
Nurses’ Work Environment during the COVID-19 Pandemic in a Person-Centred Practice—A Systematic Review

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
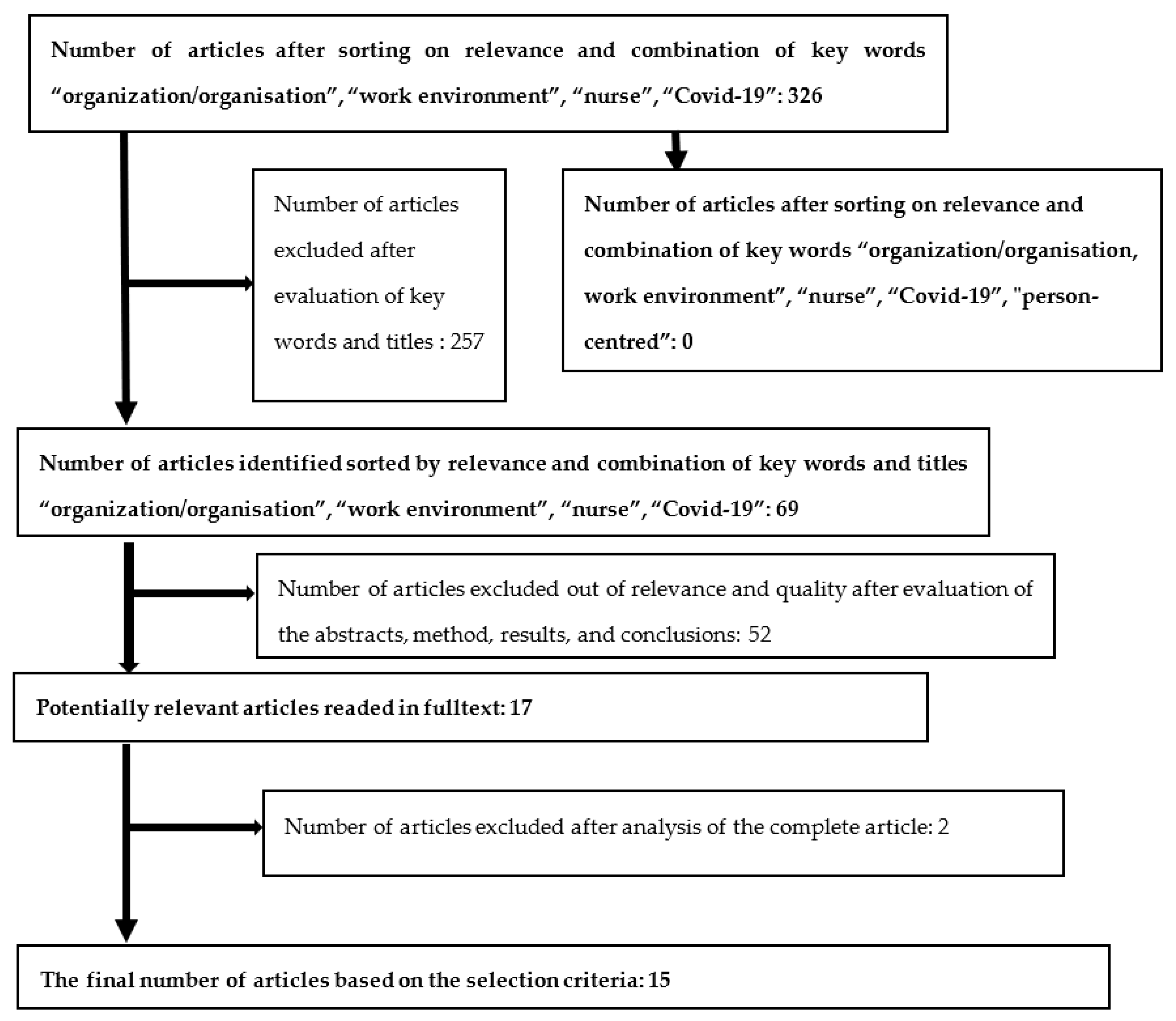
2.1. Systematic Review
- i.
- empirical investigations
- ii.
- nurse was the interested profession for this systematic review, and therefore nurses had to be investigated
- iii.
- the nurses should have worked during the COVID-19 pandemic
- iv.
- the nurses work environment situation was the topic
- v.
- the organisation of the work situation and work environment was also of importance
- vi.
- due to the increased importance of person-centred the care, the word person-centred was important
- vii.
- the article needs to be a full text paper
- viii.
- the published or accepted articles need to have been processed by peer-review
- ix.
- published in scientific journals
- x.
- in English language
- xi.
- as the authors of this paper is from Sweden paper published in Nordic languages was also stated to be possible for inclusion.
- i.
- articles that did not apply to the aim of the study, i.e., nurses work situation during the COVID-19 pandemic
- ii.
- review papers or other publications that not in first line handle performed empirical investigations
- iii.
- literature that was not scientifically published
- iv.
- articles that were not available in full text
- v.
- articles published in another language than English or Nordic language.
2.2. Analysis Method
- ➢
- The health effects of the work environment, which include the following areas of determination:
- (1)
- Self-rated health, diagnoses, and diverse physical and mental health functionality in work,
- (2)
- physical work environment with unilateral movements, heavy lifting, risk of accidents, climate, chemical exposure, and risk of contagion,
- (3)
- mental work environment; stress and fatigue syndrome, threats, and violence
- (4)
- working hours, work pace, and possibility of recuperation during and between work shifts.
- ➢
- Financial incentives are associated with society’s control of various financial carrots and sticks, such as through the social insurance system. Financial incentives include the following determinant area:
- (5)
- The personal financial situation’s effects on individuals’ needs and willingness to work.
