Abstract
(1) Background: Schools report a high number of schoolchildren with poor attention and hyperactive behavior, with 5% being diagnosed with attention deficit/hyperactivity disorder (ADHD). This causes specific problems during homework and classroom times, and the extension of all-day schooling in German primary schools makes this a challenge for support staff working in the after-school programs. Such staff have a very wide variety of qualifications, ranging from no formal teacher training to full teaching qualifications. (2) Methods: This study documents the knowledge of 196 support staff working in all-day primary schools about ADHD, and their subjective view of whether they feel competent with regard to homework situations in general and ADHD in particular. (3) Results: Those with an educational background have significantly more knowledge than those without such a background, staff feel less prepared to supervise children with ADHD, and there is a small but significant correlation here with knowledge about ADHD. (4) Conclusions: The importance of trained pedagogical staff in the supervision of children with concentration problems is emphasized.
1. Introduction
Attention deficit/hyperactivity disorder (ADHD) is one of the most common disorders in children and adolescents, with a probability of occurrence of about 5% worldwide [1,2,3]. Originally thought of as a disorder of childhood and adolescence, ADHD has now been shown by long-term studies to have persistence rates in adulthood of between 20% and 80% [4,5].
This underlines the importance of early interventions to counteract negative developments as early as possible [6], with the school context and its associated demands playing a significant role in this respect. When starting school, children are expected to adopt certain behavior, which causes children with ADHD, who have deficits in self-regulation and difficulties in terms of both achievement and social matters. Such children are more at risk of failing at school, achieve lower school-leaving qualifications than their peers, have to repeat a year more often, and are excluded from school more frequently [7,8,9,10]. In addition, comorbid learning disorders, defiant behavior, disorders in social behavior, and fears or depression can appear [11,12,13]. Such children therefore represent a particular challenge for teachers in terms of both performance and social behavior [14]. As a result, the past decade has seen a proliferation of publications on school and ADHD investigating the underlying knowledge that teachers have about ADHD. Questionnaires surveying this knowledge show that, overall, their knowledge is satisfactory with regard to symptoms, behavior, and essential diagnostics, but less satisfactory when it comes to causes, treatments, and interventions. Misconceptions typically manifest in overestimating the frequency of occurrence and in assuming that the disorder will simply grow out in the course of adolescence. Many of the teachers surveyed still believe that the symptoms are caused by errors in upbringing and poor nutrition (e.g., [14,15,16]). Various studies have shown that teachers with more knowledge about ADHD are more likely to have a positive attitude toward children with ADHD and seem to interact more positively with such children (e.g., [17,18]).
Several studies have examined differences in knowledge between groups with varying degrees of experience or training, such as teachers versus students training to be teachers. Although Jerome et al. [19] were unable to find any differences in knowledge between these two groups, a number of subsequent studies (e.g., [17,20,21]) have shown that teachers know significantly more about ADHD than student teachers. In a study by Weyandt et al. [22], school psychologists had a higher level of knowledge than special education teachers and those working in mainstream schools (between whom there were no significant differences). Better knowledge seems to be associated with a higher level of self-efficacy among teachers [23]. Self-efficacy in this context is defined as the expectation of being able to cope successfully with the difficult demands of professional life even under adverse circumstances [24,25], and, in the context of ADHD, means that teachers feel able to address the specific needs of these children and are also more willing to use new teaching methods [26]. West et al. [27] showed that parents with children with ADHD knew more about the condition than teachers. This is not surprising, as parents need to deal with both the diagnosis and the everyday challenges that come with it. Here, the homework situation poses a particular challenge for parents.
Particularly challenging for such children is, like the classroom situation in the morning, the homework situation in the afternoon, since it exposes in many ways their deficits in terms of organization, time management, and planning [28,29]. Children with ADHD therefore have significantly more difficulties with their homework than their classmates, leading more frequently to negative teacher–child and parent–child interactions [30,31]. Homework, then, has a high potential for conflict for such children, and often also places a heavy burden on the interaction partners. How these children do their homework is a key predictor of their later success at school [32].
