
A Simulation Model for Forecasting COVID-19 Pandemic Spread: Analytical Results Based on the Current Saudi COVID-19 Data

 ,
,  ,
,  , , ,
, , ,  ,
,
Abstract
1. Introduction
- Introducing a new simulation model to forecast the spreading behavior of the COVID-19 based on Saudi real data;
- Developing a decision support interface for the public and officials to raise their awareness of COVID-19;
- Proposing a suitable curve fitting function (Gaussian) to fit the current infected cases and predicting, later, the potential number of infected cases;
- Suggesting a novel method for one-day prediction of the number of infected cases and comparing it with similar existing techniques.
- -
- Early closing of the borders was set on 15 March 2020, followed by a lockdown and confinement after few days;
- -
- All holy places in Mecca and Medina and all mosques in KSA were closed to avoid people gatherings. Afterward, there was a suspension of Taraweeh prayers during the month of Ramadan in 2020 (March 2020) and in 2021 (April 2021);
- -
- COVID-19 PCR tests are free, available on demand and can be obtained outside hospitals in mobile points all over the country to avoid bringing the infection to healthcare institutions;
- -
- The extensive use of numerical systems: different applications have been deployed and used to manage the COVID-19 crisis: Tawakalna to control the movement of people, Tabaud for contact tracing, Tataman and Sehhaty for PCR tests and vaccine, and Itamarna to organize the access to holy places. Disregarding the instructions proposed by the above-mentioned applications implies immediate infractions and penalties. For example, the ministry of interior announced that 12,855 violations of precautionary measures were seized in just one week in March 2020 [5];
- -
- The existence of advanced online educational systems even before the outbreak of COVID-19. These education systems ensure the continuation of the academic year without any disturbances;
- -
- The support and funding of scientific research in different fields related to COVID-19 issues. Medical, biological, technological, and human studies were funded by several institutes, such as the KACST, KAUST, and regional universities;
- -
- Several packages of financial aid were provided to citizens, residents, and the private sector to avoid economic recession and layoffs. Among these measures, the payment, for several consecutive months in 2020, of half the salary of workers in the private small- and medium-sized enterprises;
- -
- Providing free vaccine for all the population including Saudis, residents, and illegal residents. In fact, by 31 March 2021, about 4.7 million people and all healthcare professionals were vaccinated [5].
- -
- What is the basis of the strategy used for fighting against COVID-19 in KSA?
- -
- What are the circumstances leading to successful control of the pandemic in Saudi Arabia?
- -
- How can the number of infections in the upcoming months in KSA be predicted accurately based on the evolution of the COVID-19 pandemic in KSA cities?
- -
- How are the parameters that may considerably reduce the number of infections and therefore affect death rates identified?
- -
- How can the suggested forecasting model be used to raise the awareness of the Saudi public and officials about the seriousness of the next waves of COVID-19 and other future possible health crises?
- -
- How can the suggested simulator be used by Saudi authorities to enhance the control of the pandemic spread and establish a protocol for the management of critical future pandemics?
- -
- How is the proposed prediction method used for general prediction purposes?
2. Literature Review
- -
- The study in [33] analyzed the data about the spread of the pandemic in KSA in the first 14 days, while the current study examines the current data after about 8 months from the appearance of COVID-19;
- -
- The methodology used in [33] included a linear regression since the data was climbing linearly at the beginning of the pandemic, while the current study involves a Gaussian curve fitting for data prediction since the data curve reached the peak and went down to become flattened;
- -
- The methodology applied in [33] utilized simple moving average, weighted moving average, and exponential smoothing during 36 days, while the current study employs the same technique for 206 days, proposes a new prediction method, and compares it with one of the well-known state-of-the-art prediction methods.
3. Materials and Methods
- The output part shows the results and helps us carry out the statistical analysis after each simulation;
- The control panel details and manages the different simulation parameters;
- The canvas visually illustrates the simulation. The created community is identified as a set of points randomly initialized in several locations in the canvas. These points represent people walking uniformly and randomly in the four possible directions. Each direction has a probability p equal to 1/4. The situation of each point is recognized by its color: black, green, red, and blue, for dead, recovered, infected, and susceptible, respectively.
