
Gendered Factors Associated with Preventive Behaviors and Mental Health among Chinese Adults during the COVID-19 Pandemic Home Quarantine

 ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Measurements
2.3. Ethical Considerations
2.4. Statistical Analysis
3. Results
3.1. Descriptive Statistics
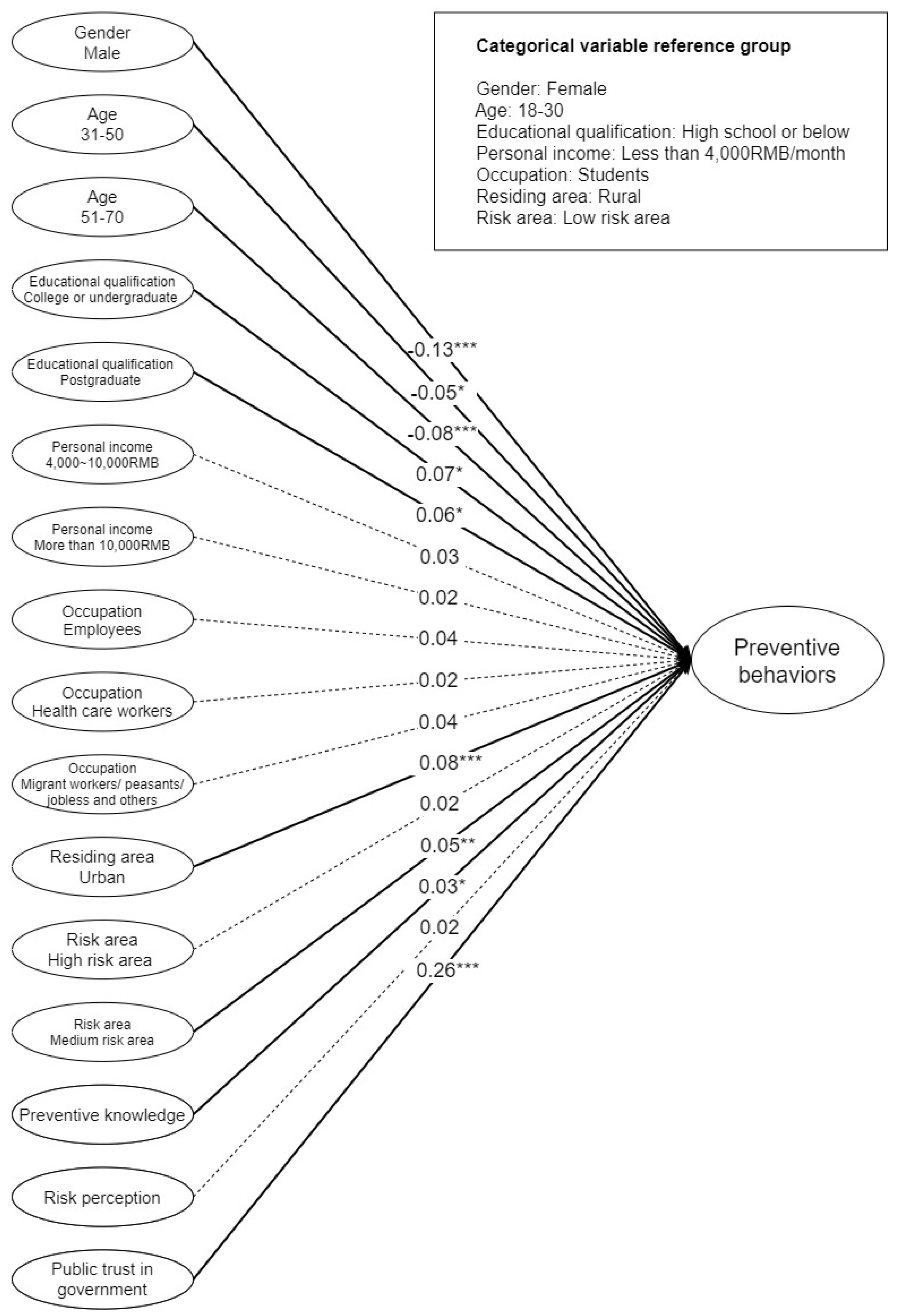
3.2. Factors Associated with Preventive Behaviors
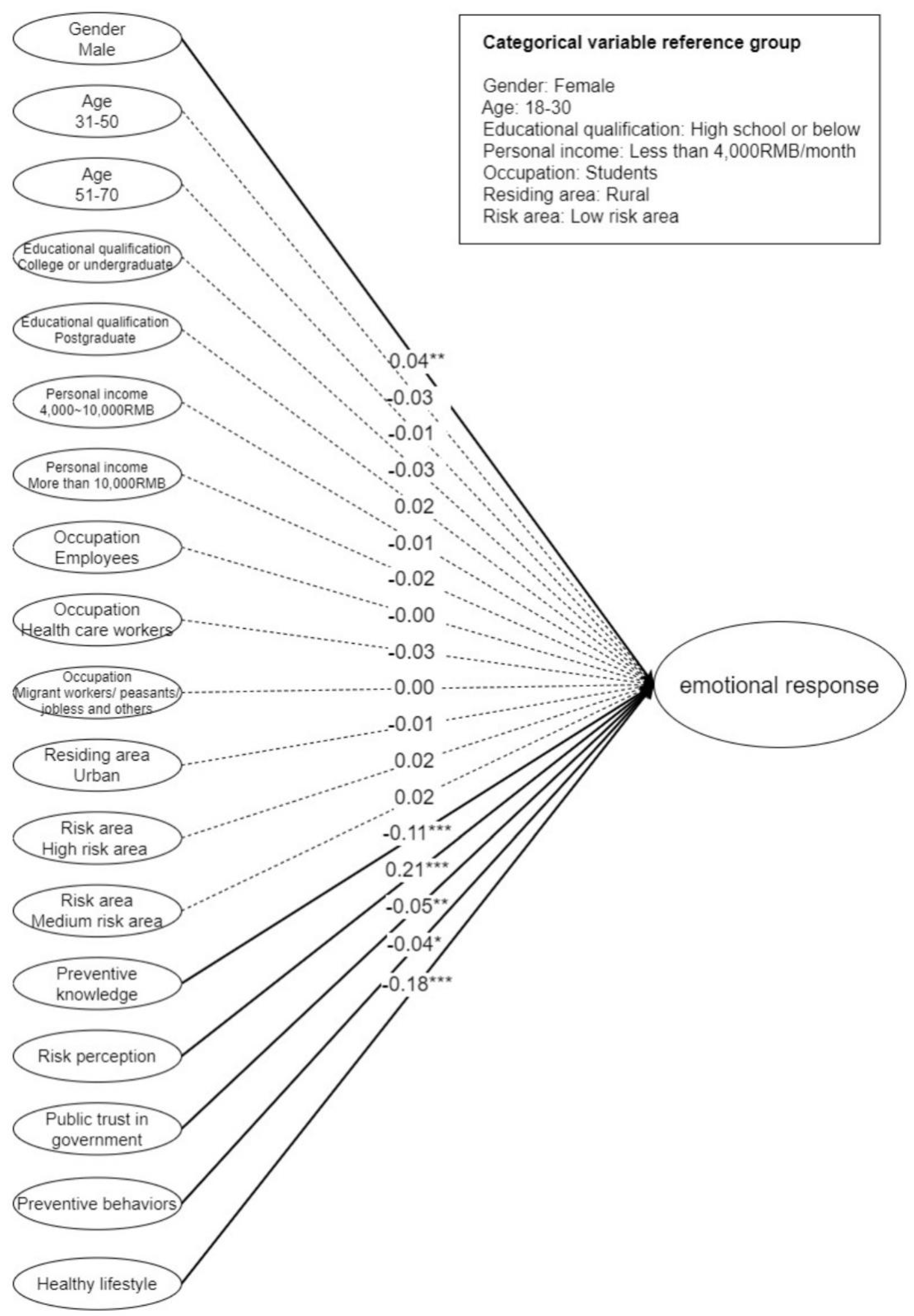
3.3. Factors Associated with Emotional Response to Home Quarantine
3.4. Factors Associated with Anxiety during the COVID-19 Outbreak
4. Discussion
4.1. Preventive Behaviors and Healthy Lifestyle during the Outbreak of COVID-19
4.2. Emotional Response to Home Quarantine and Anxiety during the COVID-19 Outbreak
4.3. The Role of Public Preventive Knowledge, Risk Perception, Trust in the Government’s Mitigation Measures to the COVID-19 Pandemic, and Healthy Lifestyle in Behavioral and Psychological Response
5. Limitations and Future Research
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix A.1. Survey Questionnaire No. 20200301VER2
| Project PI: Shu-Mei Liu |
| Jing Hengyi College of Education, Hangzhou Normal University |
| Project team member: Wei-Ta Fang |
| Graduate Institute of Environmental Education, NTNU |
- Gender: □Male □Female
- Age ______________
- Education qualification: □ High school or below □ College or undergraduate □ Postgraduate
- Personal income: □ Less than RMB 4000/month □ RMB 4000/month RMB ~10,000/month □ More than RMB 10,000/month
- Occupation: □ Student □ Employee □ Health care worker □ Migrant worker/peasant/jobless and other
- Do you reside in an urban or rural area? □ Urban □ Rural
- Place (Where you live): _____________ (City/town/village, Province)
| Please fill in the level of agreement to the best of your understanding of the following statements. | Yes (1) | No (2) | I don’t know (3) |
| □ | □ | □ |
| □ | □ | □ |
| □ | □ | □ |
| □ | □ | □ |
| Please fill in the level of agreement to the best of your understanding of the following statements. | Strongly disagree (1) | Disagree (2) | Slightly disagree (3) | Slightly Agree (4) | Agree (5) | Strongly agree (6) |
| (1) Do you think you may be infected with COVID-19? | □ | □ | □ | □ | □ | □ |
| (2) Do you think your family may be infected with COVID-19? | □ | □ | □ | □ | □ | □ |
| (3) Do you think people around you may be infected with COVID-19? | □ | □ | □ | □ | □ | □ |
| (4) The government’s policy on preventive measures against COVID-19 is credible. | □ | □ | □ | □ | □ | □ |
| (5) The government’s policy on preventive measures against COVID-19 is correct. | □ | □ | □ | □ | □ | □ |
| (6) The government should develop a long-term plan to address the problem of COVID-19. | □ | □ | □ | □ | □ | □ |
| (7) The government has the ability to resolve the problem of COVID-19. | □ | □ | □ | □ | □ | □ |
| (8) How did you feel when you were confined at home during the COVID-19 outbreak? | ||||||
| Boredom | □ | □ | □ | □ | □ | □ |
| Quarantine | □ | □ | □ | □ | □ | □ |