In recent years, the expansion of all-day schools or after-school programs has shifted responsibility for supervising homework for many children to school or other institutions. In addition to compatibility between family and career, the constant expansion of such schools and programs is intended to achieve another central goal: to support pupils in developing their social and cognitive skills [33]. In Germany, the after-school program is offered on the school’s premises at the end of regular school lessons. The central requirement that parents have (apart from a regular school meal for their child) is that the child does their homework, and almost 90% of primary schools in Germany offer homework supervision by educational staff as learning support. Such staff are extremely heterogeneous across all schools in terms of their qualifications and conditions of employment [34,35]. Increasing numbers of specialist staff working in after-school supervision are therefore facing the special challenges of children with ADHD symptoms.
While considerable efforts have been devoted to helping both parents and teachers in supporting children with ADHD, there is as yet no information on support staff working in after-school supervision at all-day primary schools and how they approach ADHD. This study was intended to provide an initial contribution to the field and to gauge the underlying knowledge and misconceptions of specialist staff about ADHD. As mentioned above, support staff in all-day schools have a wide range of educational qualifications. The comparisons between the level of knowledge shown by, for example, teachers and students training to be teachers allowed us to hypothesize that support staff who have an educational background will know more about ADHD than those who lack such a background. In addition, we investigated how well support staff feel prepared for dealing with the children in the homework situation, and we assumed a positive correlation here with their knowledge about ADHD. Of practical relevance is whether they identify further training needs and, if so, which.
2. Materials and Methods
2.1. Sample
The survey of support staff was conducted at primary schools in the states of North Rhine-Westphalia and Hesse, Germany. We contacted a total of 65 schools in rural areas and medium-sized towns, and 40 schools expressed their willingness to participate. A total of 196 support staff completed the questionnaire, with between 1 and 19 questionnaires being completed per school.
The vast majority of the support staff were women (89.3%), and there was no information regarding the sex of 3.6% of the respondents. The average age was 43.01 years (SD = 14.16 years), with the youngest participant being 17 and the oldest 72 years. The average length of time that they had worked in after-school supervision was 6.65 years (SD = 6.22 years) with a median of 4.75 years. The length of time ranged from half a year to 40 years.
2.2. Instrument of Measurement
To gauge the knowledge of the support staff, we used a questionnaire that was as comparable as possible with questionnaires previously used for teachers. Internationally, teacher surveys generally use the Knowledge of Attention Deficit Disorders Scale (KADDS) [23]. Since not all items in KADDS are appropriate for the German-speaking context, and since there is an imbalance in the number of items on different areas of knowledge, we used a scale in which each area of knowledge is represented by a balanced number of items, with these items in turn having an equal number of right/wrong/do not know statements. We selected the items in line with pilot studies to differentiate as finely as possible between persons with a low and a high level of knowledge [36]. The survey instrument consisted of 24 items covering four areas. To depict uncertain knowledge, too, we used a three-point answer scale with the alternatives: statement is right, statement is wrong, and do not know. The four areas, together with the internal consistency of each according to Cronbach’s alpha, are: (A) symptoms, development, and prevalence (α = 0.59); (B) diagnostics and comorbidity (α = 0.62); (C) causes (α = 0.63), and (D) treatment and knowledge about changes (α = 0.69). The total knowledge value is formed across all items (α = 0.85). Besides surveying the support staff in terms of their knowledge and demographics, a five-point scale (1 = not at all, to 5 = absolutely) was used to investigate how they assessed their competence in dealing with children with ADHD, how prepared they felt for working with such children, and how they evaluated the challenge that dealing with such children involves. Each of these areas was surveyed with a single item (“How competent do you feel in dealing with…?”; “How prepared do you feel to deal with…?”; “How burdened do you feel when dealing with children with poor concentration/hyperactivity?”), the same being asked with regard to homework supervision in general.
