
Could Assistive Technology Provision Models Help Pave the Way for More Environmentally Sustainable Models of Product Design, Manufacture and Service in a Post-COVID World?

 , , and
, , and 
{kind=link}
Abstract
1. Introduction
2. Aims of This Paper
3. Methods and Content
- Section 4.
- The Relationship between Disability Inclusion and Environmental Sustainability.
- Section 5.
- Circular Model of AT Provision.
- Section 6.
- Potential Opportunities in a Systems Approach to Local Production of AT.
- Section 7.
- Innovation Opportunity Areas that Could Allow Increased and Sustainable AT Provision:
- Section 7.1.
- Potential of Digital Fabrication;
- Section 7.2.
- Repair of AT;
- Section 7.3.
- Reuse Strategies;
- Section 7.4.
- Material Efficiency and Recovery from AT.
- Section 8.
- Conclusion:
- Section 8.1.
- What needs to be done;
- Section 8.2.
- Concluding Summary and Final Remarks.
4. The Relationship between Disability Inclusion and Environmental Sustainability
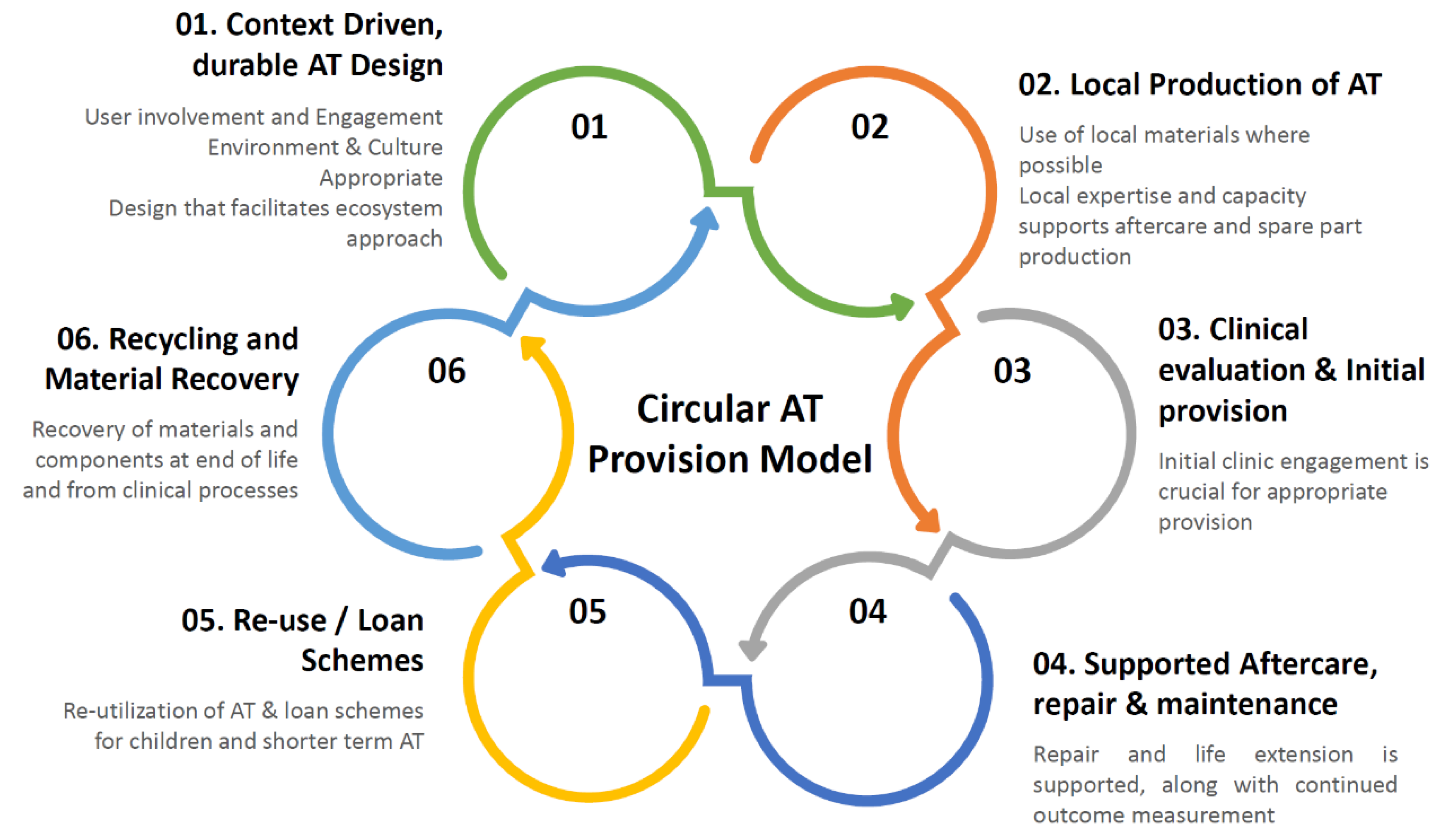
5. Circular Models of AT Provision
6. Potential Opportunities in a Systems Approach to Local Production of AT
AT2030 Case Study: Wazi
The Ugandan company, Wazi, are being supported through the AT Impact Fund. Wazi have a specific goal of localising eyeglasses frame production within Uganda as currently there is a complete lack of regional manufacture, and all components are imported, mostly from China. These imports come with high taxation and customs duties, as eyeglasses are deemed to be luxury items, increasing the price of these ATs that are a requirement for nearly 2 million people per year in Uganda. This includes both adults and children and takes into account the spectacle replacement rate for different groups.