- ➢
- Relationships, social support, and participation, i.e., attitudes in the social context in which the individual finds himself/herself, whether the individual feels included or excluded in the group and receives sufficient social support from the environment when needed, include the areas of determination:
- (6)
- The effects of the personal social environment, with family, friends, and leisure context, and
- (7)
- the social work environment with leadership, discrimination, and the significance of the employment relationship context for individuals’ work.
- ➢
- Execution of tasks and activities, relate to individual and instrumental support and include the following areas of determination:
- (8)
- Motivation, appreciation, satisfaction, and stimulation in work tasks, and
- (9)
- knowledge, competence, and the importance of competence development for the individual’s work.
3. Results
3.1. Inclusion and Exclusion Result
3.2. Result Overview of the Articles
3.3. Analyses of the Included Articles
3.3.1. Determinant Sphere: A: The Health Effects of the Work Environment
- (1)
- the employees own self-rated health and diagnoses:
- (2)
- physical work environment at the workplace:
- (3)
- mental work environment at the workplace:
- (4)
- working hours, work pace, time for recuperation:
3.3.2. Determinant Sphere: B: Economics and Financial Incentives
- (5)
- financial situation:
3.3.3. Determinant Sphere: C: Relationships, Social Support, and Participation
- (6)
- personal social environment outside work:
- (7)
- work social environment at the workplace:
3.3.4. Determinant Sphere: D: Execution of Tasks and Activities Relate to Individual and Instrumental Support
- (8)
- stimulation, appreciation, and motivation within work tasks:
- (9)
- competence, skills, and possibility to knowledge development in work
4. Discussion
- Health and diagnoses
- Physical work environment
- Mental work environment
- Working hours, work pace, time for recuperation
- Financial situation
- Personal social environment
- Work social environment
- Stimulation, appreciation, and motivation
- Competence, skills, and possibility to knowledge development
- Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 14 January 2022).
- WHO. Protecting Workers’ Health; World Health Organization: Geneva, Switzerland, 2019; Available online: https://www.who.int/en/news-room/fact-sheets/detail/protecting-workers’-health (accessed on 15 November 2021).
- WHO. Healthy Workplaces: A Model for Action for Employers, Workers, Policymakers, and Practitioners; World Health Organization: Geneva, Switzerland, 2019; Available online: https://www.who.int/publications-detail/healthy-workplaces-a-model-for-action (accessed on 15 November 2021).
- WHO. Mental Disorders; World Health Organization: Geneva, Switzerland, 2019; Available online: https://www.who.int/mental_health/management/en/ (accessed on 15 November 2021).
- Shone, E. More Than 850 Health and Social Care Workers Have Died of Covid in England and Wales Since the Pandemic Began; The Scotsman: Edinburgh, Scotland, 2021; Available online: https://www.scotsman.com/health/coronavirus/more-850-health-and-social-care-workers-have-died-covid-england-and-wales-pandemic-began-3114202 (accessed on 27 January 2021).
- European Network for Workplace Health Promotion. The Case for WHP; European Network for Workplace Health Promotion: Perugia, Italy, 2018; Available online: https://www.enwhp.org/?i=portal.en.the-case-for-whp (accessed on 25 January 2022).
- UN Sustainable Development Goals. Available online: https://www.un.org/en/academic-impact/page/sustainable-development-goals (accessed on 7 February 2022).
- Nilsson, K. A sustainable working life for all ages—The swAge-model. Appl. Ergon. 2020, 86, 103082. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, K.; Nilsson, E. Organisational Measures and Strategies for a Healthy and Sustainable Extended Working Life and Employability—A Deductive Content Analysis with Data Including Employees, First Line Managers, Trade Union Representatives and HR-Practitioners. Int. J. Environ. Res. Public Health 2021, 18, 5626. [Google Scholar] [CrossRef] [PubMed]
- SwAge-Model. Available online: www.swage.org/en.html (accessed on 10 January 2022).
- Nilsson, K. Attraktivt och Hållbart Arbetsliv på Människors Villkor—Arbete, Hälsa och LEDARSKAP Med SwAge-Modellen i Teori och Praktik; [Attractive and sustainable working life on human terms—Work, health, and leadership with the SwAge model in theory and practice]; Studentlitteratur: Lund, Sweden, 2021; pp. 1–420. [Google Scholar]
- McCormack, B.; McCance, T.V. Development of a framework for person-centred nursing. J. Adv. Nurs. 2006, 56, 472–479. [Google Scholar] [CrossRef] [PubMed]
- McCormack, B.; McCance, T. Person-Centred Practice in Nursing and Healthcare: Theory and Practice; Wiley Blackwell: Chichester, UK, 2017. [Google Scholar]
- Öhlén, J.; Friberg, F. (Eds.) Person. In Omvårdnadensgrunder. Perspektiv och Förhållningssätt, 3rd ed.; Studentlitteratur: Lund, Sweden, 2019; pp. 313–336. [Google Scholar]
- McCabe, C. Nurse-patient communication: An exploration of patients’ experiences. J. Clin. Nurs. 2004, 13, 41–49. [Google Scholar] [CrossRef]
- Sjögren, K.; Lindkvist, M.; Sandman, P.O.; Zingmark, K.; Edvardsson, D. To what extent is the work environment of staff related to person-centred care? A cross-sectional study of residential aged care. J. Clin. Nurs. 2015, 24, 1310–1319. [Google Scholar] [CrossRef]
- Gough, D.; Oliver, S.; Thomas, J. An Introduction to Systematic Reviews; SAGE Publications Ltd.: London, UK, 2017. [Google Scholar]
- Pursell, E.; McCrae, N. How to Perform a Systematic Literature Review—A Guide for Healthcare Researchers, Practitioners, and Students; Springer Nature Switzerland AG: Cham, Switzerland, 2020. [Google Scholar]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (Updated February 2021); Cochrane: London, UK, 2021; Available online: www.training.cochrane.org/handbook (accessed on 2 November 2021).
