Abstract
The balanced allocation of medical and health resources is an important basis for the sustainable development of health undertakings. In recent years, China has made remarkable achievements in the medical and health services, but there is still a phenomenon of unbalanced allocation of medical and health resources among different regions, which has become an urgent problem to be solved in deepening the reform of the medical and health system during the 14th Five-Year Plan period. From the perspective of people’s needs for health, this study analyzed the equity and efficiency of urban medical and health resources allocation in China by using the Theil index method and DEA method. Meanwhile, the authors used the coupling coordination degree model to construct a balanced development model with equity and efficiency as subsystems, taking the city of Nanjing as an example to analyze its balanced allocation of medical and health resources from 2008 to 2019. In general, taking Nanjing as an example, it shows that the balanced allocation of medical and health resources in Chinese cities is good, but in geographical dimension, the level of balanced allocation is low, and there are still significant differences in the equity and efficiency of allocation among regions. In the future, the government can strengthen the rationality of regional planning, appropriately increasing health investment and medical supply, considering both equity and efficiency to further realize the balanced allocation of medical and health resources and improve the sustainability of urban medical service system. The main contribution of this paper lies in that, from the perspective of sustainable development, the evaluation system is integrated to measure the equity and efficiency respectively, and the balanced development model is used to investigate the allocation of urban medical and health resources. The research results can provide reference for optimizing resources allocation and promoting the sustainable development of medical and health undertakings.
1. Introduction
According to the theory of sustainable development, sustainable development can be defined as meeting the needs of the present generation without hindering the development of the ability of future generations to meet the needs. It focuses on multi-dimensional development, including equity, efficiency, integrity and sustainability of development [1]. As a new concept of social development and values, the 2030 Agenda for Sustainable Development was adopted by The United Nations Sustainable Development Summit in 2015. One of the 17 Sustainable Development Goals (SDGS) is to “Ensure healthy lives and promote well-being for all at all ages” [2]. Health is a basic right of mankind, and health care for all is the goal of the development of medical and health services. From the perspective of sustainable development, the sustainability of the development of medical and health services should be reasonable allocation and effective use of medical and health resources under the premise of not violating the objective law of development, which should not only meet the growing needs of current residents, but also contribute to the long-term development of medical and health service system, so as to achieve the improvement of human health level [3]. As a social resource to implement medical and health care activities, medical and health resources are scarce and limited. The rational allocation of these resources matters to realize the sustainable development of medical and health undertakings and protect citizens’ equal right to health, which is advocated as a basic principle by the World Health Organization [4]. However, this is also a worldwide problem in health system reform. There are differences in regional health resource allocations both in developing and developed countries [5].
As the largest developing country and the most populous country in the world, China has repeatedly proposed to deepen the reform of the medical and health system, and has tried to increase health investment and implement graded diagnosis and treatment to guide the sinking of high-quality medical and health resources since the implementation of the new medical reform in 2009 [6]. The government aims to improve the current situation of “difficult and expensive medical treatment” of residents, meet the growing medical needs of the people and gradually realize the equity of medical and health services. However, drawbacks still exist in the aspects of the unbalanced urban-rural distribution of medical and health resources [7] and unequal access to resources and structural imbalance [8]. The medical and health resources in different urban areas may vary from each other even in the first-tier and new first-tier cities like Beijing, Shenzhen and Nanjing, which is mainly reflected in the concentration of resources in the central urban area [9,10]. The resources of large hospitals in cities are over concentrated and the patients are overcrowded, while the total resources of primary medical and health institutions are insufficient and less utilized [11]. The medical and health service system is structured as an “inverted pyramid”, and the imbalance tends to expand further between and within regions. As the increasing aging of the population, people’s health demands have been further released with the substantial improvement in residents’ living standards and the medical security system. Accordingly, the apparent contradiction has intensified between the unbalanced and insufficient allocation of medical and health resources and people’s demand for high-quality medical and health resources. At the end of 2019, the sudden outbreak of the coronavirus (COVID-19) epidemic not only challenged the country’s governance capacity as well as the prevention and control capacity of the whole society, but also tested the medical and health resources of cities, exposing their many shortcomings [12]. On 13 March 2021, the Outline of the 14 Five-Year Plan (2021–2025) for National Economic and Social Development and the Long-Range Objectives Through the Year 2035 of the People’s Republic of China, was released, which stressed to deepen the reform of the medical and health system, expand the supply of medical service resources guided by improving medical quality and efficiency, and speed up the expansion of high-quality medical resources and regionally balanced layout [13]. Therefore, in this context, it remains an obstacle for China in the current and future to optimize the allocation of medical and health resources, promote the modern medical and health service system and effectively improve the social security for people in the sustainable development of medical and health undertakings.
Scientific evaluation of the allocation of medical and health resources within the city is an evidence-based premise for optimizing the input structure and rational allocation of resources. At present, many scholars have measured and analyzed the level of medical and health resources allocation from national and provincial macro levels, but few studies have focused on cities and their interior. However, in the context of China’s aging urban population and increasing urbanization, attention should be paid to the sustainable development of urban medical and health service system. We not only need to evaluate and analyze the equity and efficiency of the allocation of medical and health resources within the city through scientific methods, but also should further analyze the coordination of these two goals, which plays an important role in improving the rationality of the allocation of medical and health resources and maximizing the benefit of the government’s financial investment.
In view of this, this paper intends to use the mainstream methods of resources allocation equity and efficiency evaluation to analyze the allocation of urban medical and health resources. On this basis, using the coupling coordination degree model for reference, the balanced development model of medical and health resources allocation is constructed to further analyze the coordination between the two goals of equity and efficiency. According to the results of empirical analysis, effective suggestions are put forward to help relevant departments formulate targeted policies and measures to strengthen the balanced allocation of medical and health resources, promote the rational planning and scientific layout of urban medical and health resources, and lay an important foundation for the sustainable development of medical and health undertakings.
2. Literature Review
Throughout history, equity and efficiency has been an important issue and main goal of medical and health resources allocation [14]. To scientifically and accurately evaluate the equity and efficiency of medical and health resources allocation is the key to optimizing its configuration. Therefore, many scholars have conducted in-depth studies on this topic. From the perspective of research objects, some scholars have evaluated the equity or efficiency of the allocation of medical and health resources in the region as a whole at the macro level, taking regions, countries, provinces and cities as different decision-making units. For example, Dlouhý used Robin Hood Indexes (RHIs) and the Data Envelopment Analysis (DEA) method to measure the inequality of health resource allocation in the Czech Republic [5]. Xu et al. applied a hybrid of panel data analysis and an augmented DEA to comprehensively evaluate the allocation efficiency of community health resources in 13 cities in Jiangsu Province of China from the perspective of horizontal and vertical integration. It was found that the overall efficiency of health resources allocation in Jiangsu province improved, but there was still a significant gap between regions [15]. Some scholars evaluated the allocation of medical and health resources from the micro level, taking hospitals, primary health care institutions and other medical and health institutions as decision-making units. Shinjo and Aramaki selected 348 Secondary Healthcare Service Areas (SHSAs) in Japan as the research objects and used Lorenz curve and Gini coefficient to evaluate the equity of doctor allocation between hospitals and clinics [16]. Czypionka et al. evaluated the efficiency of the acute care sector in Austrian, using DEA models based on data of 128 public and private non-profit hospitals from 2010 [17]. After reviewing the literature, it is found that few scholars take cities as their research objects to conduct in-depth analysis on the allocation of medical and health resources within the city. What is the input and utilization condition of medical and health resources in urban areas? Is there waste and the allocation equitable? These issues are worth exploring in depth.
From the perspective of research content, some scholars had evaluated the equity of medical and health resources allocation. For example, Horev et al. used the Gini coefficient to measure the degree of equality in the distribution of doctors and hospital beds in various states and counties in the United States [18]. Zhang et al. evaluated equity of medical and health resources allocation between hospitals and primary care institutions in China [19]. Liu et al. applied the Theil index to study the equity and changes of medical and health resources allocation in China from 2009 to 2013 [20]. Most scholars had evaluated the efficiency of medical and health resources allocation. For example, Cetin and Bahce assessed the allocation of health resources in 34 OECD countries and found that 11 countries are more efficient in the allocation and 15 countries still have room for improvement Using health resources as the input indicator [21]. Top et al. measured the efficiency of health care systems in 36 African countries and found that 41.67% of them have inefficient health care systems [22]. Retzlaf-Roberts et al. utilized the traditional DEA model to analyze the utilization efficiency of medical and health resources in each OECD country from a technical perspective [23]. De et al. used DEA and Tobit models to compare the efficiency of health systems and their influencing factors in various Indian states [24]. Yi et al. [25] and Lin et al. [26] respectively analyzed the input and utilization efficiency of medical and health resources in China by using super efficiency three-stage slack-based measure model (SBM-DEA) and DEA-Malmquist Index model. Furthermore, some scholars conducted a comprehensive evaluation from the above two perspectives by measuring equity and efficiency at the same time. For example, Sun et al. investigated the equity of health resources allocation in China from 2011 to 2015 by adopting Gini coefficient and Concentration index, and evaluated the allocation efficiency by using DEA method [27]. Zhang et al. used the same method to measure the equity and efficiency of medical and health resources and services in 31 provinces of China in 2011 [28]. However, existing studies simply evaluated the equity and efficiency of medical and health resources allocation, few scholars had effectively combined equity and efficiency to analyze the internal coordination mechanism between them. Are equity and efficiency developing in a coordinated way? Do they promote or constrain each other? How balanced is the allocation of medical and health resources? Obviously, it is of great significance to study these problems to optimize the allocation of medical and health resources.