A lack of local production also means a lack of local design, and for eyeglasses, aesthetic is of high importance, no matter the income setting–it has a significant influence on the stigma associated with visually impairment, which carries more connotations in low resource settings compared to high for various social reasons. It is also important to keep in mind that eyeglasses are a medical device and once frames have the prescription lenses glazed in them, not only does the perceived benefit for them increase, they have the potential to increase someone’s productivity and quality of life over a life course [45]. Such small batch, local manufacture is not specific to LMICs, Cubitts in the UK manage this eyeglass manufacturing model while residing in central London where property prices are some of the highest in the world.
7. Innovation Opportunity Areas That Could Allow Increased and Sustainable AT Provision
7.1. Potential of Digital Fabrication
7.2. Repair of AT
7.3. Reuse Strategies
7.4. Material Efficiency and Recovery from AT
AT2030 Case Study: Amparo
Frequent socket replacement is especially common in the earliest stages of becoming a prosthesis wearer, as the residual limb shrinks and stabilises over the first few years of prosthesis wear [105]. Prosthetic service delivery models, therefore, need to be set up for the initial prescription process, and the continued needs of maintenance and adaption. In LMICs, scarce resources, limited-service delivery locations and a lack of trained experts make the delivery and continued maintenance of prosthetics challenging.
Amparo’s leading innovation is a mouldable prosthetic socket which prosthetists can reshape multiple times to fit a wearer’s residual limbs as they naturally change shape. Additionally, the socket is not fitted using the traditional plaster-casting method, it uses a novel direct to limb vacuum moulding technique.
While addressing the user requirements was primary for the Amparo team, the potential for increased environmental sustainability through better material efficiency is significant for the approach they have taken. Not only does their fitting process remove the material usage during the plaster casting process and prototyping, but the continued reshapability means the same socket replaces multiple discarded sockets over the first few years of a user’s journey through rehabilitation. There is also a high degree of reduction in overall machinery requirements meaning less footprint associated with upkeep and eventual replacement.
8. Conclusions
8.1. What Needs to Be Done?
8.2. Concluding Summary and Final Remarks
- People with disabilities are particularly vulnerable to the negative effects of climate change, which will also likely exacerbate the difficulties of AT provision globally.
- Localised models of AT production could increase user and context specific AT innovations, while concurrently enabling circular approaches that reduce their environmental impact as well as bringing economic benefit to local communities.
- Localised models of AT could enable the potential of much needed service aspects of AT provision such as reuse and repair-increasing stable, reliable access to devices, and prolonging the useful life of products, and reduce the environmental impact of AT.
- AT needs to be designed with end of life in mind, this means designing for a system where the materials and components can easily be recovered and recirculated to the local points of production.
- Resilient, stable, and importantly equitable access to AT are an imperative and will become more so as climate change intensifies. The circular approaches we have outlined in this paper are the foundation of a systems approach to reducing the impact of climate change while increasing AT provision.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organisation. Assistive Technology. Available online: https://www.who.int/news-room/fact-sheets/detail/assistive-technology (accessed on 6 September 2021).
- Rohwerder, B. Assistive Technologies in Developing Countries; Institute of Development Studies: Brighton, UK, 2018. [Google Scholar]
- Bringezu, S.; Arden Clarke, C.; Fischer-Kowalski, M.; Graedel, T.; Hajer, M.; Hashimoto, S.; Hatfield-Dodds, S.; Havlik, P.; Hertwich, E.; Ingram, J.; et al. Resource Efficiency: Potential and Economic Implications, A Report by the International Resource Panel Report; International Resource Panel: Paris, France, 2017; ISBN 9789280736458. [Google Scholar]
- Kejariwal, R.; Kobayashi, E.; Savage, M.; Seghers, F.; Bhosa, T. Product Narrative: Hearing Aids, AT2030 Programme & ATscale Global Partnership for Assistive Technology. 2019. Available online: https://at2030.org/pn-hearing-aids/ (accessed on 15 July 2021).
- Chaudron, M.; Savage, M.; Seghers, F. Product Narrative: Eyeglasses, AT2030 Programme & ATscale Global Partnership for Assistive Technology. 2020. Available online: https://at2030.org/pn-eyeglasses/ (accessed on 15 July 2021).