- The “size of the community,” in which a 100 means that one hundred people are randomly located in the canvas;
- The “period” of the simulations (in days);
- The “initial number of infections” in the community;
- The “infection rate” (probability of infection) reflects the degree of propagation of the pandemic among susceptible people. If a susceptible person is in closer contact with an infected subject within the indicated social distance, the probability of infection of the first person will be equal to this parameter;
- The “hygiene rate” is the complement of the infection rate. If the former rate is set to p, the latter rate will be 1-p and vice versa. Indeed, hygiene refers to both cleaning of hands and applying all the preventive healthcare measures such as wearing masks. Since the community members do not follow the same hygienic procedures, an average rate was assumed to be the same for all the community;
- The “recovery rate” is the probability of an infected person’s recovery;
- The “death rate” is the probability of the death of infected people. This parameter is the complement of the recovery rate;
- The “social distance” between people should be at least two meters according to the WHO recommendations [34]. In our experiments, its value was set to two, and it was assumed that the person becomes infected if the Euclidean distance between this person and an infected one is less than the social distance. In fact, this infected person was attained with a probability equal to the value of the infection rate., i.e., the simulation is based on infected individuals, who are within a 2 m diameter, if and only if one of them is infected using the infection rate;
- The “delay” is the time separating two frames. It is used to visualize the components, especially small populations;
- The “stride,” which represents the walking distance of individuals, is the distance of the person’s movement at each time frame in a specific direction. Two random numbers [−Stride, +Stride] define the range X–Y coordinates of each person. Hence, the stride reflects the movement restriction degree. The more the individuals move, the greater the chance that they will meet and more likely to be infected;
- The “recovery period” is the time of healing of an infected person. In the performed experiments, it is equal to 14 days [35]. This period can be changed if used by practitioners in other applications;
- The width and height define the dimensions of the community area measured in meters. Each pixel in the canvas area was set to one meter. Then, the dimension of the population was computed based on the real density of the population. In our experiments, the dimension of the population 500 × 500 m2 was used. In this population, the number of people per square kilometer was divided by four.
4. Results and Discussion
- Large stride, large movements of people, no quarantine;
- Small stride, large movements of people, quarantine;
- Medium movements of people, partial quarantine;
- High infection rate, then low hygiene;
- Low infection rate, then high hygiene.
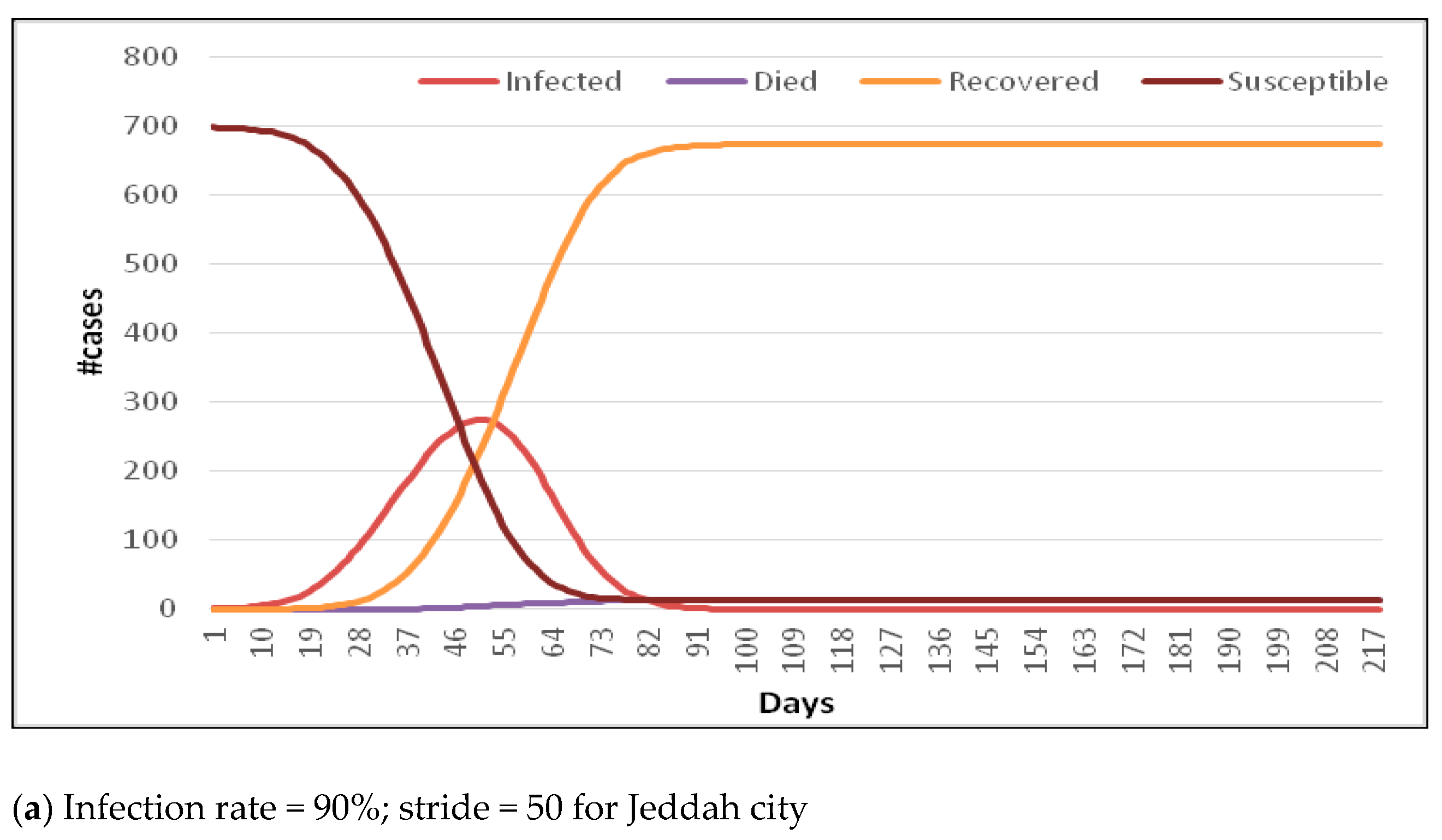
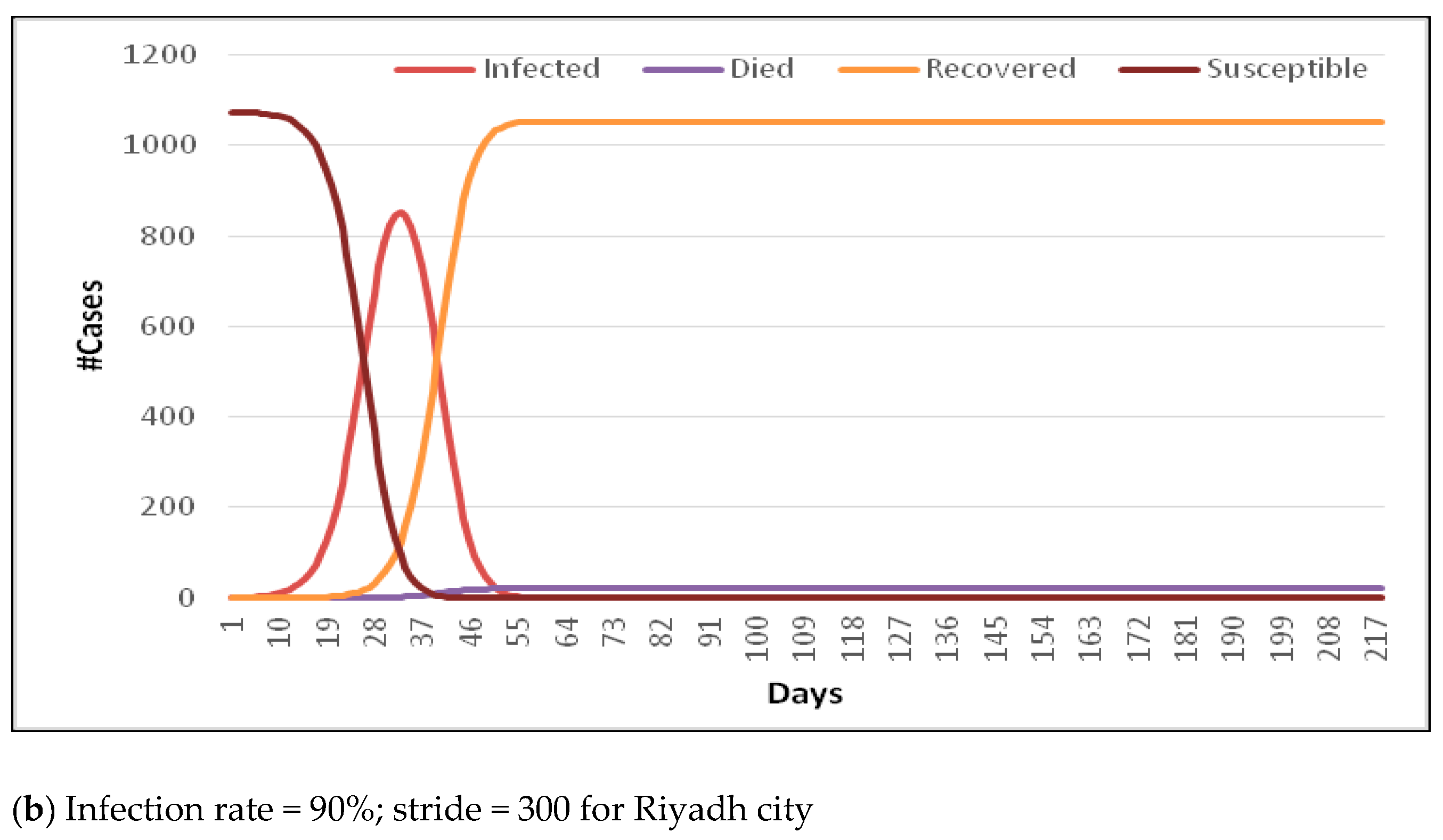
4.1. Scenarios of Simulation
- -
- Measuring the infection day by day with a normal random walk;
- -
- Measuring the infection during the previous three days with random walks in infected locations.