| Frustration | □ | □ | □ | □ | □ | □ |
| Loneliness | □ | □ | □ | □ | □ | □ |
| Melancholy | □ | □ | □ | □ | □ | □ |
| Helplessness | □ | □ | □ | □ | □ | □ |
| Anger | □ | □ | □ | □ | □ | □ |
| Distress | □ | □ | □ | □ | □ | □ |
| Depression | □ | □ | □ | □ | □ | □ |
| Stress | □ | □ | □ | □ | □ | □ |
| Please fill in the level of frequency to the best of your understanding of the following statements. | Rarely (1) | Occasionally (2) | Often (3) | Always (4) |
| (1) Do you use some personal protection? | ||||
| Wear a mask. | □ | □ | □ | □ |
| Eye protection. | □ | □ | □ | □ |
| Wash your hands frequently with soap. | □ | □ | □ | □ |
| Avoid touching your eyes, nose, and mouth. | □ | □ | □ | □ |
| To stop the spread of the virus, I had better use serving chopsticks. | □ | □ | □ | □ |
| Keep the windows and doors open for ventilation. | □ | □ | □ | □ |
| Improve cleaning and disinfection. | □ | □ | □ | □ |
| (2) Do you use some respiratory etiquette/cough etiquette? | ||||
| Cover your mouth and nose with a tissue when you cough or sneeze. | □ | □ | □ | □ |
| Dispose tissue paper immediately after coughing or sneezing. | □ | □ | □ | □ |
| Wash your hands immediately after coughing or sneezing. | □ | □ | □ | □ |
| Perform hand hygiene (e.g., hand washing with soap or antiseptic handwash) after having contact with respiratory secretions or contaminated objects. | □ | □ | □ | □ |
| (3) Do you use any contact precautions? | ||||
| Avoid proximity (closeness) with other people. | □ | □ | □ | □ |
| Avoid group gathering. | □ | □ | □ | □ |
| Avoid taking public transportation. | □ | □ | □ | □ |
| Avoid the act of shopping in stores instead of online shopping. | □ | □ | □ | □ |
| Avoid unnecessary outings. | □ | □ | □ | □ |
| (4) Do you do any voluntary quarantine? | ||||
| If I am feeling unwell, I distance myself from others. | □ | □ | □ | □ |
| (5) Prompt reporting | ||||
| If I am feeling unwell, I will immediately declare my symptoms to the authority/healthcare providers. | □ | □ | □ | □ |
| Please fill in the level of frequency to the best of your understanding of the following statements. | Less than before (1) | The same as before (2) | A little more than before (3) | Much more than before(4) |
| (1) Do you do any regular physical exercise during the COVID-19 outbreak? | □ | □ | □ | □ |
| (2) Do you pay attention to nutrition during the COVID-19 outbreak? | □ | □ | □ | □ |
| (3) Do you go to sleep on time and get adequate sleep during the COVID-19 outbreak? | □ | □ | □ | □ |
| (4) Do you focus on positive emotions during the COVID-19 outbreak? | □ | □ | □ | □ |
| (5) Do you take the initiative to drink water during the COVID-19 outbreak? | □ | □ | □ | □ |
| Please fill in the level of your feeling to the best of your understanding of the following statements. | Not at all (1) | Somewhat (2) | Moderately (3) | Very much (4) |
| How are you feeling during the COVID-19 outbreak? | ||||
| Calm | □ | □ | □ | □ |
| Tense | □ | □ | □ | □ |
