Abstract
Climate change-related natural disasters, including wildfires and extreme weather events, such as intense storms, floods, and heatwaves, are increasing in frequency and intensity. These events are already profoundly affecting human health in the United States and globally, challenging the ability of communities to prepare, respond, and recover. The purpose of this research was to examine the peer-reviewed literature on community resilience initiatives in one of the most densely populated and economically important regions, the Northeastern United States, and to identify evidence-based interventions and metrics that had been field-tested and evaluated. This paper addresses two critical gaps in the literature: (1) what strategies or interventions have been implemented to build or enhance community resilience against climate change-related natural disasters; and (2) what metrics were used to measure community resilience as an outcome of those strategies or interventions? This review provides a succinct list of effective interventions with specific health outcomes. Community or state-level health officials can use the results to prioritize public health interventions. This review used existing database search tools to discover 205 studies related to community resilience and health outcomes. Methods set criteria to assess if interventions were able to measure and change levels of community resilience to the health impacts associated with a changing climate. Criteria included: (a) alignment with the United States’ National Preparedness Goal for reducing risks to human health and for recovering quickly from disasters; (b) derived from publicly available data sources; (c) developed for use by communities at a local scale; and (d) accessible to modestly resourced municipalities and county health agencies. Five (5) peer-reviewed, evidence-based studies met all of the selection criteria. Three of these articles described intervention frameworks and two reported on the use of standardized tools. Health-related outcomes included mental health impacts (PTSD/depression), mental stress, emergency preparedness knowledge, social capital skills, and emergency planning skills. The paper recommends the COAST project, COPEWELL Rubric for self-assessment, and Ready CDC intervention as examples of strategies that could be adapted by any community engaged in building community resilience.
1. Introduction
Climate change-related natural disasters, including wildfires and extreme weather events, such as intense storms, floods, and heatwaves, are increasing in frequency and intensity in the Northeastern United States and globally [1,2,3]. These events challenge the ability of communities to prepare, respond, and recover, resulting in impacts to both human health and community resilience [1,2]. Natural disasters and extreme weather events affect the public’s physical or mental health through injury and other trauma, vector-borne diseases, heat-related illness, and illness resulting from reduced air and water quality [4,5]. Natural disasters impact the overall functioning of a community by overwhelming available healthcare and disaster response resources [6].
Interventions designed to reduce the health impacts of natural disasters may focus on the individual, family, or community to build and enhance community resilience [7,8]. Here, we define community as a group of individuals who are linked together by shared geographical space, situations, or interests, and collectively engage in action [9,10].
The purpose of this research was to examine the existing peer-reviewed literature on community resilience initiatives and to identify which interventions and metrics had been field-tested and evaluated. The Northeastern United States contain some of the largest metropolitan areas, including New York City, and the three most rural states (Maine, Vermont, and West Virginia), where more than 50% of the populations live in rural areas [11]. The Northeast also exceeds all other regions of the contiguous United States in precipitation intensity, and additional precipitation increases are expected [12] as the climate becomes warmer and wetter [13]. As a result, the projected changes in the climate of the Northeast are expected to increase the exposure, susceptibility, and vulnerability of both urban and rural communities to flooding [14]. We expected that by focusing on this region, specifically, we would find generalizable evidence-based interventions and metrics for strengthening community resilience. We also were interested in how the community resilience-building process aligns with the United States’ National Preparedness Goal for reducing risks to human health and for recovering quickly from disasters, such as flooding. In this article, we review various definitions of community resilience. We explore how community resilience can be built or enhanced and review the metrics that have been used to measure the extent to which the interventions strengthened resilience. We then discuss the parameters and results of our review that addressed two critical gaps in the literature: (1) what strategies or interventions have been implemented to build or enhance community resilience against climate change-related natural disasters, and (2) what metrics were used to measure community resilience as an outcome of those strategies or interventions? We conclude with recommendations for public health practitioners engaged in building community resilience.
1.1. National Preparedness Goal and Standards for Community Resilience
Community resilience at the local level is situated within and influenced by national-level policy and actions. This national context is important for understanding the focus of this paper on local community resilience action. In 2003, President George W. Bush issued Homeland Security Presidential Directive-8: National Preparedness, which directed the Secretary of the Department of Homeland Security (DHS) to develop a national all-hazards preparedness goal for the nation to prevent, respond to, and recover from emergencies in the United States [15]. The directive was replaced in 2011 by Presidential Policy Directive/PPD-8: National Preparedness which directed the Secretary of DHS to develop a national preparedness goal in which all U.S. citizens and organizations shared responsibility [16]. This new directive downscaled the focus on local and individual preparedness leadership and action, making community-level resilience initiatives even more important.
The National Preparedness Goal (NPG) is to create “a secure and resilient nation with the capabilities required across the whole community to prevent, protect against, mitigate, respond to, and recover from the threats and hazards that pose the greatest risk” [17]. The NPG was conceptualized as five interconnected missions to: (1) prevent terrorism; (2) protect against hazards; (3) mitigate loss of life and property; (4) respond quickly to human needs after a disaster; and (5) recover in a timely and productive manner [18]. Mitigation included hazard identification, risk assessment, vulnerability reduction, public warning systems, and community resilience (Figure 1). The U.S. Centers for Disease Control and Prevention (CDC) created national standards for the public health components of the NPG; these standards were designed to improve public health emergency preparedness and response capabilities at both the state and local levels [19]. The national standards consisted of six domains, including incident and information management, countermeasures and mitigation, surge management, biosurveillance, and community resilience [19]. The CDC standards divided community resilience into two tiers: (1) community preparedness; and (2) community recovery (Figure 1).
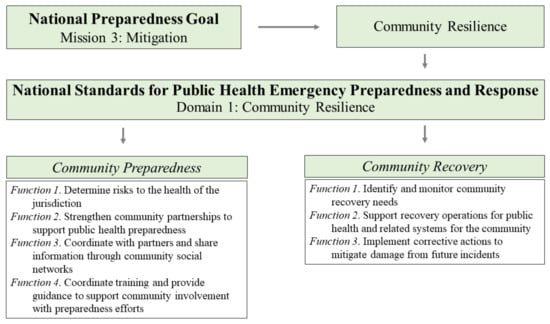
Figure 1.
Community resilience, although affected by all five missions, is named explicitly within Mission 3 of the National Preparedness Goal [14], and Domain 1 of the National Standards for Public Health Emergency Preparedness and Response [19].
The national preparedness standards were revised in 2018. The former definition of at-risk populations—“children, those with disabilities and others who have access and functional needs, and populations with limited English proficiency” [17]—became individuals who have “access and functional needs that may be disproportionately impacted by an incident or event” [19]. In addition, program evaluation measures were no longer included. The revised standards encouraged state and local public health agencies to devise their own strategies to assess the impact of their programs on increasing public health preparedness and response through enhanced community resilience. This state and local level assessment imperative is a primary focus of—and motivation for—this review.
1.2. What Is Community Resilience and Why Is It Important?
There is no commonly accepted working definition of community resilience [20,21]. Community resilience is defined differently by organizations engaged in: (1) disaster risk reduction; (2) public health; and (3) national health security [20,22]. Definitions typically focus on the strengths of a community and how those strengths can be used to improve and sustain health [23,24]. We present definitions of community resilience from these three perspectives as they emphasize three important community resilience outcomes: maintaining basic functions; using community assets; and becoming self-reliant.
1.2.1. Community Resilience and Disaster Risk Reduction
In the field of disaster risk reduction, community resilience is defined as “the ability of a system, community or society exposed to hazards to resist, absorb, accommodate to and recover from the effects of a hazard in a timely and efficient manner, including through the preservation and restoration of its essential basic structures and functions” [25]. From the disaster risk reduction perspective, a resilient community is one that has the ability to: (1) prepare for natural threats; (2) reduce vulnerability by decreasing disaster risks; (3) absorb and recover from disasters; (4) adapt to changing conditions; and (5) sustain the health of the community [22,26,27].
1.2.2. Community Resilience and Public Health
Public health defines community health resilience as “the ability of a community to use its assets to strengthen public health and healthcare systems and to improve the community’s physical, behavioral, and social health to withstand, adapt to, and recover from adversity.” [28]. Community resilience is measured by “the ability of people, businesses, governments, nonprofit groups, and faith-based organizations to work together to create systems that can withstand, adapt to, and recover from a public health emergency” [29]. The CDC, through its Public Health 3.0 initiative, has taken a community-level approach to public health that engages multiple community partners from both public and private sectors. The initiative is based on the premise that local communities have the ability to improve their own public health and wellbeing, equity, and resilience [30].
1.2.3. Community Resilience and National Health Security
At the level of national health security, community resilience is defined as a set of skills and behaviors already in place before a disaster, that can be strengthened through education and training, to enable communities to become more self-reliant in response to public health emergencies when external assistance may be delayed or limited [31]. The national health security strategy for the United States has been attained when “the Nation and its people are prepared for, protected from, and resilient in the face of health threats or incidents with potentially negative health consequences” [31].
Each of the three definitions are similar in that they address the means by which a community can respond to and recover from a disaster. However, definitions differ in terms of perspective. Disaster risk reduction aims to reduce risks and maintain basic structures and functions within a community. A disaster risk reduction perspective is helpful for city planners focused on infrastructure issues. The public health perspective utilizes community assets to improve physical and mental health at the population level (rather than individual), and is the focus of interest in this review of the literature. National health security defines the essence of community resilience—to prepare communities to be self-sufficient during disaster events while waiting for help to arrive.
Based on these definitions, community resilience is both an outcome and a process [22,23,32,33]. As an outcome, community resilience is an attribute that is attained through strategies or interventions designed to: (1) enhance community preparedness for public health incidents; or (2) identify critical assets within the public health, human services, environmental health, and emergency management sectors that are needed for community recovery [19,34]. A resilient community has the ability to prevent, respond or adapt to, and recover from incidents that impact human health in a timely manner and at a level of functioning that supports equity and well-being [35].
As an ongoing and dynamic process, community resilience involves a focus on building social connectedness and improving the everyday health and wellness of a community over time [14,28,36]. These definitions of community resilience provide a foundation for understanding how to strengthen and measure resilience. We explore those questions in the following sections.
1.3. How Is Community Resilience Built or Enhanced?
Interventions to improve community resilience are often designed differently than actions that enhance individual resilience (Figure 2). Community resilience focuses on networking community members and organizations within and beyond the community to support the health and wellness needs of the whole community, including at-risk populations. Individual resilience interventions address the wellness needs of an individual [36].
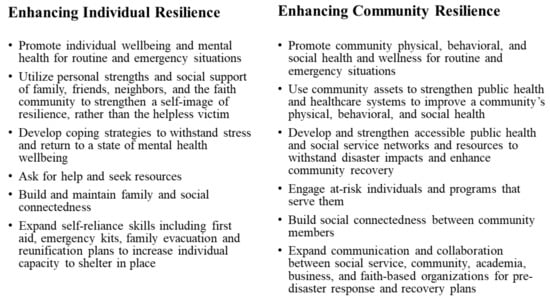
Figure 2.
A comparison of individual and community resilience characteristics [28,37,38].
Community Resilience and Vulnerable Populations
Identifying vulnerable populations is central to the goal of strengthening the overall resilience of a community. Populations are vulnerable to climate-related hazards when they: (1) are exposed to a perceived hazard or threat; (2) are sensitive to its physical or health impacts; and (3) lack the capacity to withstand, resist, or adapt [18,39,40]. Vulnerable populations lack adaptive capacity when they live in isolation from the community as a whole. Social isolation has been correlated with post-disaster mortality; populations that are socially isolated from support systems, participation in community organizations, or access to municipal and governmental institutions in daily life are more likely to experience health impacts or death post-disaster [40]. Vulnerable populations may include: older adults, children, communities of color, lower-income neighborhoods, individuals or families with physical or medical challenges, including chronic diseases and addictions; homeless, tourist, or community-living populations; people with limited English literacy or education, and people with no access to transportation, healthcare, technology, or citizen status [18,40].
The vulnerability of a population to climate change-related natural hazards is dependent upon both hazard type and location [41]. Climate projections indicate that vulnerable populations in the Northeast will experience increased extreme heat and precipitation events. Local planners are encouraged to include heat resilience strategies in their climate and health adaptation plans, particularly in rural areas that are more physically isolated, and that have higher poverty rates and natural resource-dependent economies [11]. At the neighborhood scale, a municipality that is vulnerable to flooding and extreme precipitation events may have a hilltop residential area that is less vulnerable than the surrounding community. The hilltop community may be more resilient due to its lower physical exposure, greater access to financial resources and generators that reduce its sensitivity to power losses, and stronger connections with social networks or health resources that increase its adaptive capacity [42]. In contrast, a nearby low-lying area may be more vulnerable to flooding and erosion. Planners can use a number of vulnerability assessment tools to identify where populations are at greatest risk for health impacts based on exposure, sensitivity, and adaptive capacity [39].
One vulnerability assessment tool is the CDC’s social vulnerability index (SVI), which uses easily available U.S. census data, such as income, special needs, age, inability to understand English, and access to housing and transportation, to assist public health officials in determining county sections that may be most vulnerable to disasters [43]. The New Hampshire Department of Health and Human Services (DHHS) adapted the CDC’s SVI to identify towns with populations at increased risk for environmental or public health hazards [44,45] (Figure 3).
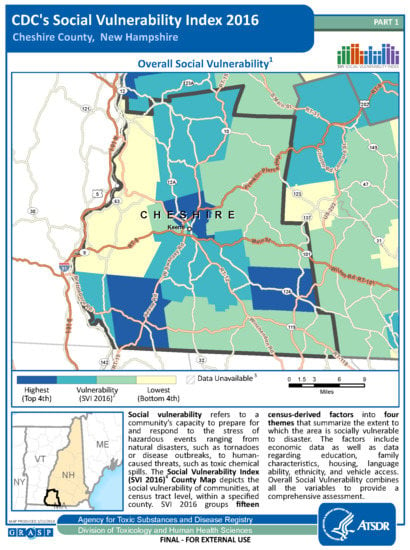
Figure 3.
An example of the CDC’s social vulnerability index in southwest NH. Regions in the darkest blue are most vulnerable to disasters. From: ATSDR [43].
Researchers used the NH SVI to determine the effects of climate change on New Hampshire’s coastal wetlands, such as inundation and flooding, and in turn, their impacts on human health [46].