To measure their prior experience of ADHD, we asked the support staff to state whether they already had knowledge from vocational training/course of studies, textbooks, further training courses, newspapers/television/Internet, experience at work, or through contact with their own children or children of friends. They were also asked to indicate on a five-point Likert scale whether they felt the need for further training in dealing with ADHD children (0 = not at all, to 4 = absolutely), and in which area they would like to have more knowledge (basic knowledge, supporting children with homework, working with parents, teachers, other institutions). As part of a small pilot study, the questionnaire was checked for comprehensibility as well as applicability and some questions were adapted.
3. Results
Of the 196 support staff surveyed, 64.3% stated that they had been trained in an educational vocation. Table 1 summarizes the information provided by the support staff in detail.

Table 1.
Standard qualifications held by the primary-school support staff (N = 196) surveyed. The two groups of other educational staff as well as staff without qualification in the field of education are further broken down.
3.1. Knowledge about ADHD
The support staff surveyed answered almost half of the statements across all items correctly. Misconceptions were made with regard to 12.7% of the statements; those surveyed said that they had no knowledge when it came to 36.9% of the statements. As Table 2 shows, these percentages vary according to the different areas of knowledge.
Table 2.
Number of items and mean values in the knowledge scales (with standard deviations) in per cent. Due to rounding errors, percentages do not always add up to 100%.
A multivariate analysis of variance with repeated measures indicates differences between the different scales (F(3;579) = 81.34, p < 0.001, = 0.30). Thus, area A (symptoms, development, and prevalence) had higher values than areas B (diagnostics and comorbidity; t(193) = 9.64, p < 0.001, d = 1.19) and C (causes; t(193) = 9.35, p < 0.001, d = 0.93). The same was true for area D (treatment and knowledge about changes), which had higher values than areas B (t(193) = 12.32, p < 0.001, d = 1.74) and C (t(193) = 11.48, p < 0.001, d = 1.33), and than A (t(193) = 2.94, p < 0.01, d = 0.41). The results were comparable when the number of wrong responses or the gaps (do not know) were used. When looking at the percentages descriptively, the “do not know” responses mainly contributed to fewer correct answers.
For each individual item, Table 3 shows the answers to right and wrong statements, as well as the lack of knowledge. Those statements with only one-third or fewer of the respondents answered correctly or, alternatively, one-third or more answered incorrectly, are highlighted in grey.
Table 3.
Knowledge about attention deficit/hyperactivity disorder (ADHD) among support staff at primary schools. Because some data are missing, the percentages do not always add up to 100%.
3.2. Sources of Knowledge and Differences in Knowledge between Groups
The knowledge of those surveyed about ADHD derived in most cases from experience at work (71%, n = 140), with support staff stating that, in an average group size of 13.48 (SD = 5.91), an average of 2.42 (SD = 2.10) children in their groups had ADHD. Other information on ADHD derived from their own vocational training (43%, n = 85), with this group consisting primarily of teachers, social workers, and caregivers (n = 76). Figure 1 provides a summary of the sources of knowledge about ADHD.
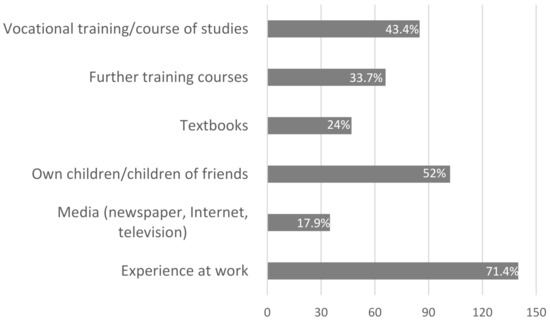
Figure 1.
Sources of knowledge about ADHD: number of support staff (in percent of respondents).