- Vieira, C.M.; Franco, O.H.; Restrepo, C.G.; Abel, T. COVID-19: The Forgotten Priorities of the Pandemic. Maturitas 2020, 136, 38–41. [Google Scholar] [CrossRef]
- Smith, E.M.; Toro Hernandez, M.L.; Ebuenyi, I.D.; Syurina, E.V.; Barbareschi, G.; Best, K.L.; Danemayer, J.; Oldfrey, B.; Ibrahim, N.; Holloway, C.; et al. Assistive Technology Use and Provision During COVID-19: Results From a Rapid Global Survey. Int. J. Health Policy Manag. 2020, 2020, 1–10. [Google Scholar] [CrossRef]
- Ebuenyi, I.D.; Smith, E.M.; Holloway, C.; Jensen, R.; D’Arino, L.; MacLachlan, M. COVID-19 as Social Disability: The Opportunity of Social Empathy for Empowerment. BMJ Glob. Health 2020, 5, 3039. [Google Scholar] [CrossRef]
- Tebbutt, E.; Brodmann, R.; Borg, J.; MacLachlan, M.; Khasnabis, C.; Horvath, R. Assistive Products and the Sustainable Development Goals (SDGs). Glob. Health 2016, 12, 79. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, M.; Griggs, D.; Visbeck, M. Policy: Map the Interactions Between Sustainable Development Goals. Nature 2016, 534, 320–322. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Report on Disability. 2011. Available online: https://apps.who.int/iris/handle/10665/44575 (accessed on 25 September 2021).
- Ito, A. Crises, Conflict and Disability: Ensuring Equality; Routledge: Abingdon, UK, 2015; ISBN 9781138960305. [Google Scholar]
- Khavul, S.; Bruton, G.D. Harnessing Innovation for Change: Sustainability and Poverty in Developing Countries. J. Manag. Stud. 2013, 50, 285–306. [Google Scholar] [CrossRef]
- Karlan, D.; Appel, J. More Than Good Intentions: Improving the Ways the World’s Poor Borrow, Save, Farm, Learn, And Stay Healthy; Plume: New York, NY, USA, 2012; ISBN 9780452297562. [Google Scholar]
- Danemayer, J.; Boggs, D.; Smith, E.M.; Delgado Ramos, V.; Battistella, L.; Polack, S.; Holloway, C. Indicating Assistive Technology Supply & Demand. Assist. Technol. J. Rehabil. Eng. Assist. Technol. Soc. N. Am. (pending publication).
- Albala, S.; Holloway, C.; Austin, V.; Kattel, R. New Economics of Assistive Technology: A Call for a Missions Approach. Available online: https://www.ucl.ac.uk/bartlett/public-purpose/publications/working-papers (accessed on 9 July 2021).
- Liao, C.; Seghers, F.; Savage, M. Product Narrative: Prostheses, AT2030 Programme & ATscale Global Partnership for Assistive Technology. 2020. Available online: https://at2030.org/pn-prostheses/ (accessed on 16 July 2021).
- Mörchen, M.; Ocasiones, E.; Relator, R.; Lewis, D. Climate Change, Vulnerability, and Disability: Do We “Leave No One Behind”? Disaster Med. Public Health Prep. 2020, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Wolbring, G.; Leopatra, V. Climate Change, Water, Sanitation and Energy Insecurity: Invisibility of People with Disabilities. Can. J. Disabil. Stud. 2012, 1, 66. [Google Scholar] [CrossRef]
- Gaskin, C.J.; Taylor, D.; Kinnear, S.; Mann, J.; Hillman, W.; Moran, M. Factors Associated with the Climate Change Vulnerability and the Adaptive Capacity of People with Disability: A Systematic Review. Weather Clim. Soc. 2017, 9, 801–814. [Google Scholar] [CrossRef]
- Wolbring, G. A Culture of Neglect: Climate Discourse and Disabled People. Media Cult. J. 2009, 12. [Google Scholar] [CrossRef]
- Fenney Salkeld, D. Sustainable Lifestyles for All? Disability Equality, Sustainability and the Limitations of Current UK Policy. Disabil. Soc. 2016, 31, 447–464. [Google Scholar] [CrossRef]
- Abbott, D.; Porter, S. Environmental Hazard and Disabled People: From Vulnerable to Expert to Interconnected. Disabil. Soc. 2013, 28, 839–852. [Google Scholar] [CrossRef]
- Bell, S.L.; Tabe, T.; Bell, S. Seeking a Disability Lens within Climate Change Migration Discourses, Policies and Practices. Disabil. Soc. 2020, 35, 682–687. [Google Scholar] [CrossRef]
- Pertiwi, P.; Llewellyn, G.; Villeneuve, M. People with Disabilities as Key Actors in Community-based Disaster Risk Reduction. Disabil. Soc. 2019, 34, 1419–1444. [Google Scholar] [CrossRef]
- Otto, I.M.; Reckien, D.; Reyer, C.P.O.; Marcus, R.; Le Masson, V.; Jones, L.; Norton, A.; Serdeczny, O. Social Vulnerability to Climate Change: A Review of Concepts and Evidence. Reg. Environ. Chang. 2017, 17, 1651–1662. [Google Scholar] [CrossRef]
- Biyanwila, J. Poverty and disability in the Global South. Third World Q. 2011, 32, 1537–1540. [Google Scholar] [CrossRef]
