
Time-Use and Spatio-Temporal Variables Influence on Physical Activity Intensity, Physical and Social Health of Travelers

 ,
,  ,
,  , and
, and
Abstract
:1. Introduction
2. The Bandung Metropolitan Area (BMA) Data Set
2.1. Data Set
2.2. Methods
3. Exploratory Analysis
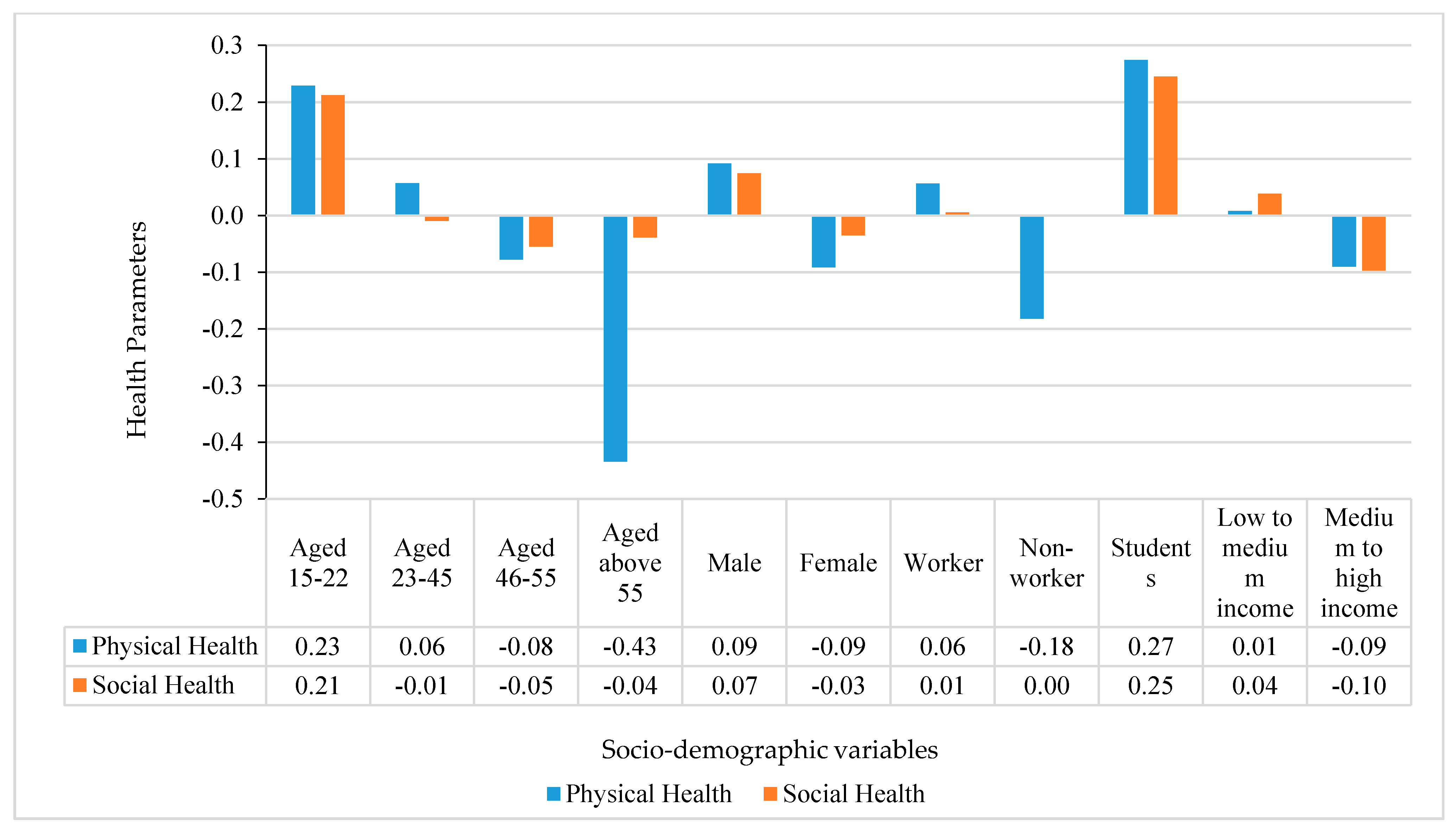
3.1. Physical Activities at Socio-Demographic Level