To investigate differences in knowledge between teachers (n = 41), other educational support staff (n = 84, e.g., caregivers, social workers), and staff without an educational background (n = 34), we conducted a univariate analysis of variance with the total knowledge as the dependent variable and the different vocational-training backgrounds as the independent variable. This revealed a significant univariate effect: F(2;156) = 10.63; p < 0.001, = 12. Subsequent post hoc tests showed that there was no difference in knowledge between the group of teachers (M = 0.48, SD = 0.22) and the other educational support staff (M = 0.54, SD = 0.21; t(123) = 1.60, p = 0.12, d = 0.28). However, both the group of teachers (t(73) = 2.68, p < 0.01, d = 0.60) and the group of other educational support staff (t(116) = 4.67, p < 0.001, d = 0.91) differed significantly in their overall knowledge from the group of staff without an educational background (M = 0.35, SD = 0.21). These results were identical when using the do not know responses as the dependent variable, while no statistically significant differences were found for the wrong answers.
3.3. Assessment of Competence and Correlation with Knowledge
Figure 2 shows how well-prepared the support staff feel for working in the context of homework supervision of children with ADHD, and contrasts this with their subjective assessment of how well-prepared they feel for working in the same context with children in general. The mean feeling of being prepared for children with ADHD (1.96, SD = 0.88) differed significantly from the feeling regarding the homework situation in general (M = 2.96; SD = 0.75; t(185) = 15.49, p < 0.001, d = 1.22). In addition, a better feeling of being prepared to homeschool children with ADHD was associated with more knowledge about ADHD (r = 0.21; p < 0.001) and the respondents stated to a lesser extent that further training on ADHD is needed (r = −0.45; p < 0.001).
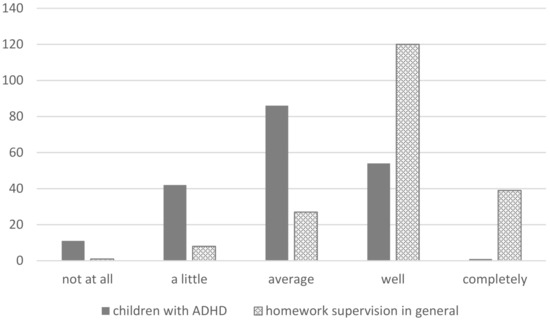
Figure 2.
Responses showing how well-prepared the support staff feel (number of support staff from a total of n = 195).
3.4. Desire for Further Training
When asked whether they had any further training needs for dealing with children with poor concentration and/or hyperactive children in homework supervision, 6% of those surveyed (from a total of n = 191) stated that they felt no need at all, while the overwhelming majority saw a medium (24%), very large (31.1%), or extremely large (19.4%) need for such training. This revealed a small and significantly negative correlation between the subjective need for further training and knowledge about ADHD (r = −0.18; p < 0.01). In particular, “helping these children with their homework” (71.1%) and “basic knowledge about the disorder” (57%) were mentioned by those surveyed as areas where more training was desired. In contrast, cooperation with parents, teachers, and other institutions was somewhat less in demand (35.7%, 33.5% and 24.3%).
4. Discussion
To the best of our knowledge, this is the first study that survey support staff in all-day schools in terms of their knowledge of ADHD. With an average rate of about 50% correct answers, they are at a level of knowledge found in other studies. In a German study [16] of teachers in primary and lower-secondary schools, for example, there was an average of 54.2% correct answers. An international comparison shows a wide range of variation, however: 42.7% correct answers in a Spanish sample [37] and 60.7% in an Australian sample [21]. These fluctuations are difficult to interpret simply because different instruments of measurement were sometimes used.