- Groce, N.; Kett, M.; Lang, R.; Trani, J.F. Disability and Poverty: The Need for a More Nuanced Understanding of Implications for Development Policy and Practice. Third World Q. 2011, 32, 1493–1513. [Google Scholar] [CrossRef]
- Priestley, M.; Hemingway, L. Disability and Disaster Recovery: A Tale of Two Cities? J. Soc. Work Disabil. Rehabil. 2006, 5, 23–42. [Google Scholar] [CrossRef]
- Neumayer, E. Weak Versus Strong Sustainability: Exploring the Limits of Two Opposing Paradigms, 3rd ed.; Edward Elgar: Cheltenham, UK, 2010; ISBN 9781849805438. [Google Scholar]
- Agyeman, J.; Evans, T. Toward Just Sustainability in Urban Communities: Building Equity Rights with Sustainable Solutions. Ann. Am. Acad. Pol. Soc. Sci. 2003, 590, 35–53. [Google Scholar] [CrossRef]
- Agyeman, J. Toward a ‘Just’ Sustainability? Continuum 2008, 22, 751–756. [Google Scholar] [CrossRef]
- Agyeman, J.; Bullard, R.D.; Evans, B. Just Sustainabilities: Development in an Unequal World; MIT Press: Cambridge, MA, USA, 2003; Volume 29, ISBN 9780262511315. [Google Scholar]
- Fritz, M.; Koch, M. Potentials for Prosperity Without Growth: Ecological Sustainability, Social Inclusion and the Quality of Life in 38 Countries. Ecol. Econ. 2014, 108, 191–199. [Google Scholar] [CrossRef]
- European Commission. EUR-Lex—52015DC0614—EN—EUR-Lex. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX%3A52015DC0614 (accessed on 14 July 2021).
- European Commission. Towards a Circular Economy: A Zero Waste Programme for Europe DG Environment. Available online: http://ec.europa.eu/europe2020/public- (accessed on 14 July 2021).
- European Commission. Development of Guidance on Extended Producer Responsibility (EPR) Final Report. Available online: https://ec.europa.eu/environment/archives/waste/eu_guidance/pdf/Guidance%20on%20EPR%20-%20Final%20Report.pdf (accessed on 25 September 2021).
- Pesce, M.; Tamai, I.; Guo, D.; Critto, A.; Brombal, D.; Wang, X.; Cheng, H.; Marcomini, A. Circular Economy in China: Translating Principles into Practice. Sustainability 2020, 12, 832. [Google Scholar] [CrossRef]
- Ellen Macarthur Foundation. Towards the Circular Economy: Economic and Business Rationale for an Accelerated Transition. Available online: https://ellenmacarthurfoundation.org/towards-the-circular-economy-vol-1-an-economic-and-business-rationale-for-an (accessed on 11 July 2021).
- Patwa, N.; Sivarajah, U.; Seetharaman, A.; Sarkar, S.; Maiti, K.; Hingorani, K. Towards a Circular Economy: An Emerging Economies Context. J. Bus. Res. 2021, 122, 725–735. [Google Scholar] [CrossRef]
- Fehrer, J.A.; Wieland, H. A Systemic Logic for Circular Business Models. J. Bus. Res. 2021, 125, 609–620. [Google Scholar] [CrossRef]
- MacLachlan, M.; Scherer, M.J. Systems Thinking for Assistive Technology: A Commentary on the GREAT Summit. Disabil. Rehabil. Assist. Technol. 2018, 13, 492–496. [Google Scholar] [CrossRef]
- Matter, R.; Harniss, M.; Oderud, T.; Borg, J.; Eide, A.H. Assistive Technology in Resource-Limited Environments: A Scoping Review. Disabil. Rehabil. Assist. Technol. 2017, 12, 105–114. [Google Scholar] [CrossRef] [PubMed]
- McSweeney, E.; Gowran, R.J. Wheelchair Service Provision Education and Training in Low and Lower Middle Income Countries: A Scoping Review. Disabil. Rehabil. Assist. Technol. 2019, 14, 33–45. [Google Scholar] [CrossRef]
- Burton, M.J.; Ramke, J.; Marques, A.P.; Bourne, R.R.A.; Congdon, N.; Jones, I.; Ah Tong, B.A.M.; Arunga, S.; Bachani, D.; Bascaran, C.; et al. The Lancet Global Health Commission on Global Eye Health: Vision Beyond 2020. Lancet Glob. Health 2021, 9, e489–e551. [Google Scholar] [CrossRef]
- Steele, K.; Steele, K.; Blaser, B.; Cakmak, M. Accessible Making: Designing Makerspaces for Accessibility. Int. J. Des. Learn. 2018, 9, 114–121. [Google Scholar] [CrossRef]
- Prendeville, S.; Hartung, G.; Brass, C.; Purvis, E.; Hall, A. Circular Makerspaces: The Founder’s View. Int. J. Sustain. Eng. 2017, 10, 272–288. [Google Scholar] [CrossRef]
- Prendeville, S.; Hartung, G.; Purvis, E.; Brass, C.; Hall, A. Makespaces: From Redistributed Manufacturing to a Circular Economy. In Proceedings of the International Conference on Sustainable Design and Manufacturing, Heraklion, Greece, 4–6 April 2016; Volume 52, pp. 577–588. [Google Scholar]
- Distributed Manufacturing in Humanitarian Logistics Operations. Emerald Publishing. Available online: https://www.emeraldgrouppublishing.com/archived/products/journals/call_for_papers.htm%3Fid%3D8083 (accessed on 15 July 2021).