To sum up, existing studies have carried out a large number of beneficial explorations on the allocation of medical and health resources, laying an important foundation for the development of this study. However, existing studies mostly start from the micro level or are based on the macro level of national and provincial administrative regions, while few scholars focus on the urban regional level to analyze the allocation of medical and health resources. In addition, few scholars consider the balanced allocation of resources from the perspective of sustainability. Therefore, this paper makes a further breakthrough from the research object and perspective, and conducts an in-depth study on the allocation of medical and health resources.
3. Materials and Methods
3.1. Study Area and Potential Data Sources
Under the guidance of the general strategy of national medical reform, cities in China, especially the first-tier and new first-tier cities with great economic power, have launched a series of reforms to promote the balanced allocation of medical and health resources in combination with their actual situation. For example, Nanjing, as a representative of the new first-tier cities, has actively promoted the construction of modern urban medical and healthcare systems under the concept of “Healthy Nanjing”. By the end of 2019, the number of beds per 1000 population, licensed (Assistant) physicians and registered nurses in the city had reached 6.95, 4.20 and 5.00 respectively, which were higher than the provincial average level, but there was still a certain gap from the expected target. In addition, there were significant differences among different administrative regions in Nanjing in the allocation of medical resources. The number of beds per 1000 people in Gulou district was 17.17, the number of licensed (assistant) physicians and registered nurses were 9.10 and 13.37 respectively. By contrast, the numbers in Pukou district were only 3.42, 2.49 and 2.58. As the capital of Jiangsu Province, and the core city of Nanjing metropolitan area, Nanjing was the only megacity in the Yangtze River Delta city group (a city with a permanent urban population of 5 million to 10 million), with 8,085,241 people living in urban areas, and the urbanization rate was 86.80%. Meanwhile, Nanjing was also one of the earliest cities in China to enter the aging population. By the end of 2020, 18.98% of the city’s permanent residents were aged 60 and above, among which 13.70% were aged 65 and above [29]. It can be seen that Nanjing is a typical sample of China’s urban development with a certain degree of representativeness. Therefore, this paper takes Nanjing city as an example to analyze the equity and efficiency of urban medical and health resources allocation based on the existing research status and urban healthy development needs. At the same time, with the help of balanced development model, the coupling coordination relationship between the equity and efficiency is analyzed to measure the balanced allocation of medical and health resources. The aim is to provide scientific basis for Nanjing to optimize the allocation of medical and health resources and promote the sustainable development of medical and health undertakings, and to provide reference for other cities.
The original data (2008–2019) of each index in this paper mainly came from literature (2009–2020), including Jiangsu Statistical Yearbook, Nanjing Statistical Yearbook, Statistical Bulletin on the Development of Health Care in Jiangsu and Statistical Bulletin of National Economic and Social Development in Nanjing. At the same time, the statistical information and publicity documents published on official websites of Nanjing municipal government and Nanjing health commission were also included. In addition, according to the geographical location and the regional division in the official document issued by Nanjing municipal government, Nanjing is divided into the main urban region, Jiangbei region and Ningnan region from north to south (Figure 1). Meanwhile, Nanjing carried out the adjustment of urban administrative divisions in 2013. Namely, the original Qinhuai district and Baixia district were merged as the new Qinhuai district and the original Gulou district and Xiaguan district were merged as the new Gulou district, and the original Lishui county and Gaochun county were changed into Lishui district and Gaochun district. Therefore, to ensure the consistency of statistical caliber of index data, the author merged the data of the original Qinhuai district withBaixia district from 2008 to 2012 into the data of Qinhuai district, combined the data of the original Gulou district with Xiaguan district into the data of Gulou district, and took the data of Lishui county and Gaochun county as the data of Lishui district and Gaochun district.
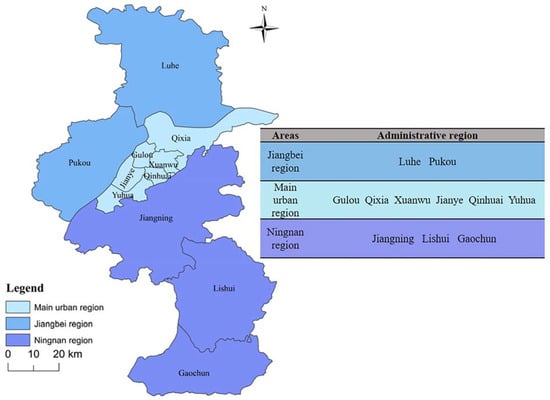
Figure 1.
Distribution map of three regions in Nanjing.
3.2. Evaluation Index
According to the objective and principle of balanced allocation of medical and health resources, the evaluation indexes can be selected from two perspectives of equity and efficiency, and the evaluation index system should be constructed under the guidance of scientific system and feasible and comparable principle. Therefore, the selection of indicators in this paper strictly follows four principles: (1) the scientific principle, which refers to the construction of evaluation index system of medical and health resources allocation based on scientific theories; (2) the systematic principle, which means to establish an evaluation indicator system that can truly reflect the allocation of medical and health resources by selecting evaluation indicators related to medical and health resources. Among them, all indicators should be independent of each other and have certain correlation; (3) the feasibility principle, which means that the selected indicators can be obtained through data sorting, observation and measurement, that is, operability; and (4) the comparability principle, which means that all indicators should be consistent in statistical caliber to ensure horizontal or vertical comparison. Among them, horizontal comparison refers to the comparison between different regions in the same period, which can reflect regional differences in medical and health resource allocation, while vertical comparison refers to the comparison between different periods in the same region, which can reflect dynamic changes in medical and health resource allocation.
The review of literature presents that the existing evaluation index system covers various dimensions, including medical and health resources supply, medical and health resources utilization, medical and health services supply and effect, etc. Specifically, in the evaluation of equity in medical and health resources allocation, scholars focused on the dimension of medical and health resource supply. That is, they started from assessing the investment of medical and health resources, and mostly selected specific indicators based on the concept of medical and health resources, which mainly covers the human resources, material resources and financial resources [20,28,30]. In assessing the efficiency, scholars might add the dimensions of medical and health resources utilization as well as medical and health service supply and effect, that is, assessing the input and output (benefits) of medical and health resources. The output indicators generally referred to specific quantitative indicators reflecting the utilization of medical and health resources and improvement of people’s health, which specifically included outpatient and emergency visits, rates of utilization of beds, the number of admitted (discharged) patients and population survival rate, etc. [15,22,25].
The direct output of the government’s financial investment in medical and health is reflected by the increase of medical human and material resources, which improves the supply of medical and health services and affects people’s satisfaction. Therefore, this study focused on the balanced development of the allocation of medical and health human and material resources in urban areas of China. To make it a scientific, systemic, feasible and comparable study, the author designs the evaluation index system from the two dimensions of input and output for the balanced allocation of medical and health resource. Combined with the urban development situation, the system consisted of five primary indicators and eight secondary indicators which were constructed in the premise that the statistical data can be obtained and consistent with the statistical caliber, as illustrated in Table 1.

Table 1.
Evaluation index system of balanced allocation of medical and health resources.
Table 2 is the descriptive statistical analysis of indicator variables. It can be seen that the 11 administrative regions of Nanjing have great differences in the allocation of medical and health resources such as the number of medical and health institutions and the number of beds. For example, the standard deviation of the number of beds is 3820.16, the minimum is 672 and the maximum is 18,313. In terms of the allocation of medical and health resources per thousand population, the number of health personnel per 1000 population of each administrative region varies greatly, with a standard deviation of 4.989, a maximum of 31.58, and a minimum of 3.26. In contrast, the difference in the number of health facilities per 1000 population is smaller, as is the difference in population survival rates as an indicator of output.
Table 2.
Descriptive statistical analysis of indicator variables.
3.3. Methods
Rational allocation of medical and health resources includes not only fair allocation of resources, that is, equity of allocation, but also effective utilization of resources, that is, efficiency of allocation. Among them, equity is unity of equal opportunities, equal results and residents’ right of choice [34]. Equitable distribution of medical and health resources can effectively improve the accessibility of residents’ health services, and then create an equal medical and health service system for everyone, and realize the real development of medical and health undertakings. Efficiency reflects how to effectively use limited medical and health resources to achieve greater benefits, which is one of the keys to achieve sustainable benefits in the development of medical and health undertakings. On the one hand, from the perspective of medical and health resources allocation means, there are usually two means of medical and health resources allocation, namely government and market. As the “visible hand”, the government is conducive to ensuring the equity of medical and health resources allocation, and as the “invisible hand”, the market allocation of resources has a significant advantage in improving the efficiency of resource allocation. Since the medical and health industry is both public welfare and economic, the medical and health resources need to be effectively allocated by both the government and the market. That is, the balanced allocation of medical and health resources is not only related to equity, but also to efficiency [35]. On the other hand, from the perspective of medical and health resources allocation process, equity affects efficiency and efficiency promotes equity. If the allocation of resources is unequal, residents in some regions may not be able to get good medical and health services due to economic, geographical and other factors, and the allocation of resources in some regions is excessive. This leads to the waste of the city’s overall health resources and low efficiency. On the contrary, an environment of fair allocation of medical and health resources can not only enable people to obtain equal rights to health, but also promote the full utilization of medical and health resources to maximize the use of labor and physical forces, thereby improving overall efficiency. At the same time, the improvement of efficiency means that more medical and health service output can be obtained with less investment of medical and health resources, so that more people can be guaranteed and enjoy high-quality medical and health resources, that is, to achieve a higher level of equity.