In addition to the consideration of existing knowledge, the investigation of misconceptions and conscious non-knowledge (gaps) is of interest. Although the latter may lead to further learning and the filling of knowledge gaps, misconceptions tend to be retained (see [23]). By far the strongest misconception identified in the present study is the belief that ADHD grows out with puberty (item 7, about 60%), followed by the belief that excessive media consumption causes the disorder (item 6, about 30%) and the belief that ADHD is not primarily genetically caused (item 19, about 28%). These misconceptions indicate that a significant proportion of support staff do not see ADHD as a problem for which early and long-term support is necessary. At this point, basic education about ADHD as a disorder over the life course, which involves specific interventions in different areas of life, is needed. This would also address existing uncertainties regarding causation and comorbid disorders.
More important here seems to be the differences in knowledge within individual studies that surveyed different groups (e.g., with different degrees of vocational training) (e.g., [21]). In line with these results, the support staff in our study that did not have an educational background knew significantly less about ADHD than those that did have such a background. We also found a small but significant correlation between the level of knowledge about ADHD and their own assessment both of feeling prepared for homework supervision with children with ADHD and of having less need for further training with regard to ADHD.
Previous studies have shown that the homework situation represents a particular challenge for children with ADHD, and is associated with a high potential for conflict with the adults who supervise them. The special challenge is also reflected in the study results here, insofar as a person’s own feeling of competence with regard to dealing with children with ADHD in the homework situation differs significantly from their feeling of competence with regard to the supervision of the homework situation in general. The relevance of appropriate homework supervision is shown in study results not only suggesting that the quality of the homework completed by children with ADHD is a predictor of later success at school [32], but also underlining the positive effects of various interventions in homework supervision for such children. In a study of intervention conducted by Abikoff et al. [28], children with ADHD benefited from parent-based, behavioral-therapy training (including positive attention, when-then contingencies, daily report card). In comparison with the control group, significant effects were observed in terms of the quantity and quality of completed homework. These effects did not occur in the group of children receiving medication alone. The positive effects of behavior-therapy interventions on homework performance were also found in other studies [38]. Precisely because of the very heterogeneous qualifications of support staff in all-day schools, it would be desirable to offer further training about the disorder and provide pedagogical support for these children with their homework. Some studies have reported that further training leads to knowledge acquisition, more targeted use of pedagogical interventions, and a higher level of felt competence and self-efficacy, with both web-based approaches and relatively brief further-training courses of 2.5 h being used [39,40,41]. As mentioned above, knowledge and the felt self-efficacy are related to the willingness to use specific methods to deal with children with ADHD and should be paid more attention in future studies.
The survey used here has some limitations. It was administered in only two regions, and there are regional differences in Germany both in the conceptual design of after-school supervision and in the further training offered to staff. Thus, a larger sample would be desirable in future research work. We did not survey the extent to which greater knowledge about ADHD is associated with the use of appropriate educational interventions. In this context, it would also be interesting to have the support staff assess which strategies they consider to be particularly effective but also feasible, so that this can in turn be incorporated into the further training of support staff. The aim here should be to create conditions that meet the demands of after-school supervision with regard to individual support of, and orientation to, pupil needs.