- PRISMA. Available online: www.prisma-statement.org/ (accessed on 21 January 2022).
- Khan, K.S.; Kunz, R.; Kleijnen, J.; Antes, G. Five steps to conducting a systematic review. J. R. Soc. Med. 2003, 96, 118–121. [Google Scholar] [CrossRef]
- Assarroudi, A.; Heshmati Nabavi, F.; Armat, M.R.; Ebadi, A.; Vaismoradi, M. Directed qualitative content analysis: The description and elaboration of its underpinning methods and data analysis process. J. Res. Nurs. 2018, 23, 42–55. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, H.-F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- Da Rosa, P.; Brown, R.; Pravecek, B.; Carotta, C.; Garcia, A.S.; Carson, P. Factors associated with nurses’ emotional distress during the COVID-19 pandemic. Appl. Nurs. Res. 2021, 62, 151502. [Google Scholar] [CrossRef]
- Bergman, L.; Falk, A.C.; Wolf, A.; Larsson, I.M. Registered nurses’ experiences of working in the intensive care unit during the COVID-19 pandemic. Nurs. Crit. Care 2021, 26, 467–475. [Google Scholar] [CrossRef]
- George, E.K.; Weiseth, A.; Edmonds, J.K. Roles and Experiences of Registered Nurses on Labor and Delivery Units in the United States during the COVID-19 Pandemic. J. Obstet. Gynecol. Neonatal Nurs. 2021, 50, 742–752. [Google Scholar] [CrossRef] [PubMed]
- Gago-Valiente, F.J.; Mendoza-Sierra, M.I.; Moreno-Sánches, E.; Arbinaga, F.; Segura-Camacho, A. Emotional Exhaustion, Depersonalization, and Mental Health in Nurses from Huelva: A Cross-Cutting Study during the SARS-CoV-2 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 7860. [Google Scholar] [CrossRef] [PubMed]
- Firew, T.; Sano, E.D.; Lee, J.W.; Flores, S.; Lang, K.; Salman, K. Protecting the front line: A cross-sectional survey analysis of the occupational factors contributing to healthcare workers’ infection and psychological distress during the COVID-19 pandemic in the USA. BMJ Open 2020, 10, e042752. [Google Scholar] [CrossRef]
- Galanis, P.; Petrogianni, E.; Vraka, I.; Konstantakopoulou, O.; Siskou, O.; Bilali, A. Fear of COVID-19 among Nurses in Mobile COVID-19 Testing Units in Greece. Int. J. Caring Sci. 2021, 14, 802–810. [Google Scholar]
- Suryavanshi, N.; Kadam, A.; Dhumal, G.; Nimkar, S.; Mave, V.; Gupta, A. Mental health, and quality of life among healthcare professionals during the COVID-19 pandemic in India. Brain Behav. 2020, 10, e01837. [Google Scholar] [CrossRef] [PubMed]
- Norful, A.A.; Rosenfeld, A.; Schroeder, K.; Travers, J.L.; Aliyu, S. Primary drivers and psychological manifestations of stress in frontline healthcare workforce during the initial COVID-19 outbreak in the United States. Gen. Hosp. Psychiatry 2021, 69, 20–26. [Google Scholar] [CrossRef]
- Giusino, D.; De Angelis, M.; Mazzetti, G.; Christennsen, M.; Innstrand, S.T.; Faiulo, I.R. “We All Held Our Own”: Job Demands and Resources at Individual, Leader, Group, and Organizational Levels During COVID-19 Outbreak in Health Care. A Multi-Source Qualitative Study. Workplace Health Saf. 2021, 70, 6–16. [Google Scholar] [CrossRef]
- van der Goot, W.E.; Duvivier, R.J.; Van Yperen, N.W.; de Carvalho-Filho, M.A.; Noot, K.E.; Ikink, R. Psychological distress among frontline workers during the COVID-19 pandemic: A mixed-methods study. PLoS ONE 2021, 16, e0255510. [Google Scholar] [CrossRef]
- Thomas, T.A.; Davis, F.D.; Kumar, S.; Thammasitboon, S.; Rushton, C.H. COVID-19 and Moral Distress: A Pediatric Critical Care Survey. Am. J. Crit. Care 2021, 30, e80–e98. [Google Scholar] [CrossRef]
- Sheppard, K.N.; Runk, B.G.; Maduro, R.S.; Fancher, M.; Mayo, A.N.; Wilmoth, D.D. Nursing moral distress and intent to leave employment during the COVID-19 pandemic. J. Nurs. Care Qual. 2021, 37, 28–34. [Google Scholar] [CrossRef]
- dos Santos, J.L.G.; Balsanelli, A.P.; Freitas, E.O.; Menegon, F.H.A.; Carneiro, I.A.; Lazzari, D.D. Working environment of hospital nurses during the COVID-19 pandemic in Brazil. Int. Nurs. Rev. 2021, 68, 228–237. [Google Scholar] [CrossRef] [PubMed]
- Diomidous, M. Sleep and Motion Disorders of Physicians and Nurses Working in Hospitals Facing the Pandemic of COVID 19. Med. Arch. 2020, 74, 210–215. [Google Scholar] [CrossRef]
- Jo, S.; Kurt, S.; Bennet, J.A.; Mayer, K.; Pituch, K.A.; Simpson, V. Nurses’ resilience in the face of coronavirus (COVID-19): An international view. Nurs. Health Sci. 2021, 23, 646–657. [Google Scholar] [CrossRef] [PubMed]
- Ferraro, M.; Piccioni, L.O.; Malzanni, G.E.; Bussi, M. Personal Protective Equipment (PPE) in COVID-19 pandemic related symptoms and adverse reactions in healthcare workers and general population. J. Occup. Environ. Med. 2021, 63, e80–e85. [Google Scholar]
- Hong, S.; Ai, M.; Xu, X.; Wang, W.; Chen, J.; Zhang, Q.; Wang, L.; Kuang, L. Immediate psychological impact on nurses working at 42 government-designated hospitals during COVID-10 outbreak in China: A cross-sectional study. Nurs. Outlook 2021, 69, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Hall, L.H.; Johnson, J.; Watt, I.; Tsipa, A.; O’Connor, D.B. Healthcare staff well-being, burnout, and patient safety: A systematic review. PLoS ONE 2016, 11, e0159015. [Google Scholar] [CrossRef]
- Young, K.P.; Kolcz, D.L.; O’Sullivan, D.M.; Ferrand, J.; Fried, J.; Robinson, K. Healthcare workers’ mental health and quality of life during COVID-19: Results from a mid-pandemic national survey. Psychiatr. Serv. 2021, 72, 122–128. [Google Scholar] [CrossRef]
- ICN. Available online: https://www.icn.ch/news/covid-effect-renewed-interest-nursing-careers-undermined-discontent-and-disputes-over-pay (accessed on 19 January 2022).