- Corsini, L.; Aranda-Jan, C.B.; Moultrie, J. The Impact of 3D Printing on the Humanitarian Supply Chain. Prod. Plan. Control 2020, 1–13. [Google Scholar] [CrossRef]
- James, L. Opportunities and Challenges of Distributed Manufacturing for Humanitarian Response. In Proceedings of the GHTC 2017—IEEE Global Humanitarian Technology Conference, San Jose, CA, USA, 19–22 October 2017; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA, 2017; Volume 2017, pp. 1–9. [Google Scholar]
- Innovation Action. Available online: https://www.innovationaction.org/ (accessed on 15 July 2021).
- Open Know-Where. Available online: https://www.internetofproduction.org/open-know-where (accessed on 15 July 2021).
- Smith, R.O.; Scherer, M.J.; Cooper, R.; Bell, D.; Hobbs, D.A.; Pettersson, C.; Seymour, N.; Borg, J.; Johnson, M.J.; Lane, J.P.; et al. Assistive Technology Products: A Position Paper from the First Global Research, Innovation, and Education on Assistive Technology (GREAT) Summit. Disabil. Rehabil. Assist. Technol. 2018, 13, 473–485. [Google Scholar] [CrossRef] [PubMed]
- Scherer, M.J. Technology Adoption, Acceptance, Satisfaction and Benefit: Integrating Various Assistive Technology Outcomes. Disabil. Rehabil. Assist. Technol. 2017, 12, 1–2. [Google Scholar] [CrossRef][Green Version]
- Scherer, M.J.; Craddock, G. Matching Person & Technology (MPT) Assessment Process. Technol. Disabil. 2002, 14, 125–131. [Google Scholar] [CrossRef]
- Visagie, S.; Mlambo, T.; Van der Veen, J.; Nhunzvi, C.; Tigere, D.; Scheffler, E. Is Any Wheelchair Better than No Wheelchair? A Zimbabwean perspective. Afr. J. Disabil. 2015, 4, 1–10. [Google Scholar] [CrossRef]
- Jefferds, A.N.; Pearlman, J.L.; Wee, J.; Cooper, R.A. International Mobility Technology Research: A Delphi Study to Identify Challenges and Compensatory Strategies. Assist. Technol. 2011, 23, 232–242. [Google Scholar] [CrossRef]
- Pearlman, J.; Cooper, R.A.; Zipfel, E.; Cooper, R.; McCartney, M. Towards the Development of an Effective Technology Transfer Model of Wheelchairs to Developing Countries. Disabil. Rehabil. Assist. Technol. 2006, 1, 103–110. [Google Scholar] [CrossRef]
- Tecchio, P.; McAlister, C.; Mathieux, F.; Ardente, F. In Search of Standards to Support Circularity in Product Policies: A Systematic Approach. J. Clean. Prod. 2017, 168, 1533–1546. [Google Scholar] [CrossRef]
- Mesa, J.; González-Quiroga, A.; Maury, H. Developing an Indicator for Material Selection Based on Durability and Environmental Footprint: A Circular Economy Perspective. Resour. Conserv. Recycl. 2020, 160, 104887. [Google Scholar] [CrossRef]
- Corona, B.; Shen, L.; Reike, D.; Carreón, J.R.; Worrell, E. Towards Sustainable Development through the Circular Economy—A Review and Critical Assessment on Current Circularity Metrics. Resour. Conserv. Recycl. 2019, 151, 104498. [Google Scholar] [CrossRef]
- Hurst, A.; Kane, S. Making “Making” Accessible. In Proceedings of the 12th International Conference on Interaction Design and Children, New York, NY, USA, 24–27 June 2013. [Google Scholar]
- Thorsen, R.; Bortot, F.; Caracciolo, A. From Patient to Maker—A Case Study of Co-Designing an Assistive Device using 3D Printing. Assist. Technol. 2019, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Barbareschi, G.; Holloway, C.S.M.; Sprigle, S. Assistive Technology Design Courses: The Mutually Beneficial Relationship between Engineering Education and the Provision of Orphan Devices; Rehabilitation Engineering and Assistive Technology Society of North America (RESNA): Rosslyn, VA, USA, 2017. [Google Scholar]
- Seelman, K.D. Universal Design and Orphan Technology: Do We Need Both? Disabil. Stud. Q. 2005, 25. [Google Scholar] [CrossRef]