Community resilience is built or enhanced by engaging the community, including vulnerable populations, in the process of learning to identify and mitigate the risks associated with climate-related natural disasters. Tools and frameworks are available to identify risks, vulnerable populations, and the steps needed to reach resilience as an outcome. Despite the availability of frameworks for guiding community resilience initiatives, few have been incorporated into interventions and evaluated [32]. The question we pose is, how do we know the methods used to build or enhance community resilience are effective and can be applied in other contexts? To answer that question, we must also ask: how do we measure community resilience? That is the question we address next.
1.4. How Is Community Resilience Measured?
Tools used to measure community resilience may assess community resilience as a whole, or focus on one indicator, such as community partnerships. These tools also range from a generalized multiple-hazard application to a specific hazard or community, such as flood zones along the coast [42]. Tools use both indicators and metrics to measure resilience. Metrics are the units of measurement or comparison, such as communication, transportation, and utilities; these metrics vary with the scope and scale of an intervention [47]. We present examples of metrics used for community disaster resilience, with a focus on public health, in Table 1.

Table 1.
Sample Metrics to Measure Community Resilience to Disasters.
Metrics may identify additional needs in a community, as with a vulnerability index, track the process of an intervention, as with a focus group during the intervention, or assess the outcomes of the intervention, as with a post-intervention survey [47]. Without metrics, how can we know if an intervention was successful at building community resilience?
A review of 36 community resilience assessment tools revealed a variety of metrics to measure preparation, recovery, and adaptation, including: emergency planning and services; knowledge and access to information; health and well-being; social connectedness; and infrastructure [10]. Data were collected in the form of interviews and surveys, and based on analytical tools, including scorecards and indices. A total of 6 percent of the 36 tools used primary data only, which included interviews and surveys from key informants; 28% of the tools relied on secondary data only, including U.S. census data, historical records, and statistical data from municipal and non-profit organizations; and 44% of the assessment tools incorporated both primary and secondary data [10]. Of the 36 tools reviewed, 24 were tested with one or more communities.
Assessment tools, by design, have either a top-down or bottom-up approach. Tools with a generalized, top-down approach are developed by external organizations, separate from the community being measured, and may be adaptable to a variety of hazards or locations. Tools with a localized, bottom-up approach are developed through active engagement with the community and adapted to the specific hazards for that community [49]. The downside to a generalized assessment tool is that it may not capture the characteristics of a community that reflect its resilience or vulnerability. The downside to a localized assessment tool is that it may not easily be used to compare one community with another.
Formative and Summative Metrics
Metrics can be categorized into two types: formative and summative. Formative metrics provide feedback during an intervention or process of designing an intervention, whereas summative metrics assess the results of the intervention [10,50]. For example, a formative metric, such as vulnerability, is measured with the SVI for a focus group discussion on how to increase the resilience or adaptive capacity of a particular population during the intervention. In contrast, a summative metric, such as a post-intervention survey, assesses the outcomes of the intervention, with a focus on improving the intervention for future use.
To answer our question of how community resilience is measured, we conducted a review of the literature. Our objectives were to understand:
- What strategies or interventions have been implemented to build or enhance community resilience and how resilience was strengthened;
- What metrics were used to measure community resilience as an outcome of those strategies or interventions; and
- Which interventions could be applied at a local level, and with modest resources, to achieve the U.S. National Preparedness Goal?
We address these questions, based on the results of our literature review, in the following section. We conclude with recommendations of evidence-based community resilience interventions, tools, and metrics that can be applied at the local level to meet the CDC standards of the National Preparedness Goal.
2. Methods
We conducted a review of the published literature to answer our questions about community resilience interventions in the Northeastern United States and the metrics used to measure their success.
Selection Criteria
We used a multiple-step process for this literature review. We began by exploring the peer-reviewed literature on community resilience interventions and metrics available through Academic Search Complete, Cochrane Library, PubMed, and Web of Science databases. We searched for studies that: (1) evaluated interventions designed to increase community resilience and reduce public health impacts of climate change and associated natural disasters; and (2) employed metrics to measure community resilience, either as a baseline assessment of the community’s resilience and adaptive capacity, or as a result of the intervention. We limited our search to studies in English conducted in the Northeastern and Mid-Atlantic United States. There were no restrictions on the year of publication.
Keyword search phrases included: (community resilience) AND (evidence-based interventions OR measures OR metrics OR assessment) AND (severe or extreme weather OR natural hazards or disasters) AND (community recovery OR adaptation strategies OR hazard mitigation) (Table 2). “Public health impacts” generated too few studies so the term was removed from the search.
Table 2.
Initial keyword search results for community resilience literature (5 October 20).
The search produced 650 publications. Using the selection criteria described previously, we reviewed the title and abstract of each publication. We excluded duplicate articles, conference papers or books, articles about research outside the Northeastern United States, non-English articles, and publications unrelated to human health and community resilience. The remaining 205 publications were selected for this review (Table 3).
Table 3.
Results of Database Search for Community Resilience Interventions and Metrics.
Next, we read each article that met the above criteria and analyzed it for information pertaining to the hazard, the intervention, and the metrics used to measure resilience. Each article was analyzed for the following information:
- (1)
- Type of climate and/or health impact;
- (2)
- Target population or community and location;
- (3)
- The method used (intervention, tool development or trial, research study);
- (4)
- The formative metrics used to measure community resilience;
- (5)
- The summative metrics, or health-related outcomes;
- (6)
- Data sources;
- (7)
- If the data was publicly available (local sources or available online);
- (8)
- Which of the CDC’s seven national standards were met;
- (9)
- Author(s) and year.
3. Results
The literature review yielded 24 articles that demonstrated a range of interventions and metrics related to community resilience in the Northeast and Mid-Atlantic states (see Table A1). Three articles described health and community resilience interventions; eight reported on the development and piloting of community resilience tools; and thirteen discussed studies of public health and community resilience. The articles explored a variety of climate and health impacts; however, 50% of the articles examined hurricane resilience, specifically to Superstorm Sandy. Five articles addressed the impacts of winter and coastal storms, floods, drought, and heatwaves.
3.1. Data Sources for All Articles Reviewed
In the 24 articles we fully reviewed, data used to measure resilience were collected using qualitative and quantitative methods in a variety of formats, and from a range of publicly available national, county, and municipal sources (see Figure 4). The most commonly used data sources were project participants and online U.S. census data. Half of the 24 projects used participant surveys and interviews to gather data on population demographics and community resilience indicators. Eleven studies accessed online U.S. census data sources for demographics and population distribution. Three projects accessed county-level U.S. census data and shapefiles for creating maps.
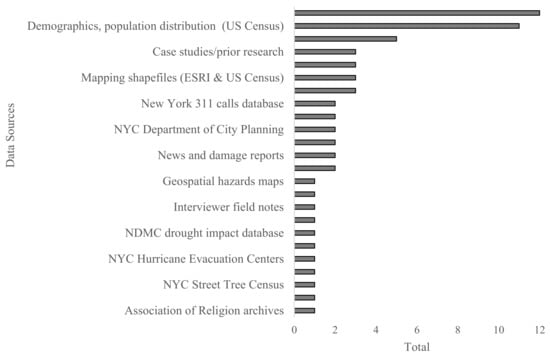
Figure 4.
Data sources for interventions, community resilience tools, and research studies.
Each article described the use of an assessment tool; however, because the focus of this paper is on applied interventions and tools with metrics to measure community resilience, we eliminated 19 research articles from this review because the tools and interventions described were conceptual and were not applied.
3.2. Articles Meeting the Selection Criteria
Five articles met all of our selection criteria. Three articles described intervention frameworks and two reported on tools: (1) COAST Project mental health intervention; (2) Resilience and Coping for the Healthcare Community (RCHC) mental health intervention; (3) Ready CDC community resilience intervention; (4) COPEWELL rubric social capital and community engagement assessment tool; and (5) Garden State community resilience tool. All five interventions or tools were implemented and evaluated (Table 4).
Table 4.
Five evaluated community resilience interventions and metrics with associated climate and health impacts in the Northeast and Mid-Atlantic states.
3.2.1. COAST Mental Health Intervention
The COAST mental health intervention enhanced community resilience for individuals and groups in two separate New York communities impacted by Superstorm Sandy. The intervention used a systemic approach to increase the mental health of youth affected by the storm, recognizing that strong parental support can reduce post-disaster stress in youth [51]. COAST addressed the mental health needs of vulnerable youth, parents, and teachers in two school communities through: (a) increased local partnerships with a mental health agency and b) the incorporation of resilience messages within the school culture [51]. Education, support, and services were provided to build student resilience, educate and support parents and teachers, and address the needs of at-risk youth. More than 6500 preK-12 students (90% of population) in 10 school buildings from both communities participated in the Tier 1 intervention which focused on building student resilience by increasing emotional, social, and cognitive assets to decrease at-risk behaviors. The Tier 3 intervention, which provided treatment for PTSD, identified 17% of students in the Long Beach community as eligible, based on 1995 screening surveys. Approximately 40% of eligible students (<100) participated in the group-based cognitive behavioral intervention for trauma in schools (CBITS) and 35 students received individual trauma-focused cognitive behavioral therapy (TF-CBT). Metrics that assessed student engagement and increased capacity to cope with stress and trauma included: (a) student, parent, and teacher feedback; (b) student volunteerism in art and media projects; and (c) participation in discussion groups and school organizations during the intervention. Tier 2 workshops for parents and faculty meetings for teachers were designed to educate and support caregivers in identifying trauma symptoms, managing stress, modelling positive coping skills, and preparing for disasters. The majority of parents and teachers indicated in a satisfaction survey that the psychological first aid and individual outreach that accompanied the Tier 2 program was extremely helpful.
Tools used to assess post-traumatic stress disorder (PTSD) and depression included a modified version of the National Child Traumatic Stress Network’s Hurricane Assessment Tool [56] that was used in New Orleans after Hurricane Katrina; the Child PTSD Symptom Scale (CPSS) [57]; the Strengths and Difficulties Questionnaire (SDQ) [58], the Children’s Depression Inventory 2 (CDI-2) [59] or Beck’s Depression Inventory 2 (BDI-II) for adolescents [60], and the CRAFFT [61] substance abuse screening tool for adolescents [51]. A comparison of pre- and post-intervention PTSD and depression assessment scores revealed that PTSD was reduced more than depression as a result of the intervention. Due to the intervention’s success at reducing the mental health impacts of Superstorm Sandy and increasing individual and school resilience, the COAST model was selected for inclusion in the socio-emotional literacy curriculum for the Long Beach school district.
3.2.2. Resilience and Coping for the Healthcare Community Intervention
The Resilience and Coping for the Healthcare Community (RCHC) mental health intervention [52] focused on building resilience among its New York and New Jersey participants. The 69 participants included healthcare, social service, and disaster response providers that operated in the dual roles of survivor and healthcare responder during and after Hurricane Sandy. The RCHC intervention increased local partnerships with three community health centers, two social service agencies, and one disaster response organization through staff cohesion and team building. Psychoeducational strategies were employed to help participants understand stress responses and to develop coping strategies, followed by a solution-focused approach to envision change and build capacity [52]. Participants completed surveys before and after the psychoeducational intervention, with one additional follow-up three weeks later to report on their experiences responding to or surviving Superstorm Sandy. Semi-structured interviews were conducted with 10 participants from five of the six intervention sites. Tools used to measure mental health resilience included the Professional Quality of Life Measure (ProQOL 5) [62] for professionals helping others through trauma, the Perceived Stress Scale [63], a self-reporting stress checklist [64], and the Coping Self-Efficacy Scale [65]. Metrics included self-reported levels of stress, fatigue, burnout, coping strategies, satisfaction, and knowledge. T-tests and Chi square analyses indicated that perceived knowledge had increased, acute stress had decreased, and that there were no significant differences between the 45 participants who completed the 3-week follow-up and the 24 who did not.
3.2.3. Ready CDC Community Resilience Intervention
The Ready CDC intervention increased community resilience among 208 CDC staff participants in Morgantown, WV, Atlanta, GA, and Fort Collins, CO, through emergency preparedness education and activities using a behavioral theory-based approach designed to support preparedness actions [53]. Metrics included a pre- and post-assessment of knowledge, beliefs, self-efficacy, and stage of household preparedness using the Transtheoretical Model (TTM) of behavior change [66,67], (Figure 5). The study used a TTM-based survey instrument to measure changes in emergency preparedness behaviors and attitudes towards community resilience.
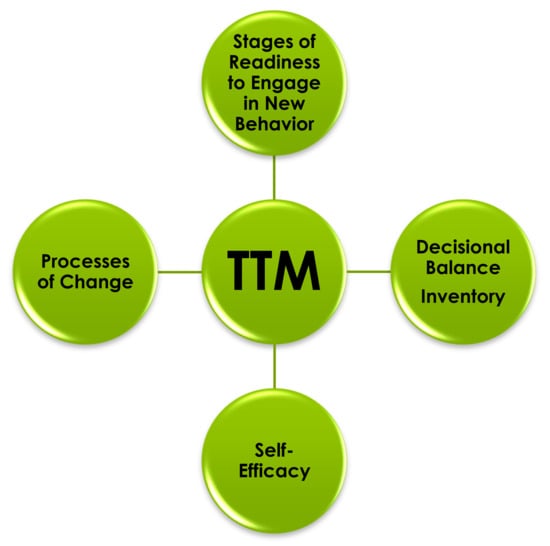
Figure 5.
Core constructs of the TTM (adapted from Abrash Walton, 2018) [68].
The TTM is an evidence-based psychological approach to understanding and facilitating behavior change [68]. The TTM has four major constructs: (a) stages of readiness to engage in a new behavior; (b) decisional balance inventory; (c) self-efficacy; and (d) processes of change (Figure 5). The stages of readiness to engage in a new behavior construct is based on the theory that there are five recognizable stages associated with any given behavior change.
These stages are:
- Pre-contemplation—not ready to engage in the new behavior (e.g., not aware, in denial);
- Contemplation—considering engaging in the new behavior;
- Preparation—actively preparing to engage in the new behavior;
- Action—engaging in the new behavior;
- Maintenance—continuing the new behavior for at least six months.
Progress through these stages is not necessarily linear or steady. For example, a person might spiral through contemplation, preparation, and action more than once. The decisional balance construct is based on the understanding that decision-making requires the consideration of potential positive and negative consequences. The self-efficacy construct concerns an individual’s confidence in engaging in the new behavior. Self-efficacy can influence motivation and persistence in engaging in the behavior change. The fourth TTM construct consists of the ten processes that can support behavior change. Specific processes tend to support effective movement through the stages when provided at a particular stage.