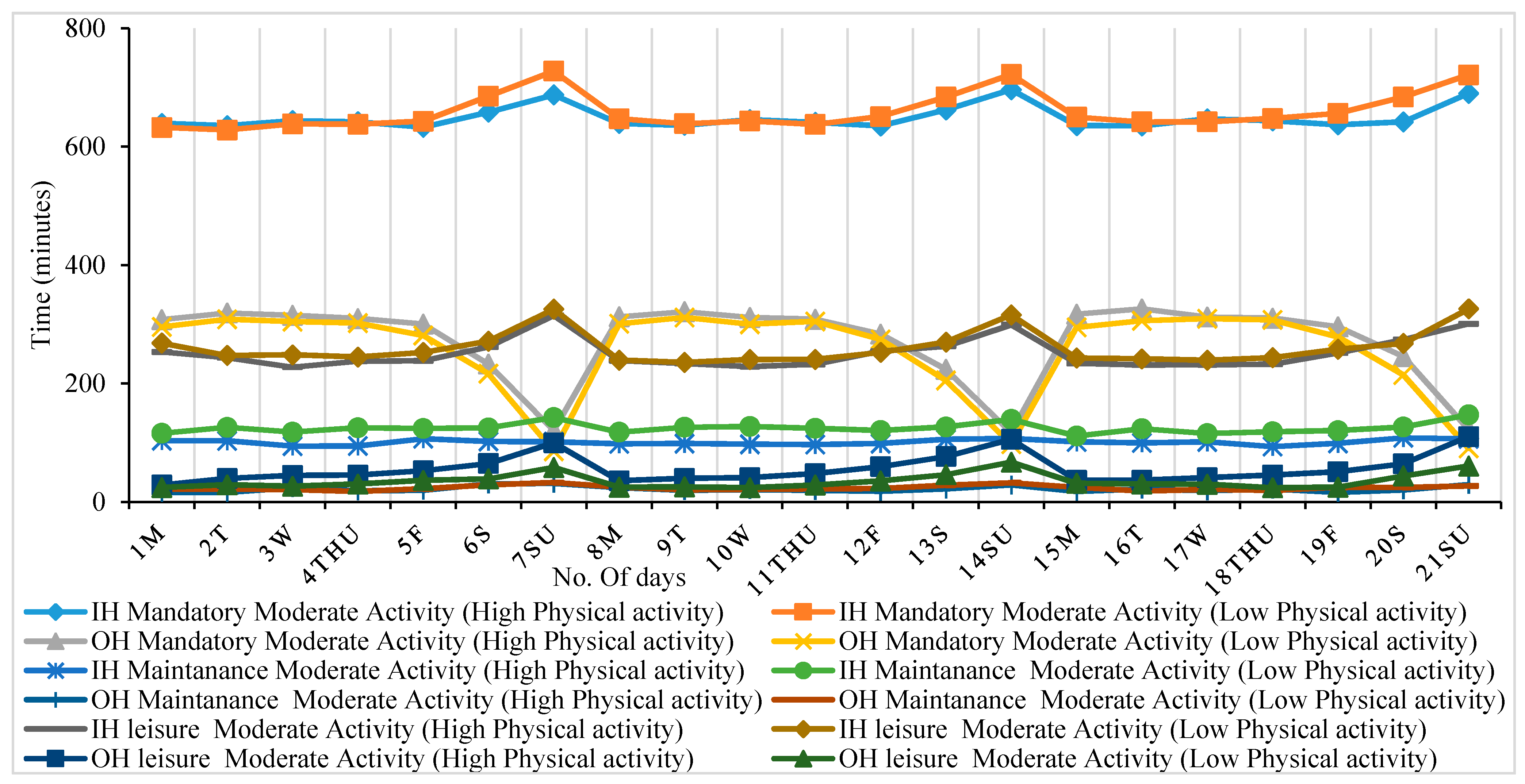
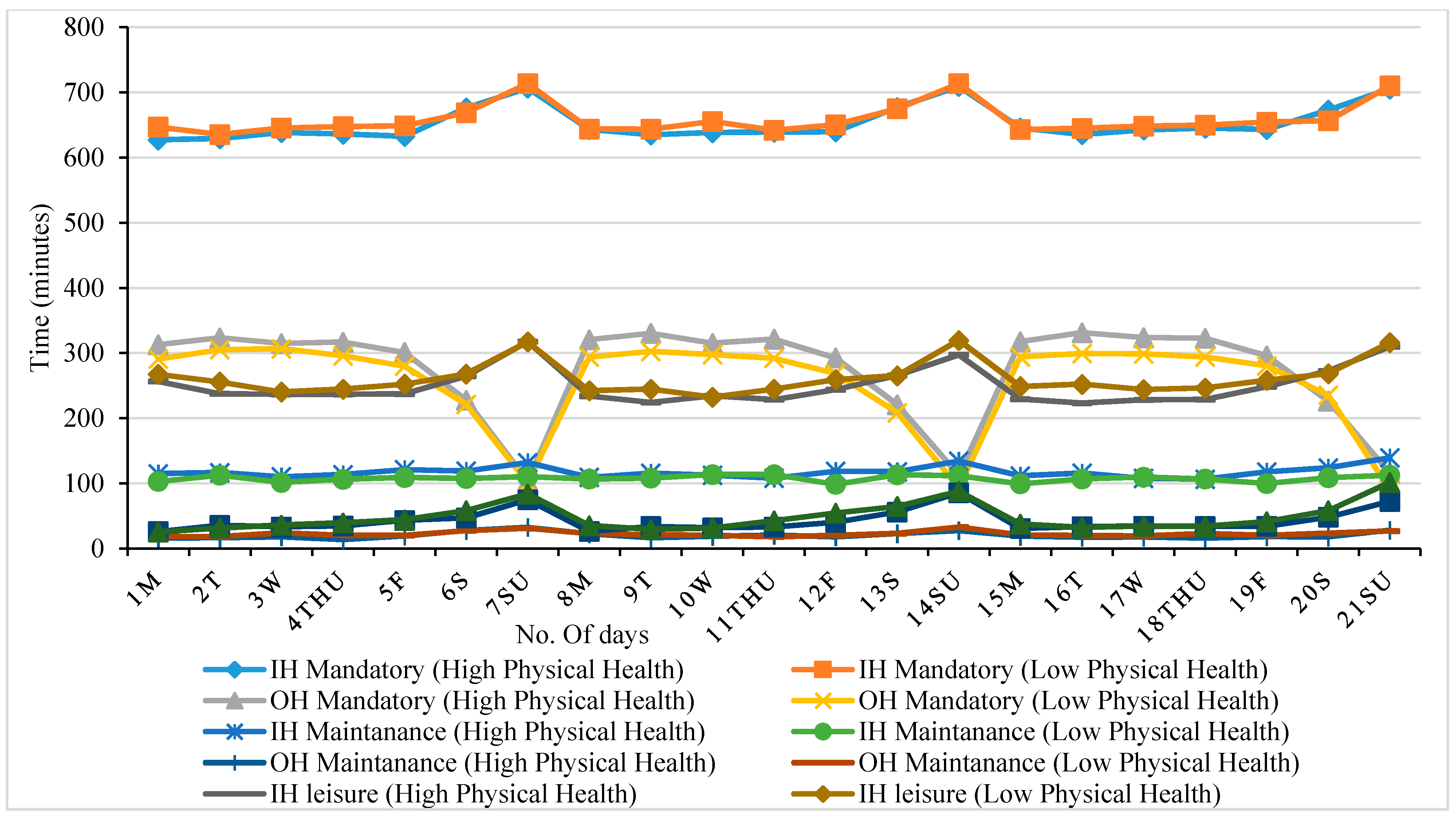
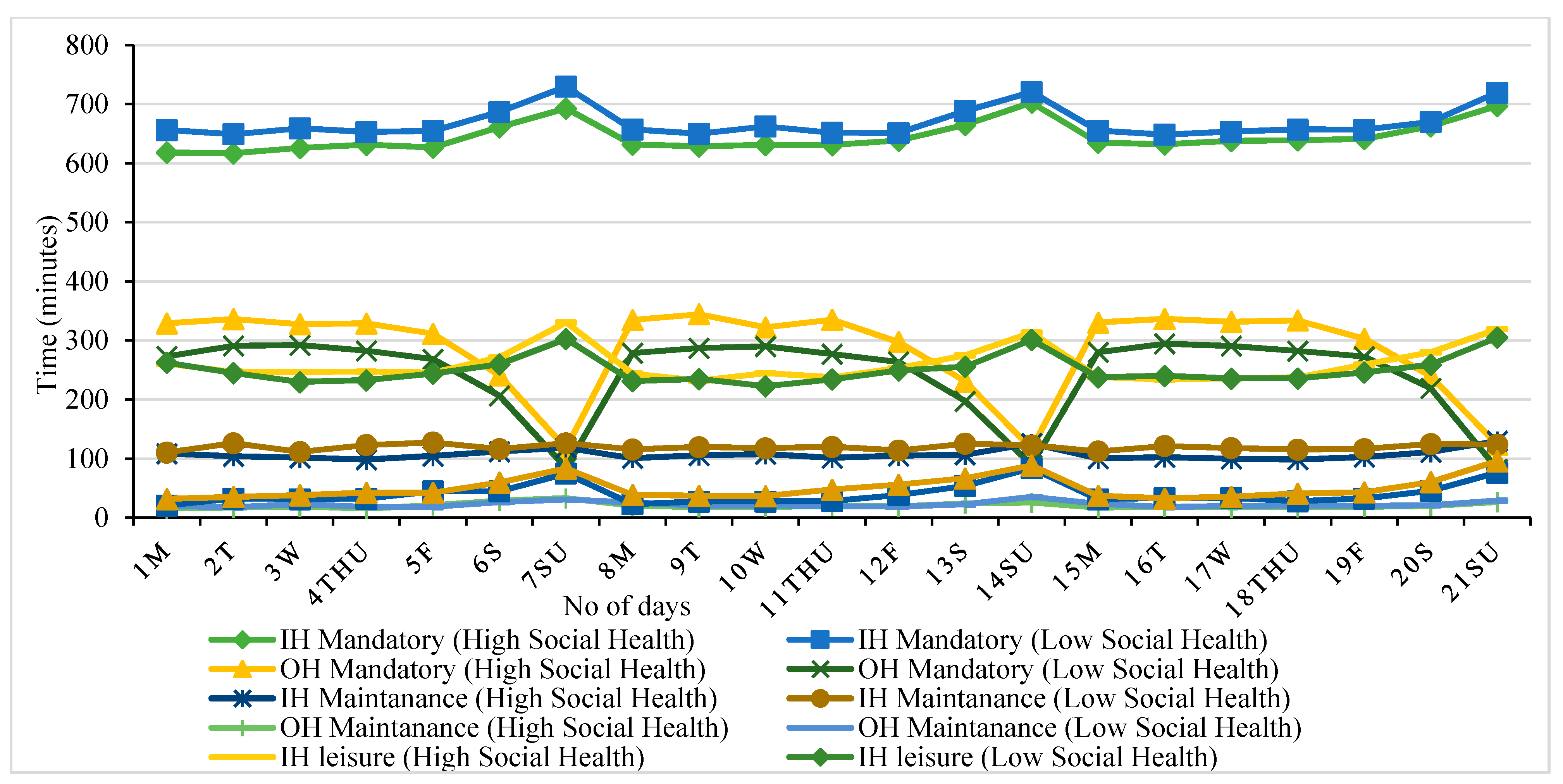
3.2. Daily Time-Use for Various Activities
4. Model Estimation Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Miller, H.J. A Measurement Theory for Time Geography. Geogr. Anal. 2005, 37, 17–45. [Google Scholar] [CrossRef]
- Miller, H.J. Modelling Accessibility Using Space-Time Prism Concepts within Geographical Information Systems. Int. J. Geogr. Inf. Syst. 1991, 5, 287–301. [Google Scholar] [CrossRef]
- Corbett, J. Torsten Hӓgerstrand, Time Geography. Available online: https://is.muni.cz/el/1431/jaro2006/Z0147/time_geography.pdf (accessed on 26 October 2021).