- Barbareschi, G.; Daymond, S.; Honeywill, J.; Singh, A.; Noble, D.; Mbugua, N.N.; Harris, I.; Austin, V.; Holloway, C. Value Beyond Function: Analyzing the Perception of Wheelchair Innovations in Kenya. In Proceedings of the ASSETS 2020—22nd International ACM SIGACCESS Conference on Computers and Accessibility, Athens, Greece, 26–28 October 2020; Association for Computing Machinery, Inc.: New York, NY, USA, 2020. [Google Scholar]
- Alifui-Segbaya, F.; George, R. Biocompatibility of 3d-Printed Methacrylate for Hearing Devices. Inventions 2018, 3, 52. [Google Scholar] [CrossRef]
- Ayyildiz, O. Customised Spectacles Using 3-D Printing Technology. Clin. Exp. Optom. 2018, 101, 747–751. [Google Scholar] [CrossRef]
- Lee, L.; Burnett, A.M.; Panos, J.G.; Paudel, P.; Keys, D.; Ansari, H.M.; Yu, M. 3-D Printed Spectacles: Potential, Challenges and the Future. Clin. Exp. Optom. 2020, 103, 590–596. [Google Scholar] [CrossRef]
- Altinkurt, E.; Ceylan, N.A.; Altunoglu, U.; Turgut, G.T. Manufacture of Custom-Made Spectacles using Three-Dimensional Printing Technology. Clin. Exp. Optom. 2020, 103, 902–904. [Google Scholar] [CrossRef]
- Brodie, F.L.; Nattagh, K.; Shah, V.; Swarnakar, V.; Lin, S.; Kelil, T.; Gillan, D.; Romero, D.; de Alba Campomanes, A.G. Computed Tomography–Based 3D Modeling to Provide Custom 3D-Printed Glasses for Children with Craniofacial Abnormalities. J. AAPOS 2019, 23, 165–167.e1. [Google Scholar] [CrossRef]
- Novel Use of iPhone Based 3D Face Scanning to Develop Custom 3D Printed Spectacles For Children With Craniofacial Malformations | IOVS | ARVO Journals. Available online: https://iovs.arvojournals.org/article.aspx?articleid=2767376 (accessed on 11 July 2021).
- Koprnicky, J.; Šafka, J.; Ackermann, M. Using of 3D Printing Technology in Low Cost Prosthetics. Mater. Sci. Forum 2018, 919, 199–206. [Google Scholar] [CrossRef]
- Pourfarzaneh, A.; Taghavi, M.; Helps, T.; Rossiter, J. Towards Adaptive Prosthetic Sockets using 3d-Printed Variable-Stiffness Shape-Memory Structures. In Proceedings of the RoboSoft 2019—2019 IEEE International Conference on Soft Robotics, Seoul, Korea, 14–18 April 2019; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA, 2019; pp. 410–415. [Google Scholar]
- Banga, H.K.; Kumar, P.; Kumar, H. Utilization of Additive Manufacturing in Orthotics and Prosthetic Devices Development. In Proceedings of the IOP Conference Series: Materials Science and Engineering, Chandigarh, India, 28–30 August 2020; IOP Publishing Ltd.: Chandigarh, India, 2021; Volume 1033, p. 012083. [Google Scholar]
- Chae, D.S.; Kim, D.H.; Kang, K.Y.; Kim, D.Y.; Park, S.W.; Park, S.J.; Kim, J.H. The Functional Effect of 3D-Printing Individualized Orthosis for Patients with Peripheral Nerve Injuries: Three Case Reports. Medicine 2020, 99, e19791. [Google Scholar] [CrossRef]
- Zhong, S.; Pearce, J.M. Tightening the Loop on the Circular Economy: Coupled Distributed Recycling and Manufacturing with Recyclebot and RepRap 3-D Printing. Resour. Conserv. Recycl. 2018, 128, 48–58. [Google Scholar] [CrossRef]
- Sun, L.; Wang, Y.; Hua, G.; Cheng, T.C.E.; Dong, J. Virgin or Recycled? Optimal Pricing of 3D Printing Platform and Material Suppliers in a Closed-Loop Competitive Circular Supply Chain. Resour. Conserv. Recycl. 2020, 162, 105035. [Google Scholar] [CrossRef]
- DePalma, K.; Walluk, M.R.; Murtaugh, A.; Hilton, J.; McConky, S.; Hilton, B. Assessment of 3D Printing using Fused Deposition Modeling and Selective Laser Sintering for a Circular Economy. J. Clean. Prod. 2020, 264, 121567. [Google Scholar] [CrossRef]