The five stages of change were measured before the intervention and three months after. A Wilcoxon analysis indicated that 90 participants (44%) advanced one stage or remained at the maintenance stage for assembling an emergency kit, while 94 participants (45%) advanced one stage or remained at the maintenance stage for creating a written emergency plan. Behavior metrics used in the Ready CDC intervention included participants signing up for emergency notifications and encouraging others to prepare for emergencies [53].
3.2.4. COPEWELL Rubric Social Capital and Community Engagement Assessment Tool
The pilot of the COPEWELL rubric’s social capital and cohesion tool increased local partnerships, enhanced social cohesion, and increased risk communication and knowledge using a bottom-up participatory approach to community self-assessment [54]. The project combined building community resilience as a process with obtaining community resilience as an outcome to advance our understanding of the features desired in a self-assessment toolkit [54]. During Phase 1, the rubric was developed by public health practitioners and social science researchers with expertise in community resilience, public health policy and emergency preparedness. Prior to launching a pilot trial, the rubric was reviewed by 13 stakeholders from local, state, and federal sectors and then used in a mock exercise with 30 public health preparedness professionals at the 2018 Annual Public Health Preparedness Summit in Atlanta, GA [54]. The rubric was then piloted with stakeholders representing municipal, county, and utility agencies. In its final phase of the pilot intervention, the social capital and cohesion self-assessment tool was implemented in Coatesville, PA, with 18 community members representing community-based organizations and local citizens.
Metrics included social support within the community, connections to the neighborhood and larger municipality, active community organizations, and opportunities for individuals and community organizations to engage in emergency preparedness planning, response, or recovery. Community engagement and buy-in were noted at the end of the tool’s evaluation when the county partners committed to implementing additional domains from the rubric. Additional domains of the COPEWELL rubric are now available for: population vulnerability, inequality and deprivation; community functioning; emergency management; and prevention/mitigation.
3.2.5. Garden State Community Resilience Tool
The Garden State community resilience tool focused on community strengths and weaknesses in relation to disaster preparedness and resilience. The Garden State assessment tool was piloted in Secaucus, a densely populated New Jersey community affected by Superstorm Sandy. The pilot intervention used planning and coordination strategies from an emergency management framework to identify the response and recovery needs of vulnerable populations and to develop emergency preparedness plans for future risk mitigation [55]. The assessment was implemented in two phases during the course of one year. In the first phase, the community’s municipal and emergency operations were reviewed, including existing plans and procedures. City officials contributed their expertise via interviews. The second phase focused on the identification of community threats, hazards, and risks using historical information and mapping of floodplains. An analysis of the populations and the community’s assets was also conducted.
Metrics included county and state demographics for comparison, including at-risk populations and population density; and county emergency planning policies, including pre-event planning, municipal operations, recovery, and mitigation. The authors did not indicate if the implementation of the tool increased partnerships for emergency preparedness initiatives. The model has since been expanded to assist other New Jersey communities.
3.3. Evidence-Based Metrics for the Five Selected Articles
The formative and summative metrics used to measure community resilience varied with each intervention or tool. Preparedness and recovery interventions focused on formative metrics such as knowledge, coping skills, and mental health, while the resilience tools measured social connectedness and partnerships, pre-event planning, and community functioning. The summative metrics indicated an increase in community resilience and decreases in mental health impacts associated with Superstorm Sandy. All three mental health and community resilience interventions were successful in increasing knowledge related to emergency preparedness and risk reduction.
Each project met at least four of the CDC’s seven national standards for community resilience (Figure 6); the COAST intervention was the only project that met all seven.
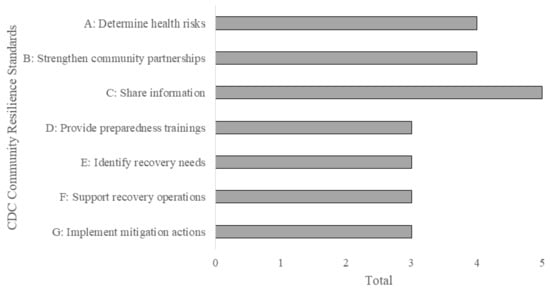
Figure 6.
Number of projects meeting the CDC national standards for community resilience.
A list of the metrics discussed in all 24 articles is available from the authors as a supplement to this article. A list of toolkits is available in Table A2.
4. Discussion
In our review of the initial 205 articles on community resilience interventions and metrics for the Northeast and the Mid-Atlantic states, we found 5 articles (2.4%) that discussed interventions which had been implemented and evaluated. Our key finding, which supported previous research, was that, despite a plethora of articles on theoretical frameworks and community resilience tools, few exist that demonstrate an evaluation of the tools or interventions to measure and build community resilience [23,32,54,69].
We located only five articles from the Northeast region that demonstrated an evaluation of the tools or interventions that measure and build community resilience [51,52,53,54,55]. The five studies used mental health, behavior change, emergency preparedness, and resilience frameworks to engage communities, build capacity, and enhance resilience; however, more evidence-base studies are needed to aid public health practitioners in choosing frameworks best-suited to specific community and climate scenarios. There is a specific need for an evaluation of existing frameworks that study the resilience and post-disaster recovery of communities affected by climate-related hazards such as hurricanes and flooding [70].
4.1. Evidence-Based Metrics for Community Resilience: Similarities and Differences
An intervention must be evaluated to know if it succeeded in enhancing community resilience [36]. Here, we compare the metrics used to measure community resilience in the five selected interventions and tools: (1) COAST Project mental health intervention; (2) RCHC mental health intervention; (3) Ready CDC community resilience intervention; (4) Garden State community resilience tool; and (5) COPEWELL rubric community engagement assessment tool.
The five selected articles (Table 4) used relatively simple, often low-cost data collection methods, including participant knowledge, pre and post surveys, semi-structured interviews, and focus groups. The metrics reflected aspects of a resilience domain that could be easily measured, such as the stage of house-hold preparedness, or the number of community organizations engaged in emergency preparedness initiatives.
In contrast, some interventions, tools, and research (Table A1) used more complicated, time-consuming, or costly methods to obtain data, making their use less accessible to local health practitioners and emergency planners. For example, data imported into the Resilience to Emergencies and Disasters Index (REDI) tool to assess neighborhood resilience after Superstorm Sandy [71] included access to the 311-call system for New York City, information on the public transportation systems, hurricane evacuation centers, and access to the census of street trees in the city. During a pilot of the COPEWELL model for hurricane resilience across the United States [72], county-level data were obtained on transportation infrastructure, physical distance to coastlines, socio-economic information, and social organizations. The study on coastal storm vulnerability for U.S. counties along the Atlantic coast [73] required population distribution data, natural habitat information, historical sea level trends, and coastal topology and elevation data to develop a coastal risk index. Despite most of the data’s availability online, acquiring and processing such data may be time-prohibitive for local planners and public health agencies. In addition, the development of the Recovery Indicators Tool [48] highlighted the reality that not all data may be available for all metrics, increasing the uncertainty of a tool’s effectiveness in measuring or enhancing community resilience.
Data that are not relevant, including climate change projections, or accessible to local planners in a way that reflects their ability to collect, interpret, or use them, are data that may be misused or not used at all [74]. Relying upon participant-based and publicly available U.S. census data may be the most affordable option for smaller communities with limited financial and personnel resources.
4.2. Strengths and Weaknesses of Community Resilience Interventions and Tools
Study authors and participants critiqued interventions and tools in this review. We discuss those critiques here with the intention of informing development of future interventions. Participants who contributed to the development of the Recovery Indicators Tool, which was created to measure disaster recovery, suggested that the tool was flexible enough to be used for a pre-disaster assessment, as well as an indicator of post-disaster recovery [48]. We believe the Ready CDC intervention may also be adapted for pre and post-disaster assessment, as well as individual and community resilience. Ready CDC combined emergency preparedness education with behavior change theory in a model that could easily be adapted for use by adults in a school, workplace, or community setting.
Authors offered suggestions on what to do with the knowledge gained from the implementation or evaluation of the intervention or tool. For example, community resilience assessment tools would be more beneficial to planners and public health officials if they went beyond a current assessment of the community; additional information could include recommendations for actions that are customized to a community’s needs [42]. This feedback was similar to the request made by participants of the COPEWELL rubric who wanted a tool that could be adapted for municipalities with different resource levels [54].
Intervention and Tool Development and Deployment Costs and Structures. We reached out to the authors of seven articles in this review who used surveys, focus groups, and participant interviews for data collection and asked about the costs for the interventions, the hours and staffing structure involved, and any funding they received.
One author reported that the costs for piloting a disaster recovery assessment tool were $23,000 for supervised graduate student stipends over nine months totaling approximately 280 h. Research included a literature review, two case studies, two focus groups, and 21 interviews with experts from academia, and public and private practice. Multiple research papers resulted from the project.
The development of a disaster preparedness assessment tool for local health departments incurred nearly $250,000 for each of the first two years for research and development and $50,000 during the third year to develop the toolkit. The piloting of the tool took four months and included a survey of 274 disaster preparedness coordinators from local health departments across the country.
A post-disaster mental health intervention that involved two school districts in ten locations took two years to complete. Activities addressed trauma and coping skills and included art therapy, workshops, service learning, and therapy. Full-time staff included a licensed social worker as program manager and a psychology fellow. Part-time staff included two social workers, a psychologist, a psychiatrist, a nurse practitioner, and two psychology students. The overall program budget was $1.2 million. Financial support was received from Americares, the CDC, and New York social services school grants.
4.3. Community Resilience Interventions and Tools for Severe Weather Events
We believe that both of the hurricane-related interventions that focused on mental health resilience could be applied to other severe weather events, such as flooding or extreme winter storms. The COAST model in particular, because of its institution-based approach, could be adapted for use in nursing homes, prisons, or the workplace. The interventions were tailored to the target populations and could be adapted for smaller communities, communities with less resources, and communities from different geographic regions.
Other severe weather events represented in this review included coastal and winter storms, drought, heat waves, and flooding. Although the tools were not implemented and evaluated to demonstrate their ability to measure or enhance community resilience, many of them could be piloted for localized, severe weather events. For instance, the Fault Tree model [75], which incorporated road systems data, may identify transportation system vulnerabilities for local planners working to improve recovery and resilience during floods, severe wind events, ice storms, or fires that disrupt accessibility to local road systems. While built on food systems resilience, the model could be applied to emergency supplies or other health-related resource needs and incorporated into a resilience-building intervention.
Pre-planning is paramount to community recovery efforts and resilience during and after an event. A community resilience study in New York after Superstorm Sandy found that recovery partnerships formed before an event were more sustainable than partnerships formed during or after an event occurred [76]. Zukowski (2014) [77], in an assessment of community resilience for all U.S. counties, found that response and recovery were improved in communities that incorporated pre-planning, protocols, exercises, and community engagement in the form of education, exercises, and community partnerships. The Assessment for Disaster Engagement with Partners Tool (ADEPT) model could be used as a baseline tool for local planners wanting to assess community partnerships before developing a disaster preparedness and recovery network; higher scores on the assessment indicate more active relationships with community and faith-based organizations [78].
4.4. Gaps in the Literature
Our review found several gaps in the literature. First and foremost was the lack of interventions, tools, and metrics that were implemented or evaluated in the New England region. This review located interventions that reflected impacts of hurricanes and floods upon relatively large geographic areas. There is a need for research and interventions to build community resilience in smaller communities with localized disasters, especially for communities that do not qualify for FEMA funding, regardless of disaster impact, due to lower recovery costs or geographical area damaged.
Our search returned no results of interventions designed to address the health impacts associated with climate-related hazards and that are increasing in New England: extreme flooding; extreme heat; mental health impacts; and vector-borne diseases such as Lyme disease [3,79]. We found no interventions that addressed the mental health challenges of multiple events, such as a hurricane followed by flooding followed by a heat wave, or a heavy snow or ice event followed by flooding or a power outage.
For example, many rural communities in Vermont were devastated by the destruction of the transportation and communication systems resulting from the flooding caused by Tropical Storm Irene in 2011 [80]; they did not have the resources to adapt and implement a disaster recovery assessment tool for their recovery needs. We view these gaps in the literature as opportunities for targeted research to advance the field of community resilience.
One additional limitation was that our review located only single-event studies. There were no peer-reviewed articles that described studies within the Northeast using the same methodology to compare design, metrics, and outcomes across multiple and/or geographically separated interventions. There were no articles that demonstrated how communities incorporated the resilience-building strategies into their everyday capacity-building efforts. In addition, and most important for a discussion on building and maintaining community resilience, we found no articles that evaluated the effectiveness of an intervention months or years later.
We attribute the lack of evidence-based literature in part to the way in which databases and search engines are designed. Our search returned no published studies on community resilience in New England; however, we know that studies do exist. We believe the issue is that some tools and metrics are published in journals that appear in specific databases so our searches did not capture all of the relevant articles. For example, despite most of our initial articles appearing in the Web of Science, four of the five articles that met our criteria were found using PubMed.
4.5. Limitations
There were limitations for this review that may affect the applicability of its findings. Our review explored literature specifically from the Northeast and Mid-Atlantic regions, to identify evidence-based interventions and strategies focused on community resilience. As a result, studies that reported on interventions or tools focused on extreme weather in other regions of the United States were not included. Studies that did not view the research from a resilience framework may not have been selected for this review. For example, we were unable to compare the interventions in this review with interventions from 35 states outside the Northeast that used the CDC’s Community Assessment for Public Health Emergency Response (CASPER) tool as a component of the intervention [81]. CASPER generates an interview-based, household-level, public health needs assessment for disaster awareness, preparedness, response, and recovery [82]. CASPER was used for community health assessment, emergency preparedness, and tick and mosquito bite prevention in New England, and to assess Superstorm Sandy response needs in New York. However, the results were not published in a peer-reviewed journal.
Another potential limitation of this study was that we included only peer-reviewed articles, eliminating gray literature, such as white papers, dissertations, and publicly available articles. Climate and health adaptation plans and interventions were implemented in New England using the BRACE framework to address extreme precipitation, heat stress, tickborne illness, and other climate-related hazards [79]. However, these works do not appear in the peer-reviewed literature and, therefore, were not added to the small list of evidence-based interventions on community resilience. The lack of peer-reviewed literature from the Northeast may be indicative of the scale and frequency of events and disasters compared to other U.S. regions that generate more substantial research and publications and are more robustly funded.