- Koren, A.; Arif Ul Alam, M.; Koneru, S.; De Vito, S.; Abdallah, L.; Liu, B. Nursing perspectives on the impact of COVID-19: Social media content analysis. JMIR Form. Res. 2021, 5, e31358. [Google Scholar] [CrossRef]
- Hu, D.; Kong, Y.; Li, W.; Han, Q.; Zhang, X.; Zhu, L.X. Frontline nurses’ burnout, anxiety, depression and fear statuses and their associated factors during the COVID-19 outbreak in Wuhan, China: A large cross-sectional study. E Clin. Med. 2020, 24, 100424. [Google Scholar]
- McCormack, B.; Karlsson, B.; Dewing, J.; Lerdal, A. Exploring person-centredness: A qualitative meta-synthesis of four studies. Scand. J. Caring Sci. 2010, 24, 620–634. [Google Scholar] [CrossRef]
- Uhlman, K.; Amaladoss, N.; Lentz, V. From languishing to flourishing: The impact of the Covid-19 pandemic. Psychiatr. Times 2021, 38, 8–13. [Google Scholar]
- SCB. Trender Och Prognoser: Om Utbildning Och Arbetsmarknad; Statistics Sweden: Örebro, Sweden, 2014. [Google Scholar]
- Lake, E.T.; Narva, A.M.; Holland, S.; Smith, J.G.; Cramer, E.; Fitzpatrick Rosenbaum, K.E.; French, R.; Clark, R.S.; Rogowski, J.A. Hospital nurses’ moral distress and mental health during COVID-19. J. Adv. Nurs. 2022, 78, 799–809. [Google Scholar] [CrossRef] [PubMed]
- Ngan, K.; Drebit, S.; Siow, S. Risks and causes of musculoskeletal injuries among healthcare workers. Occup. Med. 2010, 60, 389–394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zuzelo, P.R. Making do during a pandemic: Morally distressing and injurious events. Holist. Nurs. Pract. 2020, 34, 259–261. [Google Scholar] [CrossRef] [PubMed]
- Chou, H.Y.; Hecker, R.; Martin, A. Predicting nurses’ well-being from job demands and resources: A cross-sectional study of emotional labour. J. Nurs. Manag. 2012, 20, 502–511. [Google Scholar] [CrossRef]
- Li, H.; Cheng, B.; Zhu, X.P. Quantification of burnout in emergency nurses: A systematic review and meta-analysis. Int. Emerg. Nurs. 2018, 39, 46–54. [Google Scholar] [CrossRef]
- ANA. American Nurses Association 2020. Available online: www.nursingworld.org (accessed on 25 January 2022).
- ICN. Available online: https://www.icn.ch/news/rapid-development-covid-resources-usa (accessed on 19 January 2022).
- Magner, C.; Greenberg, N.; Timmins, F.; O’Doherty, V.; Lyons, B. The psychological impact of COVID-19 on frontline healthcare workers ‘From heartbreak to hope’. J. Clin. Nurs. 2021, 30, e53–e55. [Google Scholar] [CrossRef]
- Chen, I.-H.; Brown, R.; Bowers, B.J.; Chang, W.-Y. Job demands and job satisfaction in latent groups of turnover intention among licensed nurses in Taiwan Nursing Homes. Res. Nurs. Health 2015, 38, 342–356. [Google Scholar] [CrossRef]
- Broetje, S.; Jenny, G.J.; Bauer, G.F. The Key Job Demands and Resources of Nursing Staff: An Integrative Review of Reviews. Front. Psychol. 2020, 11, 84. [Google Scholar] [CrossRef]
- Sagherian, K.; Steege, L.M.; Cobb, S.J.; Cho, H. Insomnia, fatigue, and psychosocial well-being during Covid-19 pandemic: A cross-sectional survey of hospital nursing staff in the United States. J. Clin. Nurs. 2020, 1–14. [Google Scholar] [CrossRef]
- Boulos, M.I.; Murray, B.J. Current evaluation and management of excessive daytime sleepiness. Can. J. Neorol. Sci. 2010, 37, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Luo, C.; Liu, S.; Chen, W.; Liu, Y.; Li, Y.; Du, Y.; Zou, H.; Pan, J. Excessive daytime sleepiness in general hospital nurses: Prevalence, correlates, and its association with adverse events. Sleep Breath. 2019, 23, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Duffy, J.F.; Willson, H.J.; Wang, W.; Czeisler, C.A. Healthy older adults better tolerate sleep deprivation than young adults. J. Am. Geriatr. Soc. 2009, 57, 1245–1251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellanti, F.; Lo Buglio, A.; Capuano, E.; Dobrakowski, M.; Kaspeczyk, A.; Kasperczyk, S.; Ventriglio, A.; Vendemiale, G. Factors related to nurses’ burnout during the first wave of Coronavirus Disease-19 in a university hospital in Italy. Int. J. Environ. Res. Public Health 2021, 18, 5051. [Google Scholar] [CrossRef] [PubMed]
- Riedl, E.M.; Thomas, J. The moderating role of work pressure on the relationships between emotional demands and tension, exhaustion, and work engagement: An experience sampling study among nurses. Eur. J. Work Organ. Psychol. 2019, 28, 414–429. [Google Scholar] [CrossRef]
- De Wijn, A.N.; van der Doef, M.P. Patient-related stressful situations and stress-related outcomes in emergency nurses: A cross-sectional study on the role of work factors and recovery during leisure time. Int. J. Nurs. Stud. 2020, 107, 103579. [Google Scholar] [CrossRef]
- Van Veldhoven, M.J.; Sluiter, J.K. Work-related recovery opportunities: Testing scale properties and validity in relation to health. Int. Arch. Occup. Environ. Health 2009, 82, 1065–1075. [Google Scholar] [CrossRef]
- Kinman, G.; Teoh, K.; Harriss, A. The Mental Health and Wellbeing of Nurses and Midwives in the United Kingdom; Society of Occupational Medicine: London, UK, 2020. [Google Scholar]
- Törnquist Agosti, M.; Bringsén, Å.; Andersson, I. The complexity of resources related to work-life balance and well-being—A survey among municipality employees in Sweden. Int. J. Hum. Res. Manag. 2017, 28, 2351–2374. [Google Scholar] [CrossRef]
- Bringsén, Å.; Sjöbeck, J.; Petersson, P. Nursing staff’s experience of appearance issues in various nursing situations. BMC Nurs. 2021, 20, 204. [Google Scholar] [CrossRef]
- Yayla, A.; Ilgin, V.E. The relationship of nurses’ psychological well-being with their corona phobia and work-life balance during the COVID-10 pandemic: A cross-sectional study. J. Clin. Nurs. 2021, 30, 3153–3162. [Google Scholar] [CrossRef]