There is a coupling relationship with unity of opposites and spiral intertwining between equity and efficiency which are two goals of medical and health resources allocation. The combination of the two and mutual promotion is manifested as balanced allocation of medical and health resources. The sustainable development concept puts forward to higher requirements for the allocation of resources, which should not only pay attention to the equity and efficiency of allocation, but also take into account the balance between the two to promote the balanced allocation of medical and health resources [36,37], so as to lay a solid foundation for the sustainable development of medical and health undertakings. At the same time, the balanced allocation of medical and health resources is not achieved overnight, but is a long-term and complex process. To achieve the balanced allocation, we need to take the sustainable development concept as the support, take into account the immediate and long-term interests, and promote the reform of medical and health resources allocation system and mechanism.
Therefore, this paper adopts the Theil Index (TI) and Data Envelopment Analysis (DEA) to evaluate the equity and efficiency of healthcare resource allocation. On this basis, under the guidance of sustainable development concept, Equity and efficiency are regarded as two subsystems, and coupled coordination degree model is introduced to construct a balanced development model which can be used to evaluate the allocation of medical and health resources, so as to comprehensively analyze the degree of balanced allocation of urban medical and health resources.
3.3.1. Equity Analysis Method
Currently, the main methods to measure the equity of medical and health resources allocation include the Lorentz curve, Gini coefficient and Theil index. Due to the difference in application of different evaluation methods, it is of great significance to select the appropriate method according to the research purpose. The research objective of this paper is mainly to identify and measure the differences in the allocation of medical and health resources in urban regions, to be specific, not only to measure the overall distribution characteristics of urban regional differences, but also to further clarify the main internal reasons for the differences. Among many methods, Lorenz curve and Gini coefficient focus on reflecting the overall inequality of resource allocation, but it is difficult to measure the internal differences. The Theil index method used by economist Theil not only contains the measurement of the overall difference but also can decompose the difference, which is helpful to further identify the fairness of resource allocation between and within regions and its contribution to the formation of the overall gap [38]. Therefore, the Theil index was selected in this paper to analyze the differences between individuals or groups quantitatively. It measures inequality based on the information entropy theory, which is also known as Theil’s entropy measure. A more significant deviation from 0 indicated a greater degree of difference, namely, worse equity and vice versa [20]. Theil index is used to measure the equity allocation of a single index, as shown in Formula (1) below [39]. Further, according to the index weight, the total tell index of medical and health resource allocation in Nanjing is generated, as shown in Formula (2) [40].
where, Ts represents Theil index of the s index, n represents 11 administrative districts of Nanjing. p, fs represents population (geographical area) and the number of medical and health resources of the sth item. pi, fis is the population (geographical area) of administrative region i and the number of medical and health resources in item s; Tc represents the total tell index of medical and health resource allocation in Nanjing. In actual calculation, when the measurement samples are divided into multiple groups, the Theil index can be decomposed into inter-regional Theil index (Tb) and intra-regional Theil index (Tw) [41]. The formula is shown as following:
k refers to the total number of divided regions, gj refers to the jth divided region; pj and fjs refers to the population (the geographical area) and the sth medical and health resources in the jth divided regions. The regional contribution rate can also be calculated based on the above decomposition formula. The specific calculation formula is shown as follows:
where Ib and Iw respectively represent the contribution rates of inter-regional differences and intra-regional differences to the total differences [42]. That is, the proportion of the two in the overall difference, and their value can reflect the influence degree of different differences.
In July 2016, China’s National Health Commission issued the Guiding Principles on Printing and Distributing the Planning for the Establishment of Medical Institutions (2016–2020), which proposed to adjust the allocation principle to “equity and accessibility, overall planning, scientific layout, coordinated development, and equal emphasis on Traditional Chinese medicine and Western medicine”. It indicated that the allocation of medical and health resources mainly follows the principle of “equity first and efficiency considered”. At the same time, the allocation of medical and health resources should be coordinated with urban planning by making a reasonable layout based on the scope of medical services to match the spatial distribution of medical and health resources with the characteristics of the local population. Thus, the accessibility of medical and health resources and the rationality of resource allocation shall be improved [43,44]. Therefore, the population demand and resource accessibility should be comprehensively considered in allocating medical and health resources. The balance evaluation was hereby conducted from dimensions of population distribution and geographical area.
3.3.2. Efficiency Analysis Method
Because the allocation of medical and health resources has the characteristics of multiple inputs and multiple outputs, a simple cost–benefit framework often cannot meet the needs of medical service system analysis. Therefore, since Data Envelopment analysis (DEA) was introduced into medical and health research, because it is suitable for multi-input-multi-output-multi-stage production efficiency evaluation and does not need to determine the weight of each index, it has been adopted by most scholars at home and abroad to evaluate the allocation efficiency of medical and health resources [45]. DEA was first proposed by American operational research scholars A. Charnes and W. W. Cooper in 1978, which is a non-parametric statistical method designed to measure the relative effectiveness of decision-making unit by using linear programming method according to multiple input and output indexes of decision-making unit [46]. The DEA method was first applied to evaluate efficiency based on a constant return to scale, namely, the Charnes, Cooper, and Rhodes model (CCR). Subsequently, Banker R. D. further liberalized the conditions of the assumption and modified it to variable return scale, namely the Banker, Charnes, and Cooper model (BCC) [47], where technical efficiency (TE) can be further divided into pure technical efficiency (PTE) and scale efficiency (SE). Considering that the return scale is generally variable in practice, the BCC model was selected in this paper to evaluate the efficiency of medical and health resource allocation [48].
Assuming that there are n decision-making units and each unit has m inputs and s outputs, for the j-th decision-making unit, its inputs and outputs can be expressed by vectors and vectors , , j = 1, 2, ⋯, n, and the efficiency value of each unit can be obtained by 23:
where x0 and y0 refers to the input and output vector of decision-making unit, is weight coefficient and is the efficiency value of decision-making unit. Meanwhile, indicates that the restrictive conditions of convexity are added on the leading edge, making a return to scale variable. When , namely, the technical efficiency equals to 1, the unit is on the production frontier, indicating the efficiency of DEA. On the contrary, when the technical efficiency is less than 1, it indicates that the unit does not reach the DEA efficiency state. PTE represents the efficiency value of each unit, excluding scale factors. When pure technical efficiency equals 1, it indicates pure technical efficiency, and when pure technical efficiency is less than 1, it indicates non-pure technical efficiency. On the other hand, scale efficiency represents the efficiency value of each unit excluding management factors. When scale efficiency equals 1, it indicates scale efficiency, and when scale efficiency is less than 1, it indicates non-scale efficiency [49]. As decomposition efficiency of technical efficiency, the comparison of efficiency values between pure technical efficiency and scale efficiency can explain the invalidity of DEA. When pure technical efficiency is less than scale efficiency, the non-efficiency in DEA is mainly caused by unreasonable management; on the contrary, when scale efficiency is less than pure technical efficiency, the non-efficiency in DEA mainly attributes to the unreasonable scale.
3.3.3. Balance Evaluation Model
In the field of resource allocation, coupling coordination degree model is widely used to measure and analyze the coordinated development of objects. The principle of coupling is derived from physics, indicating that two or more systems are interdependent, coordinated, and promoted as related forms and phenomena [50]. Subsequently, in the fields of economics, medicine, geography and ecology, most scholars used the coupling coordination degree model to measure the degree of association between systems. For example, Fan et al. studied the coupling and coordinated development of ecological resource utilization destruction and urban economic development among various regions in China [51]. Hu et al. applied coupling coordination degree model to measure the coupling coordination degree of pharmaceutical manufacturing industry and medical service industry in China [52]. Li et al. used the coupling coordination degree model to measure the interaction between urbanization and ecosystem health [53]. Dong et al. took the coupling coordination degree model and spatial autocorrelation model to quantitatively study the spatio-temporal characteristics and dynamic mechanism of the coupling coordination relationship between green urbanization and green finance from 2010 to 2017 [54].
Based on the concept of sustainable development, after evaluating the equity and efficiency respectively and referring to the coupling coordination model, the study first introduced the capacity coupling coefficient to measure the coordination relationship between the two subsystems of equity and efficiency, which is expressed as follows [55]:
where C represents the coordination degree of the two systems, whose value is set as [0, 1]. When C is closer to 0, it indicates that the two systems are closer to imbalance; when C is closer to 1, they are closer to coordination, indicating a higher coordination degree. F refers to the equity index, whose calculation result of the Theil index can be expressed in the equity measuring process: F = 1 − Tc. The closer the result of the Theil index is to 0, the higher the equity is, which is considered a negative index. Therefore, it will be positively processed in the actual calculation of coordination degree. While may present negative values in the actual situation, the deviation range from 0 can represent equity. Therefore, the absolute value is taken as the result in the equilibrium calculation. E refers to the efficiency index, which can be directly expressed by the DEA calculation results in the measurement of efficiency, i.e., E is equal to technical efficiency. k refers to the adjustment coefficient, which is set as 2 in this paper according to the existing studies [56].