In our research, we surfaced two in-depth case studies of public health community resilience interventions: one well-developed community resilience framework from Los Angeles County; the other, from New Hampshire. We did not include these case studies in this review because the first was outside the geographic scope criterion and the second was from the gray literature. We describe these case studies in a separate publication [83].
5. Conclusions
The purpose of our research was to identify evidence-based interventions and metrics that were used to build and measure community resilience in the Northeast United States. We were interested in locating studies to serve as models for local public health planners and for communities with modest resources to help a community prepare for, withstand, recover from, and prevent the physical and mental health impacts of a climate change-related natural disaster. This research identified five peer-reviewed articles to serve as models for future community resilience initiatives.
Local planners and public health professionals who wish to measure community resilience need readily available resources that are cost effective, time efficient, and easy to access, whether they want to implement an intervention, or just establish a baseline assessment for community resilience planning. We propose that much of the data needed for measuring resilience can be generated through the use of semi-structured interviews, surveys, and focus groups. Additional demographic and socio-economic data can be gathered from publicly available sources, such as the U.S. census website. Online mapping tools, including the National Environmental Public Health Tracking Program [84], weather stations, and local emergency preparedness, mitigation, and recovery plans can generate low-cost data needed for other metrics. We suggest that community partnerships are a critically important resource for additional data as community-based organizations and other local entities may have access to resources and personnel unavailable to smaller local governments.
We recommend that interventions to build community resilience attempt to: (1) use pre- and post-intervention surveys to document progress and participant input; (2) engage the community in the entire process; and (3) publish the results to inform other local planners and public health officials while advancing the field of community resilience.
Replicating the use of these tools for assessment and enhancement of community resilience would: (1) advance our knowledge of the intervention or tool’s effectiveness over time; (2) indicate the stage of recovery for the community; and (3) determine the community’s adaptive capacity and resilience.
We recommend that local planners and public health practitioners review the literature cited in this article for suggestions on enhancing community resilience in their own jurisdictions. We encourage local health officials to implement community resilience interventions using evidence-based models, and frameworks, such as BRACE, which has low exposure in the peer-reviewed literature. We encourage those developing tools and frameworks to engage the community in piloting and improving tools for low-cost implementation using readily accessible data. We encourage community engagement and public participation in initiatives that increase social cohesion and ownership of both the process and outcome known as community resilience.
This review identified the paucity of peer-reviewed literature from the Northeast and Mid-Atlantic regions that is currently available to serve as models for building and measuring community resilience. While the public health and resilience community has conducted assessments to determine health risks within a community that align with some of the CDC national standards, few assessments revealed evidence-based interventions or tools designed to enhance community resilience that were implemented and evaluated. We found five evidence-based projects to guide local planners and public health officials in designing and implementing their own resilience interventions.
The models that best approached strengthening and measurement of public health dimensions of community resilience were the COAST project and the COPEWELL rubric. We suggest that these models could be adapted for use by public health officials in other states or regions, in other settings, and with other populations or extreme weather events to achieve the U.S. National Preparedness Goal. The models used easily accessible data sources, including participant-based data. They demonstrated the use of metrics to measure the extent to which community resilience was enhanced through these interventions. The Ready CDC intervention, which incorporated the TTM behavior assessment method, offered an easy-to-implement, evidence-based approach. Gaps that we identified in the literature offer rich applied research opportunities moving forward. We encourage local planners and public health officials to draw on the insights gained by this review to enhance community resilience in their own jurisdictions through adaptation and implementation of the interventions and metrics discussed here.
Author Contributions
Conceptualization, A.A.W., M.J.C., and K.B.; methodology, A.A.W. and J.M.; formal analysis, A.A.W. and J.M.; investigation, J.M.; writing—original draft preparation, J.M. and A.A.W.; writing—review and editing, A.A.W., M.J.C., and K.B.; supervision, A.A.W.; project administration, A.A.W.; funding acquisition, A.A.W. and M.J.C. All authors have read and agreed to the published version of the manuscript.
Funding
This report was supported by grant #5 NUE1EH001332-04-00 provided by the Centers for Disease Control and Prevention (CDC) in Atlanta, and administered by the New Hampshire Department of Health and Human Services (DHHS). The findings and conclusion do not necessarily reflect the opinions or position of the CDC.
Acknowledgments
We are grateful to Terri Downing, Don Woodhouse, and Rich Ryan for their administrative support of this project.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
Table A1.
Community Resilience Interventions and Metrics with Climate Focus and Health Impact.
Table A1.
Community Resilience Interventions and Metrics with Climate Focus and Health Impact.
| Climate and Health Focus | Target Population and Location | Study Type | Formative Metrics (Unit Measured) | Summative Metrics (Health-Related Outcomes) | Method/Data Sources | Data Available Locally? | 2011 CDC National Standards a | Source |
|---|---|---|---|---|---|---|---|---|
| Hurricane recovery (Superstorm Sandy) and mental health resilience | Community mental health workers in NY and NJ | Mental health intervention | Self-efficacy, stress response, coping strategies, demographics | RCHC intervention increased perceived knowledge and decreased stress scores | Participant surveys and interviews before, during, and after education intervention | √ | b, c, d, f | Powell and Yuma-Guerrero (2016) [52] |
| Hurricane and flood recovery (Superstorm Sandy), community mental health | Residents of Long Island, Queens and Rockaways, NY | Health study | Hurricane exposure (including flood severity), PTSD | More participants from the Rockaways reported PTSD symptoms than from Queens and lower Manhattan | LIGHT Study, Project Restoration, World Trade Center Health Registry | √ | a, c, e | Schwartz et al. (2019) [85] |
| Hurricane recovery (Superstorm Sandy) and mental health | Residents of Oakwood, NY | Health study | Effects of buyout program on peripheral community | Peripheral community experienced loss of safety, and trust in government, affecting recovery process | Qualitative interviews with residents near buyout zone; field notes from interviewers | √ | a, c, e | Binder et al. (2020) [86] |
| Hurricane recovery (Superstorm Sandy) and mental health | Residents of New York City | Health study | PTSD, depression, location, demographics | Mapped results showed clusters of PTSD and depression more prevalent in areas exposed to the ocean | Telephone survey, Posttraumatic Stress Checklist, Patient Health Questionnaire; NYC Department of City Planning | √ | a, c, e | Gruebner et al. (2015) [87] |
| Hurricane recovery (Superstorm Sandy) and mental health | Residents along the eastern shore of Staten Island, NY | Community resilience study | Perceived recovery, neighborhood satisfaction | Residents satisfied with neighborhoods and/or had a college education perceived a higher recovery rate | Mail survey to residents; US census | √ | c | Frey, N. (2017) [88] |
| Hurricane recovery (Superstorm Sandy) and community resilience | Students, parents, teachers in Far Rockaway and Long Beach, NY | Mental health intervention | Coping skills, behavioral risk and stress reduction, PTSD, depression | Youth PTSD and depression reduced; model adopted for Long Beach’s curriculum; students created YouTube PSA | Pre and post survey of students, parents, educators, and school-based providers participating in COAST Project | √ | All of the above | D’Amico et al. (2017) [51] |
| Hurricane recovery (Superstorm Sandy) and community resilience | Community in Hudson County, NJ | Community resilience tool | Pre-event planning, municipal operations, demographics | Piloted Garden State model; community in need of Continuity of Operations Plan for flooding, storm surge, and sea level rise impacts | Emergency plans; geospatial mapping of flooding, sea level rise, and storm surge; risk assessment index; in-person discussions | √ | a, b, c, e, f, g | Bowman and Newman (2017) [55] |
| Hurricane (Superstorm Sandy) and urban neighborhood resilience | Residents of New York City | Community resilience tool | Distance to emergency services and transportation, % of area flooded | REDI found that neighborhood resilience capacity decreased as distance from public transportation and city infrastructure increased | NYC 311 system; US census; NYCDCP; MTA; FEMA Hurricane Sandy Impact Analysis; NYC Emergency Management Hurricane Evacuation Centers; NYC Directory of Parks Properties; NYC Street Tree Census | May be time-consuming; data available online | c, e | Kontokosta and Malik (2018) [71] |
| Hurricane (Superstorm Sandy) and community partnership network resilience | Community-based organizations in New York City | Community resilience study | Structure and durability of partnerships, storm exposure and effects | Recovery partnerships formed before disaster were more sustainable than partnerships formed after and in relation to disaster | Online survey to partnership networks of community-based organizations and NY Department of Health and Mental Hygiene | √ | a, c, e | Acosta et al. (2018) [76] |
| Hurricane recovery (Superstorm Sandy) | Residents of Oakwood Beach and Rockaway Park, New York City | Community resilience study | Disaster management, exposure to hurricane, demographics | Loss of neighborhood and sense of place affected a community’s decision to relocate or rebuild | Survey based on CART resilience domains; interviews with residents | √ | c, e | Binder, Baker, and Barile (2015) [89] |
| Community recovery and resilience (hurricane example) | Counties in the United States | Community resilience tool | Population demographics, infrastructure, and community resources | Piloted the COPEWELL model; produced a county-level map of community functioning and resilience | County level data | May be time-consuming | a, b, c, e | Links et al. (2018) [72] |
| Hurricane (Superstorm Sandy) and coastal port resilience | Stakeholders of the Red Hook Container Terminal, Brooklyn, NY | Community resilience study | Damages interrupting operations and impairing recovery | Disruption of food, blood, medical and emergency supplies; emotional toll from damage and power outages; recovery impaired where no pre-event coordination | Interviews with stakeholders (Port Authority of NY & NJ, Coast Guard, Portside New York); review of news and technical damage reports | √ | c, e | Ryan-Henry and Becker (2020) [90] |
| Diverse threats (winter storm, drought) and food system resilience | Residents of city of Baltimore, MD, and state of California | Community resilience tool | Barriers to transportation, supply, distribution; production failures | Fault tree model found winter storm and drought disrupted food systems, making food inaccessible, unavailable, or unacceptable for consumption | Baltimore DOT and Maryland Transport Administration (winter storm); CA agricultural production data (drought 2013–2017) | √ | a, c | Chodur et al. (2018) [75] |
| Multiple hazard risks (heat waves and flooding) | Residents of New York City | Community resilience study | Hurricane inundation zones, demographics | Combined vulnerability and multi-hazard risks on map of New York City; suggested prioritizing adaptation and mitigation measures in highest risk coastal areas of Brooklyn, Bronx, and Harlem | NOAA temperature and precipitation data (Central Park); New York Times (articles day after event); local decision-maker survey; US census data; 311 call data | √ | a, c, e | Depietri et al. (2018) [91] |
| Weather hazards and community resilience and social vulnerability | Counties in the United States | Community resilience study | Population density and demographics, county resources, civic organizations | Mapped hazard risk and capacity for recovery; high vulnerability correlated with low resilience; Midwest and Northeast more resilient and less vulnerable than South and West | US Census data and shapefiles, USA Counties website, City & County Data book; NY Times 2008 Presidential election voting data, Association of Religion Data archives | √ | a, c | Bergstrand et al. (2015) [92] |
| Coastal storm vulnerability | Counties along US Atlantic coast | Community resilience study | Ocean distance, population demographics | Developed Coastal Risk Index with and without natural coastal habitat scenarios; 40% more counties at high risk without natural coastal habitat | Bio-geo-physical data (natural habitat type, geomorphology, coastal relief, wind and wave exposure, surge potential, elevation); US Atlantic coast historical sea level trends | May be time-consuming, costly, technical | a, c | Sajjad et al. (2020) [73] |
| Drought recovery | Municipalities across the US | Community resilience study | Water conservation, drought plan | Media more likely to report on short-term emergency-coping responses rather than long-term drought resilience initiatives | NDMC’s Drought Impact Reporter database | √ | c | Jedd, T.M. (2019) [93] |
| Community disaster resilience | Community partners in Chester County, PA and community members in Coatesville, PA | Social capital and community engagement tool development and pilot | Participation in community groups, trust, connectedness | Piloted COPEWELL rubric’s social capital domain; user’s guide needed for community self-assessment | Participant knowledge and experience on social capital and resilience. | √ | a, b, c, e | Schoch-Spana et al. (2019) [54] |
| Disaster resilience and social capital | Counties across the US | Community resilience tool | Demographics, civic organizations, political activities | Created Social Capital Index; highest social capital in West and South, lowest in Southwest | US Census 2010; County Business Patterns 2010; ESRI | √ | c | Kyne and Aldrich (2020) [94] |
| Disaster preparedness | CDC staff in GA, WV and CO | Community resilience intervention | Preparedness attitudes and behaviors | Emergency preparedness knowledge and community resilience increased. | Ready CDC evaluation and pre-post survey | √ | a, c, d, g | Thomas et al. (2018) [53] |
| Disaster response & recovery | Counties and parishes in US affected by major disaster in 2011 | Community resilience study | Pre-event response and recovery plans, partnerships, training | Pre-event planning, NIMS, ICS, full-scale exercises, and community engagement improved response and recovery outcomes | Survey of local county emergency managers; 2010 US Census; FEMA regional data | √ | c, e | Zukowski, R. S. (2014) [77] |
| Disaster recovery | Disaster recovery experts in US | Community engagement tool pilot | Disaster plans, demographics, FEMA funding | Developed online Recovery Indicators Tool; adding spatial data would aid recovery assistance | Interviews and focus groups with experts; pre-disaster recovery plans; case studies in NJ and NC | Open source data unavailable for some metrics | a, b, c, e, f | Dwyer and Horney (2014) [48] |
| Disaster preparedness, response, and recovery collaboration | Local health departments and community/faith-based organizations in the US | Community resilience tool | Engaging or collaborating with organizations in trainings and outreach | Piloted ADEPT; higher scores reflected more active relationships with community and faith-based organizations for disaster preparedness, response, and recovery collaboration | National survey of local health department disaster preparedness coordinators | √ | b, c | Glik et al. (2014) [78] |
| Disaster communication | Journalists across the US | Community resilience study | Warnings, disaster reports, mitigation information | Journalists facilitated recovery via information and engaging the community; disaster reporting increased stress and depression | Telephone interviews with US journalists | √ | c | Houston et al. (2019) [95] |
Notes. Abbreviations include: CDC: Centers for Disease Control and Prevention; RCHC: Resilience and Coping for the Healthcare Community; PTSD: post-traumatic stress disorder; PSA: public service announcement; COAST: Creating Optimism After Sandy Trauma; COPEWELL: Composite of Post-Event Well-being model. a CDC National Standards: (a) determining health risks in a community; (b) coordinating and strengthening community partnerships; (c) sharing information; (d) providing preparedness trainings; (e) identifying recovery needs; (f) supporting recovery operations; and g) implementing actions to mitigate future adverse effects from future incidents.