- Garmulewicz, A.; Holweg, M.; Veldhuis, H.; Yang, A. Disruptive Technology as an Enabler of the Circular Economy: What Potential Does 3D Printing Hold? Calif. Manage. Rev. 2018, 60, 112–132. [Google Scholar] [CrossRef]
- Dickinson, A.; Donovan-Hall, M.; Kheng, S.; Wiegand, S.; Wills, G.; Ostler, C.; Srors, S.; Tech, A.; Granat, M.; Kenney, L.; et al. Technologies to Enhance Quality and Access to Prosthetics & Orthotics: The Importance of a Multidisciplinary, User-Centred Approach. Glob. Rep. Assist. Technol. Consult. 2019, 22–23. [Google Scholar] [CrossRef]
- Campbell, A.I.; Sexton, S.; Schaschke, C.J.; Kinsman, H.; McLaughlin, B.; Boyle, M. Prosthetic Limb Sockets from Plant-Based Composite Materials. Prosthet. Orthot. Int. 2012, 36, 181–189. [Google Scholar] [CrossRef]
- World Health Organization. WHO Standards for Prosthetics and Orthotics. Available online: http://apps.who.int/bookorders (accessed on 13 July 2021).
- Oldfrey, B.; Miodownik, M.; Barbareschi, G.; Williams, R.; Holloway, C. Digital Fabrication of Lower Limb Prosthetic Sockets. AT2030 Programme. Available online: https://at2030.org/digital-fabrication-of-lower-limb-prosthetic-sockets/ (accessed on 9 July 2021).
- Petrick, I.J.; Simpson, T.W. 3D Printing Disrupts Manufacturing: How Economies of One Create New Rules of Competition. Res. Manag. 2013, 56, 12–16. [Google Scholar] [CrossRef]
- Groom, R.C. Think global and Act Local. J. Extra. Corpor. Technol. 2012, 44, 177. [Google Scholar]
- Geddes, P. Cities in Evolution—An Introduction to the Town Planning Movement and to the Study of Civics; Williams & Norgate: London, UK, 1915. [Google Scholar]
- Buehler, E.; Branham, S.; Ali, A.; Chang, J.J.; Hofmann, M.K.; Hurst, A.; Kane, S.K. Sharing is Caring: Assistive Technology Designs on Thingiverse. In Proceedings of the 33rd Annual ACM Conference on Human Factors in Computing Systems, Seoul, Korea, 18–23 April 2015; ACM: New York, NY, USA, 2015. [Google Scholar]
- Open Assistive. Available online: https://openassistive.org/ (accessed on 13 July 2021).
- What We Want—Right to Repair Europe. Available online: https://repair.eu/what-we-want/ (accessed on 6 February 2021).
- Manzini, E.; Vezzoli, C.; Clark, G. Product-Service Systems. Using an Existing Concept as a New Approach to Sustainability. J. Des. Res. 2001, 1, 27–40. [Google Scholar] [CrossRef]
- Song, J.S.; Zhang, Y. Stock or Print? Impact of 3-d Printing on Spare Parts Logistics. Manag. Sci. 2020, 66, 3860–3878. [Google Scholar] [CrossRef]
- Kostidi, E.; Nikitakos, N. Is It Time for the Maritime Industry to Embrace 3d Printed Spare Parts? TransNav Int. J. Mar. Navig. Saf. Sea Transp. 2018, 12, 557–564. [Google Scholar] [CrossRef]
- Savastano, M.; Amendola, C.; D’Ascenzo, F.; Massaroni, E. 3-D Printing in the Spare Parts Supply Chain: An Explorative Study in the Automotive Iindustry. In Lecture Notes in Information Systems and Organisation; Springer: Berlin/Heidelberg, Germany, 2016; Volume 18, pp. 153–170. [Google Scholar]
- Kretzschmar, N.; Chekurov, S.; Salmi, M.; Tuomi, J. Evaluating the Readiness Level of Additively Manufactured Digital Spare Parts: An Industrial Perspective. Appl. Sci. 2018, 8, 1837. [Google Scholar] [CrossRef]
- Kirchherr, J.; Reike, D.; Hekkert, M. Conceptualizing the Circular Economy: An Analysis of 114 Definitions. Resour. Conserv. Recycl. 2017, 127, 221–232. [Google Scholar] [CrossRef]
- Adya, M.; Samant, D.; Scherer, M.J.; Killeen, M.; Morris, M.W. Assistive/Rehabilitation Technology, Disability, and Service Delivery Models. Cogn. Process. 2012, 13, 75–78. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, G.; Samanta, A. Wheelchair Charity: A Useless Benevolence in Community-Based Rehabilitation. Disabil. Rehabil. 2005, 27, 591–596. [Google Scholar] [CrossRef] [PubMed]