Secondly, on the basis of the coordination degree model, the balanced development model is further introduced to measure the comprehensive development degree of equity and efficiency under the coordination relationship, that is, the balanced allocation of medical and health resources. The specific calculation is as follows:
where T is calculated by the weighted correction of the two systems, indicating the comprehensive harmonic index of equity and efficiency of medical and health resources allocation. , are contribution coefficients of equity and efficiency respectively, + = 1. Since the author perceived that equity and efficiency pose the same effect on the balanced allocation of medical and health resources, the values of , are both set as 0.5 [52]. D refers to the balanced development degree of medical and health resources, indicating the balanced allocation level of medical and health resources; The value range of the balanced development degree is from 0 to 1. To conduct qualitative research on the balanced allocation level of medical and health resources, the study referred to the existing research results [51,52,53,54], and subordinated the balanced development degree of a certain interval to the same type. As the result, the balanced development degree of medical and health resources allocation is divided into five types. The higher the balanced development degree is, the more coordinated and mutually promoted the equity and efficiency are in the medical and health resources allocation and vice versa. Details are illustrated in Table 3.
Table 3.
Level Classification of Balanced Development Degree.
4. Results
4.1. Results of Equity Analysis
4.1.1. Total Theil Index Analysis
Figure 2 illustrates the overall Theil index and its changing trend of growth rate concerning medical and health resources allocation in Nanjing based on the population distribution and geographical area from 2008 to 2019.
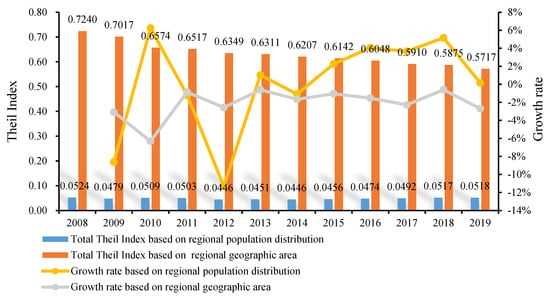
Figure 2.
Total Theil index and its growth rate of medical and health resources allocation in Nanjing from 2008 to 2019.
On the whole, the equity of medical and health resources allocation in Nanjing from 2008 to 2019 is insufficient, which is failed to improve synchronously with the population scale and regional planning. Compared with the allocation equity from population dimension, there is more room to improve from geographical dimension. Specifically, from the perspective of population, the total Theil index deviates from zero to a certain extent, floating between 0.04 and 0.06. It decreased from 0.0524 in 2008 to 0.0518 in 2019 at the decline rate of 1.21%, indicating that improvement still requires to be made in the coordination degree between resource allocation and population distribution. In terms of changing trend, the growth rate of the total Theil index fluctuates from year to year, and the average annual value from 2015 to 2019 are positive, indicating that the Theil index has an upward trend, which should be carefully noted. From the perspective of geographical area, the total Theil index is measured between 0.24 and 0.32, which is larger than the value in the population dimension. The equity of the city’s geographical allocation is inferior compared with the equity of population allocation. However, the growth rate in the geographical dimension is negative, with an average annual decrease of 2.11%, indicating that the coordination degree between resource allocation and geographical area is increasing year by year.
4.1.2. Regional Theil Index Analysis
From the perspective of Theil index decomposition and contribution rate (Table 4), the intra-regional differences in the population dimension are the main reasons that hinder the improvement of medical and health resources allocation equity. In contrast, the inter-regional differences are prominent in the geographical dimension. In the population dimension, the intra-regional Theil index in 2008–2019 is greater than the inter-regional index, the contribution rate of the former is measured between 55–63%, indicating that the differences in the allocation of medical and health resources in the main urban region, Jiangbei region and Ningnan region is more significant in the population dimension. This explains the mismatch between the allocation of medical and health resources and population distribution. In contrast, the intra-regional index under the geographical dimension is smaller than the inter-regional index, indicating that the difference between the three regions in Nanjing is the main reason for the inferior equity allocation of medical and health resources according to the geographical area. However, the contribution rate of the intra-regional difference is measured in the range 42–45%, which should also be noted.
Table 4.
Theil index and contribution rate of each region based on population distribution and geographical area.
The equity of medical and health resources allocation in the three regions is sorted as “Jiangbei region > Ningnan region > main urban region”. The specific analysis shows that the Theil index of the main urban region increase from 0.0370 to 0.0439 under the population dimension (2008–2019), indicating that the mismatch between its internal medicine and health resource allocation and population distribution has been further intensified. However, The Theil index of Jiangbei region and Ningnan region respectively decrease from 0.0026 to 0.0003 and 0.0160 to 0.0022, with a decrease of 88.10% and 86.10%, indicating that the matching between resource allocation and population distribution has been significantly improved. From the perspective of geographical area, the Theil index of the main urban region is also higher than that of Jiangbei region and Ningnan region, measured between 0.3600–0.4400, while Ningnan region remains at the level of 0.0180–0.0390, Jiangbei region is measured 0.0004–0.0080, which further indicating that there are significant differences within the main urban region. The Theil index of the main urban region decreases from 0.4332 to 0.3652, a decrease of 15.70% explains that the synergy between internal resource allocation and regional planning in the main urban region has been slightly improved. Overall, the contribution rate of the main urban region is measured highest in both dimensions, that is, the internal difference of the main urban region accounts for the inferior equity of medical and health resources allocation in the region.
Based on the analysis results given above, the explanations for the significant differences in the allocation of medical and health resources are further analyzed (Table 5). There are insufficient and excessive resource allocations in the main urban region in both dimensions, accounting for the significant internal allocation difference. Specifically, in the population dimension, the Theil index of Qixia, Yuhuatai and Jianye has remained negative during the study, that is, the supply of medical and health resources in the two districts failed to meet the population scale indicating that there is a shortage of resources, and the equity of resource allocation is insufficient. The value of Theil index in Xuanwu district showed a staggering fluctuation of “negative-positive-negative-positive” and there is a significant increase, indicating that the area changed from insufficient resource allocation to excessive resource allocation, and the degree of differentiation also expanded. The Theil index value of Qinhuai and Gulou are positive, suggesting that the supply of medical and health resources exceeds its population scale. In the geographical dimension, the Theil index values of the other six administrative regions are positive except for Qixia, indicating that the proportion of medical and health resources exceeded the proportion of the geographical area, namely, a surplus of resources. Among these regions, the most significant deviation is found in Gulou, indicating the worst equity of geographical allocation, while Yuhuatai presents much less deviation in the Theil index value.
Table 5.
Theil index of each administrative district within the main urban region based on population distribution and geographical area.
4.2. Results of Efficiency Analysis
4.2.1. Technical Efficiency Analysis
On the overall, the efficiency of medical and health resources allocation in Nanjing is low (Table 6). From 2008 to 2019, the technical efficiency ranged from 0.770 to 0.890, without reaching the DEA efficiency. Although the technical efficiency increased during the study period (by 14.41%) in a slight way, further improvements still must be made.
Table 6.
The technical efficiency value of medical and health resources allocation in Nanjing from 2008 to 2019.
From the perspective of each region (Figure 3 and Table 6), there is a particular gap in the technical efficiency of inter-regional medical and health resources allocation in Nanjing from 2008 to 2019, which is generally sorted as “Jiangbei region > Ningnan region > main urban region”. Specifically, the utilization of medical and health resources in Jiangbei region is relatively good, whose technical efficiency value is measured highest among the three regions more than half the time during the study period, and Pukou district is the most prominent among the regions. Pukou reached the DEA efficient level in 2010, 2012 and 2016–2019, and the average technical efficiency in 2008–2019 exceeds 0.950, indicating a high utilization efficiency of medical and health resources. However, the utilization level of medical and health resources in the Ningnan region and the main urban region is inferior. The overall utilization in Ningnan region presents a degradation trend, and its technical efficiency value has decreased from 0.903 in 2008 to 0.834 in 2019, showing a decrease of 7.60%. There is a significant efficiency gap within the main urban region, which affects its overall efficiency.
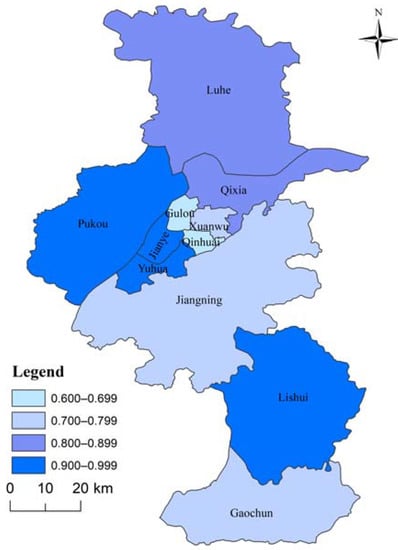
Figure 3.
Average technical efficiency of medical and health resources allocation in administrative districts of Nanjing from 2008 to 2019.
From the perspective of each administrative region, the mean spatial distribution of the technical efficiency of medical and health resources allocation in the 11 administrative regions of Nanjing from 2008 to 2019 is obviously different, showing an increasing feature in time. The average technical efficiency of Jianye district, Yuhuatai District, Pukou District and Lishui District is above 0.900, close to DEA efficiency, but it is worth noting that the allocation efficiency of medical and health resources in Jianye district fluctuates significantly from 2008 to 2019. Luhe district and Qixia District belong to the second echelon, with average technical efficiency of 0.810 and 0.868, respectively. Xuanwu district, Jiangning District and Gaochun District are the third echelon, with an average technical efficiency of 0.700–0.799. Finally, the average technical efficiency of Gulou District and Qinhuai District is only 0.600–0.699, and the efficiency value is low during the study period, both of which are DEA ineffective. Fortunately, the efficiency level has a significant trend of improvement, with growth rates of 105% and 86%, respectively.