Table A2.
Resource List of Toolkits to Measure Community Resilience.
Table A2.
Resource List of Toolkits to Measure Community Resilience.
| Toolkit | Target Population/Task | Source |
|---|---|---|
| Assessment for Disaster Engagement with Partners Toolkit (ADEPT) | Local health departments building community partnerships | Martel et al. (2014) Retrieved 13 September 2020 from https://cphd.ph.ucla.edu/sites/default/files/downloads/ADEPT%20Toolkit.pdf [96] |
| Baseline Resilience Indicators for Communities (BRIC) | Health and planning officials comparing communities at the county level using social, economic, community, institutional, infrastructure, and environment resilience indicators; scores available for 2010 and 2015 | University of South Carolina College of Arts and Sciences (n.d.) Retrieved 13 September 2020 from https://artsandsciences.sc.edu/geog/hvri/bric [97] |
| Building Resilience Against Climate Effects Framework (BRACE) | Health officials assisting communities prepare for climate-related health hazards | Centers for Disease Control and Prevention (2019c) Retrieved 9 September 2020 from https://www.cdc.gov/climateandhealth/BRACE.htm [98] |
| Communities Advancing Resilience Toolkit (CART) | Communities self-assessing their capacity for disaster preparedness, prevention, response, and recovery | Pfefferbaum et al. (2011) Retrieved 14 September 2020 from https://www.oumedicine.com/docs/ad-psychiatry-workfiles/cart_online-final_042012.pdf [99] |
| Community Assessment for Public Health Emergency Response Toolkit, 3rd edition (CASPER) | Public health and emergency managers assessing community needs at the household level | Centers for Disease Control and Prevention (2020a) Retrieved 29 July 2020 from https://www.cdc.gov/nceh/casper/default.htm [81] |
| COPEWELL Rubric Self-Assessment Tools | Communities wanting to self-assess community functioning; population, vulnerability, inequality, and deprivation; prevention and mitigation; social capital and cohesion; emergency management | Johns Hopkins University (2020) Retrieved 13 September 2020 from https://www.copewellmodel.org/self-assessment-tools.html [100] |
| PARTNER Tool | Communities assessing community partnerships and networks | Visible Network Labs (2010) Retrieved 28 July 2020 from https://visiblenetworklabs.com/partner-platform/ [101] |
| Resilience Builder Toolkit | Communities wanting to identify community needs to build a resilience work plan | Chandra et al. (2015b) Retrieved 14 September 2020 from http://www.laresilience.org/documents/resilience-builder.pdf [102] |
| Social Vulnerability Index | Local officials wanting to identify vulnerable populations | Agency for Toxic Substances and Disease Registry (2018) Retrieved 24 August 2020 from https://svi.cdc.gov/ [43] |
| TTM Transtheoretical Model of Behavior Change | Public health officials measuring changes in stages of emergency preparedness actions and attitudes | Pro-Change Behavior Systems Inc. (2018) Retrieved 14 September 2020 from https://www.prochange.com/transtheoretical-model-of-behavior-change |
| U.S. Climate Resilience Toolkit | Over 200 tools for communities and local planners to create plans and build resilience | Tools|U.S. Climate Resilience Toolkit (2020) Retrieved 13 September 2020 from https://toolkit.climate.gov/tools [103] |
References
- Ghazali, D.A.; Guericolas, M.; Thys, F.; Sarasin, F.; Arcos González, P.; Casalino, E. Climate change impacts on disaster and emergency medicine focusing on mitigation disruptive effects: An international perspective. Int. J. Environ. Res. Public Health 2018, 15, 1379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- IPCC. Summary for Policy Makers. In Global Warming of 1.5 °C. An IPCC Special Report on the Impacts of Global Warming of 1.5 °C above Pre-industrial Levels and Related Global Greenhouse Gas Emission Pathways, in the Context of Strengthening the Global Response to the Threat of Climate Change, Sustainable Development, and Efforts to Eradicate Poverty; Masson-Delmotte, V., Zhai, P., Pörtner, H.-O., Roberts, D., Skea, J., Shukla, P.R., Pirani, A., Moufouma-Okia, W., Péan, C., Pidcock, R., et al., Eds.; IPCC: Geneva, Switzerland, 2018; Available online: https://www.ipcc.ch/site/assets/uploads/sites/2/2019/05/SR15_SPM_version_report_LR.pdf (accessed on 28 July 2020).
- USGCRP. Impacts, Risks, and Adaptation in the United States: Fourth National Climate Assessment, Volume II; U.S. Global Change Research Program: Washington, DC, USA, 2018; p. 1515. Available online: https://nca2018.globalchange.gov (accessed on 10 April 2020).
- Ebi, K.L.; Balbus, J.M.; Luber, G.; Bole, A.; Crimmins, A.; Glass, G.; Saha, S.; Shimamoto, M.M.; Trtanj, J.; White-Newsome, J.L. Human Health. In Impacts, Risks, and Adaptation in the United States: Fourth National Climate Assessment; U.S. Global Change Research Program: Washington, DC, USA, 2018; Volume II, pp. 572–603. Available online: https://nca2018.globalchange.gov/downloads/NCA4_Ch14_Human-Health_Full.pdf (accessed on 26 April 2020).
- Petkova, E.P.; Ebi, K.L.; Culp, D.; Redlener, I.E. Climate change and health on the u.s. gulf coast: Public health adaptation is needed to address future risks. Int. J. Environ. Res. Public Health 2015, 12, 9342–9356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- March, G. Natural Disasters and the Impacts on Health; University of Western Ontario: London, ON, Canada, 2002; p. 18. Available online: https://www.eird.org/isdrbiblio/PDF/Natural%20disasters%20and%20the%20impacts.pdf (accessed on 18 March 2020).
- Keller, L.O.; Strohschein, S.; Lia-Hoagberg, B.; Schaffer, M.A. Population-based public health interventions: Practice-based and evidence-supported. Part I. Public Health Nurs. 2013, 21, 453–468. [Google Scholar] [CrossRef]
- Marinucci, G.D.; Luber, G.; Uejio, C.K.; Saha, S.; Hess, J.J. Building resilience against climate effects—A novel framework to facilitate climate readiness in public health agencies. Int. J. Environ. Res. Public Health 2014, 11, 6433–6458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacQueen, K.M.; McLellan, E.; Metzger, D.S.; Kegeles, S.; Strauss, R.P.; Scotti, R.; Blanchard, L.; Trotter, R.T. What is community? An evidence-based definition for participatory public health. Am. J. Public Health 2001, 91, 1929–1938. [Google Scholar] [CrossRef]
- Sharifi, A. A critical review of selected tools for assessing community resilience. Ecol. Indic. 2016, 69, 629–647. [Google Scholar] [CrossRef] [Green Version]
- Winter, J.M.; Bowen, F.L.; Partridge, T.F.; Chipman, J.W. Future extreme event risk in the rural northeastern united states. Ann. Am. Assoc. Geogr. 2019, 109, 1110–1130. [Google Scholar] [CrossRef]
- Dupigny-Giroux, L.A.; Mecray, E.L.; Lemcke-Stampone, M.D.; Hodgkins, G.A.; Lentz, E.E.; Mills, K.E.; Lane, E.D.; Miller, R.; Hollinger, D.Y.; Solecki, W.D.; et al. Northeast. In Impacts, Risks, and Adaptation in the United States: Fourth National Climate Assessment, Volume II; Reidmiller, D.R., Avery, C.W., Easterling, D.R., Kunkel, K.E., Lewis, K.L.M., Maycock, T.K., Stewart, B.C., Eds.; U.S. Global Change Research Program: Washington, DC, USA, 2018; pp. 669–742. [Google Scholar] [CrossRef]
- Rustad, L.; Campbell, J.; Dukes, J.S.; Huntington, T.; Lambert, K.F.; Mohan, J.; Rodenhouse, N. Changing Climate, Changing Forests: The Impacts of Climate Change on Forests of the Northeastern United States and Eastern Canada; General Technical Report NRS-99; US Forest Service Northern Research Station: Madison, WI, USA, 2012; p. 50. Available online: https://www.nrs.fs.fed.us/pubs/gtr/gtr_nrs99.pdf (accessed on 17 February 2019).
- Zahmatkesh, Z.; Karamouz, M. An uncertainty-based framework to quantifying climate change impacts on coastal flood vulnerability: Case study of New York City. Environ. Monit. Assessm. 2017, 189, 567. [Google Scholar] [CrossRef] [PubMed]
- Department of Homeland Security. National Preparedness Guidelines, September 2007; Department of Homeland Security: Washington, DC, USA, 2007; p. 51. Available online: https://www.cms.gov/Medicare/Provider-Enrollment-and-Certification/SurveyCertEmergPrep/Downloads/National-Preparedness-Guidelines.pdf (accessed on 19 September 2020).
- White House. Presidential Policy Directive/PPD-8: National Preparedness. The White House. 2011. Available online: https://www.dhs.gov/xlibrary/assets/presidential-policy-directive-8-national-preparedness.pdf (accessed on 19 September 2020).
- FEMA. National Preparedness Goal, 1st ed.; U.S. Department of Homeland Security: Washington, DC, USA, 2011; p. 26. Available online: https://www.fema.gov/pdf/prepared/npg.pdf (accessed on 28 July 2020).
- FEMA. National Preparedness Goal, Second Edition, September 2015; U.S. Department of Homeland Security: Washington, DC, USA, 2015; p. 29. Available online: https://www.fema.gov/media-library-data/1443799615171-2aae90be55041740f97e8532fc680d40/National_Preparedness_Goal_2nd_Edition.pdf (accessed on 7 April 2020).
- Centers for Disease Control and Prevention (CDC). Public Health Emergency Preparedness and Response Capabilities: National Standards for State, Local, Tribal, and Territorial Public Health—October 2018; U.S. Department of Health and Human Services: Washington, DC, USA, 2019; p. 176. Available online: https://www.cdc.gov/cpr/readiness/00_docs/CDC_PreparednesResponseCapabilities_October2018_Final_508.pdf (accessed on 26 February 2020).
- Chandra, A.; Acosta, J.; Meredith, L.; Sanches, K.; Howard, S.; Uscher-Pines, L.; Williams, M.; Yeung, D. Understanding Community Resilience in the Context of National Health Security: A Literature Review; Working Paper WR-737-DHHS; RAND Corporation: Santa Monica, CA, USA, 2010; p. 39. [Google Scholar] [CrossRef] [Green Version]
- Patel, S.S.; Rogers, M.B.; Amlôt, R.; Rubin, G.J. What do we mean by ‘community resilience’? A systematic literature review of how it is defined in the literature. PLOS Curr. Disasters 2017, 9, 34. [Google Scholar] [CrossRef]
- Djalante, R.; Thomalla, F. Community resilience to natural hazards and climate change: A review of definitions and operational frameworks. Asian J. Environ. Disaster Manag. 2011, 3, 164–178. [Google Scholar] [CrossRef]
- Chuang, W.C.; Garmestani, A.; Eason, T.N.; Spanbauer, T.L.; Fried-Petersen, H.B.; Roberts, C.P.; Sundstrom, S.M.; Burnett, J.L.; Angeler, D.G.; Chaffin, B.C.; et al. Enhancing quantitative approaches for assessing community resilience. J. Environ. Manag. 2018, 213, 353–362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plough, A.; Fielding, J.E.; Chandra, A.; Williams, M.; Eisenman, D.; Wells, K.B.; Law, G.Y.; Fogleman, S.; Magaña, A. Building community disaster resilience: Perspectives from a large urban county department of public health. Am. J. Public Health 2013, 103, 1190–1197. [Google Scholar] [CrossRef] [PubMed]
- United Nations Office for Disaster Risk Reduction. Proposed Updated Terminology on Disaster Risk Reduction: A Technical Review; Background Paper; The United Nations Office for Disaster Risk Reduction: Geneva, Switzerland, 2015; p. 32. Available online: https://www.preventionweb.net/files/45462_backgoundpaperonterminologyaugust20.pdf (accessed on 28 July 2020).
- Goodykoontz, E.; Taylor, A. (Eds.) Measuring for Results: Application of Key Concepts to Resilience Measurement 12 October 2015; Publication No. RP14-02.02-02; 2015; p. 134. Available online: https://www.anser.org/docs/reports/HSSAI_Report-MeasuringforResults-ApplicationofKeyConceptstoResilienceMeasurement-10-12-15.pdf (accessed on 21 February 2020).
- Summers, J.K.; Harwell, L.C.; Smith, L.M.; Buck, K.D. Measuring community resilience to natural hazards: The natural hazard resilience screening index (nahrsi)—Development and application to the United States. GeoHealth 2018, 2, 372–394. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services. Community Resilience; Public Health Emergency: Washington, DC, USA, 2015. Available online: https://www.phe.gov/Preparedness/planning/abc/Pages/community-resilience.aspx (accessed on 13 July 2020).
- CDC. Center for Preparedness and Response: Create Community; Centers for Disease Control and Prevention: Athens, GA, USA, 2020. Available online: https://www.cdc.gov/prepyourhealth/createcommunity/index.htm (accessed on 16 April 2020).
- DeSalvo, K.B.; Wang, Y.C.; Harris, A.; Auerbach, J.; Koo, D.; O’Carroll, P. Public Health 3.0: A call to action for public health to meet the challenges of the 21st Century. Prev. Chronic Dis. 2017, 14, 170017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- U.S. Department of Health and Human Services. Roundtable on the National Health Security Strategy and At-Risk Individuals, Behavioral Health, and Community Resilience; U.S. Department of Health and Human Services, Office of the Assistant Secretary for Preparedness and Response: Washington, DC, USA, 2010; p. 32. Available online: https://www.phe.gov/Preparedness/planning/abc/Documents/nhss-roundtable-110128.pdf (accessed on 11 July 2020).