- Holland, P.; Long Tham, T.; Sheehan, C.; Cooper, B. The impact of perceived workload on nurse satisfaction with work-life balance and intention to leave the occupation. Appl. Nurs. Res. 2019, 49, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Crisp, N. The art of medicine: Human flourishing in a health-creating society. Lancet 2021, 397, 1054–1055. [Google Scholar] [CrossRef]
- Ness, M.M.; Saylor, J.; Di Fusco, L.A.; Evans, K. Leadership, professional quality of life and moral distress during COVID-19: A mixed methods approach. J. Nurs. Manag. 2021, 29, 2412–2422. [Google Scholar] [CrossRef] [PubMed]
- Dickson-Swift, V.; Fox, C.; Marshall, K.; Welch, N.; Willis, J. What really improves employee health and well-being -Findings from regional Australian workplaces. Int. J. Workplace Health Manag. 2014, 7, 138–155. [Google Scholar] [CrossRef]
- Schneider, A.; Weigl, M. Associations between psycho-social work factors and provider mental well-being in emergency departments: A systematic review. PLoS ONE 2018, 13, e0197375. [Google Scholar] [CrossRef] [PubMed]
- Schön Persson, S.; Nilsson Lindström, P.; Pettersson, P.; Nilsson, M.; Blomqvist, K. Resources for work-related well-being: A qualitative study about healthcare employees’ experiences of relationships at work. J. Clin. Nurs. 2018, 27, 4302–4310. [Google Scholar] [CrossRef]
- Schön Person, S.; Nilsson Lindström, P.; Pettersson, P.; Andersson, I. Workplace relationships impact self-rated health: A survey of Swedish municipal health care employees. Work 2018, 60, 85–94. [Google Scholar]
- Schön Persson, S.; Blomqvist, K.; Nilsson Lindström, P. Meetings are an important prerequisite for flourishing workplace relationships. Int. J. Environ. Res. Public Health 2021, 18, 8092. [Google Scholar] [CrossRef]
- Morley, G.; Sese, D.; Rajendram, P.; Cole Horsburgh, C. Addressing caregiver moral distress during the Covid-19 pandemic. Clevel. Clin. J. Med. 2020. [Google Scholar] [CrossRef]
- Antonovsky, A. Unravelling the Mysteries of Health: How People Manage Stress and Stay Well, 1st ed.; Jossey-Bass: San Francisco, CA, USA, 1987. [Google Scholar]
- Adrianenssens, J.; De Gucht, V.; van der Doef, M.; Maes, S. Exploring the burden of emergency care: Predictors of stress-health outcomes in emergency nurses. J. Adv. Nurs. 2011, 67, 1317–1328. [Google Scholar] [CrossRef]
- Flinkman, M.; Isopahkala-Bouret, U.; Salanterä, S. Young registered nurses’ intention to leave the profession and professional turnover in early career: A qualitative case study. ISRN Nurs. 2013, 2013, 916061. [Google Scholar] [CrossRef] [PubMed]
- Brewer, C.S.; Kovner, C.T.; Greene, W.; Tukov-Shuser, M.; Djukic, M. Predictors of actual turnover in a national sample of newly licensed registered nurses employed in hospitals. J. Adv. Nurs. 2012, 68, 521–538. [Google Scholar] [CrossRef] [PubMed]
- Muntz, J.; Dormann, C. Moderating effects of appreciation on relationships between illegitimate tasks and intrinsic motivation: A two-wave shortitudinal study. Eur. J. Work. Organ. Psychol. 2020, 29, 391–404. [Google Scholar] [CrossRef]

{kind=link}
| Author, Year, Reference, Article Number | Aim | Method, Participants | Results | Discussion and Conclusion | The Nine Determinant Areas Important for a Sustainable Working Life (swAge-Model): 1. Diagnosis and Self-Rated Health 2. Physical Work Environment 3. Mental Work Environment 4. Workhours, Pace, Recovery 5. Economics 6. Private-Social Environment 7. Work-Social Environment 8. Motivation, Stimulance, Task Satisfaction 9. Knowledge, Competence |
|---|---|---|---|---|---|
| Da Rosa et al., 2021. Factors associated with nurses’ emotional distress during the COVID-19 pandemic [24]. | To examine the prevalence of emotional distress and the associated factors among nurses practicing in South Dakota during the COVID-19 pandemic. | Quantitative design. An online survey. Respondents: 1505 licenced nurses in South Dakota during the pandemic Emotional distress was measured using the Depression, Anxiety, and Stress Scale (DASS-21). (July–August 2020). | Overall emotional distress was reported by 22.2%, while anxiety, depression, and stress were 15.8%, 14.5%, and 11.9% respectively. Factors associated with moderate to severe emotional distress, depression, anxiety, and stress were as follows: concerns for worsening of pre-existing mental health condition, job dissatisfaction, encountering higher number of COVID-19 cases at one’s work facility, feeling unprepared for the pandemic, and concern for contracting the illness (all p < 0.05). | A high prevalence of emotional distress among nurses highlights the factors associated with emotional distress during the COVID-19 pandemic. Promoting appropriate support is imperative to reduce nurses’ emotional distress and promote psychological well-being during the COVID-19 world health crisis and in future pandemics. | 1,5,6,7,8,9 |
| Bergman et al., 2021. Registered nurses’ experiences of working in the intensive care unit during the COVID-19 pandemic [25]. | To describe Swedish registered nurses’ experiences of caring for patients with COVID-19 in ICUs during the pandemic. | Mixed method survey design. 282 respondents. An online questionnaire was distributed through social media to registered nurses who had been working in the ICU during the COVID-19 outbreak. Data were collected for 1 week (May 2020). | Of the 282 nurses who participated, the majority were ICU nurses (n = 151; 54%). Among non-intensive care nurses, only 19% received introduction to the COVID-19 ICU (n = 26). Three categories: tumbling into chaos, diminished nursing care, and transition into pandemic ICU care. Participants perceived that patient safety and care quality were compromised, and that nursing care was severely deprioritized during the pandemic. Not being able to to provide nursing care resulted in ethical stress. An increased workload and worsened work environment affected nurses’ health and well-being. | Nurses perceived that patient safety and quality of care were compromises during the pandemic. This resulted in ethical stress among nurses, which may have affected their physical and psychosocial well-being. | 1,2,3,4,5,6,7,8,9 |