| Upset | □ | □ | □ | □ |
| Relaxed | □ | □ | □ | □ |
| Content | □ | □ | □ | □ |
| Worried | □ | □ | □ | □ |
References
- Choi, W.S.; Kim, H.S.; Kim, B.; Nam, S.; Sohn, J.W. Community treatment centers for isolation of asymptomatic and mildly symptomatic patients with coronavirus disease, South Korea. Emerg. Infect. Dis. 2020, 26, 2338. [Google Scholar] [CrossRef]
- Vali, M.; Mirahmadizadeh, A.; Maleki, Z.; Goudarzi, F.; Abedinzade, A.; Ghaem, H. The Impact of Quarantine, Isolation, and Social Distancing on COVID-19 Prevention: A Systematic Review. J. Health Sci. Surveill. Syst. 2020, 8, 138–150. [Google Scholar]
- Rodríguez-Fernández, P.; González-Santos, J.; Santamaría-Peláez, M.; Soto-Cámara, R.; Sánchez-González, E.; González-Bernal, J.J. Psychological Effects of Home Confinement and Social Distancing Derived from COVID-19 in the General Population—A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 6528. [Google Scholar] [CrossRef]
- Media, P.N. All Provinces, Municipalities and Autonomous Regions Across the Country Have Launched a First-Level Response. 2020. Available online: http://news.ifeng.com/c/7tUoW6aZsa8 (accessed on 20 March 2020).
- National Health Commission of the People’s Republic of China. Latest Situation of New Coronavirus Pneumonia as of 1 March 2020. 2020. Available online: http://www.gov.cn/xinwen/2020-03/02/content_5485524.htm (accessed on 20 March 2020).
- Li, J.-B.; Yang, A.; Dou, K.; Wang, L.-X.; Zhang, M.-C.; Lin, X.-Q. Chinese public’s knowledge, perceived severity, and perceived controllability of COVID-19 and their associations with emotional and behavioural reactions, social participation, and precautionary behaviour: A national survey. BMC Public Health 2020, 20, 1–14. [Google Scholar] [CrossRef]
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen. Psychiatry 2020, 33, e100213. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.; Zhao, N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 epidemic in China: A web-based cross-sectional survey. Psychiatry Res. 2020, 288, 112954. [Google Scholar] [CrossRef]
- Li, J.; Yang, Z.; Qiu, H.; Wang, Y.; Jian, L.; Ji, J.; Li, K. Anxiety and depression among general population in China at the peak of the COVID-19 epidemic. World Psychiatry 2020, 19, 249. [Google Scholar] [CrossRef]
- Zhou, S.-J.; Zhang, L.-G.; Wang, L.-L.; Guo, Z.-C.; Wang, J.-Q.; Chen, J.-C.; Liu, M.; Chen, X.; Chen, J.-X. Prevalence and socio-demographic correlates of psychological health problems in Chinese adolescents during the outbreak of COVID-19. Eur. Child Adolesc. Psychiatry 2020, 29, 749–758. [Google Scholar] [CrossRef]
- Choi, E.P.H.; Hui, B.P.H.; Wan, E.Y.F. Depression and Anxiety in Hong Kong during COVID-19. Int. J. Environ. Res. Public Health 2020, 17, 3740. [Google Scholar] [CrossRef]
- Serafini, R.A.; Powell, S.K.; Frere, J.J.; Saali, A.; Krystal, H.L.; Kumar, V.; Yashaswini, C.; Hernandez, J.; Moody, K.; Aronson, A. Psychological distress in the face of a pandemic: An observational study characterizing the impact of COVID-19 on immigrant outpatient mental health. Psychiatry Res. 2021, 295, 113595. [Google Scholar] [CrossRef]