4.2.2. Pure Technical Efficiency and Scale Efficiency Analysis
Viewing from the decomposition indicators of technical efficiency (Figure 4), the pure technical efficiency of medical resource allocation in Nanjing from 2008 to 2019 was less than the scale efficiency, that is, the shortage in pure technical efficiency hinders the improvement of technical efficiency. From 2008 to 2019, the scale efficiency of the city’s medical and health resources allocation was higher than 0.900 and reached 0.999 in 2018, indicating that the city’s medical and health resources investment is approaching the optimal state. However, the pure technical efficiency remains at the level of 0.800–0.890 with room for improvement, indicating that the inferior management method and insufficient utilization of medical and health resources account for the less developed efficiency level.
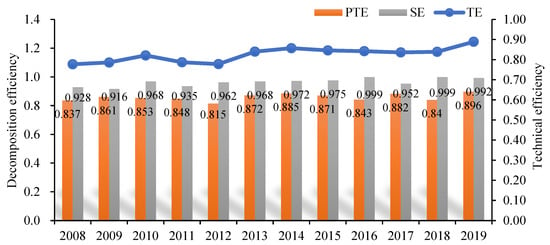
Figure 4.
Decomposition of technical efficiency of medical and health resources allocation in Nanjing from 2008 to 2019.
Viewing each administrative region (Figure 5), the mean value of pure technical efficiency presents a large gap, and the mean value of scale efficiency tends to be consistent. Specifically, the average pure technical efficiency of Pukou, Xuanwu, Lishui and other administrative districts is high, ranking 0.900–0.999. In contrast, the values of Jiangning and Gaochun are at the level of 0.700–0.799, while the average pure technical efficiency of Qinhuai is merely measured between 0.600–0.699, which seriously hinders the improvement of technical efficiency. In terms of scale efficiency, Xuanwu and Gulou present low scale efficiency (about 0.700 for Xuanwu and about 0.800 for Gulou). The scale efficiency of Qixia, Jianye and the other eight administrative districts is better, measured above the level of 0.900, reaching the scale-effective state. The scale efficiency of Pukou even reaches 1, indicating that the medical and health resources investment is reasonable.
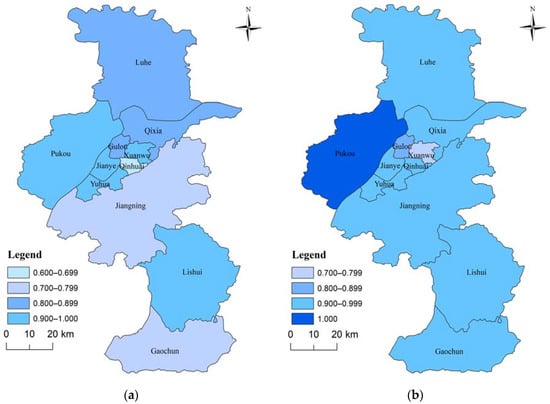
Figure 5.
Decomposition value of technical efficiency of medical and health resources allocation: (a) Mean value of pure technical efficiency; (b) Mean valued of scale efficiency.
4.3. Results of Balance Evaluation
Overall, the balanced level of medical and health resources in Nanjing allocated by population is better than that by geography (Table 7). Viewing from the population dimension, the evaluation value of a balanced development degree is higher than 0.90, indicating a superior, balanced development. The highest value was 0.96 in 2019 and the lowest was 0.92. In contrast, the evaluation value of the balanced development degree in the geographical dimension remains between 0.56–0.71, reaching the primary-level and medium-level balanced development. In 2018, it was the lowest (0.56). However, the balanced development degree of the allocation according to the geographical area increased from 0.56 to 0.71 (2008–2019), an increase of 27%. According to the geographical area, the balanced level of allocation increased, suggesting an upward trend from 2008 to 2019, having a good development trend and room for improvement.
Table 7.
Evaluation value of balanced development degree (D) of medical and health resources allocation in Nanjing from 2008 to 2019.
Viewing from the regional level (Table 8, Figure 6), the balanced level of medical and health resources allocation in each region is sorted as “Jiangbei region > Ningnan region > main urban region”. From the perspective of population and geography, the Jiangbei region and Ningnan region are both featured with superior balanced development, the index value of the Jiangbei region has always been higher than 0.95 from 2008–2019, showing an excellent balance in medical and health resources allocation. While the development of Jiangning district in the Ningnan region presents a slight downward trend in the geographical dimension, the balanced development degree has decreased from superior balanced development in 2008 to good balanced development in 2019, leading to degradation in the balanced level of medical and health resources allocation in Ningnan region and the expansion of internal differences. Compared with the Jiangbei region and Ningnan region, the balanced development degree in the main urban region can be more complex. Viewing the population, the balanced development degree of the main urban region is lower than 0.90 from 2008 to 2009, indicating a good balanced development. Since 2010, the balanced development degree has fluctuated and increased as a whole, and the value has remained 0.94 above since 2014. In the geographical dimension, the main urban region presented a medium-level balanced development in 2008. The administrative districts within this region present four degrees of development from primary to superior, indicating a significant intra-difference. However, it maintained a good balanced development after 2008, and the intra difference was significantly narrowed in 2019.
Table 8.
Balanced development degree of medical and health resources allocation in three regions of Nanjing from 2008 to 2019.
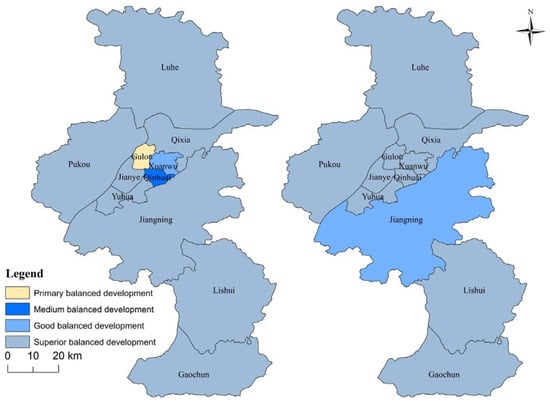
Figure 6.
Comparison of balanced development of various districts in 2008 (left) and 2019 (right). Note: Considering that the balanced development degree of medical and health resources allocation is inferior in the geographical dimension, this dimension is selected here for display, similarly hereinafter.
Viewing from each administrative district’s specific values and changing trends (Table 9), the differences among each district are apparent, which can be divided into four echelons. Concerning the balanced development degree of medical and health resources allocation, the first echelon includes Qixia, Yuhuatai and Jianye, all of which remained a fully balanced development state (D = 1) from 2008 to 2019. In particular, Yuhuatai has maintained a fully balanced state from 2009 to 2018, indicating that the allocation of medical and health resources is characterized by both equity and efficiency, and the overall balanced allocation level is superior. The second echelon includes Pukou, Luhe and Lishui, whose balanced development degrees are measured at 0.90–1.00, ranking in the superior balanced development. Then the third echelon involves Gaochun and Jiangning, both of which maintained a good or superior balanced development level. It is worth noting that the balanced allocation level in Jiangning presents a downward trend, from 2008 to 2015, it was a high-quality and balanced development, but the level of balanced development declined in 2016 and 2017, that is, its balanced allocation of medical and health resources level has deteriorated. Finally, Xuanwu, Qinhuai and Gulou are listed in the fourth echelon, whose balanced development degree is inferior to other administrative districts. The lowest value is mainly measured as 0.66 in Gulou, namely, a primary level.
Table 9.
Evaluation value of balanced development degree of medical and health resources allocation in various administrative districts of Nanjing from 2008 to 2019.
To promote the balanced allocation level of medical and health resources in each administrative district of Nanjing, the Boston matrix model was applied in this paper. The equity measurement Index (Theil index mean) is set as the x-axis, and the average efficiency of medical and health resources allocation in each administrative region from 2008 to 2019 is set as the y-axis. The boundary-value of each quadrant is selected as the overall average value of efficiency and equity to analyze various strategies for improving the balanced medical and health resources allocation level of administrative district in Nanjing (Figure 7). Many administrative districts are concentrated in the second quadrant where the average value of Theil index is lower than the overall average, and the efficiency is greater than the overall average, including Yuhuatai, Pukou and three other administrative districts, accounting for 45.45% of the total. These districts are featured with good equity and efficiency in allocating medical and health resources, presenting a superior level of balanced development. The administrative districts located in the third quadrant include Luhe, Jiangning, Xuanwu and Gaochun, whose mean value of Theil index and efficiency is less than the overall mean value, indicating a fine equity rather than efficiency. Improvement in the efficiency of medical and health resources allocation may help to promote balanced development. Qinhuai and Gulou are located in the fourth quadrant, indicating that the mean value of the Theil index in these two districts is greater than the overall mean value and the mean value of efficiency is less than that. That is, the equity and efficiency of medical and health resources allocation are both poor, leading to the low balanced development of medical and health resources allocation in the two districts. The fairness and efficiency should be improved at the same time.
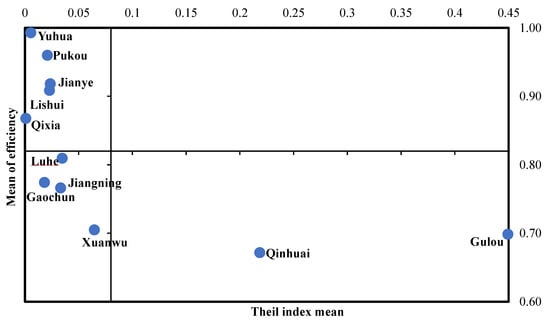
Figure 7.
Boston matrix of equity and efficiency of medical and health resources allocation in administrative districts of Nanjing.