- Neutens, T.; Schwanen, T.; Witlox, F. The Prism of Everyday Life: Towards a New Research Agenda for Time Geography. Transp. Rev. 2011, 31, 25–47. [Google Scholar] [CrossRef]
- Fauzi, N.F.M.; Dharmowijoyo, D.B.E. Activity-Travel Participation, Multitasking in Travel and Daily Well-Being. In MATEC Web of Conferences; EDP Sciences: Ulis, France, 2019; Volume 270, p. 8. [Google Scholar] [CrossRef] [Green Version]
- Dharmowijoyo, D.B.; Susilo, Y.O.; Karlström, A.; Adiredja, L.S. Collecting a Multi-Dimensional Three-Weeks Household Time-Use and Activity Diary in the Bandung Metropolitan Area, Indonesia. Transp. Res. Part A Policy Pract. 2013, 80, 231–246. [Google Scholar] [CrossRef]
- Dharmowijoyo, D.B.; Joewono, T.B. Mobility and Health: The Interaction of Activity-Travel Patterns, Overall Well-Being, Transport-Related Social Exclusion on Health Parameters. In Energy Efficiency in Mobility Systems; Springer: Boston, MA, USA, 2020; pp. 53–83. [Google Scholar]
- Susilo, Y.O.; Liu, C. The Influence of Parents’ Travel Patterns, Perceptions and Residential Self-Selectivity to Their Children Travel Mode Shares. Transportation 2016, 43, 357–378. [Google Scholar] [CrossRef]
- Pereira, A. Live and Let Live: Healthcare Is a Fundamental Human Right. Conn. Public Interest Law J. 2003, 3, 481. [Google Scholar]
- Axhausen, K.W. Concepts of Travel Behaviour Research, in Threats from Car Traffic to the Quality of Urban Life: Problems, Causes and Solutions; Gärling, T., Steg, L., Eds.; Emerald Group Publishing Limited: Bingley, UK, 2007; pp. 165–185. [Google Scholar]
- Wee, B.V.; Ettema, D. Travel Behaviour and Health: A Conceptual Model and Research Agenda. J. Transp. Health 2016, 3, 240–248. [Google Scholar] [CrossRef] [Green Version]
- Acker, V.V.; Van Wee, B.; Witlox, F. When Transport Geography Meets Social Psychology: Toward a Conceptual Model of Travel Behaviour. Transp. Rev. 2010, 30, 219–240. [Google Scholar] [CrossRef] [Green Version]
- Bhat, C.R.; Koppelman, F.S. Activity-Based Modeling of Travel Demand. In Handbook of Transportation Science; Springer: Boston, MA, USA, 1999; pp. 35–61. [Google Scholar]
- Schwanen, T.; Kwan, M.-P.; Ren, F. How Fixed Is Fixed? Gendered Rigidity of Space–Time Constraints and Geographies of Everyday Activities. Geoforum 2008, 39, 2109–2121. [Google Scholar] [CrossRef]
- Cullen, I.; Godson, V. Urban Networks: The Structure of Activity Patterns. Prog. Plan. 1975, 4, 1–96. [Google Scholar] [CrossRef]
- Ali, M.; Dharmowijoyo, D.B.; Harahap, I.S.; Puri, A.; Tanjung, L.E. Travel Behaviour and Health: Interaction of Activity-Travel Pattern, Travel Parameter and Physical Intensity. Solid State Technol. 2020, 63, 4026–4039. [Google Scholar]
- Petersen, J.; Austin, D.; Mattek, N.; Kaye, J. Time Out-of-Home and Cognitive, Physical, and Emotional Wellbeing of Older Adults: A Longitudinal Mixed Effects Model. PLoS ONE 2015, 10, e0139643. [Google Scholar] [CrossRef] [PubMed]
- Ramli, M.I.; Dharmowijoyo, D.E. Activity-Travel Behaviour, and Daily and Global Well-Being. In MATEC Web of Conferences; EDP Sciences: Ulis, France, 2018; Volume 203, p. 11. [Google Scholar] [CrossRef]
- Susilo, Y.O.; Dijst, M. How Far Is Too Far? Travel Time Ratios for Activity Participation in the Netherlands. Transp. Res. Rec. J. Transp. Res. Board 2009, 2134, 89–98. [Google Scholar] [CrossRef]
- Huang, Y.; Kockelman, K.M.; Quarles, N. How Will Self-Driving Vehicles Affect U.S. Megaregion Traffic? The Case of the Texas Triangle. Res. Transp. Econ. 2020, 84, 101003. [Google Scholar] [CrossRef]
- Hansson, S.O.; Belin, M.-Å.; Lundgren, B. Self-Driving Vehicles—An Ethical Overview. Philos. Technol. 2021. [Google Scholar] [CrossRef]
- Farber, S.; Páez, A. My Car, My Friends, And Me: A Preliminary Analysis of Automobility and Social Activity Participation. J. Transp. Geogr. 2009, 17, 216–225. [Google Scholar] [CrossRef]
- Arroyo, R.; Mars, L.; Ruiz, T. Perceptions of Pedestrian and Cyclist Environments, Travel Behaviors, and Social Networks. Sustainability 2018, 10, 3241. [Google Scholar] [CrossRef] [Green Version]