- Brug, J.; Aro, A.R.; Oenema, A.; De Zwart, O.; Richardus, J.H.; Bishop, G.D. SARS risk perception, knowledge, precautions, and information sources, the Netherlands. Emerg. Infect. Dis. 2004, 10, 1486. [Google Scholar] [CrossRef]
- Bults, M.; Beaujean, D.J.; de Zwart, O.; Kok, G.; van Empelen, P.; van Steenbergen, J.E.; Richardus, J.H.; Voeten, H.A. Perceived risk, anxiety, and behavioural responses of the general public during the early phase of the Influenza A (H1N1) pandemic in the Netherlands: Results of three consecutive online surveys. BMC Public Health 2011, 11, 2. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.S.; Choi, J.S. Middle East respiratory syndrome–related knowledge, preventive behaviours and risk perception among nursing students during outbreak. J. Clin. Nurs. 2016, 25, 2542–2549. [Google Scholar] [CrossRef]
- Piltch-Loeb, R.; Abramson, D.M.; Merdjanoff, A.A. Risk salience of a novel virus: US population risk perception, knowledge, and receptivity to public health interventions regarding the Zika virus prior to local transmission. PLoS ONE 2017, 12, e0188666. [Google Scholar] [CrossRef]
- Xie, X.; Xue, Q.; Zhou, Y.; Zhu, K.; Liu, Q.; Zhang, J.; Song, R. Mental Health Status Among Children in Home Confinement During the Coronavirus Disease 2019 Outbreak in Hubei Province, China. JAMA Pediatrics 2020, 174, 898–900. [Google Scholar] [CrossRef] [Green Version]
- National Bureau of Statistics of China. National Census Report. 2021. Available online: http://www.stats.gov.cn/tjsj/tjgb/rkpcgb/qgrkpcgb/202106/t20210628_1818826.html (accessed on 9 September 2021).
- The State Council, The People’s Republic of China. COVID-19 Latest Statistics on 9 March 2020. 2020. Available online: http://www.gov.cn/fuwu/2020-03/10/content_5489342.htm (accessed on 20 March 2020).
- Wong, L.P.; Hung, C.-C.; Alias, H.; Lee, T.S.-H. Anxiety symptoms and preventive measures during the COVID-19 outbreak in Taiwan. BMC Psychiatry 2020, 20, 1–9. [Google Scholar] [CrossRef]
- Marteau, T.M.; Bekker, H. The development of a six-item short-form of the state scale of the Spielberger State—Trait Anxiety Inventory (STAI). Br. J. Clin. Psychol. 1992, 31, 301–306. [Google Scholar] [CrossRef]
- Tluczek, A.; Henriques, J.B.; Brown, R.L. Support for the reliability and validity of a six-item state anxiety scale derived from the State-Trait Anxiety Inventory. J. Nurs. Meas. 2009, 17, 19. [Google Scholar] [CrossRef] [Green Version]
- Shek, D.T. The Chinese version of the State-Trait Anxiety Inventory: Its relationship to different measures of psychological well-being. J. Clin. Psychol. 1993, 49, 349–358. [Google Scholar] [CrossRef]
- Cao, Y.; Liu, Z. Factor structure and factorial invariance of the State-Trait Anxiety Inventory for Chinese children and adolescents. Psych J. 2015, 4, 74–87. [Google Scholar] [CrossRef]