| George et al., 2021. Roles and experiences of registered nurses on labor and delivery units in the United States during the COVID-19 pandemic [26]. | To examine the roles and experiences of labor and delivery nurses (LD) during the COVID-19 pandemic. | Mixed method design. Quantitative data from a cross-sectional online national survey. Qualitative data was an open-ended question about changes to their roles during the COVID-19 pandemic. Respondents: 757 nurses (July–August 2020). | Four major categories emerged: Changes in roles and responsibilities; Adaptions to changes; Psychological changes; and Perceived effects on labor support. Nearly half (n = 328) of respondents reported changes in their roles and responsibilities during the pandemic. Infection control policies and practises along with the stress of rapidly changing work environment affected the provision of labor support and personal well-being. | Policies and practises that can fascilitate the ability of LD nurses to safely and securely remain at the bedside and provide high-touch, hands-on labor support are needed. | 1,2,3,4,5,6,8 |
| Gago-Valiente et al., 2021. Emotional exhaustion, depersonalization, and mental health in nurses from Huelva: a cross-cutting study during the SARS-CoV-2 pandemic [27]. | To examine the prevalence of emotional exhaustion, depersonalization, and possible non-psychotic psychiatric disorders in nursing professionals during the COVID-19 pandemic. | Quantitative design. Descriptive cross-sectional study. Respondents: 318 nursing professionals (April–June 2020). | Nurses who had contact with SARS-CoV-2 in their work environment showed higher levels of emotional exhaustion (49.6%) and depersonalization (34.3%) than nurses who had no contact (38.3% and 21.1% respektively). Among the cases of emotional exhaustion, there were around 60% with non-psychotic psychiatric symptoms compared to 28.5% who did not show it. On the other hand, in the cases of depersonalization, almost 40% evidenced non-psychotic psychiatric symptoms, compared to 25% who did not. | The nursing staff who have had contact with COVID-19 in their work environment had poorer state of health leading to high emotional exhaustion, high depersonalization, with a likely precense of a non-psychotic psychiatric pathologies. In this study sample the men, in general, showed a poorer state of mental health than that of the women. | 1,3,4,6,9 |
| Firew et al., 2020. Protecting the front line: a cross-sectional survey analysis of the occupational factors contributing to healthcare workers’ infections and psychological distress during the COVID-19 pandemic in the USA [28]. | To investigate factors contributing to healthcare workers (HCWs) infection and psychological distress for HCWs, with COVID-19 exposure risk during the COVID-19 pandemic in the USA. | Quantitative design. A cross sectional survey of HCWs Respondents: 2040 (physicians 31%, nurses 27%, emergency medical technicians (EMTs) 13%, non-clinical staff 29%) from 48 states, the District of Columbia, and US territories (May 2020) | HCWs in the emergency department (31.64%) were more likely to contract COVID-19 compared with HCWs in the ICU (23.17%) and inpatient settings (25.53%). HCWs that contracted COVID-19 reported higher levels of depressive symptoms (mean diff. = 0.31; 95% CI 0.16 to 0.47), anxiety symptoms (mean diff. = 0.34; 95% CI 0.17 to 0.52) and burn-out (mean diff. = 0.54; 95% CI 0.36 to 0.71). Primary outcome: prevalence of self-reported COVID-19 infection, in addition to burn-out, depression and anxiety symptoms. | HCWs have experienced significant physical and psychological risk while working during the COVID-19 pandemic. These findings highlight the urgent need for increased support for providing physical and mental health well-being. | 1,2,3,5,6,7 |
| Galanis et al., 2021. Fear of COVID-19 among nurses in mobile COVID-19 testing units in Greece [29]. | To assess the level of fear of COVID-19 among nurses in mobile COVID-19 testing units and compare it with demographic characteristics | Quantitative design. A cross-sectional study Respondents: 57 nurses working in mobile testing units. The fear of COVID-19 scale was used to measure fear of the COVID-19 pandemic. (November–December 2020) | Among nurses, 31.6% experienced elevated fear of COVID-19 indicative of presence of anxiety and post-traumatic stress symptommatology were 22.8% and 17.5%. Fear of COVID-19 was not affected by demographic variables. Fear was higher in females, nurses who had children, and nurses who lived with others. Increased clinical experience was related with decreased fear. | A secure work environment with access to personal protective equipment (PPE) and relevant training for nurses in these units could decrease fear of COVID-19 and increase work performance. | 1,3,6,9 |