- Macioszek, E.; Kurek, A. P&R Parking and Bike-Sharing System As Solutions Supporting Transport Accessibility of the City. Transp. Probl. 2020, 15, 275–286. [Google Scholar]
- Macioszek, E.; Kurek, A. The Use of a Park and Ride System—A Case Study Based on the City of Cracow (Poland). Energies 2020, 13, 3473. [Google Scholar] [CrossRef]
- Hodgson, S.; Namdeo, A.; Araujo-Soares, V.; Pless-Mulloli, T. Towards an Interdisciplinary Science of Transport and Health: A Case Study on School Travel. J. Transp. Geogr. 2012, 21, 70–79. [Google Scholar] [CrossRef] [Green Version]
- Ammad, S.; Alaloul, W.S.; Saad, S.; Qureshi, A.H.; Sheikh, N.; Ali, M.; Altaf, M. Personal Protective Equipment In Construction, Accidents Involved In Construction Infrastructure Projects. Solid State Technol. 2020, 63, 4147–4159. [Google Scholar]
- Wee, B.V. The Traffic and Transport System and Effects on Accessibility, the Environment and Safety: An Introduction. In Transport System and Transport Policy; van Wee, B., Annema, J.A., Banister, D., Eds.; Edward Elgar Publishing: Cheltenham, UK, 2013; pp. 4–18. [Google Scholar]
- Mackett, R.L.; Thoreau, R. Transport, Social Exclusion and Health. J. Transp. Health 2015, 2, 610–617. [Google Scholar] [CrossRef]
- Memon, A.M.; Sutanto, M.H.; Napiah, M.; Yusoff, N.I.M.; Memon, R.A.; Al-Sabaeei, A.M.; Ali, M. Physicochemical, Rheological and Morphological Properties of Bitumen Incorporating Petroleum Sludge. Constr. Build. Mater. 2021, 297, 123738. [Google Scholar] [CrossRef]
- Zhang, J. Urban Forms and Health Promotion: An Evaluation Based on Health-Related QOL Indicators. In Proceedings of the 13th World Conference on Transportation Research, Rio de Janeiro, Brazil, 15–18 July 2013. [Google Scholar]
- Dharmowijoyo, D.B.; Susilo, Y.O.; Syabri, I. Time Use and Spatial Influence on Transport-Related Social Exclusion, and Mental and Social Health. Travel Behav. Soc. 2020, 21, 24–36. [Google Scholar] [CrossRef]
- Raglin, J.S. Exercise and Mental Health. Sports Med. 1990, 9, 323–329. [Google Scholar] [CrossRef]
- de Azevedo, A.R.G.; Marvila, M.T.; Ali, M.; Khan, M.I.; Masood, F.; Vieira, C.M.F. Effect of the Addition and Processing of Glass Polishing Waste on the Durability of Geopolymeric Mortars. Case Studies Constr. Mater. 2021, 15, e00662. [Google Scholar] [CrossRef]
- Dharmowijoyo, D.B.; Susilo, Y.O.; Karlström, A. Day-to-Day Interpersonal and Intrapersonal Variability of Individuals’ Activity Spaces in a Developing Country. Envir. Plan. B Plan. Des. 2014, 41, 1063–1076. [Google Scholar] [CrossRef]
- Barreto, E.D.; Stafanato, K.V.; Marvila, M.T.; de Azevedo, A.R.; Ali, M.; Pereira, R.M.; Monteiro, S.N. Clay Ceramic Waste as Pozzolan Constituent in Cement for Structural Concrete. Materials 2021, 14, 2917. [Google Scholar] [CrossRef]
- Krejcie, R.V.; Morgan, D.W. Determining Sample Size for Research Activities. Educ. Psychol. Meas. 1970, 30, 607–610. [Google Scholar] [CrossRef]
- Ali, M.; de Azevedo, A.R.G.; Marvila, M.T.; Khan, M.I.; Memon, A.M.; Masood, F.; Almahbashi, N.M.; Shad, M.K.; Khan, M.A.; Fediuk, R.; et al. The Influence of COVID-19-Induced Daily Activities on Health Parameters—A Case Study in Malaysia. Sustainability 2021, 13, 7465. [Google Scholar] [CrossRef]
- Tarigan, A.K.; Sagala, S.; Samsura, D.A.A.; Fiisabiilillah, D.F.; Simarmata, H.A.; Nababan, M. Bandung City, Indonesia. Cities 2016, 50, 100–110. [Google Scholar] [CrossRef]
- Tarigan, A.K.; Susilo, Y.O.; Joewono, T.B. Segmentation of Paratransit Users Based on Service Quality and Travel Behaviour in Bandung, Indonesia. Transp. Plan. Technol. 2014, 37, 200–218. [Google Scholar] [CrossRef]
- Ali, M.; Abbas, S.; Salah, B.; Akhter, J.; Saleem, W.; Haruna, S.; Room, S.; Abdulkadir, I. Investigating Optimal Confinement Behaviour of Low-Strength Concrete through Quantitative and Analytical Approaches. Materials 2021, 14, 4675. [Google Scholar] [CrossRef]
- Lwanga, S.K.; Lemeshow, S. Sample Size Determination in Health Studies: A Practical Manual; World Health Organization: Geneva, Switzerland, 1991; Available online: https://apps.who.int/iris/handle/10665/40062 (accessed on 26 October 2021).