Author Contributions
Conceptualization, H.D., M.R. and I.L.; methodology, H.D., M.R. and I.L.; formal analysis, H.D. and M.R.; investigation, H.D., M.R. and I.L.; resources, H.D., M.R. and I.L.; data curation, H.D.; writing—original draft preparation, H.D. and M.R.; writing—review and editing, H.D., M.R. and I.L.; visualization, M.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study since no vulnerable samples are examined, and the study does not violate the physical or psychological integrity, the right to privacy or other subjective rights or the interests of study participants.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets are stored at Muenster University of Applied Studies and can be accessed there.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Polanczyk, G.V.; Willcutt, E.G.; Salum, G.A.; Kieling, C.; Rohde, L.A. ADHD prevalence estimates across three decades: An updated systematic review and metaregression analysis. Int. J. Epidemiol. 2014, 43, 434–442. [Google Scholar] [CrossRef] [PubMed]
- Schlack, R.; Mauz, E.; Hebebrand, J.; Hölling, H.; KiGGS Study Group. Hat die Haeufigkeit elternberichteter Diagnosen einer Aufmerksamkeitsdefizit/Hyperaktivitätsstörung (ADHS) in Deutschland zwischen 2003–2006 und 2009–2012 zugenommen? Bundesgesundheitsblatt Gesundh. Gesundh. 2014, 57, 820–829. [Google Scholar] [CrossRef] [PubMed]
- Willcutt, E.G. The prevalence of DSMIV attentiondeficit/hyperactivity disorder: A meta-analytic review. Neurotherapeutics 2012, 9, 490–499. [Google Scholar] [CrossRef] [PubMed]
- Fischer, M.; Barkley, R.A. The persistence of ADHD into adulthood: (once again) it depends on whom you ask. ADHD Rep. 2007, 7–16. [Google Scholar] [CrossRef]
- Steinhausen, H.-C.; Drechsler, R.; Földényi, M.; Imhof, K.; Brandeis, D. Clinical course of attention-deficit/hyperactivity disorder from childhood toward early adolescence. J. Am. Acad. Child Adolesc. Psychiatry 2003, 42, 1085–1092. [Google Scholar] [CrossRef] [PubMed]
- Christiansen, H. Aufmerksamkeitsdefizit-/Hyperaktivitätsstörung über die Lebensspanne. Verhaltenstherapie 2016, 26, 182–193. [Google Scholar] [CrossRef]
- Barbaresi, W.J.; Katusic, S.K.; Colligan, R.C.; Weaver, A.L.; Jacobsen, S.J. Long-term school outcomes for children with attention-deficit / hyperactivity dirsorder: A population-based perspective. J. Dev. Behav. Pediatrics 2007, 28, 265–273. [Google Scholar] [CrossRef]
- Fried, R.; Petty, C.; Faraone, S.V.; Hyder, L.L.; Day, H.; Biederman, J. Is ADHD a risk factor for high school dropout? A controlled study. J. Atten. Disord. 2016, 20, 383–389. [Google Scholar] [CrossRef]
- Loe, I.M.; Feldman, H.M. Academic and educational outcomes of children with ADHD. J. Pediatr. Psychol. 2007, 32, 643–654. [Google Scholar] [CrossRef]
- McConaughy, S.H.; Volpe, R.J.; Antshel, K.M.; Gordon, M.; Eiraldi, R.B. Academic and social impairments of elementary school children with attention deficit hyperactivity disorder. Sch. Psychol. Rev. 2011, 40, 200–225. [Google Scholar] [CrossRef]
- Barkley, R.A. Attentiondeficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment; Guilford Press: New York, NY, USA, 2006. [Google Scholar]
- Kain, W.; Landerl, K.; Kaufmann, L. Komorbidität bei ADHS. Mon. Kinderheilkd. 2008, 156, 757–767. [Google Scholar] [CrossRef]
- Schuchardt, K.; Grube, D.; Mähler, C. “Schwierige Kinder” von Anfang an? Kindh. Entwickl. 2013, 22, 217–223. [Google Scholar] [CrossRef]