4.1.1. Scenario 1: Assuming That the Locations from the Previous Day(s) Are Not Contaminated
4.1.2. Scenario 2: Assuming That the Locations from the Previous Three Days Are Contaminated
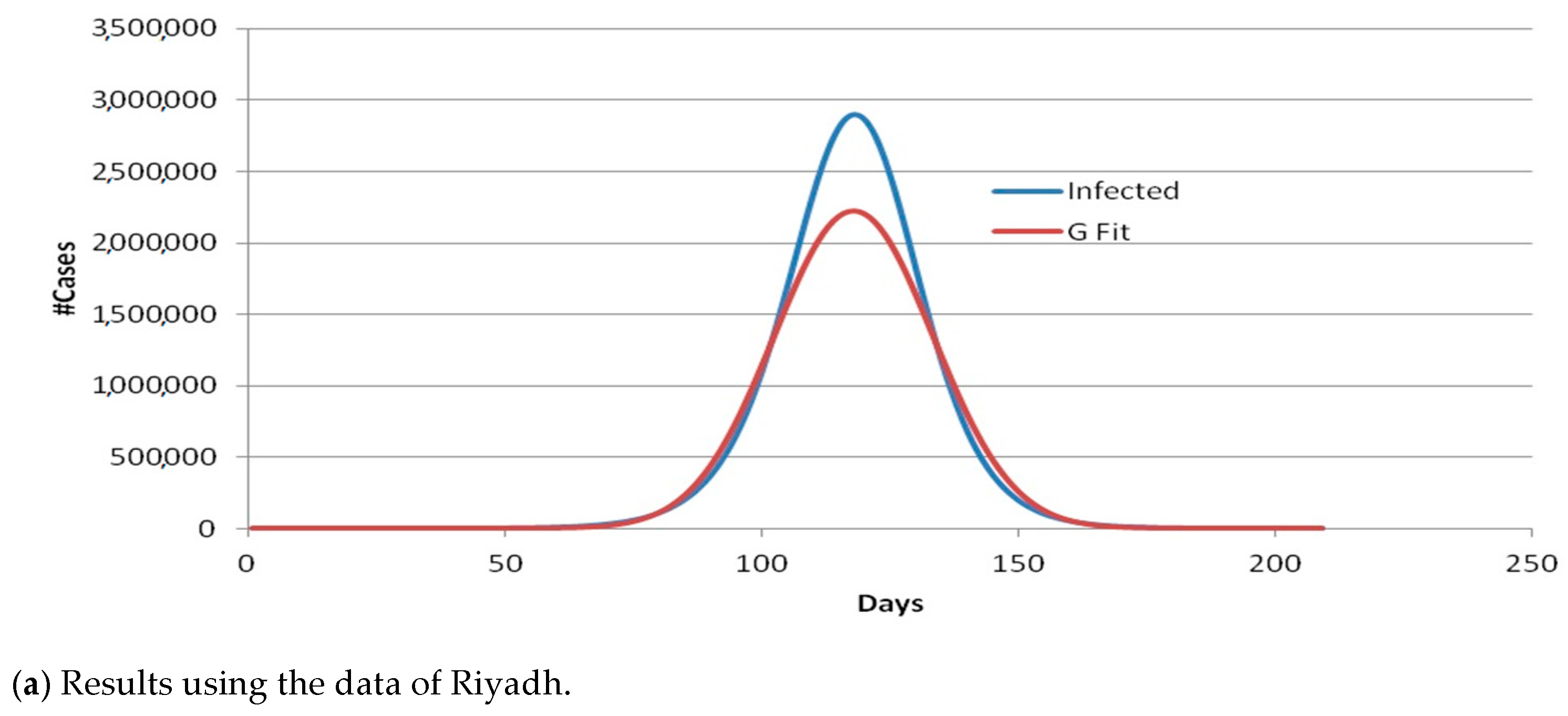
4.2. Regression Analysis of Data
4.3. One-Day Prediction Results
5. Discussion and Interpretations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Ethics Statements
References
- Li, Q.; Guan, X.; Wu, P.; Qun, L.; Xuhua, G.; Peng, W.; Xiaoye, W.; Lei, Z.; Yeqing, T.; Ruiqi, R.; et al. Early transmission dynamics in Wuhan, China, of Novel Coronavirus—Infected pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef]
- Koenig, K.L.; Bey, C.K.; McDonald, E.C. 2019-nCoV: The Identify-Isolate-Inform (3I) Tool Applied to a Novel Emerging Coronavirus. West. J. Emerg. Med. 2020, 21, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- WHO Coronavirus Disease (COVID-19) Dashboard. 2021. Available online: https://covid19.who.int (accessed on 3 April 2021).
- Official Statistics of the Saudi Ministry of Health. 2021. Available online: https://www.moh.gov.sa/en/ (accessed on 3 April 2021).