- Kniskern, J.; Phillips, C.P.; Patterson, T. Technology (AT) Reutilization (Reuse): What We Know Today. Assist. Technol. Outcomes Benefits 2008, 5, 59–71. [Google Scholar]
- Morgan, K.A.; Walker, C.; Walker, K. Assistive Technology Reutilization Program Outcomes—Wheel Mill System View project. In Proceedings of the 136st APHA Annual Meeting and Exposition, San Diego, CA, USA, 25–29 October 2008. [Google Scholar]
- Wilcox, M.J.; Campbell, P.H.; Fortunato, L.; Hoffman, J. A First Look at Early Intervention and Early Childhood Providers’ Reports of Assistive Technology Reuse. J. Spec. Educ. Technol. 2013, 28, 47–57. [Google Scholar] [CrossRef]
- Sund, T. The Norwegian Model of Assistive Technology Provision. Presentation at the Global Research, Innovation and Education on Assistive Technology (GREAT). In Proceedings of the GREAT Summit, Geneva, Switzerland, 3–4 August 2017. [Google Scholar]
- MacLachlan, M.; Banes, D.; Bell, D.; Borg, J.; Donnelly, B.; Fembek, M.; Ghosh, R.; Gowran, R.J.; Hannay, E.; Hiscock, D.; et al. Assistive Technology Policy: A Position Paper from the First Global Research, Innovation, and Education on Assistive Technology (GREAT) Summit. Disabil. Rehabil. Assist. Technol. 2018, 13, 454–466. [Google Scholar] [CrossRef]
- Sanders, J.E.; Fatone, S. Residual Limb Volume Change: Systematic Review of Measurement and Management. J. Rehabil. Res. Dev. 2011, 48, 949–986. [Google Scholar] [CrossRef]
- Williams, R.; Oldfrey, B.; Holloway, C. An AT Innovator Case Study: Amparo. Available online: https://at2030.org/an-at-innovator-case-study-amparo/ (accessed on 15 July 2021).
- Wyss, D.; Lindsay, S.; Cleghorn, W.L.; Andrysek, J. Priorities in Lower Limb Prosthetic Service Delivery Based on an International Survey of Prosthetists in Low- and High-Income Countries. Prosthet. Orthot. Int. 2015, 39, 102–111. [Google Scholar] [CrossRef]
- Vollmer, I.; Jenks, M.J.F.; Roelands, M.C.P.; White, R.J.; van Harmelen, T.; de Wild, P.; van der Laan, G.P.; Meirer, F.; Keurentjes, J.T.F.; Weckhuysen, B.M. Beyond Mechanical Recycling: Giving New Life to Plastic Waste. Angew. Chem. Int. Ed. 2020, 59, 15402–15423. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oldfrey, B.; Barbareschi, G.; Morjaria, P.; Giltsoff, T.; Massie, J.; Miodownik, M.; Holloway, C. Could Assistive Technology Provision Models Help Pave the Way for More Environmentally Sustainable Models of Product Design, Manufacture and Service in a Post-COVID World? Sustainability 2021, 13, 10867. https://doi.org/10.3390/su131910867
Oldfrey B, Barbareschi G, Morjaria P, Giltsoff T, Massie J, Miodownik M, Holloway C. Could Assistive Technology Provision Models Help Pave the Way for More Environmentally Sustainable Models of Product Design, Manufacture and Service in a Post-COVID World? Sustainability. 2021; 13(19):10867. https://doi.org/10.3390/su131910867
Chicago/Turabian StyleOldfrey, Ben, Giulia Barbareschi, Priya Morjaria, Tamara Giltsoff, Jessica Massie, Mark Miodownik, and Catherine Holloway. 2021. "Could Assistive Technology Provision Models Help Pave the Way for More Environmentally Sustainable Models of Product Design, Manufacture and Service in a Post-COVID World?" Sustainability 13, no. 19: 10867. https://doi.org/10.3390/su131910867
APA StyleOldfrey, B., Barbareschi, G., Morjaria, P., Giltsoff, T., Massie, J., Miodownik, M., & Holloway, C. (2021). Could Assistive Technology Provision Models Help Pave the Way for More Environmentally Sustainable Models of Product Design, Manufacture and Service in a Post-COVID World? Sustainability, 13(19), 10867. https://doi.org/10.3390/su131910867