- Ruhmland, M.; Christiansen, H. Konzepte zu Grundlagen von ADHS und Interventionen im Unterricht bei Grundschullehrkräften. Psychol. Erzieh. Unterr. 2017, 64, 109–120. [Google Scholar] [CrossRef]
- Sciutto, M.J.; Terjesen, M.D.; Kucerová, A.; Michalová, Z.; Schmiedeler, S.; Antonopoulou, K.; Drake, B.; Rossouw, J. Cross-national comparisions of teachers´ knowledge and misconceptions of ADHD. Int. Perspect. Psychol. Res. Pract. Consult. 2016, 5, 34–50. [Google Scholar]
- Schmiedeler, S. Wissen und Fehlannahmen von deutschen Lehrkräften über die Aufmerksamkeitsdefizit-/Hyperaktivitätsstörung (ADHS). Psychol. Erzieh. Unterr. 2013, 60, 143–153. [Google Scholar] [CrossRef]
- Bekle, B. Knowledge and attitudes about Attention-Deficit Hyperactivity Disorder (ADHD): A comparison between practicing teachers and undergraduate education students. J. Atten. Disord. 2004, 7, 151–161. [Google Scholar] [CrossRef]
- Ohan, J.L.; Visser, T.A.W.; Strain, M.C.; Allen, L. Teachers’ and education students’ perceptions of and reactions to children with and without the diagnostic label “ADHD”. J. Sch. Psychol. 2011, 49, 81–105. [Google Scholar] [CrossRef]
- Jerome, L.; Washington, P.; Laine, C.J.; Segal, A. Graduating teachers’ knowledge and attitudes about attention-deficit hyperactivity disorder: a comparison with practicing teachers. Canadian journal of psychiatry. Rev. Can. Psychiatr. 1999, 44, 192. [Google Scholar]
- Anderson, D.L.; Watt, S.E.; Noble, W.; Shanley, D.C. Knowledge of attention deficit hyperactivity disorder (ADHD) and attitudes toward teaching children with ADHD: THE role of teaching experience. Psychol. Sch. 2012, 49, 511–525. [Google Scholar] [CrossRef]
- Kos, J.M.; Richdale, A.L.; Jackson, M.S. Knowledge about Attention-Deficit/Hyperactivity Disorder: A comparison of in-service and preservice teachers. Psychol. Sch. 2004, 41, 517–526. [Google Scholar] [CrossRef]
- Weyandt, L.L.; Fulton, K.M.; Schepman, S.B.; Verdi, G.R.; Wilson, K.G. Assessment of teacher and school psychologist knowledge of Attention-Deficit/Hyperactivity Disorder. Psychol. Sch. 2009, 46, 951–961. [Google Scholar] [CrossRef]
- Sciutto, M.J.; Terjesen, M.D.; Bender Frank, A.S.B. Teachers’ knowledge and misperceptions of attention-deficit/hyperactivity disorder. Psychol. Sch. 2000, 37, 115–122. [Google Scholar] [CrossRef]
- Bandura, A. Self-efficacy: toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef] [PubMed]
- Tschannen-Moran, M.; Hoy, A.W. Teacher efficacy: Capturing an elusive construct. Teach. Teach. Educ. 2001, 17, 783–805. [Google Scholar] [CrossRef]
- Latouche, A.P.; Gascoigne, M. In-service training for increasing teachers’ ADHD knowledge and self-efficacy. J. Atten. Disord. 2019, 23, 270–281. [Google Scholar] [CrossRef]
- West, J.; Taylor, M.; Houghton, S.; Hudyma, S. A Comparison of Teachers’ and Parents’ Knowledge and Beliefs About Attention-Deficit/Hyperactivity Disorder(ADHD). Sch. Psychol. Int. 2005, 26, 192–208. [Google Scholar] [CrossRef]
- Abikoff, H.; Gallagher, R.; Wells, K.C.; Murray, D.W.; Huang, L.; Lu, F.; Petkova, E. Remediating organizational functioning in children with ADHD: immediate and long-term effects from a randomized controlled trial. J. Consult. Clin. Psychol. 2013, 81, 113–128. [Google Scholar] [CrossRef]