- Chudik, A.; Mohaddes, K.; Pesaran, M.H.; Raissi, M.; Rebucci, A.A. Counterfactual Economic Analysis of Covid-19 Using a Threshold Augmented Multi-Country Model; Cambridge Working Papers in Economics 2088; Faculty of Economics, University of Cambridge: Cambridge, UK, 2020. [Google Scholar]
- Althobaity, H.M.; Alharthi, R.A.; Altowairqi, M.H.; Alsufyani, Z.A.; Aloufi, N.S.; Altowairqi, A.E.; Alqahtani, A.S.; Alzahrani, A.K.; Abdel-Moneim, A.S. Knowledge and awareness of Middle East respiratory syndrome coronavirus among Saudi and Non-Saudi Arabian pilgrims. Int. J. Health Sci. 2020, 11, 20–25. [Google Scholar]
- AlMofada, S.K.; Alherbisch, R.J.; AlMuhraj, N.A.; Almeshary, B.N.; Alrabiah, B.; Al Saffan, A.; Baseer, M.A. Knowledge, Attitudes, and Practices Toward COVID-19 in a Saudi Arabian Population: A Cross-Sectional Study. Cureus 2020, 12, e8905. [Google Scholar] [CrossRef]
- Shi, Y.; Wang, Y.; Shao, C.; Huang, J.; Gan, J.; Huang, X.; Bucci, E.; Piacentini, M.; Ippolito, G.; Melino, G. COVID-19 infection: The perspectives on immune responses. Cell Death Differ. 2020, 27, 1451–1454. [Google Scholar] [CrossRef] [PubMed]
- Xiong, H.; Yan, H. Simulating the Infected Population and Spread Trend of 2019-nCov Under Different Policy by EIR Model. Ssrn Electron. J. 2020. [Google Scholar] [CrossRef]
- Wu, J.T.; Leung, K.; Leung, G.M. Nowcasting and forecasting the potential domestic and international spread of the 2019-nCoV outbreak originating in Wuhan, China: A modelling study. Lancet 2020, 395, 689–697. [Google Scholar] [CrossRef]
- Read, J.M.; Bridgen, J.R.; Cummings, D.A.; Ho, A.; Jewell, C.P. Novel coronavirus 2019-nCoV: Early estimation of epidemi-ological parameters and epidemic predictions. medRxiv 2020, 34, 126–139. [Google Scholar]
- Rhodes, T.; Lancaster, K.; Rosengarten, M. A model society: Maths, models and expertise in viral outbreaks. Crit. Public Health 2020, 30, 253–256. [Google Scholar] [CrossRef]
- Li, T. Simulating the Spread of Epidemics in China on the Multi-layer Transportation Network: Beyond the Coronavirus in Wuhan. arXiv 2020, arXiv:2002.12280. [Google Scholar]
- Yang, Q.; Yi, C.; Vajdi, A.; Cohnstaedt, L.W.; Wu, H.; Guo, X.; Scoglio, C.M. Short-term forecasts and long-term mitigation evaluations for the COVID-19 epidemic in Hubei Province, China. Infect. Dis. Model. 2020, 5, 563–574. [Google Scholar] [CrossRef] [PubMed]
- Estrada, M.A.R. The Monitoring of COVID-19 Infected Cases by Continent under the Application of MDNIDC-Mapping Simulator. Ssrn Electron. J. 2020. [Google Scholar] [CrossRef]
- Mnasri, S.; Nasri, N.; Val, T. The Deployment in the Wireless Sensor Networks: Methodologies, Recent Works and Applications. In Proceedings of the International Conference on Performance Evaluation and Modeling in Wired and Wireless Networks (PEMWN 2014), Sousse, Tunisia, 4–7 November 2014. [Google Scholar]
- Mnasri, S.; Abbès, F.; Zidi, K.; Ghedira, K. A multi-objective hybrid BCRC-NSGAII algorithm to solve the VRPTW. In Proceedings of the 13th International Conference on Hybrid Intelligent Systems (HIS 2013), Gammarth, Tunisia, 4–6 December 2013; pp. 60–65. [Google Scholar]
- Tarawneh, A.S.; Hassanat, A.B.; Celik, C.; Chetverikov, D.; Rahman, M.S.; Verma, C. Deep Face Image Retrieval: A Comparative Study with Dictionary Learning. In Proceedings of the 2019 10th International Conference on Information and Communication Systems (ICICS), Irbid, Jordan, 11–13 June 2019; pp. 185–192. [Google Scholar]
- Mnasri, S.; Zidi, K. A heuristic approach based on the multi-agents negotiation for the resolution of the DDBAP. In Proceedings of the 4th In-ternational Conference on Metaheuristic and Nature Inspired Computing, Sousse, Tunisia, 27–31 October 2012. [Google Scholar]
- Mnasri, S.; Nasri, N.; Van Den Bossche, A.; Val, T. A Comparative analysis with validation of NSGA-III and MOEA/D in re-solving the 3D indoor redeployment problem in DL-IoT. In Proceedings of the 2017 International Conference on Internet of Things, Embedded Systems and Communications (IINTEC), Gafsa, Tunisia, 20–22 October 2017; pp. 15–20. [Google Scholar]