- Ali, M.; Room, S.; Khan, M.I.; Masood, F.; Ali Memon, R.; Khan, R.; Memon, A.M. Assessment of Local Earthen Bricks in Perspective of Physical and Mechanical Properties Using Geographical Information System in Peshawar, Pakistan. In Structures; Elsevier: London, UK, 2020; Volume 28, pp. 2549–2561. [Google Scholar] [CrossRef]
- Axhausen, K.W.; Zimmermann, A.; Schönfelder, S.; Rindsfüser, G.; Haupt, T. Observing the Rhythms of Daily Life: A Six-Week Travel Diary. Transportation 2002, 29, 95–124. [Google Scholar] [CrossRef]
- Akar, G.; Clifton, K.J.; Doherty, S.T. Discretionary Activity Location Choice: In-Home or Out-of-Home? Transportation 2011, 38, 101–122. [Google Scholar] [CrossRef]
- Suzukamo, Y.; Fukuhara, S.; Green, J.; Kosinski, M.; Gandek, B.; Ware, J.E. Validation Testing of a Three-Component Model of Short Form-36 Scores. J. Clin. Epidemiol. 2011, 64, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.; Abbas, S.; Khan, M.I.; Gad, M.A.; Ammad, S.; Khan, A. Experimental Validation of Mander’s Model for Low Strength Confined Concrete Under Axial Compression. In 2020 Second International Sustainability and Resilience Conference: Technology and Innovation in Building Designs(51154), Proceedings of the 2020 Second International Sustainability and Resilience Conference, Sakheer, Bahrain, 11–12 November 2020; IEEE: Piscataway, NJ, USA, 2021. [Google Scholar] [CrossRef]
- DiStefano, C.; Zhu, M.; Mindrila, D. Understanding and Using Factor Scores: Considerations for the Applied Researcher. Pract. Assess. Res. Eval. 2009, 14, 20. [Google Scholar] [CrossRef]
- Yong, A.G.; Pearce, S. A Beginner’s Guide to Factor Analysis: Focusing on Exploratory Factor Analysis. Tutor. Quant. Methods Psychol. 2013, 9, 79–94. [Google Scholar] [CrossRef]
- Baiocchi, M.; Cheng, J.; Small, D.S. Instrumental Variable Methods for Causal Inference. Stat. Med. 2014, 33, 2297–2340. [Google Scholar] [CrossRef] [Green Version]
- Rhodes, R.E.; Blanchard, C.M.; Blacklock, R.E. Do Physical Activity Beliefs Differ by Age and Gender? J. Sport Exerc. Psychol. 2008, 30, 412–423. [Google Scholar] [CrossRef]
- Azevedo, M.R.; Araújo, C.L.P.; Reichert, F.F.; Siqueira, F.V.; da Silva, M.C.; Hallal, P.C. Gender Differences in Leisure-Time Physical Activity. Int. J. Public Health 2007, 52, 8. [Google Scholar] [CrossRef] [Green Version]
- Mueller, N.; Rojas-Rueda, D.; Cole-Hunter, T.; De Nazelle, A.; Dons, E.; Gerike, R.; Goetschi, T.; Panis, L.I.; Kahlmeier, S.; Nieuwenhuijsen, M. Health Impact Assessment of Active Transportation: A Systematic Review. Prev. Med. 2015, 76, 103–114. [Google Scholar] [CrossRef]
- De Hartog, J.J.; Boogaard, H.; Nijland, H.; Hoek, G. Do the Health Benefits of Cycling Outweigh the Risks? Environ. Health Perspect. 2010, 118, 1109–1116. [Google Scholar] [CrossRef] [PubMed]
- Ettema, D.; Verschuren, L. Multitasking and Value of Travel Time Savings. Transp. Res. Rec. 2007, 2010, 19–25. [Google Scholar] [CrossRef]
- Kang, H.; Scott, D.M. Exploring Day-to-Day Variability in Time Use for Household Members. Transp. Res. A Policy Pract. 2010, 44, 609–619. [Google Scholar] [CrossRef]
- Novaco, R.W.; Gonzalez, O.I. Commuting and Well-Being. In Technology and Well-Being; Cambridge University Press: Cambridge, UK, 2009; pp. 174–205. [Google Scholar]
- DiPietro, L. Physical Activity in Aging: Changes in Patterns and Their Relationship to Health and Function. J. Gerontol. Ser. A 2001, 56, 13–22. [Google Scholar] [CrossRef]
- Roberts, R.; Golding, J.; Towell, T.; Reid, S.; Woodford, S.; Vetere, A.; Weinreb, I. Mental and Physical Health in Students: The Role of Economic Circumstances. Br. J. Health Psychol. 2000, 5, 289–297. [Google Scholar] [CrossRef]
- Lum, T.Y.; Lightfoot, E. The Effects of Volunteering on the Physical and Mental Health of Older People. Res. Aging 2005, 27, 31–55. [Google Scholar] [CrossRef]
- Renalds, A.; Smith, T.H.; Hale, P.J. A Systematic Review of Built Environmenta Health. Fam. Community Health 2010, 33, 68–78. [Google Scholar] [CrossRef]
- Pappalardo, G.; Cafiso, S.; Di Graziano, A.; Severino, A. Decision Tree Method to Analyze the Performance of Lane Support Systems. Sustainability 2021, 13, 846. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Percentage or Mean |
|---|---|
| Socio-demographic characteristic at individual level | |
| Male | 53.54% |
| Female | 46.45% |
| Worker | 40.0% |
| Non-worker | 26.5% |
| Student | 32.0% |
| Dependent Children (<15 years) | 18.66% |
| Age below 22–15 (Years old) | 18.34% |
| Age below 44–23 (Years old) | 42.50% |
| Age below 55–45 (Years old) | 11.70% |
| Age above 55 years old | 9.50% |
| Medium household income (3–6 IDR) | 91.5% |
| High household income (>6 million) | 8.5% |
| Household Characteristics | |
| Number of members in a household | 4.20 |