- Chen, Y.; Cao, Y.; Liu, Z. The application of a revised Chinese version of the State-Trait Anxiety Inventory in migrant children. Chin. J. Behav. Med. Brain Sci. 2013, 22, 755–757. [Google Scholar]
- Knight, R.G.; Waal-Manning, H.J.; Spears, G.F. Some norms and reliability data for the State-Trait Anxiety Inventory and the Zung Self-Rating Depression scale. Br. J. Clin. Psychol. 1983, 22, 245–249. [Google Scholar] [CrossRef] [PubMed]
- Leung, G.M.; Ho, L.-M.; Chan, S.K.; Ho, S.-Y.; Bacon-Shone, J.; Choy, R.Y.; Hedley, A.J.; Lam, T.-H.; Fielding, R. Longitudinal assessment of community psychobehavioral responses during and after the 2003 outbreak of severe acute respiratory syndrome in Hong Kong. Clin. Infect. Dis. 2005, 40, 1713–1720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glenister, K.M.; Ervin, K.; Podubinski, T. Detrimental Health Behaviour Changes among Females Living in Rural Areas during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 722. [Google Scholar] [CrossRef]
- Cheng, C.; Jun, H.; Liang, B. Psychological health diathesis assessment system: A nationwide survey of resilient trait scale for Chinese adults. Stud. Psychol. Behav. 2014, 12, 735–742. [Google Scholar]
- Hsu, C.-H.; Lin, H.-H.; Wang, C.-C.; Jhang, S. How to defend COVID-19 in Taiwan? Talk about people’s disease awareness, attitudes, behaviors and the impact of physical and mental health. Int. J. Environ. Res. Public Health 2020, 17, 4694. [Google Scholar] [CrossRef] [PubMed]
- Mattioli, A.V.; Sciomer, S.; Cocchi, C.; Maffei, S.; Gallina, S. Quarantine during COVID-19 outbreak: Changes in diet and physical activity increase the risk of cardiovascular disease. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 1409–1417. [Google Scholar] [CrossRef]
- Sañudo, B.; Fennell, C.; Sánchez-Oliver, A.J. Objectively-assessed physical activity, sedentary behavior, smartphone use, and sleep patterns pre-and during-COVID-19 quarantine in young adults from Spain. Sustainability 2020, 12, 5890. [Google Scholar] [CrossRef]
- Qian, M.; Wu, Q.; Wu, P.; Hou, Z.; Liang, Y.; Cowling, B.J.; Yu, H. Anxiety levels, precautionary behaviours and public perceptions during the early phase of the COVID-19 outbreak in China: A population-based cross-sectional survey. BMJ Open 2020, 10, e040910. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [Green Version]
- Xu, X.; Chew, K.A.; Xu, X.; Wu, Z.; Xiao, X.; Yang, Q. Demographic and social correlates and indicators for behavioural compliance with personal protection among Chinese community-dwellers during COVID-19: A cross-sectional study. BMJ Open 2021, 11, e041453. [Google Scholar] [CrossRef]
- Gomez-Aguinaga, B.; Dominguez, M.S.; Manzano, S. Immigration and Gender as Social Determinants of Mental Health during the COVID-19 Outbreak: The Case of US Latina/os. Int. J. Environ. Res. Public Health 2021, 18, 6065. [Google Scholar] [CrossRef]