- Fong, S.J.; Li, G.; Dey, N.; Crespo, R.G.; Herrera-Viedma, E. Composite Monte Carlo decision making under high uncertainty of novel coronavirus epidemic using hybridized deep learning and fuzzy rule induction. Appl. Soft Comput. 2020, 93, 106282. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Guo, Q.; Li, M.; Wang, C.; Fang, Z.; Wang, P.; Tan, J.; Wu, S.; Xiao, Y. Host and infectivity prediction of Wuhan 2019 novel coronavirus using deep learning algorithm. BioRxiv 2020. [Google Scholar] [CrossRef]
- Chang, S.L.; Harding, N.; Zachreson, C.; Cliff, O.M.; Prokopenko, M. Modelling transmission and control of the COVID-19 pandemic in Australia. Nat. Commun. 2020, 11, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Yu, X.; Sun, H.; Tick, G.R.; Wei, W.; Jin, B. COVID-19 infection and recovery in various countries: Modeling the dynamics and evaluating the non-pharmaceutical mitigation scenarios. arXiv 2020, arXiv:2003.13901. [Google Scholar]
- Zia, K.; Farooq, U. Covid-19 outbreak in pakistan: Model-driven impact analysis and guidelines. arXiv 2020, arXiv:2004.00056. [Google Scholar]
- Anastassopoulou, C.; Russo, L.; Tsakris, A.; Siettos, C. Data-based analysis, modelling and forecasting of the COVID-19 out-break. PLoS ONE 2020, 15, e0230405. [Google Scholar] [CrossRef]
- Li, R.; Lu, W.; Yang, X.; Feng, P.; Muqimova, O.; Chen, X.; Wei, G. Prediction of the Epidemic of COVID-19 Based on Quar-antined Surveillance in China. medRxiv 2020. [Google Scholar] [CrossRef]
- Silva, P.C.; Batista, P.V.; Lima, H.S.; Alves, M.A.; Guimarães, F.G.; Silva, R.C. COVID-ABS: An agent-based model of COVID-19 epidemic to simulate health and economic effects of social distancing in-terventions. Chaossolitons Fractals 2020, 139, 110088. [Google Scholar] [CrossRef]
- Ivanov, D. Predicting the impacts of epidemic outbreaks on global supply chains: A simulation-based analysis on the coronavirus outbreak (COVID-19/SARS-CoV-2) case. Transp. Res. Part. E Logist. Transp. Rev. 2020, 136, 101922. [Google Scholar] [CrossRef] [PubMed]
- Bartsch, S.M.; Ferguson, M.C.; McKinnell, J.A.; O’Shea, K.J.; Wedlock, P.T.; Siegmund, S.S.; Lee, B.Y. The Potential Health Care Costs and Resource Use Associated With COVID-19 In The United States: A simulation estimate of the direct medical costs and health care resource use associated with COVID-19 infections in the United States. Health Aff. 2020, 10, 1377. [Google Scholar] [CrossRef] [PubMed]
- Weissman, G.E.; Crane-Droesch, A.; Chivers, C.; Luong, T.; Hanish, A.; Levy, M.Z.; Lubken, J.; Becker, M.; Draugelis, M.E.; Anesi, G.L.; et al. Locally Informed Simulation to Predict Hospital Capacity Needs During the COVID-19 Pandemic. Ann. Intern. Med. 2020, 173, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Aseeri, M.; Hassanat, A.B.; Mnasri, S.; Tarawneh, A.S.; Alhazmi, K.; Altarawneh, G.; Alrashidi, M.; Alharbi, H.; Almohammadi, K.; Chetverikov, D.; et al. Modelling-based Simulator for Forecasting the Spread of COVID-19: A Case Study of Saudi Arabia. Int. J. Comput. Sci. Netw. Secur. 2020, 20, 114–125. [Google Scholar]
- WHO. Management of Ill Travelers at Points of Entry–International Airports, Seaports and Ground Crossings—In the Context of COVID-19 Outbreak: Interim Guidance; Technical Report; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Q&A on Coronaviruses (COVID-19). Available online: https://www.who.int/news-room/q-a-detail/q-a-coronaviruses (accessed on 12 January 2021).
- Ma, S.; Zhang, J.; Zeng, M.; Yun, Q.; Guo, W.; Zheng, Y.; Zhao, S.; Wang, M.H.; Yang, Z. Epidemiological Parameters of COVID-19: Case Series Study. J. Med. Internet Res. 2020, 22, e19994. [Google Scholar] [CrossRef]
- Lu, Q.-B.; Zhang, Y.; Liu, M.-J.; Zhang, H.-Y.; Jalali, N.; Zhang, A.-R.; Li, J.-C.; Zhao, H.; Song, Q.-Q.; Zhao, T.-S.; et al. Epidemiological parameters of COVID-19 and its implication for infectivity among patients in China, 1 January to 11 February 2020. Eurosurveillance 2020, 25, 2000250. [Google Scholar] [CrossRef]
- Sun, C.; Zhai, Z. The efficacy of social distance and ventilation effectiveness in preventing COVID-19 transmission. Sustain. Cities Soc. 2020, 62, 102390. [Google Scholar] [CrossRef]
- Althoff, T.; Sosič, R.; Hicks, J.L.; King, A.C.; Delp, S.L.; Leskovec, J. Large-scale physical activity data reveal worldwide activity inequality. Nat. Cell Biol. 2017, 547, 336–339. [Google Scholar] [CrossRef]
- WHO. COVID-2019 Situation Reports. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports/ (accessed on 12 January 2021).