5. Discussion
This paper uses the Theil index, DEA and balanced development model to measure the balanced allocation of medical and health resources in Nanjing from 2008 to 2019. It is found that the equity of medical and health resources allocation in Nanjing is insufficient, and the equity of medical and health resources allocation by geographical area is poor compared with that by population distribution. The study also found that from 2008 to 2019, the allocation efficiency of medical and health resources in Nanjing showed a trend of gradual improvement, but did not reach the effective DEA level, and there were significant regional differences. Finally, we found that under the premise of considering fairness and efficiency at the same time, Nanjing keeps a better balance of medical and health resources allocation level, especially in the population distribution configuration, the coordination of equity and efficiency two goal of medical and health resources allocation is higher, but under the geographical area of dimensions, the overall degree of balanced development has room to improve.
First, the equity of allocation of urban medical and health resources is still insufficient, but it has a gradual trend to be better. On the one hand, from 2008 to 2019, the total Theil index of medical and health resources allocation in Nanjing ranged from 0.04 to 0.06 in the dimension of population distribution. The total Theil index in geographical dimension fluctuated from 0.24 to 0.32, both of which deviated from zero, indicating that there is certain space for improvement in the equity of medical and health resources allocation in Nanjing. Compared with the dimension of population distribution, more improvement can be made in the geographical dimension. The conclusion concords with Jin et al. [31]. Zhang et al. [33] and Sun et al. [27] proposed that the phenomenon is related to the fact that documents issued by the Chinese government to optimize medical and health resources tend to emphasize the equity of allocation according to population rather than geography. For example, in relevant documents and statistics released by the government, the number of beds per thousand people rather than the number of beds per 10,000 square kilometers is taken as the priority of statistics on the allocation of health resources in China. In the dimension of population, the contribution rate of medical and health resource allocation difference in the main urban area, Jiangbei district and Ningnan district is higher, which is the main reason that hinders the mismatch between medical and health resources allocation and population distribution. In the geographical dimension, however, the contribution rate of regional differences is between 42% and 45%, which is not low and should also be paid attention to.
However, it is worth noting that the total Theil index in the population dimension decreased from 0.0524 in 2008 to 0.0518 in 2019, and the total Theil index in the geographical dimension decreased from 0.7240 to 0.5717. That is to say, the total Theil index in the two dimensions decreased by varying degrees, and the uneven allocation of medical and health resources in Nanjing had been improved to some extent. On the one hand, this is due to the government’s increasing investment in medical and health resources. For example, the number of beds per thousand people has increased from 3.66 in 2008 to 6.95 in 2019, and the number of health personnel per thousand people has increased from 7.09 in 2008 to 13.48 in 2019, which is conducive to improve the equity of medical and health resources allocation [57]. On the other hand, this may be due to the fact that, in 2015, China launched the hierarchical medical system at the national level, and Nanjing actively implemented the national medical and health system reform policy. In 2017, Nanjing issued the Implementation Opinions on Further Propelling the Building of the Hierarchical Diagnosis and Treatment System. It proposed that, by 2020, the city’s hierarchical diagnosis and treatment service capabilities will be comprehensively improved, the guarantee mechanism will be gradually improved and high-quality medical resources will be reasonable and effective sinking. In addition, the policy placed emphasis on vigorously promoting the joint construction and sharing of regional medical resources, which greatly promotes the equity of resource allocation.
In order to further improve the equity of medical and health resources allocation, promote equitable access to medical and health services, and enhance the driving force of sustainable development of medical and health undertakings, on the one hand, it is urgent to match the resource distribution considering the population and geographical characteristics of each region, that is, ensure the accessibility of medical and health services and realize the balance between supply and demand by regional planning. According to the data analysis, it can be seen that surplus medical and health resources are concentrated in Gulou, Qinhuai, Xuanwu and other districts. Therefore, in terms of regional planning, the government should lead the planning and strictly control the total amount of resources in each district, and narrow the regional differences by adjusting the stock and optimizing the increment, ensuring that high-quality medical and health resources are accessible throughout the city. On the other hand, in order to promote the realization of health care for all, strengthening the construction of grassroots medical and health service system should become an important starting point to improve the accessibility of medical and health resources. By accelerating the standardization of community-level medical and health institutions, improving the contract system for family doctors and promoting the hierarchical diagnosis and treatment system, the capacity and quality of community-level medical and health services will be fundamentally improved, so as to meet the needs of residents seeking medical treatment at home and realize a virtuous cycle of sustainable development of medical and health services.
Second, though the allocation efficiency of urban medical and health resources has been improved, it has not reached the effective level of DEA and there is a significant regional gap. From 2008 to 2019, the technical efficiency of medical and health resources allocation in Nanjing ranged from 0.770 to 0.890, with ample space for improvement. Its decomposition index, namely pure technical efficiency, remains at the level of 0.800, and the scale efficiency is higher than 0.900, approaching the optimal state. The index value indicates that the low pure technical efficiency mainly accounts for the low overall utilization efficiency of resources. Pure technical efficiency is mainly related to the level of medical and health resources management, reflecting the management philosophy and awareness of managers. Improper personnel allocation by managers, excessive investment in equipment but insufficient utilization, and poor capital operation will affect the pure technology of medical and health resources allocation efficiency [27]. In the future, it is imperative to improve the management methods of resource allocation and improve resource utilization to promote the efficiency of medical and health resources allocation in Nanjing. In addition, the overall efficiency of medical and health resources allocation in Nanjing is characterized by “Jiangbei region > Ningnan region > main urban region”. The average ten-year efficiency in the three regions is respectively measured as 0.885, 0.816 and 0.806. There is a degradation trend in the utilization of medical and health resources in the Ningnan region. Furthermore, there are significant differences in resource allocation efficiency among administrative districts in the main urban region. It can be seen that there is an obvious gap in the allocation efficiency of medical and health resources among urban regions, which is consistent with the research results of Hao et al. [58]. At the micro level, the mean values of the technical efficiency of medical and health resource allocation in the 11 administrative regions of Nanjing from 2008 to 2019 were significantly different. Yuhuatai District all achieved DEA efficiency from 2009 to 2018, with an average efficiency of 0.993, while Qinhuai District did not achieve DEA efficiency during the study period, and the efficiency level was low. Further investigation explains that resource redundancy in administrative districts with low efficiency lowers the overall efficiency level. For instance, in Jianye district of the main urban region, the average annual growth rates of health institutions and beds per 1000 population are respectively 7.71% and 7.09%, while the average annual growth rate of population survival rate is −0.01%, indicating that the input of resources has increased year by year but the increase of output is relatively insufficient and affects the improvement of efficiency.
On this basis, to improve the allocation efficiency of medical and health resources in Nanjing, differentiated efficiency promotion strategies should be implemented to promote the allocation of medical resources from extensive to refined, maximize the benefit of financial funds, fundamentally improve the vitality of sustainable development of medical and health undertakings. Concerning the main urban region with excessive medical and health resources, the government may integrate the existing resources, merge the medical institutions with low resource utilization rates or combine them based on the medical consortium. For urban regions with degraded efficiency and relatively backward technical level, it is suggested to allocate the limited funds to technological innovation and talent team construction, so as empower the operation of medical and health institutions and promote the improvement of efficiency. Additionally, the varied regions should establish a holistic view of sustainable development, strengthen communication and cooperation and promote learning with each other to improve the overall allocation efficiency of medical and health resources.
Third, under the premise of considering equity and efficiency, the balanced allocation level of medical and health resources in Chinese cities is generally fine, while there are specific improvements to be made in some regions. From 2008 to 2019, the evaluation value of the balanced development degree of medical and health resources allocation according to the population distribution in Nanjing is higher than 0.90, which presents a superior balanced development, while the value in the geographical dimension remains between 0.56 and 0.71, indicating a primary and medium balanced development. But the balanced allocation level under the two dimensions has increased by different degrees. The balanced allocation level in each region is sorted as “Jiangbei region > Ningnan region > main urban region”. It is not difficult to find that the equity and efficiency of the allocation of medical and health resources in the main urban area are not as good as those of the other two regions. Because the equity and efficiency of the allocation of medical and health resources are complementary to each other, the poor equity is not conducive to the improvement of efficiency, and the poor efficiency cannot promote higher equity, which in turn leads to poor allocation balance. There are noticeable differences among the administrative districts at the micro-level, which can be divided into four echelons. The average balanced development degrees of Gulou, Xuanwu and Qinhuai in the main urban region are 0.770, 0.88 and 0.84, with much room for improvement. Jiangning in Jiangnan region presents an obvious backward trend, from 0.94 in 2008 to 0.89 in 2019, which requires more engagement in strengthening the coordination of equity and efficiency of its resource allocation in the future.
The mismatch between the limited medical and health resources and the unlimited demand for health services is one of the deep contradictions of the sustainable development of medical and health undertakings. It is necessary to adjust the balance between equity and efficiency dynamically and rationally allocate medical and health resources by combining immediate and long-term interests, taking urban medical and health service planning as the guide and based on the changes of residents’ demand and disease spectrum [34]. The research of Cohen et al. [59] demonstrates that efficiency and equity can be combined through management that leads to improvements in efficiency and the health policy measures that reduce current inequities in the distribution of health resources. In this regard, to promote the balanced allocation level, full attention should be paid to the essence of resource allocation. Under the premise of equity and efficiency, the government may increase the investment of high-quality medical and health resources, and strengthen the incremental distribution of medical and health resources and the adjustment of stock. In particular, the allocation of medical and health resources in the fourth tier of administrative areas is poor, and they all belong to administrative areas in the main urban areas. It is worth noting that the GDP of the main urban area is the highest among the three regions (accounting for 53.28% of the whole city in 2019), which indicates that areas with better economic level should not only pay attention to the efforts in resource investment, but also pay attention to the mechanism of resource allocation. Liu et al.‘s study also reached a similar conclusion [20]. The government should determine the increment and supply of resources according to the functions and development needs of medical and health institutions, reducing the waste of resources and promoting the sustainable development of medical and health services.
