relationship Problems and Mobile Device Use. Sustainability 2022, 14, 8845. https://doi.org/10.3390/su14148845
Konok V, Szőke R. Longitudinal Associations of Children’s Hyperactivity/Inattention, Peer Relationship Problems and Mobile Device Use. Sustainability. 2022; 14(14):8845. https://doi.org/10.3390/su14148845
Chicago/Turabian StyleKonok, Veronika, and Rebeka Szőke. 2022. "Longitudinal Associations of Children’s Hyperactivity/Inattention, Peer Relationship Problems and Mobile Device Use" Sustainability 14, no. 14: 8845. https://doi.org/10.3390/su14148845
APA StyleKonok, V., & Szőke, R. (2022). Longitudinal Associations of Children’s Hyperactivity/Inattention, Peer Relationship Problems and Mobile Device Use. Sustainability, 14(14), 8845. https://doi.org/10.3390/su14148845