- Eisenman, D.; Chandra, A.; Fogleman, S.; Magana, A.; Hendricks, A.; Wells, K.; Williams, M.; Tang, J.; Plough, A. The Los Angeles county community disaster resilience project—A community-level, public health initiative to build community disaster resilience. Int. J. Environ. Res. Public Health 2014, 11, 8475–8490. [Google Scholar] [CrossRef] [Green Version]
- Pfefferbaum, B.; Pfefferbaum, R.L.; Van Horn, R.L. Community resilience interventions: Participatory, assessment-based, action-oriented processes. Am. Behav. Sci. 2015, 59, 238–253. [Google Scholar] [CrossRef]
- Community and Regional Resilience Institute (CARRI). Building Resilience in America’s Communities: Observations and Implications of the CRS Pilots, a CARRI Report; Community and Regional Resilience Institute: Portland, OR, USA, 2013; p. 79. Available online: http://community.resilienceguild.org/system/files/CRS-Final-Report.pdf (accessed on 7 April 2020).
- Haarsaker, C. Integrating Disaster Risk Reduction and Climate Change Adaptation in the UN Sustainable Development Cooperation Framework: Guidance Note on Using Climate and Disaster Risk Management to Help Build Resilient Societies (Draft); Guidance Note; United Nations Office for Disaster Risk Reduction: Geneva, Switzerland, 2020; Available online: https://www.undrr.org/publication/integrating-disaster-risk-reduction-and-climate-change-adaptation-un-sustainable (accessed on 13 July 2020).
- Chandra, A.; Acosta, J.D.; Howard, S.; Uscher-Pines, L.; Williams, M.V.; Yeung, D.; Garnett, J.; Meredith, L.S. Building Community Resilience to Disasters: A Way Forward to Enhance National Health Security; Technical Report No. TR915; RAND Corporation: Santa Monica, CA, USA, 2011; p. 102. Available online: https://www.rand.org/pubs/technical_reports/TR915.html (accessed on 7 February 2020).
- U.S. Department of Health and Human Services. Community Resilience; Public Health Emergency: Washington, DC, USA, 2017. Available online: https://www.phe.gov/Preparedness/planning/abc/Pages/community.aspx (accessed on 13 April 2020).
- U.S. Department of Health and Human Services. Individual Resilience; Public Health Emergency: Washington, DC, USA, 2018. Available online: https://www.phe.gov/Preparedness/planning/abc/Pages/individual-resilience.aspx (accessed on 13 July 2020).
- Manangan, A.P.; Uejio, C.K.; Sahai, S.; Schramm, P.J.; Marinucci, G.D.; Langford Brown, C.; Hess, J.J.; Luber, G. Assessing Health Vulnerability to Climate Change: A Guide for Health Departments; Climate and Health Technical Report Series No. CS249409-A; Climate and Health Program, Centers for Disease Control and Prevention: Atlanta, GA, USA, 2015; p. 24. Available online: https://www.cdc.gov/climateandhealth/pubs/AssessingHealthVulnerabilitytoClimateChange.pdf (accessed on 26 April 2020).
- Martin, S.A. A framework to understand the relationship between social factors that reduce resilience in cities: Application to the City of Boston. Int. J. Disaster Risk Reduct. 2015, 12, 53–80. [Google Scholar] [CrossRef] [Green Version]
- Cutter, S.L.; Barnes, L.; Berry, M.; Burton, C.; Evans, E.; Tate, E.; Webb, J. A place-based model for understanding community resilience to natural disasters. Glob. Environ. Chang. 2008, 18, 598–606. [Google Scholar] [CrossRef]
- Johansen, C.; Horney, J.; Tien, I. Metrics for evaluating and improving community resilience. J. Infrastruct. Syst. 2017, 23, 11. [Google Scholar] [CrossRef]
- Agency for Toxic Substances and Disease Registry. CDC’s Social Vulnerability Index (SVI). 2018. Available online: https://svi.cdc.gov/factsheet.html (accessed on 28 April 2020).
- Holt, D. Measuring Social Vulnerability. 2014. Available online: https://svi.cdc.gov/Documents/Publications/SVI_Community_Materials/Measuring%20social%20vulnerabilities%20holt_09Sep’14.pdf (accessed on 9 May 2020).
- NH Environmental Public Health Tracking Program. Social Vulnerability Index: An Emergency Response Tool; NH Department of Health and Human Services: Concord, NH, USA, 2018. Available online: https://www.nh.gov/epht/highlights/documents/social-vulnerability-index.pdf (accessed on 16 July 2020).
- Kirshen, P.; Aytur, S.; Burdick, D.M.; Foster, D.; Lippmann, T.; Douglas, E.; Nick, S.; Watson, C. Integrated Analysis of the Value of Wetland Services in Coastal Adaptation; Methodology and Case Study of Hampton-Seabrook Estuary, New Hampshire; Institute for the Study of Earth, Oceans, and Space, University of New Hampshire: Durham, NH, USA, 2018; p. 68. Available online: https://scholars.unh.edu/cgi/viewcontent.cgi?article=1154&context=jel (accessed on 11 May 2020).
- Leiter, T.; Pringle, P. Pitfalls and potential of measuring climate change adaptation through adaptation metrics. In Adaptation Metrics: Perspectives on Measuring, Aggregating and Comparing Adaptation Results; Christiansen, L., Martinez, G., Naswa, P., Eds.; UNEP DTU Partnership: Copenhagen, Denmark, 2018; pp. 29–47. Available online: https://resilientcities2018.iclei.org/wp-content/uploads/UDP_Perspectives-Adaptation-Metrics-WEB.pdf (accessed on 25 August 2020).
- Dwyer, C.; Horney, J. Validating indicators of disaster recovery with qualitative research. PLOS Curr. Disasters 2014, 6. [Google Scholar] [CrossRef]
- National Research Council. Developing a Framework for Measuring Community Resilience: Summary of a Workshop. In Developing a Framework for Measuring Community Resilience: Summary of a Workshop; National Academies Press (US): Washington, DC, USA, 2015. Available online: https://www.ncbi.nlm.nih.gov/books/NBK285736/ (accessed on 16 July 2020).
- Caye, M. Formative Research and Community Resilience: A Case of Under Addressed Youth Problem Gambling; Antioch University New England: Keene, NH, USA, 2012; Available online: https://aura.antioch.edu/cgi/viewcontent.cgi?article=1076&context=etds (accessed on 22 July 2020).
- D’Amico, P.J.; Carmine, L.; Roderick, H.; Vogel, M.D. A three-tiered model of school-based trauma services to address long-term impact of a major natural disaster. Adolesc. Psychiatry 2017, 7, 315–329. [Google Scholar] [CrossRef]
- Powell, T.; Yuma-Guerrero, P. Supporting community health workers after a disaster: Findings from a mixed-methods pilot evaluation study of a psychoeducational intervention. Disaster Med. Public Health Prep. 2016, 10, 754–761. [Google Scholar] [CrossRef]
- Thomas, T.N.; Sobelson, R.K.; Wigington, C.J.; Davis, A.L.; Harp, V.H.; Leander-Griffith, M.; Cioffi, J.P. Applying instructional design strategies and behavior theory to household disaster preparedness training. J. Public Health Manag. Pract. JPHMP 2018, 24, e16–e25. [Google Scholar] [CrossRef]
- Schoch-Spana, M.; Gill, K.; Hosangadi, D.; Slemp, C.; Burhans, R.; Zeis, J.; Carbone, E.G.; Links, J. The COPEWELL Rubric: A self-assessment toolkit to strengthen community resilience to disasters. Int. J. Environ. Res. Public Health 2019, 16, 2372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bowman, R.; Newman, A. A model to improve preparedness and strategically enhance resiliency at a community level: The Garden State approach. J. Bus. Contin. Emerg. Plan. 2017, 10, 124–131. [Google Scholar]
- Peterson, S. Screening and Assessment; The National Child Traumatic Stress Network: Boulder, CO, USA, 2017. Available online: https://www.nctsn.org/treatments-and-practices/screening-and-assessment (accessed on 30 August 2020).
- Foa, E.B.; Johnson, K.M.; Feeny, N.C.; Treadwell, K.R. The child PTSD Symptom Scale: A preliminary examination of its psychometric properties. J. Clin. Child Psychol. 2001, 30, 376–384. [Google Scholar] [CrossRef] [PubMed]
- Goodman, R.; Renfrew, D.; Mullick, M. Predicting type of psychiatric disorder from Strengths and Difficulties Questionnaire (SDQ) scores in child mental health clinics in London and Dhaka | SpringerLink. Eur. Child Adolesc. Psychiatry 2000, 9, 129–134. [Google Scholar] [CrossRef]
- Kovacs, M. Children’s Depression Inventory 2nd Edition™; MHS: North Tonawanda, NY, USA, 2019; Available online: https://www.apa.org/obesity-guideline/depression-inventory.pdf (accessed on 30 August 2020).
- Beck, A.T.; Steer, R.A.; Brown, G.K. Manual for the Beck Depression Inventory-Second Edition (BDI-II); Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Knight, M.D., Jr. The CRAFFT Screening Interview; The Center for Adolescent Substance Abuse Research, (CeASAR) at Boston Children’s Hospital: Boston, MA, USA, 2016; Available online: http://www.childrenshospital.org/~/media/microsites/ceasar/2016-2sided-crafft-card_clinician-interview.ashx?la=en (accessed on 30 August 2020).
- Stamm, B.H. Professional Quality of Life Scale (ProQOL) Compassion Satisfaction and Compassion Fatigue (ProQOL) Version 5 (2009); ProQOL: St. Paul, MN, USA, 2009; Available online: https://proqol.org/uploads/ProQOL_5_English.pdf (accessed on 30 August 2020).
- Cohen, S.; Kessler, R.; Underwood, G.L. Perceived Stress Scale; Oxford University Press: New York, NY, USA, 1994. [Google Scholar]
- Cox, T.; Mackay, C. The measurement of self-reported stress and arousal. Br. J. Psychol. 1985, 76 Pt 2, 183–186. [Google Scholar] [CrossRef] [PubMed]
- Chesney, M.A.; Neilands, T.B.; Chambers, D.B.; Taylor, J.M.; Folkman, S. Coping Self-Efficacy Scale; University of California San Francisco Department of Medicine: San Francisco, CA, USA, 2005; Available online: https://prevention.ucsf.edu/sites/prevention.ucsf.edu/files/CopingSelf-EfficacyScale.pdf (accessed on 30 August 2020).
- Prochaska, J.O.; DiClemente, C.C. Stages and processes of self-change in smoking: Toward an integrative model of change. J. Consult. Clin. Psychol. 1983, 51, 390–395. [Google Scholar] [CrossRef]
- Prochaska, J.O.; DiClemente, C.C.; Norcross, J.C. In search of how people change: Applications to addictive behaviors. Am. Psychol. 1992, 47, 1102–1114. [Google Scholar] [CrossRef]
- Abrash Walton, A. Positive deviance and behavior change: A research methods approach for understanding fossil fuel divestment. Energy Res. Soc. Sci. Probl. Method Soc. Study Energy Clim. Chang. 2018, 45, 235–249. [Google Scholar] [CrossRef]
- Ostadtaghizadeh, A.; Ardalan, A.; Paton, D.; Jabbari, H.; Khankeh, H.R. Community disaster resilience: A systematic review on assessment models and tools. PLoS Curr. Disasters 2015, 7. [Google Scholar] [CrossRef] [PubMed]
- Koliou, M.; van de Lindt, J.W.; McAllister, T.P.; Ellingwood, B.R.; Dillard, M.; Cutler, H. State of the research in community resilience: Progress and challenges. Sustain. Resil. Infrastruct. 2020, 5. [Google Scholar] [CrossRef] [PubMed]
- Kontokosta, C.E.; Malik, A. The resilience to emergencies and disasters index: Applying big data to benchmark and validate neighborhood resilience capacity. Sustain. Cities Soc. 2018, 36, 272–285. [Google Scholar] [CrossRef]
- Links, J.M.; Schwartz, B.S.; Lin, S.; Kanarek, N.; Mitrani-Reiser, J.; Sell, T.K.; Watson, C.R.; Ward, D.; Slemp, C.; Burhans, R.; et al. COPEWELL: A conceptual framework and system dynamics model for predicting community functioning and resilience after disasters. Disaster Med. Public Health Prep. 2018, 12, 127–137. [Google Scholar] [CrossRef]
- Sajjad, M.; Chan, J.C.L.; Lin, N. Incorporating natural habitats into coastal risk assessment frameworks. Environ. Sci. Policy 2020, 106, 99–110. [Google Scholar] [CrossRef]
- Abrash Walton, A.; Simpson, M.; Rhoades, J.; Daniels, C. Local Solutions Report: Identifying and Meeting the Needs of Local Communities Adapting to Climate Change; Center for Climate Preparedness and Community Resilience, Antioch University: New England, Keene, NH, USA, 2016; p. 48. [Google Scholar]
- Chodur, G.M.; Zhao, X.; Biehl, E.; Mitrani-Reiser, J.; Neff, R. Assessing food system vulnerabilities: A fault tree modeling approach. BMC Public Health 2018, 18, 817. [Google Scholar] [CrossRef]
- Acosta, J.D.; Burgette, L.; Chandra, A.; Eisenman, D.P.; Gonzalez, I.; Varda, D.; Xenakis, L. How community and public health partnerships contribute to disaster recovery and resilience. Disaster Med. Public Health Prep. 2018, 12, 635–643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zukowski, R.S. The impact of adaptive capacity on disaster response and recovery: Evidence supporting core community capabilities. Prehosp. Disaster Med. 2014, 29, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Glik, D.C.; Eisenman, D.P.; Donatello, I.; Afifi, A.; Stajura, M.; Prelip, M.L.; Sammartinova, J.; Martel, A. Reliability and validity of the Assessment for Disaster Engagement with Partners Tool (ADEPT) for local health departments. Public Health Rep. 2014, 129 (Suppl. 4), 77–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- New Hampshire Department of Health and Human Services. Lyme and Other Tickborne Diseases; NH Department of Health and Human Services Bureau of Infectious Disease Control: Washington, DC, USA, 2016. Available online: https://www.dhhs.nh.gov/dphs/cdcs/lyme/index.htm (accessed on 22 June 2020).
- Pierre-Louis, K. Five Years after Hurricane Irene, Vermont Still Striving for Resilience. Inside Climate News. 1 September 2016. Available online: https://insideclimatenews.org/news/31082016/five-years-after-hurricane-irene-2011-effects-flooding-vermont-damage-resilience-climate-change (accessed on 7 February 2020).
- Centers for Disease Control and Prevention. Community Assessment for Public Health Emergency Response (CASPER). 2020. Available online: https://www.cdc.gov/nceh/casper/default.htm (accessed on 29 July 2020).