| Suryavanshi et al., 2020. Mental health and quality of life among healthcare professionals during the COVID-19 pandemic in India [30]. | To assess the mental health and quality of life (QoL) of Indian Health Care Professionals (HCPs), the fourth highest-burden country for COVID-19. | Quantitative design. Online survey) Respondents: 197 (24% nurses, 34% physichans, 42% other health care workes) (May 2020) | Of 197 HCPs assessed, 130 participants (66%) worked in public hositals, 47 (24%) were nurses, 66 (34%) physicians. A large proportion reported symptoms of depression (92.47%), anxiety (98.5%), and low QoL (89.45%). Odds of combined depression and anxiety were 2.37 times higher among single HCPs compared to married (95% CI: 1.03–4.96). Work environment stressors were associated with 46% increased risk of combined depression and anxiety (95% CI: 1.15–1.85). Moderate to severe depression and anxiety were independently associated with increased low QoL OR: 3:19 (95% CI: 1.30–7.84), OR:2.84 (95% CI: 1.29–6.29). | A high prevalence of symptoms of depression and anxiety and low QoL among Indian HCPs during the COVID-19 pandemic. There is an urgent need to prevent and treat mental health symptoms among frontline HCPs. | 1,2,4,5,6,7,9 |
| Norful et al., 2021. Primary drivers and psychological manifestation of stress in frontline healthcare workforce during the initial COVID-19 outbreak in the United States [31]. | To understand the physical and psychological impact of high stress clinical environments and contributory factors of burnout in multi-disciplinary healthcare workforce during the initial outbreak of COVID-19. | Qualitative design. In-person interviews Respondents: 55 healthcare workers (21 registrerd nurses, 5 respiratory therapists, 12 physitians, 4 pharmacists, 13 patent care technicians) (March–April 2020) | Themes revolved around three main areas: fear of uncertainty, physical and psychological manifestations of stress, and resilience building. Shifting information, a lack of PPE, and fear of infecting others prompted worry for those working with COVID-infected patients. Stress manifested more psychologically than physically. Individualized stress mitigation efforts, social media and organizational transparence were reported by healthcare workers to be effective against rising stressors. | In order to understanding stressors and supporting clinicians during healthcare emergencies, more research is necessary to effectively promote healthcare workforce well-being. | 1,3,4,5,6,7,9 |
| Giusino et al., 2021. “We all held our own” Job demands and resources at Individual, Leader, Group and Organizational levels during COVID-19 outbreak in healthcare [32]. | To explore the fitness of integrating the Job Demands-Resources model (JD-R) and the Individual-Group-Leader-Organization (IGLO) framework to investigate the pandemic’s impact on healthcare workers’ mental health | Qualitative design. Semi-structured interviews and focus group interviews. Respondents: 21 senior and middle nurse managers and healthcare workers from the Department of Emergency, Department of Medicine, and Research Institute of Neuroscience. (September–October 2020) | Several COVID-19-related job demands and resources were found at all IGLO levels. Individual-level demands included emotional load, while resources included resilience and motivation. Group-level demand included social distancing, while resources included team support and cohesion. Leader-level demands included managers’ workload, while resources included leader support. Organizational-level demands included work reorganization while resources included mental health initiatives | Integrating JD-R and IGLO proved feasible as job demands and resources could be categorized according to the different levels of the framework. The findings fills the lack of knowledge on how job demands and resources might unfold at different workplace levels during a pandemic. Results provide unitlevel evidence for designing and implementing multilevel interventions to manage healthcare workers’ mental health during COVID-19 and future pandemics. | 1,2,3,4,6,7,8,9 |
| van der Goot et al., 2021. Psychological distress among frontline workers during the COVID-19 pandemic: a mixed-methods study [33]. | To investigate experienced psychological distress during the COVID-19 pandemic from a self-determination theory perspective | Mixed-method design. Quantitative data: repeated measures: survey. Qualitative data: audio diaries. Respondents: 46 (50% nurses, 33% junior doctors, 17% hospital consults). (April–November 2020) | Quantitative results indicated that perceived psychological distress during COVID-19 was higher than pre-COVID and fluctuated over time. Need frustration, specifically autonomy and competence, was positively associated with psychological distress while need satisfaction, especially relatedness, was negatively associated with psychological distress. The qualitative thematic analysis stated that especially organizational logistics frustrated autonomy, and unfamiliarity with COVID-19 frustrated competence. Despite many need frustrating experiences, a strong connection with colleagues and patients were important sources of relatedness support that seemed to mitigate psychological distress | Challenging times require healthcare organisations to better support their professionals by tailored formal and informal support. The authors propose to address both indirect (e.g., organisation) and direct (e.g., colleagues) elements of the clinical and social environment in order to reduce need frustration and enhance need satisfaction. | 1,3,6,7,8,9 |