- Alyami, M.H.; Naser, A.Y.; Orabi, M.A.A.; Alwafi, H.; Alyami, H.S. Epidemiology of COVID-19 in the Kingdom of Saudi Arabia: An Ecological Study. Front. Public Health 2020, 8. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus Disease (COVID-19): How Is It Transmitted? 9 July 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/question-and-answers-hub/q-a-detail/q-a-how-is-covid-19-transmitted (accessed on 23 April 2021).
- Song, K.-B.; Baek, Y.-S.; Hong, D.H.; Jang, G. Short-Term Load Forecasting for the Holidays Using Fuzzy Linear Regression Method. IEEE Trans. Power Syst. 2005, 20, 96–101. [Google Scholar] [CrossRef]
- Johannesen, N.J.; Kolhe, M.; Goodwin, M. Relative evaluation of regression tools for urban area electrical energy demand forecasting. J. Clean. Prod. 2019, 218, 555–564. [Google Scholar] [CrossRef]
- COVID 19 Dashboard: Saudi Arabia. Available online: https://covid19.moh.gov.sa/en/ (accessed on 10 January 2021).
- COVID 19 Interactive Dashboard. Available online: https://covid19.cdc.gov.sa/daily-updates/ (accessed on 6 January 2021).
- Brown, A.M. A step-by-step guide to non-linear regression analysis of experimental data using a Microsoft Excel spreadsheet. Comput. Methods Programs Biomed. 2001, 65, 191–200. [Google Scholar] [CrossRef]
- Al-tarawneh, G.A. Prediction of stock price using a hybrid technical analysis method. Sci. Int. Lahore 2019, 31, 391–396. [Google Scholar]
- Hooker, R.H. Correlation of the Marriage-Rate with Trade. J. R. Stat. Soc. 1901, 64, 485–492. [Google Scholar]
- Brown, R.G.; Meyer, R.F. The Fundamental Theorem of Exponential Smoothing. Oper. Res. 1961, 9, 673–685. [Google Scholar] [CrossRef]
- Nejah, N.; Sami, M.; Thierry, V. 3D node deployment strategies prediction in wireless sensors network. Int. J. Electron. 2020, 107, 808–838. [Google Scholar] [CrossRef]
- Perc, M.; Miksić, N.G.; Slavinec, M.; Stožer, A. Forecasting COVID-19. Front. Phys. 2020, 8. [Google Scholar] [CrossRef]
- Lo, A.; Huang, J.-J.; Chen, C.-C.; Chou, F.H.-C.; Shieh, V. From biological safety to social safety: How Taiwan’s community centered prevention program controlled the COVID-19 outbreak. J. Glob. Health 2020, 10. [Google Scholar] [CrossRef]
- Ayanshina, O.A.; Adeshakin, A.O.; Afolabi, L.O.; Adeshakin, F.O.; Alli-Balogun, G.O.; Yan, D.; Essien-Baidoo, S.; Wan, X. Seasonal variations in Nigeria: Understanding COVID-19 transmission dynamics and immune responses. J. Glob. Health Rep. 2020, 4, e2020084. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Method | Description | Limitations |
|---|---|---|
| [13] | Mathematical model (formulation of the spread rate) | No use of real data. |
| [14] | Simulation system | Limited applicability (cannot be generalized to study other countries). |
| [15] | Markovian-based method | Non-Markovian methods are better to describe the current stage of the pandemic as the parameters COVID19 do not follow the Markovian distribution yet. |
| [16] | Simulation system | No use of real data. |
| [22] | Simulation system | No sufficient comparisons to validate the efficiency of the system. |
| [25] | Simulation system (SEIR) | Limited applicability (cannot be generalized to study other countries). |
| [26] | Simulation system (SDIR) | Lack of accuracy in the absence of the real number of infected cases. |
| [33] | A Simulation system, linear regression, and simple time series prediction | Analyzed the Saudi data in the early 14 days of the pandemic spread only, when infected cases were increasing linearly, while it is not the case of the current data. Moreover, this study used simple time series analysis. |
| Property | Value |
|---|---|
| Size of the random population | Riyadh: 1075 Jeddah: 699 |