- Centers for Disease Control and Prevention (CDC). Community Assessment for Public Health Emergency Response (CASPER) Toolkit: Third Edition; CDC: Athens, GA, USA, 2019; p. 64. Available online: https://www.cdc.gov/nceh/casper/docs/CASPER-toolkit-3_508.pdf (accessed on 29 July 2020).
- Abrash Walton, A.; Marr, J.; Bush, K.; Cahillane, M. How Do We Build Community Resilience to Disasters in a Changing Climate? A Review of Interventions to Improve and Measure Public Health Outcomes in the Northeastern United States. 2021. Available online: https://aura.antioch.edu/facarticles/72 (accessed on 27 July 2021).
- Centers for Disease Control and Prevention. National Environmental Public Health Tracking. 2020. Available online: https://www.cdc.gov/nceh/tracking/index.html (accessed on 23 July 2020).
- Schwartz, R.M.; Rasul, R.; Gargano, L.M.; Lieberman-Cribbin, W.; Brackbill, R.M.; Taioli, E. Examining associations between hurricane sandy exposure and posttraumatic stress disorder by community of residence. J. Trauma. Stress 2019, 32, 677–786. [Google Scholar] [CrossRef] [PubMed]
- Binder, S.B.; Ritchie, L.A.; Bender, R.; Thiel, A.; Baker, C.K.; Badillo, E.; Goodfellow, S.; Kulp, B.; Weir, P. Limbo: The unintended consequences of home buyout programmes on peripheral communities. Environ. Hazards 2020, 19, 488–507. [Google Scholar] [CrossRef]
- Gruebner, O.; Lowe, S.R.; Sampson, L.; Galea, S. The geography of post-disaster mental health: Spatial patterning of psychological vulnerability and resilience factors in New York City after Hurricane Sandy. Int. J. Health Geogr. 2015, 14, 16. [Google Scholar] [CrossRef] [Green Version]
- Frey, N. Place satisfaction and perceived recovery after Hurricane Sandy on Staten Island’s East Shore: Environmental Hazards. Environ. Hazards 2018, 17, 40–55. [Google Scholar] [CrossRef]
- Binder, S.B.; Baker, C.K.; Barile, J.P. Rebuild or Relocate? Resilience and Postdisaster Decision-Making After Hurricane Sandy. Am. J. Community Psychol. 2015, 56, 180–196. [Google Scholar] [CrossRef]
- Ryan-Henry, J.; Becker, A. Port stakeholder perceptions of Sandy impacts: A case study of Red Hook, New York. Marit. Policy Manag. 2020, 47, 885–902. [Google Scholar] [CrossRef] [Green Version]
- Depietri, Y.; Dahal, K.; McPhearson, T. Multi-hazard risks in New York City. Nat. Hazards Earth Syst. Sci. 2018, 18, 3363–3381. [Google Scholar] [CrossRef] [Green Version]
- Bergstrand, K.; Mayer, B.; Brumback, B.; Zhang, Y. Assessing the relationship between social vulnerability and community resilience to hazards. Soc. Indic. Res. 2015, 122, 391–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jedd, T.M. The limits of resilience in U.S. community responses to recent drought events. Community Dev. 2019, 50, 141–159. [Google Scholar] [CrossRef]