- National Health Commission of the People’s Republic of China. Notification of the Prevention and Control of COVID-19 Epidemic Situation Scientifically and Accurately in Accordance with the Law. 2020. Available online: http://www.gov.cn/xinwen/2020-02/25/content_5483024.htm (accessed on 20 March 2020).
- Lin, L.Y.; Sidani, J.E.; Shensa, A.; Radovic, A.; Miller, E.; Colditz, J.B.; Hoffman, B.L.; Giles, L.M.; Primack, B.A. Association between social media use and depression among US young adults. Depress. Anxiety 2016, 33, 323–331. [Google Scholar] [CrossRef] [PubMed]
- Hou, F.; Bi, F.; Jiao, R.; Luo, D.; Song, K. Gender differences of depression and anxiety among social media users during the COVID-19 outbreak in China: A cross-sectional study. BMC Public Health 2020, 20, 1–11. [Google Scholar] [CrossRef]
- Kobayashi, T.; Maeda, M.; Takebayashi, Y.; Sato, H. Traditional Gender Differences Create Gaps in the Effect of COVID-19 on Psychological Distress of Japanese Workers. Int. J. Environ. Res. Public Health 2021, 18, 8656. [Google Scholar] [CrossRef]
- Zhang, Y.; Ma, Z.F. Impact of the COVID-19 Pandemic on Mental Health and Quality of Life among Local Residents in Liaoning Province, China: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 2381. [Google Scholar] [CrossRef] [Green Version]
- Khosravi, M. Perceived Risk of COVID-19 Pandemic: The Role of Public Worry and Trust. Electron. J. Gen. Med. 2020, 17, em203. [Google Scholar] [CrossRef] [Green Version]
- Bronfman, N.; Repetto, P.; Cordón, P.; Castañeda, J.; Cisternas, P. Gender Differences on Psychosocial Factors Affecting COVID-19 Preventive Behaviors. Sustainability 2021, 13, 6148. [Google Scholar] [CrossRef]
- Hawke, L.D.; Hayes, E.; Darnay, K.; Henderson, J. Mental health among transgender and gender diverse youth: An exploration of effects during the COVID-19 pandemic. Psychol. Sex. Orientat. Gend. Divers. 2021. [Google Scholar] [CrossRef]
- Wang, Y.; Pan, B.; Liu, Y.; Wilson, A.; Ou, J.; Chen, R. Health care and mental health challenges for transgender individuals during the COVID-19 pandemic. Lancet Diabetes Endocrinol. 2020, 8, 564–565. [Google Scholar] [CrossRef]
- Liu, S.; Chiang, Y.-T.; Tseng, C.-C.; Ng, E.; Yeh, G.-L.; Fang, W.-T. The theory of planned behavior to predict protective behavioral intentions against PM2. 5 in parents of young children from urban and rural Beijing, China. Int. J. Environ. Res. Public Health 2018, 15, 2215. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
| Participants | Population 1 | ||
|---|---|---|---|
| Variables | n | % | % |
| Gender | |||
| Male | 1079 | 27.8 | 51.2 |
| Female | 2799 | 72.2 | 48.8 |
| Age | |||
| 18~30 | 2071 | 53.4 | 21.7 |
| 31~50 | 1490 | 38.4 | 33.1 |
| 51 and above | 317 | 8.2 | 24.3 |
| Educational qualification | |||
| High school or below | 687 | 17.7 | 88.8 (18 years and above) |
| College or undergraduate | 2408 | 62.1 | 10.8 (18 years and above) |
| Postgraduate | 783 | 20.2 | 0.3 (18 years and above) |
| Personal income | N/A | ||
| Less than RMB 4000/month | 2152 | 55.5 | |
| RMB 4001~10,000/month | 1394 | 35.9 | |
| More than RMB 10,001/month | 332 | 8.6 | |