| Initial number of infected people | 1 |
| Number of days for prediction of infection | 209 |
| Infection rate/probability | 90% |
| Recovery rate | 95.89% |
| Remaining period of virus | 1 day (scenario 1) 4 days (scenario 2) |
| Social distance radius | 2 m |
| Delay | 100 ms |
| Stride ± xy (walking distance) | Variable, (50,300) |
| Recovery period | 14 days [35] |
| Area | 500 × 500 |
| Number of repeated simulations | 30 |
| Day | KSA | Riyadh | Jeddah |
|---|---|---|---|
| 210 | 62 | 0 | 0 |
| 211 | 58 | 0 | 0 |
| 212 | 53 | 0 | 0 |
| 213 | 49 | 0 | 0 |
| 214 | 46 | 0 | 0 |
| 215 | 42 | 0 | 0 |
| 216 | 39 | 0 | 0 |
| 217 | 36 | 0 | 0 |
| 218 | 33 | 0 | 0 |
| 219 | 31 | 0 | 0 |
| 220 | 28 | 0 | 0 |
| 221 | 26 | 0 | 0 |
| 222 | 24 | 0 | 0 |
| 223 | 22 | 0 | 0 |
| Reported Data | Simulation Data | |||
|---|---|---|---|---|
| Riyadh | Jeddah | Riyadh | Jeddah | |
| Curve fitting | 0.73 | 0.82 | 0.984 | 0.999 |
| Period | SMA | WMA | ||||
|---|---|---|---|---|---|---|
| Riyadh | Jeddah | KSA | Riyadh | Jeddah | KSA | |
| 1 | 31.00 | 21.02 | 62.32 | 31.00 | 21.02 | 62.32 |
| 2 | 30.46 | 19.93 | 71.05 | 30.09 | 19.74 | 66.68 |
| 3 | 32.83 | 18.90 | 80.46 | 31.06 | 19.04 | 72.46 |
| 4 | 35.83 | 19.84 | 91.50 | 32.69 | 19.16 | 79.48 |
| 5 | 38.31 | 19.89 | 103.30 | 34.41 | 19.31 | 87.00 |
| 6 | 41.48 | 20.28 | 112.88 | 36.24 | 19.47 | 93.89 |
| 7 | 44.33 | 20.59 | 122.31 | 38.11 | 19.53 | 100.77 |
| 8 | 47.16 | 21.05 | 131.27 | 39.97 | 19.72 | 107.45 |
| 9 | 49.68 | 21.68 | 140.47 | 41.70 | 20.10 | 113.64 |
| 10 | 52.15 | 22.29 | 149.11 | 43.24 | 20.46 | 119.61 |
| Minimum | 30.46 | 18.90 | 62.32 | 30.09 | 19.04 | 62.32 |
| Alpha | ES | ||
|---|---|---|---|
| Riyadh | Jeddah | KSA | |
| 0.1 | 64.17 | 26.08 | 202.54 |
| 0.2 | 44.04 | 21.26 | 128.82 |
| 0.3 | 37.55 | 19.64 | 101.48 |
| 0.4 | 34.42 | 19.18 | 86.51 |
| 0.5 | 32.48 | 19.08 | 77.27 |
| 0.6 | 31.18 | 19.19 | 70.99 |
| 0.7 | 30.50 | 19.47 | 66.68 |
| 0.8 | 30.25 | 19.83 | 63.98 |
| 0.9 | 30.40 | 20.35 | 62.55 |
| Minimum | 30.25 | 19.08 | 62.55 |
| Method | Riyadh | Jeddah | KSA |
|---|---|---|---|
| SMA | 30.5 | 18.9 | 62.3 |
| WMA | 30.1 | 19.0 | 62.3 |
| ES | 30.3 | 19.1 | 62.6 |
| Literature | 25.7 | 19.1 | 59.8 |
| Proposed | 16.3 | 9.6 | 38.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hassanat, A.B.; Mnasri, S.; Aseeri, M.A.; Alhazmi, K.; Cheikhrouhou, O.; Altarawneh, G.; Alrashidi, M.; Tarawneh, A.S.; Almohammadi, K.S.; Almoamari, H. A Simulation Model for Forecasting COVID-19 Pandemic Spread: Analytical Results Based on the Current Saudi COVID-19 Data. Sustainability 2021, 13, 4888. https://doi.org/10.3390/su13094888
Hassanat AB, Mnasri S, Aseeri MA, Alhazmi K, Cheikhrouhou O, Altarawneh G, Alrashidi M, Tarawneh AS, Almohammadi KS, Almoamari H. A Simulation Model for Forecasting COVID-19 Pandemic Spread: Analytical Results Based on the Current Saudi COVID-19 Data. Sustainability. 2021; 13(9):4888. https://doi.org/10.3390/su13094888
Chicago/Turabian StyleHassanat, Ahmad B., Sami Mnasri, Mohammed A. Aseeri, Khaled Alhazmi, Omar Cheikhrouhou, Ghada Altarawneh, Malek Alrashidi, Ahmad S. Tarawneh, Khalid S. Almohammadi, and Hani Almoamari. 2021. "A Simulation Model for Forecasting COVID-19 Pandemic Spread: Analytical Results Based on the Current Saudi COVID-19 Data" Sustainability 13, no. 9: 4888. https://doi.org/10.3390/su13094888
APA StyleHassanat, A. B., Mnasri, S., Aseeri, M. A., Alhazmi, K., Cheikhrouhou, O., Altarawneh, G., Alrashidi, M., Tarawneh, A. S., Almohammadi, K. S., & Almoamari, H. (2021). A Simulation Model for Forecasting COVID-19 Pandemic Spread: Analytical Results Based on the Current Saudi COVID-19 Data. Sustainability, 13(9), 4888. https://doi.org/10.3390/su13094888