- Merrill, B.M.; Morrow, A.S.; Altszuler, A.R.; Macphee, F.L.; Gnagy, E.M.; Greiner, A.R.; Coles, E.K.; Raiker, J.S.; Coxe, S.; Pelham, W.E. Improving homework performance among children with ADHD: A randomized controlled clinical trial. J. Consult. Clin. Psychol. 2017, 85, 111–122. [Google Scholar] [CrossRef]
- Power, T.J.; Werba, B.E.; Watkins, M.W.; Angelucci, J.G.; Eiraldi, R.B. Patterns of parent-reported homework problems among ADHD-referred and non-referred children. Sch. Psychol. Q. 2006, 21, 13–33. [Google Scholar] [CrossRef]
- Rogers, M.A.; Wiener, J.; Marton, I.; Tannock, R. Parental involvement in children’s learning: comparing parents of children with and without Attention-Deficit/Hyperactivity Disorder (ADHD). J. Sch. Psychol. 2009, 47, 167–185. [Google Scholar] [CrossRef]
- Langberg, J.M.; Dvorsky, M.R.; Molitor, S.J.; Bourchtein, E.; Eddy, L.D.; Smith, Z.; Schuitz, B.K.; Evans, S.W. Longitudinal evaluation of the importance of homework assignement competition for the academic performance of middle school students with ADHD. J. Sch. Psychol. 2016, 55, 27–38. [Google Scholar] [CrossRef]
- Durlak, J.A.; Weissberg, R.P.; Pachan, M. A meta-analysis of after-school programs that seek to promote personal and social skills in children and adolescents. Am. J. Community Psychol. 2010, 45, 294–309. [Google Scholar] [CrossRef]
- Steiner, C.; Tillmann, K. Koordinierte Vielfalt? Über die Arbeit in multiprofessionellen Ganztagsteams. In Ganztagsschulische Kooperation und Professionsentwicklung. Studien zu multiprofessionellen Teams und sozialräumlicher Vernetzung; Speck, K., Olk, T., Böhm-Kasper, O., Stolz, H.-J., Wiezorek, C., Eds.; Belz/Juventa: Weinheim, Germany; Basel, Switzerland, 2011; pp. 48–68. [Google Scholar]
- Fischer, N.; Klieme, E.; Holtappels, H.G.; Stecher, L.; Rauschenbach, T. Ganztagsschule 2012/2013. Deskriptive Befunde einer bundesweiten Befragung; DIPF/IFS/JLU/DJI: Frankfurt, Germany, 2013. [Google Scholar]
- Stellmacher, J.; Ruhmland, M.; Schwinger, M.; Christiansen, H. Was wissen Lehramtsstudierende und Lehrkräfte über ADHS? Internal Research Paper; Marburg University, Department of Psychology: Marburg, Germany, 2016. [Google Scholar]
- Fernández, S.J.; Mínguez, R.T.; Casas, A.M. Conocimientos, concepciones erróneas y lagunas de los maestros sobre el trastorno por déficit de atención con hiperactividad. Psicothema 2007, 19, 585–590. [Google Scholar]
- Power, T.J.; Mautone, J.A.; Soffer, S.L.; Clarke, A.T.; Marshall, S.A.; Sharman, J.; Blum, N.J.; Marianne, G.; Elia, J.; Jawad, A.F. A family–school intervention for children with ADHD: Results of a randomized clinical trial. J. Consult. Clin. Psychol. 2012, 80, 611–623. [Google Scholar] [CrossRef]
- Barnett, B.; Corkum, P.; Elik, N. A web-based intervention for elementary school teachers of students with attention-deficit/hyperactivity disorder (ADHD). Psychol. Serv. 2012, 9, 227–230. [Google Scholar] [CrossRef]
- Both, F.; Schmiedeler, S.; Abelein, P.; Schneider, W. Wirksamkeit eines Workshops für Lehrkräfte über die Aufmerksamkeitsdefizit-/Hyperaktivitätsstörung (ADHS). Prax. Kinderpsychol. Kinderpsychiatr. 2016, 65, 315–327. [Google Scholar] [CrossRef]
- Jones, H.A.; Chronis-Tuscano, A. Efficacy of teacher in-service training for attention-deficit/hyperactivity disorder. Psychol. Sch. 2008, 45, 918–929. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).