| Occupation | N/A | ||
| Students | 1288 | 33.2 | |
| Employees | 1966 | 50.7 | |
| Health care workers | 136 | 3.5 | |
| Migrant workers/peasants/jobless and others | 488 | 12.6 | |
| Residing area | |||
| Urban | 2466 | 63.6 | 30.3% (cities) |
| Rural | 1412 | 36.4 | 69.7% (villages and rural areas) |
| Cumulative risk area of infection 1 | |||
| High-risk area | 131 | 3.4 | 3.4 |
| Medium-risk area | 2391 | 61.6 | 61.7 |
| Low-risk area | 1356 | 35.0 | 35 |
| Variables | Number of Items | Possible Range | Mean | SD | Cronbach’sAlpha |
|---|---|---|---|---|---|
| Preventive knowledge | 4 | 0–1 | 0.96 | 0.12 | 0.60 |
| Risk perception | 3 | 1–6 | 3.01 | 1.20 | 0.96 |
| Public trust in government | 4 | 1–6 | 5.09 | 0.90 | 0.95 |
| Preventive behaviors | 18 | 1–4 | 3.58 | 0.39 | 0.84 |
| Healthy lifestyle | 5 | 1–4 | 2.06 | 0.63 | 0.83 |
| Anxiety symptoms | 6 | 20–80 | 48.20 | 11.30 | 0.80 |
| Emotional response to home quarantine | 10 | 1–6 | 3.34 | 1.08 | 0.96 |
| Variables | β | t | Adj. R2 | F |
|---|---|---|---|---|
| Constant | 43.71 *** | |||
| Gender (Reference: Female) | ||||
| Male | −0.13 | −8.03 *** | ||
| Age (Reference: 18–30) | ||||
| 31–50 | −0.05 | −2.19 * | ||
| 51–70 | −0.08 | −4.31 *** | ||
| Educational qualification (Reference: High school or below) | ||||
| College or undergraduate | 0.07 | 2.54 * | ||
| Postgraduate | 0.06 | 2.47 * | ||
| Personal income (Reference: Less than RMB 4000/month) | ||||
| RMB 4000~10,000/month | 0.03 | 1.55 | ||
| More than RMB 10,000/month | 0.02 | 0.96 | ||
| Occupation (Reference: Students) | ||||
| Employees | 0.04 | 1.52 | ||
| Health care workers | 0.02 | 0.89 | ||
| Migrant workers/peasants/jobless and others | 0.04 | 1.95 | ||
| Residing area (Reference: Rural) | ||||
| Urban | 0.08 | 4.88 *** | ||
| Risk area (Reference: Low-risk area) | ||||
| High-risk area | 0.02 | 0.96 | ||
| Medium-risk area | 0.05 | 3.35 ** | ||
| Preventive knowledge (4 items) | 0.03 | 1.99 * | ||
| Risk perception (3 items) | 0.02 | 1.54 | ||
| Trust in the government’s mitigation measures to the COVID-19 pandemic (4 items) | 0.26 | 16.98 *** | ||
| 0.100 | 27.97 *** |
| Variables | β | t | Adj. R2 | F |
|---|---|---|---|---|
| Constant | 23.63 *** | |||
| Gender (Reference: Female) | ||||
| Male | 0.04 | 2.76 ** | ||
| Age (Reference: 18–30) | ||||
| 31–50 | −0.03 | −1.49 | ||
| 51–70 | −0.01 | −0.57 | ||
| Educational qualification (Reference: High school or below) | ||||
| College or undergraduate | −0.03 | −1.15 | ||
| Postgraduate | 0.02 | −0.80 | ||
| Personal income (Reference: Less than RMB 4000/month) | ||||
| RMB 4000~10,000 | −0.01 | −0.48 | ||
| More than RMB 10,000/month | −0.02 | −1.16 | ||
| Occupation (Reference: Students) | ||||
| Employees | −0.00 | −0.18 | ||
| Health care workers | −0.03 | −1.73 | ||
| Migrant workers/peasants/jobless | 0.00 | 0.12 | ||
| Residing area (Reference: Rural) | ||||
| Urban | −0.01 | −0.71 | ||
| Risk area (Reference: Low-risk area) | ||||