6. Conclusions
In order to evaluate the balanced allocation of urban medical and health resources scientifically, some suggestions are put forward. Based on the theory and literature review, this paper builds an evaluation index system. Taking Nanjing city as an example, it evaluates and analyzes the equity and efficiency of medical and health resources allocation in 11 administrative regions of Nanjing city based on the Theil index and DEA-BCC model. Furthermore, by referring to the coupling coordination degree model and taking the fairness and efficiency of medical and health resource allocation as subsystems, the balanced development model is constructed to analyze the level of balanced medical and health resource allocation in urban areas from 2008 to 2019, and the main conclusions are as follows:
We found that the Nanjing medical and health resources allocation equity has improved, but the Theil index is still partial zero amplitude, there exists inequity in the medical and health resources allocation, and from the point of population dimension and geographical dimension, equity in population level is superior to the geographic level, namely, the area of medical and health resources allocation needs to further improve the planning level. From the perspective of the causes of differences, regional differences are more prominent, especially in the main urban areas. Under the two dimensions, there are both insufficient and excessive resource allocation in the main urban area, which is the main cause of the significant difference in internal allocation.
In terms of the allocation efficiency of medical and health resources, the allocation efficiency of medical and health resources in Nanjing is low, and the low pure technical efficiency is the main reason for the low overall utilization efficiency of resources. In terms of region, the efficiency level shows the characteristic of “Jiangbei District > Ningnan District > main urban area”. The utilization level of medical and health resources in the whole Ningnan District is degraded, and the efficiency level of each unit in the main urban area varies greatly. At the level of administrative regions, the mean values of technical efficiency of medical and health resource allocation in 11 administrative regions differed significantly during the study period, mainly because the mean values of pure technical efficiency differed greatly, while the mean values of scale efficiency tended to be consistent.
On the whole, although the equity and efficiency of medical and health resources in Nanjing are still insufficient, the overall allocation of medical and health resources is in a balanced development state, and the balanced development of population is better than that of geography. Under the population dimension, the evaluation value of balanced development degree of the whole city is higher than 0.90, which means that the two goals of equity and efficiency of medical resource allocation promote each other and are coordinately developed. However, the evaluation value of balanced development degree under the geographical area dimension remains between 0.56 and 0.71, which is the primary and intermediate balanced development. In other words, under the geographical area allocation, the coordination between equity and efficiency is poor, but there is a trend of improvement.
The advantage of this study is to investigate the allocation of medical and health resources from the urban level, and provide reference for the government to optimize the resource investment structure and improve the sustainability of the urban medical and health resource-based service system under the background of urbanization and population aging. In addition, by referring to the coupling coordination model, our research builds a balanced development model of medical and health resource allocation with fairness and efficiency as subsystems, which contributes to the research in the field of medical and health resource allocation evaluation.
In addition, this paper has two limitations. Firstly, based on the constructed model, this study analyzes the differences in the horizontal allocation of medical and health resources in urban regions. However, the balance of resource allocation among different levels of medical and health institutions from a vertical perspective was not involved, such as tertiary medical and health institutions and primary medical and health institutions. At the same time, the balanced allocation of different types of medical and health resources, such as doctors and nurses, has not been analyzed, and further research needs to be carried out to make a more comprehensive evaluation of the balanced allocation of medical and health resources. Secondly, the model and index system basically constructed in this paper evaluates and analyzes the balanced allocation of medical and health resources in Nanjing and its interior, but does not extend to the comparison of different cities, which needs to be further deepened in future research.
Author Contributions
Conceptualization, F.W. and W.C.; Data curation, W.C., L.L. and X.R.; Formal analysis, F.W. and W.C.; Funding acquisition, F.W.; Methodology, L.L. and Y.Q.; Supervision, F.W. and W.C.; Writing—original draft preparation, F.W. and X.R.; Writing—review and editing, F.W. and Y.Q. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by Humanity and Social Science Youth Foundation of Ministry of Education of China (19YJC630183), the General Project of Philosophy and Social Science Research in Colleges and Universities in Jiangsu Province (2019SJA0058), and the Key Project of Social Science Foundation in Jiangsu Province (20ZLA014).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to legal and privacy issues.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Zhu, D. Sustainability science: An Object-Process-Subject analytical framework. China Popul. Resour. Environ. 2016, 26, 1–9. [Google Scholar] [CrossRef]
- United Nations. Transforming Our World: The 2030 Agenda for Sustainable Development; United Nations: New York, NY, USA, 2014; p. 18. [Google Scholar]
- Zhang, Y. Analysis of Subjective Reasons and Influence Factors on Sustainable Development of Medical Car e Services. Chin. Health Econ. 2008, 8, 23–25. Available online: https://kns.cnki.net/kcms/detail/detail.aspx?dbcode=CJFD&dbname=CJFD2008&filename=WEIJ200808012&uniplatform=NZKPT&v=ztISZyzr_KWAq3ccrcznD_i4x-T3rRyaN6D20jgd_Cb1Ys4TS7HmSfC_6W5FQhKB (accessed on 10 April 2022).
- World Health Organization. Health Topics About Health Equity. 2020. Available online: http://www.who.int/topics/health_equity/en/ (accessed on 11 December 2021).
- Dlouhý, M. Measuring Geographic Inequalities: Dealing with Multiple Health Resources by Data Envelopment Analysis. Front. Public Health 2018, 6, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yip, W.C.; Hsiao, W.C.; Chen, W.; Hu, S.; Ma, J.; Maynard, A. Early appraisal of China’s huge and complex health-care reforms. Lancet 2012, 379, 833–842. [Google Scholar] [CrossRef]
- Jin, C.; Cheng, J.; Lu, Y.; Huang, Z.; Cao, F. Spatial inequity in access to healthcare facilities at a county: A case study of Deqing County, Zhejiang, China. Int. J. Equity Health 2015, 14, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, R.; Dong, S.; Zhao, Y.; Hu, H.; Li, Z. Assessing potential spatial accessibility of health services in rural China: A case study of Donghai county. Int. J. Equity Health 2013, 12, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, L.; Zhang, Z.; Lan, X. Impact of China’s Referral Reform on the Equity and Spatial Accessibility of Healthcare Resources: A Case Study of Beijing. Soc. Sci. Med. 2019, 235, 112386. [Google Scholar] [CrossRef]
- Cheng, G.; Zeng, X.; Duan, L.; Lu, X.; Sun, H.; Jiang, T.; Li, Y. Spatial difference analysis for accessibility to high level hospitals based on travel time in Shenzhen, China. Habitat Int. 2016, 53, 485–494. [Google Scholar] [CrossRef] [Green Version]
- Jiang, S.; Gu, Y.; Yang, F.; Wu, T.; Wang, H.; Cutler, H.; Zhang, L. Tertiary hospitals or community clinics? An enquiry into the factors affecting patients’ choice for healthcare facilities in urban China. China Econ. Rev. 2020, 63, 101538. [Google Scholar] [CrossRef]
- Wu, F.; Hu, Q.; Zhu, C.; Wang, H.; Yu, Q.; Sun, H. New Structural Economic Analysis of Anti-COVID-19 Pandemic Model of BEST Region. Int. J. Environ. Res. Public Health 2021, 18, 7822. [Google Scholar] [CrossRef]
- XinHua Net. The Fourteenth Five-Year Plan for National Economic and Social Development of the People’s Republic of China and the Outline of Long-Term Goals for 2035. 2021. Available online: http://www.xinhuanet.com/2021-03/13/c_1127205564.htm (accessed on 14 December 2021).