- Kyne, D.; Aldrich, D.P. Capturing Bonding, Bridging, and Linking Social Capital through Publicly Available Data. Risk Hazards Crisis Public Policy 2020, 11, 61–86. [Google Scholar] [CrossRef]
- Houston, J.B.; Schraedley, M.K.; Worley, M.E.; Reed, K.; Saidi, J. Disaster journalism: Fostering citizen and community disaster mitigation, preparedness, response, recovery, and resilience across the disaster cycle. Disasters 2019, 43, 591–611. [Google Scholar] [CrossRef] [PubMed]
- Martel, A.; Stajura, M.; Sammartinova, J.; Prelip, M.; Eisenman, D.; Glik, D. Assessment for Disaster Engagement with Partners Toolkit (ADEPT); UCLA Fielding School of Public Health: Los Angeles, CA, USA, 2014; Available online: https://cphd.ph.ucla.edu/sites/default/files/downloads/ADEPT%20Toolkit.pdf (accessed on 13 September 2020).
- University of South Carolina College of Arts and Sciences. Baseline Resilience Indicators for Communities (BRIC); University of South Carolina: Columbia, SC, USA, 2020; Available online: https://artsandsciences.sc.edu/geog/hvri/bric (accessed on 13 September 2020).
- Centers for Disease Control and Prevention. CDC’s Building Resilience Against Climate Effects (BRACE) Framework; CDC Climate and Health: Athens, GA, USA, 2019. Available online: https://www.cdc.gov/climateandhealth/BRACE.htm (accessed on 15 June 2020).
- Pfefferbaum, R.L.; Pfefferbaum, B.; Van Horn, R.L. Communities Advancing Resilience Toolkit (CART): The CART Integrated System©; Terrorism and Disaster Center at the University of Oklahoma Health Sciences Center: Oklahoma City, OK, USA, 2011; Available online: https://www.oumedicine.com/docs/ad-psychiatry-workfiles/cart_online-final_042012.pdf (accessed on 14 September 2020).
- Johns Hopkins University. COPEWELL Self-Assessment Tools. COPEWELL. 2020. Available online: https://www.copewellmodel.org/self-assessment-tools.html (accessed on 13 September 2020).
- Visible Network Labs. PARTNER: Program to Analyze, Record, and Track Networks to Enhance Relationships. 2010. Available online: https://visiblenetworklabs.com/partner-platform/ (accessed on 28 July 2020).
- Chandra, A.; Charles, A.; Hung, P.; Lopez, A.; Magana, A.; Rodriguez, Y.; Williams, M. Resilience Builder: Tools for Strengthening Disaster Resilience in Your Community; Los Angeles County Department of Public Health: Los Angeles, CA, USA, 2015; p. 148. Available online: http://www.laresilience.org/documents/resilience-builder.pdf (accessed on 14 September 2020).
- Tools | U.S. Climate Resilience Toolkit. 2020. Available online: https://toolkit.climate.gov/tools (accessed on 13 September 2020).
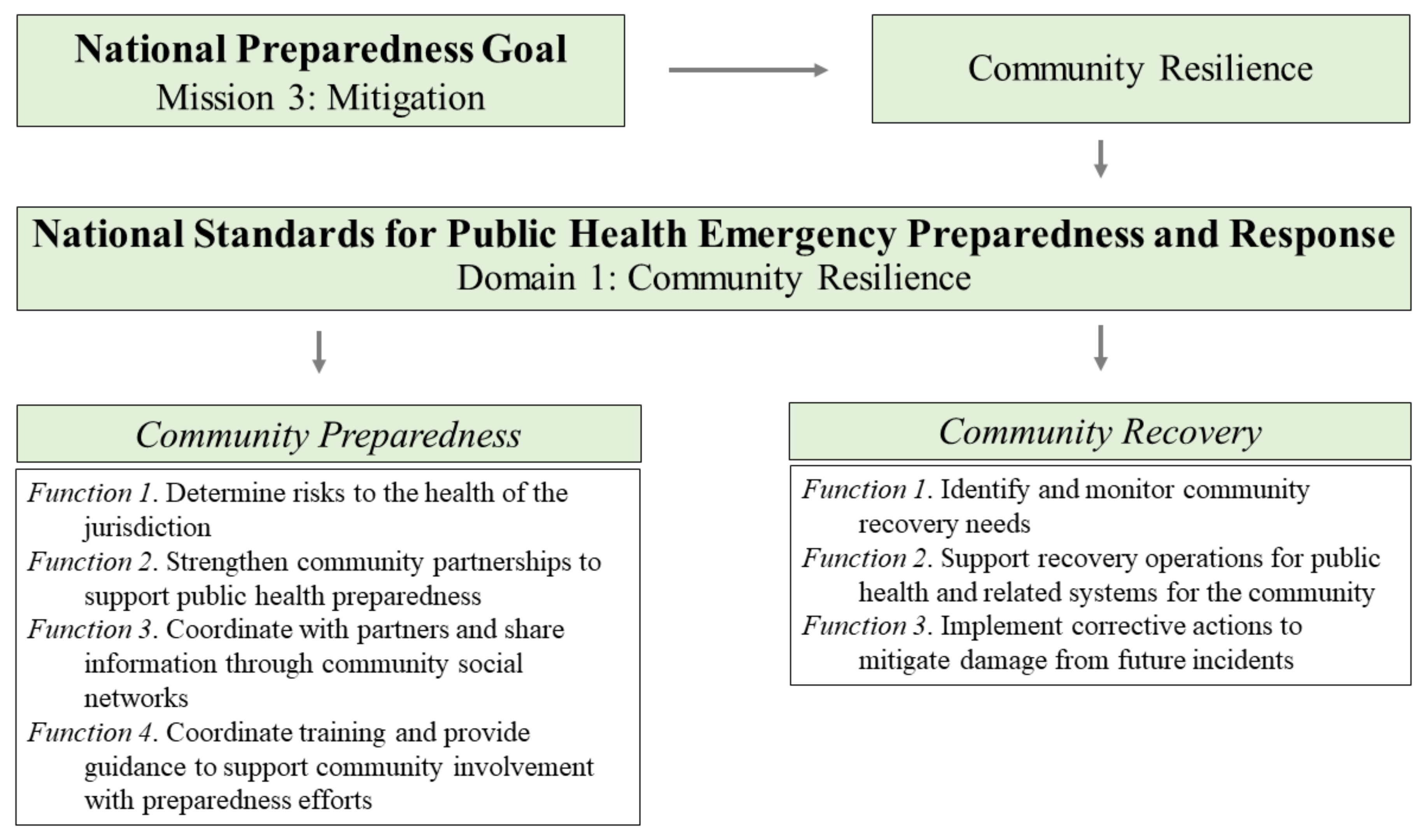
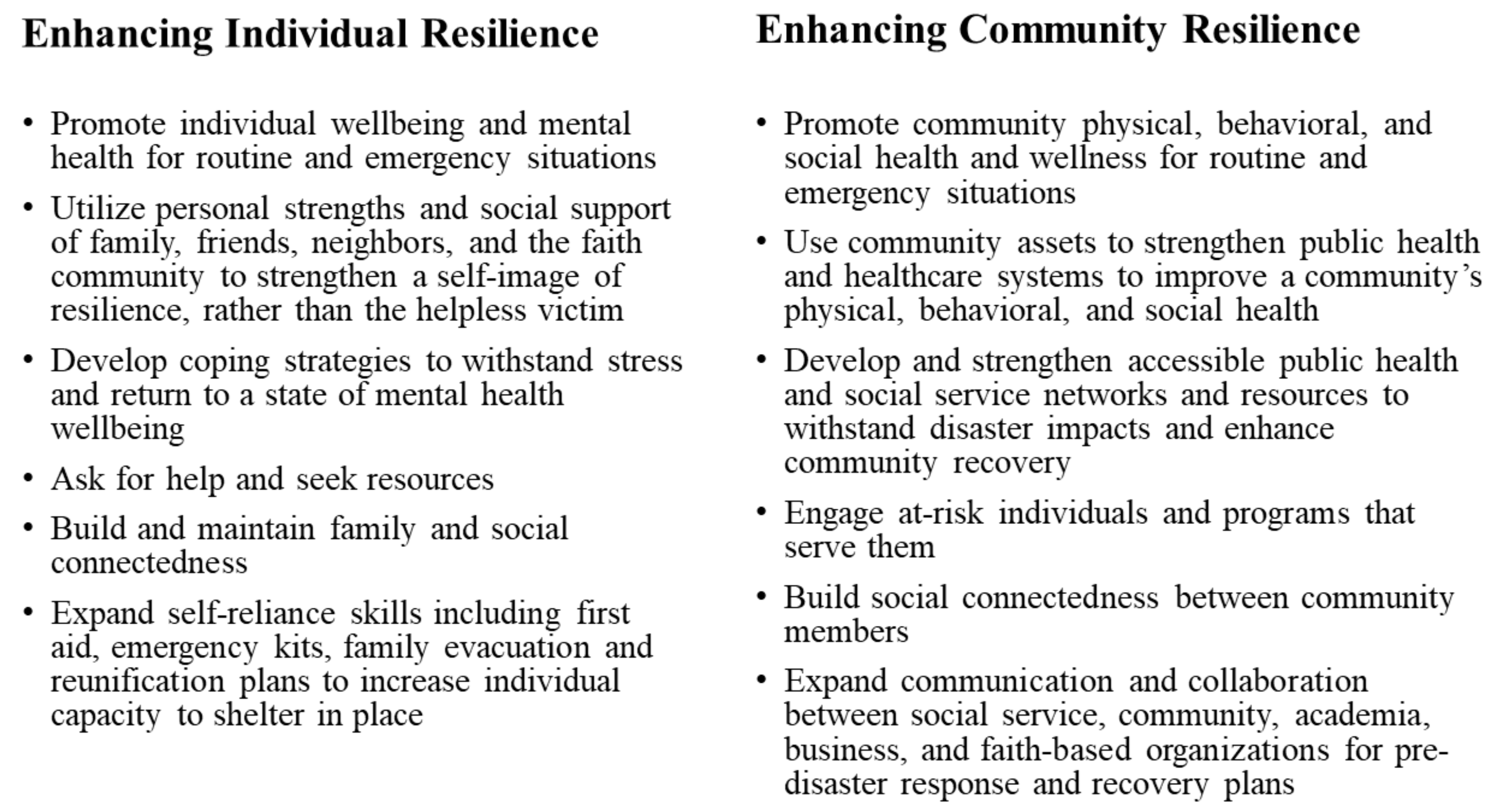
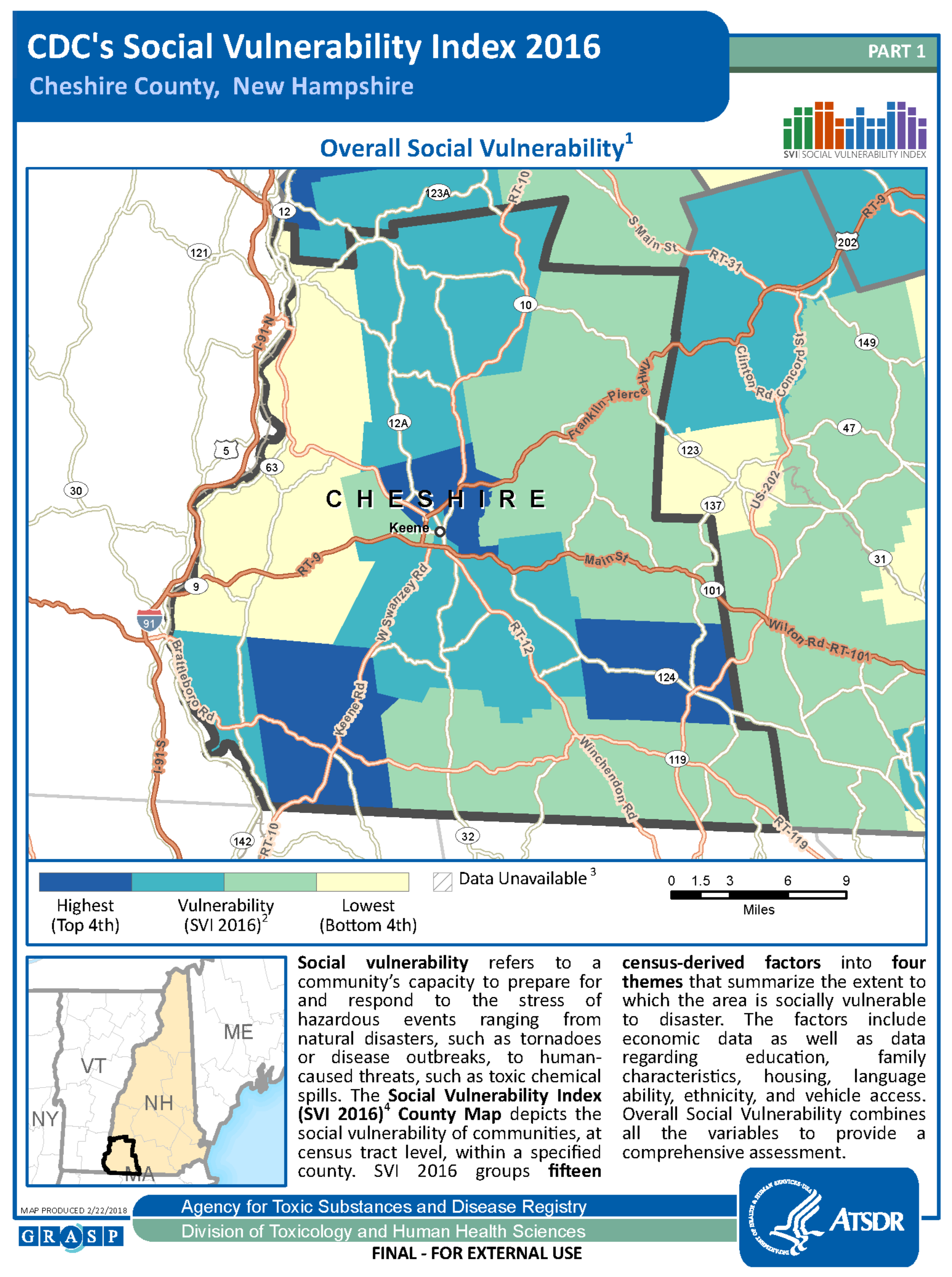
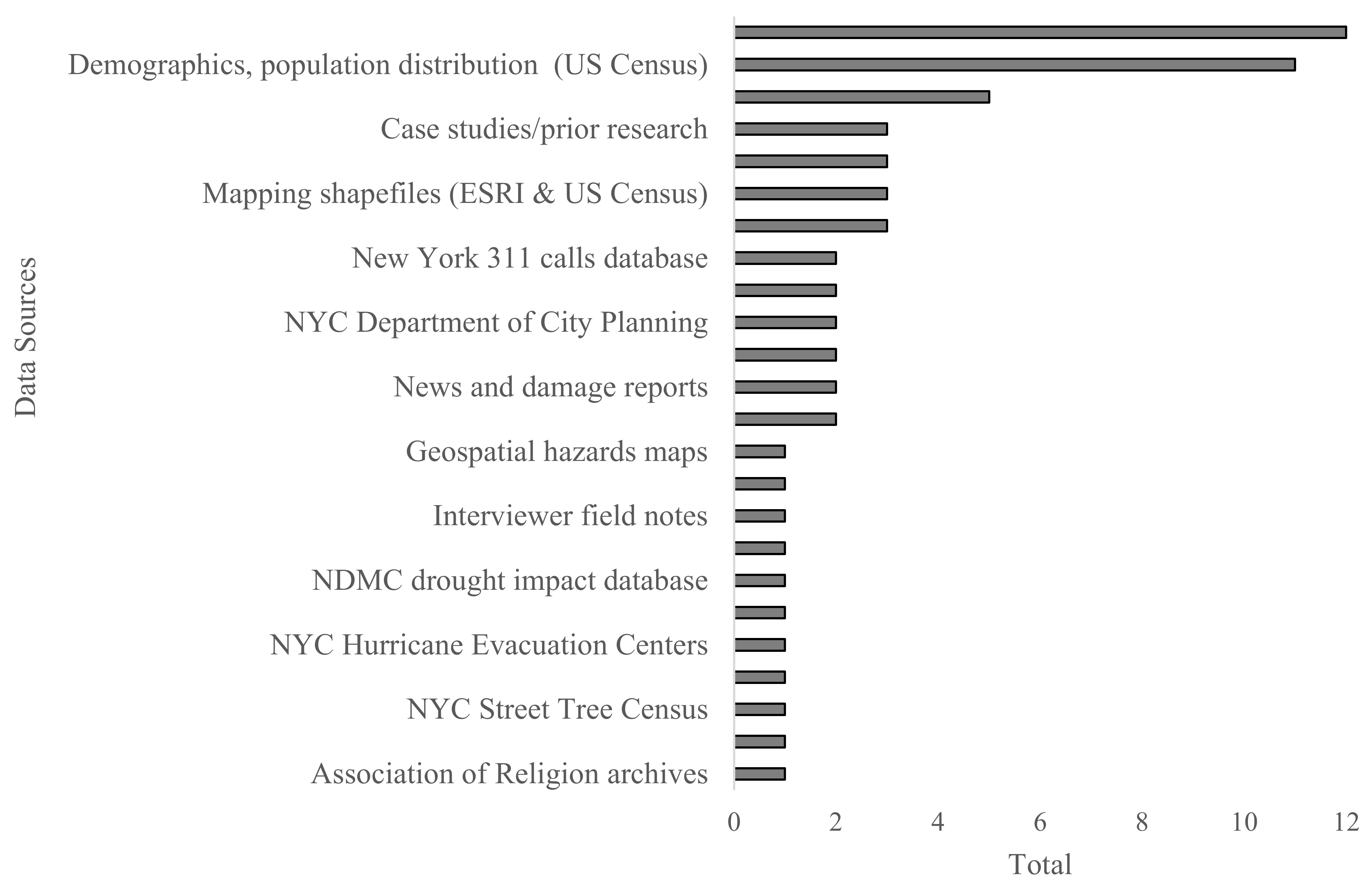
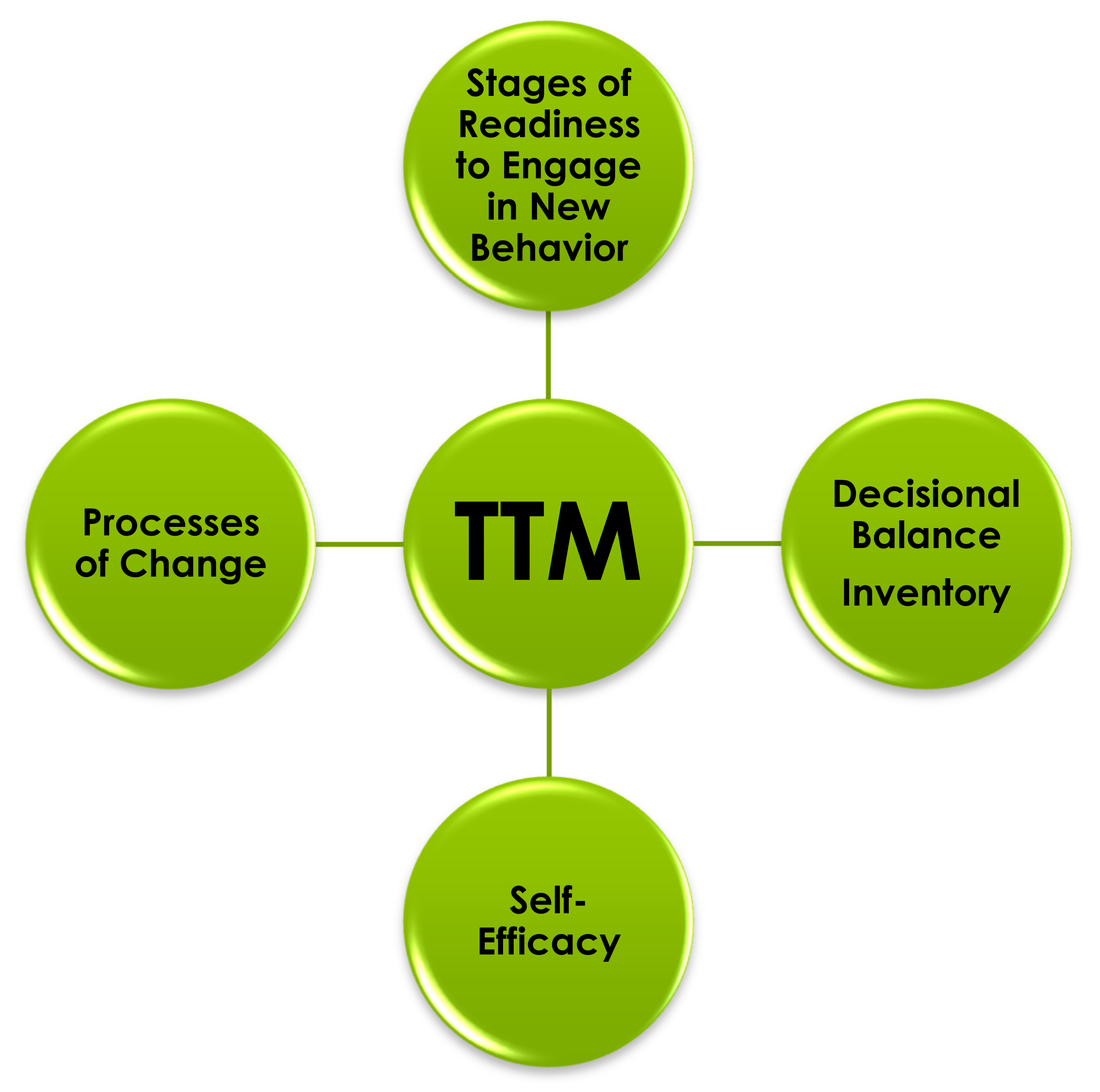
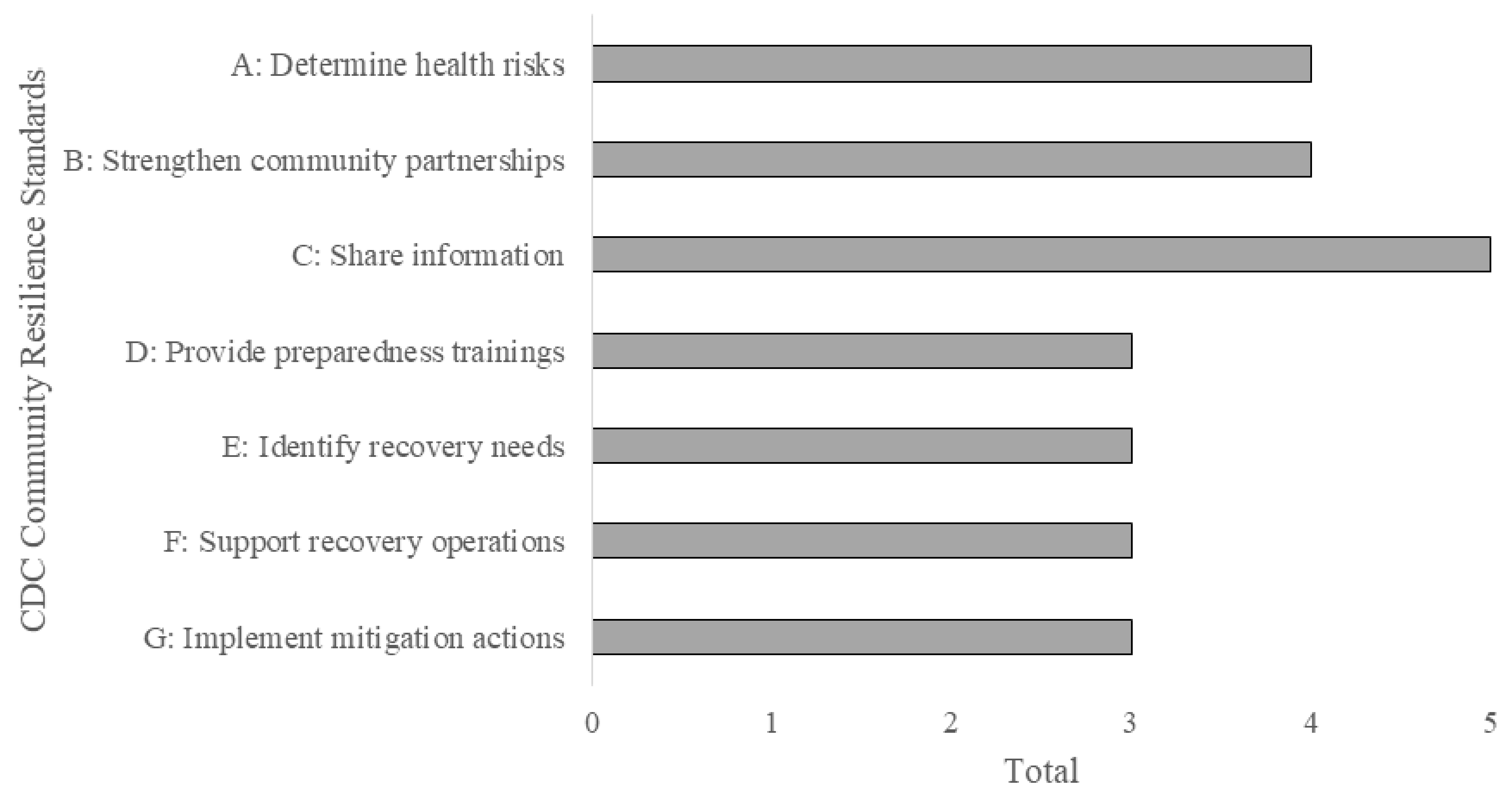
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).