| High-risk area | 0.02 | 0.99 | ||
| Medium-risk area | 0.02 | −1.39 | ||
| Preventive knowledge (4 items) | −0.11 | −7.21 *** | ||
| Risk perception (3 items) | 0.21 | 13.46 *** | ||
| Trust in the government’s mitigation measures to the COVID-19 pandemic (4 items) | −0.05 | −3.37 ** | ||
| Preventive behaviors (18 items) | −0.04 | −2.30 * | ||
| Healthy lifestyle (5 items) | −0.18 | −12.04 *** | ||
| 0.127 | 32.33 *** |
| Variables | Moderate to Severe Anxiety vs. Moderate Anxiety | ||
|---|---|---|---|
| Adj. OR | 95%CI | ||
| Gender (Reference: Female) | |||
| Male | 0.66 *** | 0.57 | 0.78 |
| Age (Reference: 18–30) | |||
| 31–50 | 0.61 *** | 0.50 | 0.74 |
| 51–70 | 0.46 *** | 0.34 | 0.61 |
| Educational qualification (Reference: High school or below) | |||
| College or undergraduate | 0.96 | 0.76 | 1.21 |
| Postgraduate | 1.13 | 0.86 | 1.50 |
| Personal income (Reference: Less than RMB 4000/month) | |||
| RMB 4000~10,000/month | 1.07 | 0.88 | 1.31 |
| More than RMB 10,000/month | 0.94 | 0.70 | 1.28 |
| Occupation (Reference: Students) | |||
| Employees | 1.03 | 0.80 | 1.31 |
| Health care workers | 0.75 | 0.49 | 1.14 |
| Migrant workers/peasants/jobless | 1.05 | 0.77 | 1.43 |
| Residing area (Reference: Rural) | |||
| Urban | 0.81 ** | 0.69 | 0.95 |
| Risk area (Reference: Low-risk area) | |||
| High-risk area | 1.44 | 0.94 | 2.21 |
| Medium-risk area | 1.02 | 0.88 | 1.18 |
| Preventive knowledge (4 items) | 0.36 ** | 0.19 | 0.70 |
| Risk perception (3 items) | 1.17 *** | 1.10 | 1.24 |
| Trust in the government’s mitigation measures to the COVID-19 pandemic (4 items) | 0.77 *** | 0.71 | 0.83 |
| Preventive behaviors (18 items) | 0.69 *** | 0.57 | 0.84 |
| Healthy lifestyle (5 items) | 0.89 * | 0.79 | 0.99 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, S.-M.; Shih, S.-F.; Meng, B.; Zhen, R.; Pan, X.-B.; Ng, E.; Hsu, C.-H.; Fang, W.-T. Gendered Factors Associated with Preventive Behaviors and Mental Health among Chinese Adults during the COVID-19 Pandemic Home Quarantine. Sustainability 2021, 13, 10819. https://doi.org/10.3390/su131910819
Liu S-M, Shih S-F, Meng B, Zhen R, Pan X-B, Ng E, Hsu C-H, Fang W-T. Gendered Factors Associated with Preventive Behaviors and Mental Health among Chinese Adults during the COVID-19 Pandemic Home Quarantine. Sustainability. 2021; 13(19):10819. https://doi.org/10.3390/su131910819
Chicago/Turabian StyleLiu, Shu-Mei, Shu-Fang Shih, Bo Meng, Rui Zhen, Xiao-Ben Pan, Eric Ng, Chia-Hsuan Hsu, and Wei-Ta Fang. 2021. "Gendered Factors Associated with Preventive Behaviors and Mental Health among Chinese Adults during the COVID-19 Pandemic Home Quarantine" Sustainability 13, no. 19: 10819. https://doi.org/10.3390/su131910819
APA StyleLiu, S.-M., Shih, S.-F., Meng, B., Zhen, R., Pan, X.-B., Ng, E., Hsu, C.-H., & Fang, W.-T. (2021). Gendered Factors Associated with Preventive Behaviors and Mental Health among Chinese Adults during the COVID-19 Pandemic Home Quarantine. Sustainability, 13(19), 10819. https://doi.org/10.3390/su131910819