- Culyer, A.J. The bogus conflict between efficiency and vertical equity. Health Econ. 2006, 5, 1155–1158. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Zhou, L.; Antwi, H.A.; Chen, X. Evaluation of health resource utilization efficiency in community health centers of Jiangsu Province, China. Hum. Resour. Health 2018, 16, 13. [Google Scholar] [CrossRef] [PubMed]
- Shinjo, D.; Aramaki, T. Geographic distribution of healthcare resources, healthcare service provision, and patient flow in Japan: A cross sectional study. Soc. Sci. Med. 2012, 75, 1954–1963. [Google Scholar] [CrossRef] [PubMed]
- Czypionka, T.; Kraus, M.; Mayer, S.; Röhrling, G. Efficiency, ownership, and financing of hospitals: The case of Austria. Health Care Manag. Sci. 2014, 17, 331–347. [Google Scholar] [CrossRef] [PubMed]
- Horev, T.; Pesis-Katz, I.; Mukamel, D.B. Trends in geographic disparities in allocation of health care resources in the US. Health Policy 2004, 68, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Xu, Y.; Ren, J.; Sun, L.; Liu, C. Inequality in the distribution of health resources and health services in China: Hospitals versus primary care institutions. Int. J. Equity Health 2017, 16, 42. [Google Scholar] [CrossRef] [Green Version]
- Liu, W.; Liu, Y.; Twum, P.; Li, S. National equity of health resource allocation in China: Data from 2009 to 2013. Int. J. Equity Health 2016, 15, 68. [Google Scholar] [CrossRef] [Green Version]
- Cetin, V.R.; Bahce, S. Measuring the efficiency of health systems of OECD countries by data envelopment analysis. Appl. Econ. 2016, 48, 3497–3507. [Google Scholar] [CrossRef]
- Top, M.; Konca, M.; Sapaz, B. Technical efficiency of healthcare systems in African countries: An application based on data envelopment analysis. Health Policy Technol. 2020, 9, 62–68. [Google Scholar] [CrossRef]
- Retzlaff-Roberts, D.; Chang, C.F.; Rubin, R.M. Technical efficiency in the use of health care resources: A comparison of OECD countries. Health Policy 2004, 69, 55–72. [Google Scholar] [CrossRef]
- De, P.; Dhar, A.; Bhattacharya, B.N. Efficiency of Health Care System in India: An Inter-State Analysis using DEA Approach. Soc. Work Public Health 2012, 27, 482–506. [Google Scholar] [CrossRef] [PubMed]
- Yi, M.; Peng, J.; Zhang, L.; Zhang, Y. Is the allocation of medical and health resources effective? Characteristic facts from regional heterogeneity in China. Int. J. Equity Health 2020, 19, 89. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Wu, F.; Chen, W.; Zhu, C.; Huang, T. Research on Urban Medical and Health Services Efficiency and Its Spatial Correlation in China: Based on Panel Data of 13 Cities in Jiangsu Province. Healthcare 2021, 9, 1167. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Luo, H. Evaluation on equality and efficiency of health resources allocation and health services utilization in China. Int. J. Equity Health 2017, 16, 127. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Zhao, L.; Cui, Z.; Wang, Y. Study on Equity and Efficiency of Health Resources and Services Based on Key Indicators in China. PLoS ONE 2015, 10, e0144809. [Google Scholar] [CrossRef] [Green Version]
- Bureau of Statistics of NanJing. Bulletin of the Seventh National Census of Nanjing. 2021. Available online: http://tjj.nanjing.gov.cn/bmfw/njsj/202105/t20210524_2945571.html (accessed on 15 December 2021).
- Murray, C.J.L.; Frenk, J. Health metrics and evaluation: Strengthening the science. Lancet 2008, 371, 1191–1199. [Google Scholar] [CrossRef]
- Jin, J.; Wang, J.; Ma, X.; Wang, Y.; Li, R. Equality of Medical Health Resource Allocation in China Based on the Gini Coefficient Method. Iran J. Public Health 2015, 44, 445–457. [Google Scholar]
- Peng, L.; Liu, Z. Empirical Study on Equalization of Public Library Services in China: Analysis Based on the Theil Index. Library 2019, 5, 47–56. [Google Scholar]
- Zhang, Y.; Wang, Q.; Jiang, T.; Wang, J. Equity and efficiency of primary health care resource allocation in mainland China. Int. J. Equity Health 2018, 17, 140. [Google Scholar] [CrossRef] [Green Version]
- Ding, J.; Hu, X.; Zhang, X.; Shang, L.; Yu, M.; Chen, H. Equity and efficiency of medical service systems at the provincial level of China’s mainland: A comparative study from 2009 to 2014. BMC Public Health 2018, 18, 214. [Google Scholar] [CrossRef]
- Zhou, D.; Yuan, J. Efficient and equitable of health resources allocation in China: Problem discovery and policy path. Chin. J. Health Policy 2018, 11, 64–71. Available online: https://kns.cnki.net/kcms/detail/detail.aspx?dbcode=CJFD&dbname=CJFDLAST2018&filename=ZGWZ201803012&uniplatform=NZKPT&v=lu05uyFogcOG1S2-dCo6CtHNQON4ls4TM-aBD8ovYIaBzDaA40piT6xVm4197SS3 (accessed on 12 April 2022).
- Maynard, A. Rationing health care: An exploration. Health Policy 1999, 49, 5–11. [Google Scholar] [CrossRef]
- Reckers-Droog, V.T.; Van Exel, N.J.A.; Brouwer, W.B.F. Looking back and moving forward: On the application of proportional shortfall in healthcare priority setting in the Netherlands. Health Policy 2018, 122, 621–629. [Google Scholar] [CrossRef] [PubMed]
- Theil, H. Information and Economic Theory; North Holland Publishing Company: Amsterdam, The Netherlands, 1967; pp. 1–488. [Google Scholar]
- Anand, S. Measuring Health Workforce Inequalities: Methods and Application to China and India; World Health Organization: Geneva, Switzerland, 2010.
- Qi, Y.; Qin, Y. Study on the relationship between public service equalization and economic development imbalance in urban agglomerations. Stat. Decis. 2020, 36, 77–81. [Google Scholar] [CrossRef]
- Shorrocks, A.F. The Class of Additively Decomposable Inequality Measure. Econometrica 1980, 3, 613–625. [Google Scholar] [CrossRef] [Green Version]
- Tao, Y.; Henry, K.; Zou, Q.; Zhong, X. Methods for measuring horizontal equity in health resource allocation: A comparative study. Health Econ. Rev. 2014, 4, 10. [Google Scholar] [CrossRef] [Green Version]
- Yang, Z.; Sun, X. The Research about the Arrangement of Basic Medical Resources and Medical Service Utilization in Shanghai. J. Gansu Adm. Inst. 2016, 5, 78–90, 127. [Google Scholar]
- Gao, J.; Han, Y.; Wang, Y.; Zhang, Q. Reflections on Space of Medical Service for Urban Residents and its Planning based on Individual Behavior: A Case Study of Central District of Guangzhou. Urban Space Stud. 2017, 41, 46–52. [Google Scholar]
- Neri, M.; Cubi-Molla, P.; Cookson, G. Approaches to Measure Efficiency in Primary Care: A Systematic Literature Review. Appl. Health Econ. Health Policy 2022, 20, 19–33. [Google Scholar] [CrossRef]
- Charnes, A.; Cooper, W.W.; Rhodes, E. Measuring the Efficiency of Decision Making Units. Eur. J. Oper. Res. 1978, 2, 429–444. [Google Scholar] [CrossRef]
- Banker, R.D.; Charnes, A.; Cooper, W.W. Some Models for Estimating Technical and Scale in Efficiencies in Data Envelopment analysis. Manag. Sci. 1984, 30, 1078–1092. [Google Scholar] [CrossRef] [Green Version]
- González-de-Julián, S.; Barrachina-Martínez, I.; Vivas-Consuelo, D.; Bonet-Pla, Á.; Usó-Talamantes, R. Data Envelopment Analysis Applications on Primary Health Care Using Exogenous Variables and Health Outcomes. Sustainability 2021, 13, 1337. [Google Scholar] [CrossRef]
- Alpandi, R.M.; Kamarudin, F.; Wanke, P.; Muhammad Salam, M.S.; Iqbal Hussain, H. Energy Efficiency in Production of Swiftlet Edible Bird’s Nest. Sustainability 2022, 14, 5870. [Google Scholar] [CrossRef]
- Li, Y.; Li, Y.; Zhou, Y.; Shi, Y.; Zhu, X. Investigation of a coupling model of coordination between urbanization and the environment. J. Environ. Manag. 2012, 98, 127–133. [Google Scholar] [CrossRef]
- Fan, Y.; Fang, C.; Zhang, Q. Coupling coordinated development between social economy and ecological environment in Chinese provincial capital cities-assessment and policy implications. J. Clean Prod. 2019, 229, 289–298. [Google Scholar] [CrossRef]
- Hu, M.; Tao, C.; Zhou, H. The Influence of Industrial Structure Upgrade on Coupling and Coordinated Development—Empirical Analysis from Chinese Pharmaceutical Manufacturing and Pharmaceutical Service Industries. Front. Public Health 2021, 9, 722006. [Google Scholar] [CrossRef]
- Li, W.; Wang, Y.; Xie, S.; Cheng, X. Coupling coordination analysis and spatiotemporal heterogeneity between urbanization and ecosystem health in Chongqing municipality, China. Sci. Total Environ. 2021, 791, 148311. [Google Scholar] [CrossRef]
- Dong, G.; Ge, Y.; Zhu, W.; Qu, Y.; Zhang, W. Coupling Coordination and Spatiotemporal Dynamic Evolution Between Green Urbanization and Green Finance: A Case Study in China. Front. Environ. Sci. 2021, 8, 621846. [Google Scholar] [CrossRef]
- Cui, X. Population Urbanization and Land Urbanization in Ethnic Minority Areas: Disequilibrium and Spatial Heterogeneity. China Popul. Resour. Environ. 2014, 24, 63–72. [Google Scholar] [CrossRef]
- Fang, Z. Research on the Optimization of Medical Service Facility Allocation in Small Towns in Wuhan from the Perspective of Supply and Demand. Master’s Thesis, Huazhong University of Science and Technology, Wuhan, China, May 2017. [Google Scholar]
- Dong, E.; Xu, J.; Sun, X.; Xu, T.; Zhang, L.; Wang, T. Differences in regional distribution and inequality in health-resource allocation on institutions, beds, and workforce: A longitudinal study in China. Arch. Public Health 2021, 79, 78. [Google Scholar] [CrossRef]
- Hao, Y.; Li, Z.; Ma, Q.; Fu, X.; Sun, C.Q. Fairness and efficiency analysis of health resource allocation in Shenzhen. Med. Soc. 2019, 32, 44–47. [Google Scholar] [CrossRef]
- Cohen, J.; Burg, E. On the possibility of a positive-sum game in the distribution of health care resources. J. Med. Philos. 2003, 28, 327–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).