| Dependent children per household | 0.45 |
| Number of the motorized vehicle per household | 1.073 |
| Trip engagement and travel time spend on weekdays (weekends) | |
| Number of trips | 2.52 (2.29) |
| Trip chains | 1.20 (1.08) |
| Travel time by a motorized mode (%) | 45.59% |
| Travel time by Non-motorized mode (%) | 29.31% |
| Travel time by public transport (%) | 11.62% |
| Total travel time (minutes) | 98.29 |
| Intensity of a physical activity | |
| Days perform strenuous-intensity physical activity (S-IPA) (Frequency) | 4.5 |
| Minutes/day to perform (S-IPA) (duration) | 52.54 |
| Days perform moderate-intensity physical activity (M-IPA) (Frequency) | 4.83 |
| Minutes/day to perform (M-IPA) (duration) | 56.21 |
| Low-intensity physical activity | 58.2% |
| Medium intensity physical activity | 32.2% |
| High-intensity physical activity | 9.6% |
| Time spend on a different set of activities on weekdays (weekends) | |
| Time spend on in-home mandatory activities (minutes) | 659.91 (704.92) |
| Time spend on in-home maintenance activities (minutes) | 105.29 (143.39) |
| Time spend on in-home leisure activities (minutes) | 247.04 (291.14) |
| Time spend on out-of-home mandatory activities (minutes) | 300 (164) |
| Time spend for out-of -home maintenance/grocery activities (minutes) | 21.26 (29.62) |
| Time spend on out-of-home leisure activities (minutes) | 25.43 (35.65) |
| Perceived accessibility variables | |
| Public transport lanes passing through respondents location (number) | 2.470 |
| Travel time to CBD (minutes) | 30.68 |
| Travel time to a government office (minutes) | 15.96 |
| Travel time to shopping centers (minutes) | 15.40 |
| Travel time to grocery shop (minutes) | 7.60 |
| Travel time to park (minutes) | 17.88 |
| Travel time to Bus stop (minutes) | 14.14 |
| Built environment variables | |
| Government office and settlement area density per square-km | 0.0020 & 0.4512 |
| Industry and trade center area density per square-km | 0.0032 & 0.0046 |
| Road and railway per square-km | 34.46 & 4.493 |
| Social, Political and family participations within a family | |
| Number of days individual spend in social activities (Days) | 3.45 |
| Minutes per day individual spend time to do social activities (minutes) | 49.43 |
| Number of days individual spend in social activities with other family members (Days) | 6.33 |
| Minutes per day individual spend time to do social activities with other family members (minutes) | 96.56 |
| Activity Criteria | Mandatory | Maintenance | Leisure | |||
| In-Home | Out-of-Home | In-Home | Out-of-Home | In-Home | Out-of-Home | |
| Sleeping Personalcare Eating and drinking at home | Indoor working activities Outdoor working activities Indoor School activities Eating and drinking Dropping/Pick up children or others Out-of-home sleeping | Household activities Babysitting activities | Sales activities Shopping activities Out-of-home maintenance Waiting for public transport | Relaxing activities Social, family activities | Out-of-home social Outdoor school Organization/Volunteer/Political activities Sports activities Holiday Other out of home | |
| Variables | Moderate Activity (Job) | Strenuous Activity (Job) | Physical Health | Social Health | ||||
|---|---|---|---|---|---|---|---|---|
| Coeff | T-statt | Coeff | T-statt | Coeff | T-statt | Coeff | T-statt | |
| Constant | 117.5 | 15.47 | 76.82 | 11.29 | −2.01 | −3.76 | −0.79 | −3.76 |
| Socio-demographic characteristic | ||||||||
| Male | 0.073 | 7.288 | 0.053 | 5.243 | 0.066 | 5.336 | ||
| Worker | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| Non-worker | −0.025 | −2.29 | −0.04 | −3.84 | 0.057 | 3.751 | 0.129 | 8.342 |
| Student | 0.031 | 2.408 | −0.13 | −10.10 | 0.325 | 5.572 | 0.278 | 4.720 |
| Dependent Children (<15 years) | - | - | 0.095 | 8.571 | −0.12 | −3.15 | −0.10 | −2.66 |
| Age 15–22 (Years old) | 0.243 | 6.774 | 0.103 | 2.811 | 0.238 | 5.385 | −0.14 | −3.16 |
| Age 23–44 (Years old) | 0.319 | 7.579 | 0.198 | 4.605 | 0.113 | 2.253 | −0.37 | −7.40 |
| Age 45–55 (Years old) | 0.245 | 8.108 | 0.059 | 1.941 | 0.245 | 5.000 | −0.13 | −2.67 |
| Older than 55 years | 0.104 | 4.110 | - | - | - | - | −0.12 | −3.31 |
| Medium household income (3–6 IDR) | - | - | - | - | - | - | - | - |
| High household income (>6 million) | Ref | Ref | Ref | Ref | Ref | Ref | Ref | Ref |
| Household Characteristics | ||||||||
| Number of household members | −0.123 | −11.3 | −0.198 | −17.80 | 0.176 | 3.448 | 0.114 | 2.219 |
| Number of dependent children per household | - | - | 0.095 | 8.571 | - | - | −0.10 | −2.66 |
| Number of the motorized vehicle per household | - | - | - | - | - | - | - | - |
| Trip engagement and travel time | ||||||||
| Number of trips | 0.368 | 16.51 | 0.379 | 16.62 | −0.36 | −4.91 | −0.51 | −6.88 |