| Thomas et al., 2021. COVID-19 and moral distress: a pediatric critical care study [34]. | To investigate whether pediatric critical care professionals are experiencing moral distress during the COVID-19 pandemic and, if so, for what reasons. | Quantitative design. An exploratory survey. Respondents: 337 paediatric critical care professionals 26% nurses, 49% physichans, 16% respiratory therapists, other health care workes 9%, via the Pediatric Acute Lung Injury and Sepsis Investigators Network from (April–May 2020) | Overall, 85.8% of survey respondents reported moral distress. Nurses reported higher degrees of moral distress than other professional groups. Inducers of moral distress were related to challenges to professional integrity and lack of organizational support. 5 themes: psychological safety, expectations of leadership, connectedness through a moral community, professional challenges, and professional vs. social responsibility. Most respondents were confident in their ability to reason through ethical dilemmas (76%) and think clearly when confronting an ethical challenge even when pressured (78.9%). | During the COVID-19 pandemic, pediatric critical care professionals are experiencing moral distress due to various factors that challenge their professional integrity. Despite these challenges, they also exhibit attributes of moral resilience. Organizations have opportunities to cultivate a psychologically safe and healthy work environment to mitigate anticipatory, present, and lingering moral distress. | 1,2,3,4,5,6,7,8,9 |
| Sheppard et al., 2021. Nursing moral distress and intent to leave employment during the COVID-19 pandemic [35]. | To explore the levels of moral distress (MD) among registered nurses in the practice environment and inform the nurse leaders about the impact of MD on nursing turnover. | Quantitative design. Questionnaire. Respondents: 129 registered nurses. Survey Measure of Moral Distress for Healthcare Professionals (MMD-HP) was used. (July–August 2020) | T-tests showed significant differences for 16 of 27 MMD-HP items in registered nurses intent to leave. RNs had 2.9 times the odds of intent to leave (p = 0.019) due to perceived issues with patient quality and safety and 9.1 times the odds of intent to leave (p < 0.001) due to perceived issues with the work environment. Results explained 40.3% of outcome variance. | MD related to work environment or patient quality and safety were significant factors in registered nurses intent to leave their positions. | 1,3,4,5,7,9 |
| Guedes dos Santos et al., 2021. Work environment of hospital nurses during the COVID-19 pandemic in Brazil [36]. | To investigate the nurses’ work environment in university hospitals during the COVID-19 pandemic in Brazil | Mixed methods design. Quantitative data was collected by an online questionnaire. Qualitative data was collected through an open question Repondents: 104 nurses from three university hospitals. (April–June 2020. | The quantitative results showed that the responses to ‘I received training on the correct use of personal protective equipment (PPE)’ and ‘I am afraid of being infected’ had the best and worst evaluations respectively. The qualitative findings revealed five themes: feeling of insecurity, lack of PPE, lack of diagnostic tests, changes in the care flow and fear of the unknown. | The study highlighted the challenges faced by hospital nurses while caring for patients with COVID-19. | 1,2,3,4,5,7,9 |
| Diomidous, M., 2020. Sleep and motion disorders of physicians and nurses working in hospitals facing the pandemic of COVID-19 [37]. | To investigate the relationship between the physical activity and sleep disorders among healthcare professionals, particularly among medical doctors and nurses | Quantitative design. Questionnaire Respondents: 204 (102 medical doctors and 102 nurses). (February–April 2020). | The results of the statistical analysis showed that there are positive correlations between the level of physical activity during the daily work and the free time of the participants with parameters that are related to sleep disorders. | A stressful situation such as the COVID-19 pandemic can provide useful information in order to better understand the relationship between physical activity and sleeping disorders in similar working conditions | 1,4,9 |
| Jo et al., 2021 Nurses’ resilience in the face of coronavirus (COVID-19): An international view [38]. | To examine factors associated with nurses’ resilience during the COVID-19 pandemic | Quantitative design. Cross-sectional descriptive study. Respondents: 904 nurses in Japan, Korea, Turkey, and the United States. (July–November 2020) | Fear of becoming infected, intention to leave nursing, and having had a positive COVID-19 test were negatively associated with resilience (p < 0.05). Regression analysis indicated that U.S. nurses had significantly higher resilience than nurses in the other countries examined (p < 0.001). Nurses reporting organizational support and those who participated in policy and procedure development had higher resilience score (p < 0.01). | Organizational support, involving nurses in policy development, and country of practice were found to be important resilience factors. The authors recommend to further determine the optimal practice environment to support nurse resilience. | 1,3,5,6,9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nagel, C.; Westergren, A.; Persson, S.S.; Lindström, P.N.; Bringsén, Å.; Nilsson, K. Nurses’ Work Environment during the COVID-19 Pandemic in a Person-Centred Practice—A Systematic Review. Sustainability 2022, 14, 5785. https://doi.org/10.3390/su14105785
Nagel C, Westergren A, Persson SS, Lindström PN, Bringsén Å, Nilsson K. Nurses’ Work Environment during the COVID-19 Pandemic in a Person-Centred Practice—A Systematic Review. Sustainability. 2022; 14(10):5785. https://doi.org/10.3390/su14105785
Chicago/Turabian StyleNagel, Cicilia, Albert Westergren, Sophie Schön Persson, Petra Nilsson Lindström, Åsa Bringsén, and Kerstin Nilsson. 2022. "Nurses’ Work Environment during the COVID-19 Pandemic in a Person-Centred Practice—A Systematic Review" Sustainability 14, no. 10: 5785. https://doi.org/10.3390/su14105785
APA StyleNagel, C., Westergren, A., Persson, S. S., Lindström, P. N., Bringsén, Å., & Nilsson, K. (2022). Nurses’ Work Environment during the COVID-19 Pandemic in a Person-Centred Practice—A Systematic Review. Sustainability, 14(10), 5785. https://doi.org/10.3390/su14105785