| Number of trip chains | −0.26 | −12.3 | −0.293 | −13.30 | 0.318 | 5.183 | 0.412 | 6.657 |
| Percentage of travel time using motorised mode | −0.055 | −0.05 | −0.07 | −4.43 | - | - | 0.064 | 2.610 |
| Percentage of travel time using Non-motorized mode | - | - | - | - | - | - | - | - |
| Percentage of travel time using public transport | −0.03 | −4.41 | −0.057 | −4.719 | 0.088 | 4.480 | 0.090 | 4.508 |
| Total travel time (minutes) | 0.049 | 4.082 | −0.05 | −2.45 | - | - | ||
| Time spend for different set of activities on weekdays (weekends) | ||||||||
| Time spend for in-home mandatory activities | - | - | - | - | −0.03 | −3.11 | - | - |
| Time spend for in-home maintenance activities | 0.029 | 2.688 | 0.032 | 2.843 | −0.04 | −3.47 | −0.03 | −2.62 |
| Time spend for in-home leisure activities | - | - | - | - | 0.107 | 4.498 | 0.064 | 2.652 |
| Time spend for out-of-home mandatory activities | - | - | - | - | - | - | ||
| Time spend for out-of -home maintenance activities | 0.042 | 4.648 | −0.028 | −3.047 | −0.09 | −9.50 | −0.14 | −14.9 |
| Time spend for out-of-home leisure activities | 0.045 | 4.874 | 0.018 | 1.916 | −0.08 | −8.50 | −0.10 | −10.1 |
| Perceived accessibility variables | ||||||||
| Number of public transport lanes passing respondents | −0.019 | −2.04 | - | - | −0.05 | −4.79 | −0.03 | −3.01 |
| Travel time to CBD | −0.163 | −13.3 | 0.032 | 2.563 | −0.17 | −3.37 | - | - |
| Travel time to government office | −0.11 | −9.61 | −0.133 | −11.14 | - | - | −0.10 | −3.40 |
| Travel time to shopping centres | 0.046 | 4.363 | −0.028 | −2.579 | 0.188 | 7.558 | 0.263 | 10.48 |
| Travel time to grocery shop | −0.181 | −15.8 | −0.025 | −2.203 | −0.19 | −5.36 | −0.12 | −3.41 |
| Travel time to park | 0.108 | 8.237 | 0.123 | 9.189 | −0.09 | −3.45 | - | - |
| Travel time to Bus stop | 0.084 | 7.438 | −0.103 | −8.943 | 0.503 | 8.385 | 0.367 | 6.069 |
| Built environment variables | ||||||||
| Density of government office/km2 within respondent | - | - | 0.190 | 6.321 | −0.48 | −6.21 | −0.29 | −3.74 |
| Density of settlement area/km2 within the respondent | −0.05 | −4.18 | −0.16 | −11.38 | 0.335 | 6.424 | 0.264 | 5.008 |
| Density of trade center/km2 within respondent location | −0.12 | −12.8 | −0.134 | −13.6 | 0.349 | 12.63 | 0.317 | 11.39 |
| Density of industrial area/km2 within the respondent | - | - | −0.16 | −5.37 | 0.471 | 6.847 | 0.258 | 3.720 |
| Km-length of road/km2 within the respondent location | −0.16 | −13.9 | - | - | −0.22 | −5.54 | −0.19 | −4.78 |
| Km-length of railway/km2 within respondent location | −0.07 | −8.24 | 0.024 | 2.522 | - | - | - | - |
| Social, Political and family participations within family | ||||||||
| How many days within a week individual spend in social activities | - | - | 0.086 | 9.053 | −0.15 | −4.74 | −0.09 | −2.87 |
| How long in a day individual spend time to do social activities | −0.06 | −7.19 | −0.05 | −5.44 | 0.074 | 3.705 | 0.047 | 2.356 |
| How many days in week individual spend in social activities with other families | −0.17 | −18.3 | - | - | −0.24 | −5.41 | −0.13 | −3.02 |
| How long in a day individual spend time to do social activities with other families | −0.08 | −8.49 | −0.03 | −3.45 | 0.075 | 5.097 | 0.036 | 2.425 |
| Endogenous of M-IPA | - | - | −0.52 | −4.69 | −0.23 | −2.09 | ||
| Endogenous of S-IPA | - | - | 0.889 | 5.180 | 0.703 | 4.061 | ||
| Error term | 7.590 | 6.804 | 0.229 | 0.231 | ||||
| F | 74.23 | 59.51 | 75.67 | 69.51 | ||||
| R-Square | 0.214 | 0.209 | 0.217 | 0.203 | ||||
| SD | 39 | 39 | 39 | 39 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ali, M.; Dharmowijoyo, D.B.E.; de Azevedo, A.R.G.; Fediuk, R.; Ahmad, H.; Salah, B. Time-Use and Spatio-Temporal Variables Influence on Physical Activity Intensity, Physical and Social Health of Travelers. Sustainability 2021, 13, 12226. https://doi.org/10.3390/su132112226
Ali M, Dharmowijoyo DBE, de Azevedo ARG, Fediuk R, Ahmad H, Salah B. Time-Use and Spatio-Temporal Variables Influence on Physical Activity Intensity, Physical and Social Health of Travelers. Sustainability. 2021; 13(21):12226. https://doi.org/10.3390/su132112226
Chicago/Turabian StyleAli, Mujahid, Dimas Bayu Endrayana Dharmowijoyo, Afonso R. G. de Azevedo, Roman Fediuk, Habil Ahmad, and Bashir Salah. 2021. "Time-Use and Spatio-Temporal Variables Influence on Physical Activity Intensity, Physical and Social Health of Travelers" Sustainability 13, no. 21: 12226. https://doi.org/10.3390/su132112226
APA StyleAli, M., Dharmowijoyo, D. B. E., de Azevedo, A. R. G., Fediuk, R., Ahmad, H., & Salah, B. (2021). Time-Use and Spatio-Temporal Variables Influence on Physical Activity Intensity, Physical and Social Health of Travelers. Sustainability, 13(21), 12226. https://doi.org/10.3390/su132112226