1. Introduction
Construction is ranked as the most hazardous operation involving musculoskeletal disorders and injuries. MSDs are caused by sudden exertion or prolonged exposure to physical factors (i.e., high force, repetitive motion, awkward body posture, and vibration) and affects the muscles, nerves, tendons, joints, cartilage, and supporting structures of the upper and lower limbs, neck, and lower back, etc. [
1]. MSDs are attributed to handling heavy manual materials, manipulating excessive and repetitive hand tools, performing repetitive screw motions, reinforcing works involving difficult postures, and so on [
2]. When the working posture differs from the neutral posture in which the body is aligned and balanced while placing minimal stress on the muscles, tendons, nerves, and bones, the stress on the body parts (i.e., the muscles, tendons, joints, arms, hands, and shoulders) increases, resulting in awkward postures and/or movements of the body parts of the workers, in turn leading to a negative impact on the safety and health of the workers as well as on productivity. The percentage of construction workers exposed to the musculoskeletal hazards in Korea while carrying heavy loads, standing long, and maintaining tiring and painful positions, is about 72%, 83.8%, and 67.9%, respectively [
3]. Herein, we identify the factors that either affect ergonomic interventions or reduce MSDs in construction workers (i.e., masons, pavers, and electricians) [
4].
Existing studies provide ergonomic analysis methods that employ motion sensing and assessment tools [
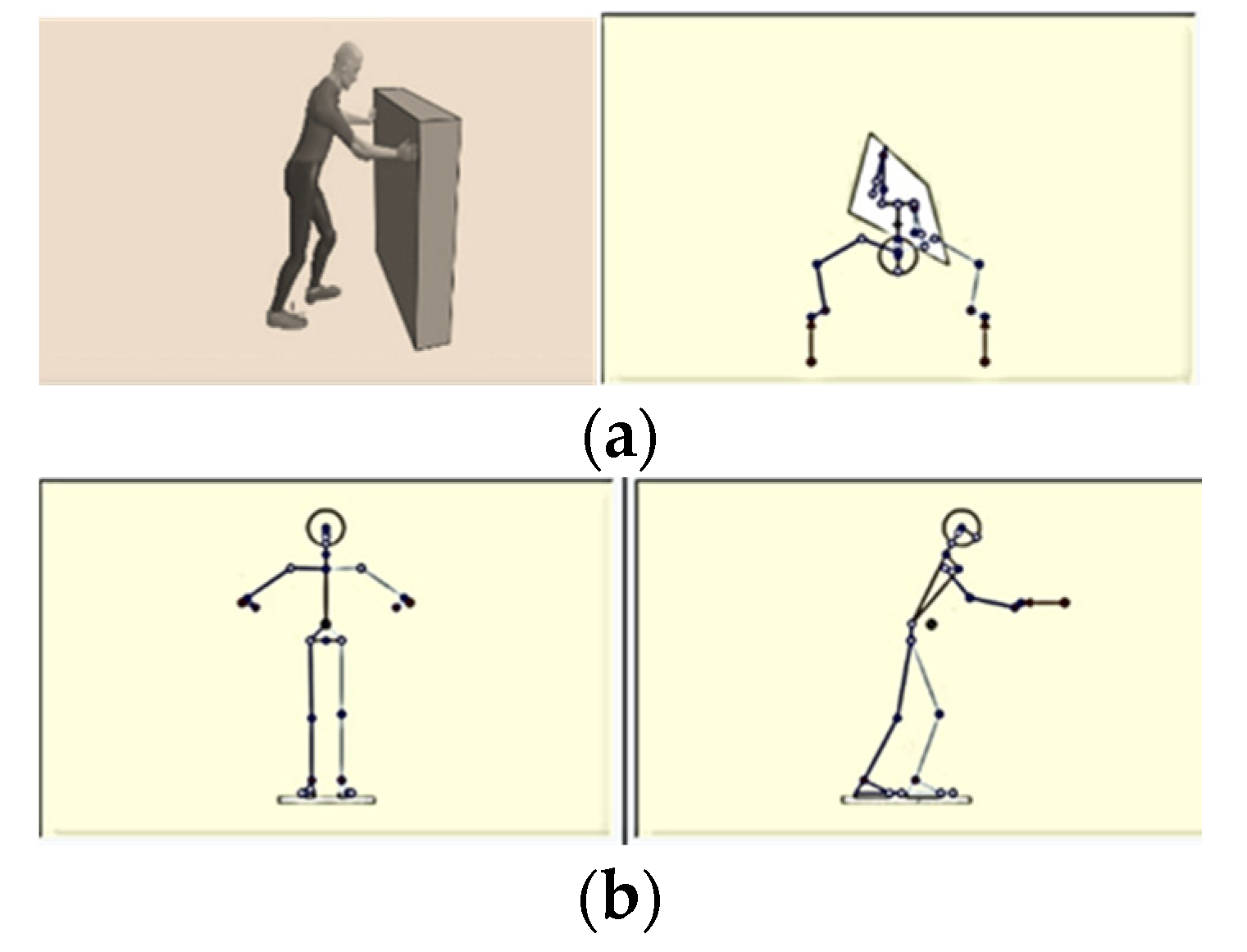
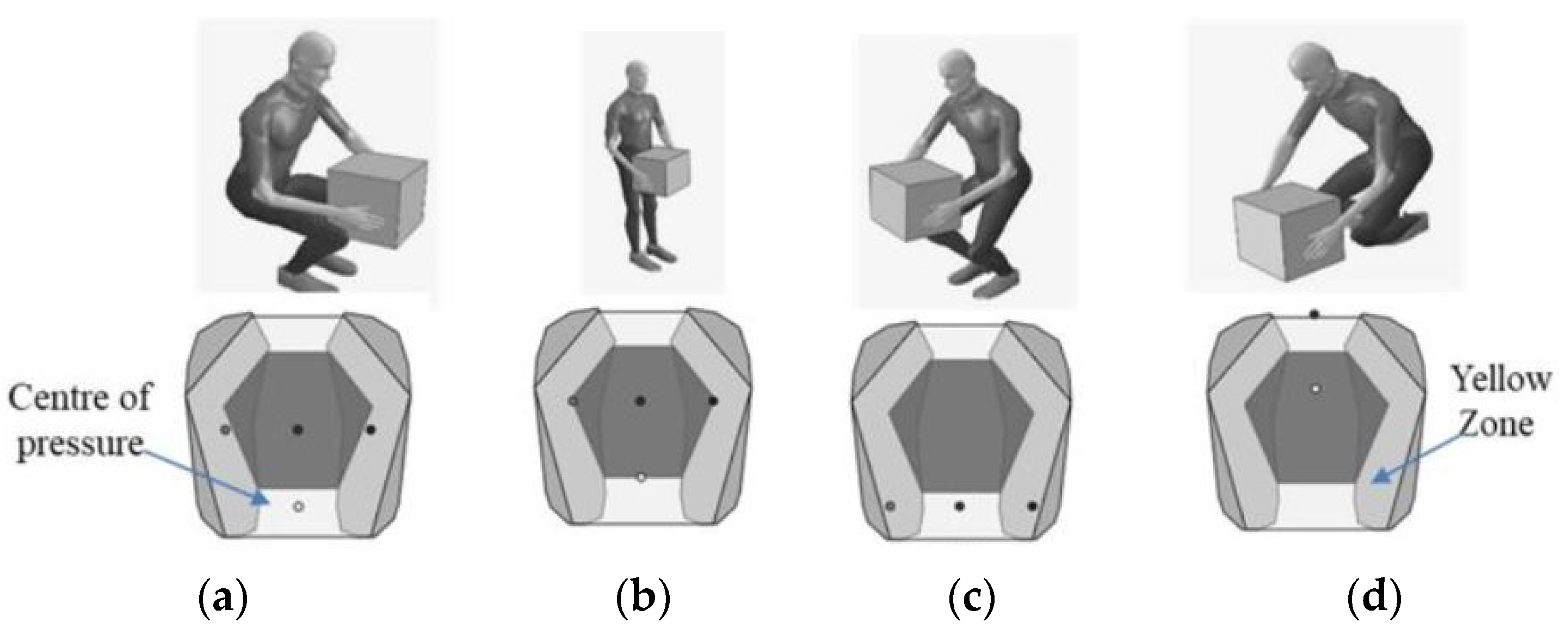
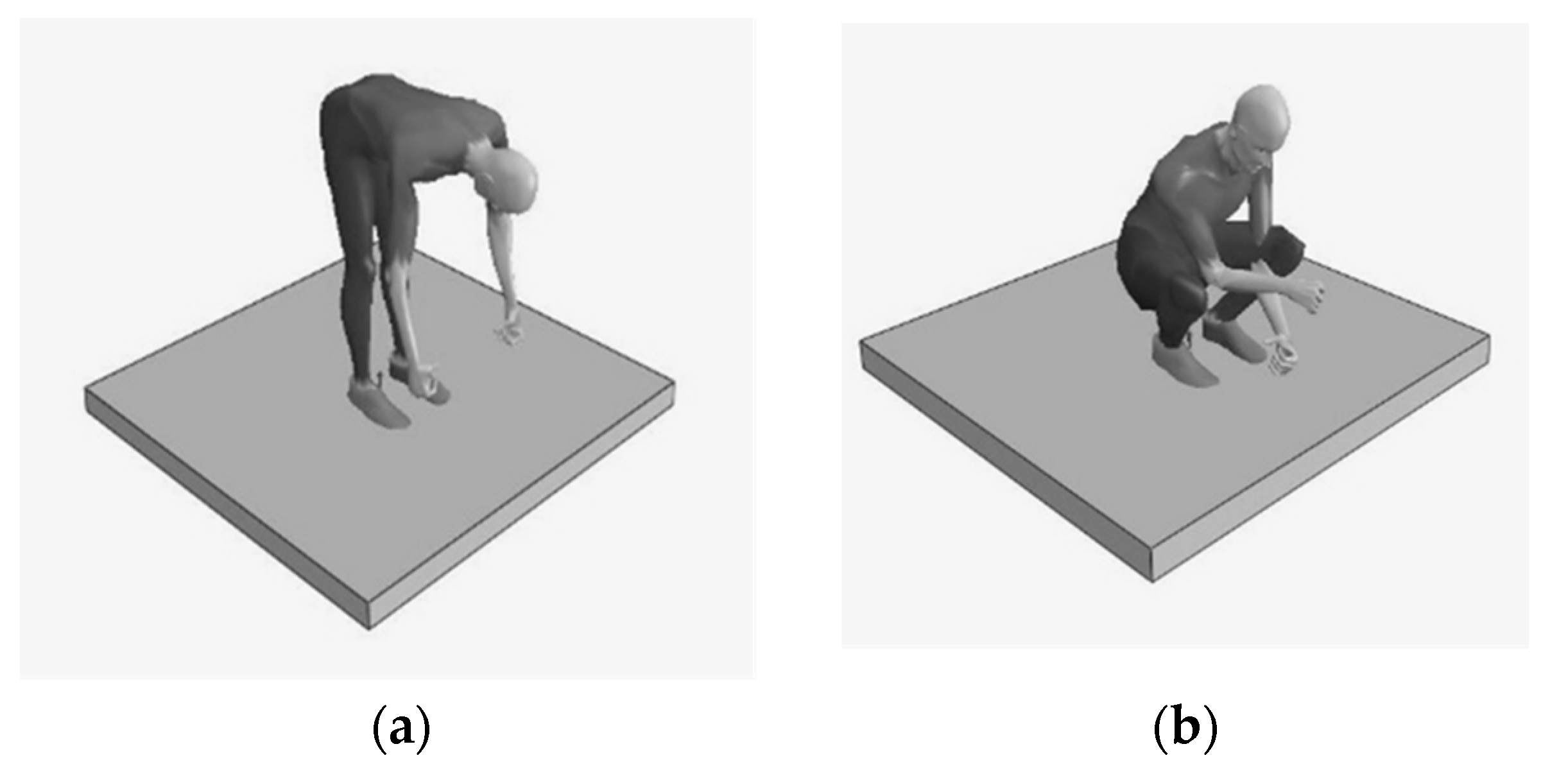
5] to alleviate MSDs or to implement preventive measures. However, the correlation between anthropometry and the magnitude of hand forces has not been well explored. A new ergonomic analysis method that identifies the correlation between these two will be beneficial to a construction administrator for estimating, say, the compression on the lower back, and for establishing a benchmark of the workload imposed on a worker using BMI and hand forces exerted in diverse working postures (i.e., pushing forward, lifting, stooping, and kneeling). Such estimations may contribute to securing labor safety and health by efficiently identifying competent workers from an ergonomic viewpoint for the given work task. Three dimensions of environment, society, and economy are frequently used to model how sustainability can be incorporated into one’s mission, goals, and practices. However, the issues involved in the social dimension of sustainability (i.e., labor relations, diversity, workers benefits/compensation, human rights, the organization of work, etc.) have often been overlooked, resulting in negative impacts (i.e., hazards to workers and creating tension between goals). Many worker issues exist within the concept of sustainability. The proposed posture simulation and benchmarking approach, relevant to the workers’ social issues that promotes labor welfare, safety, and health.
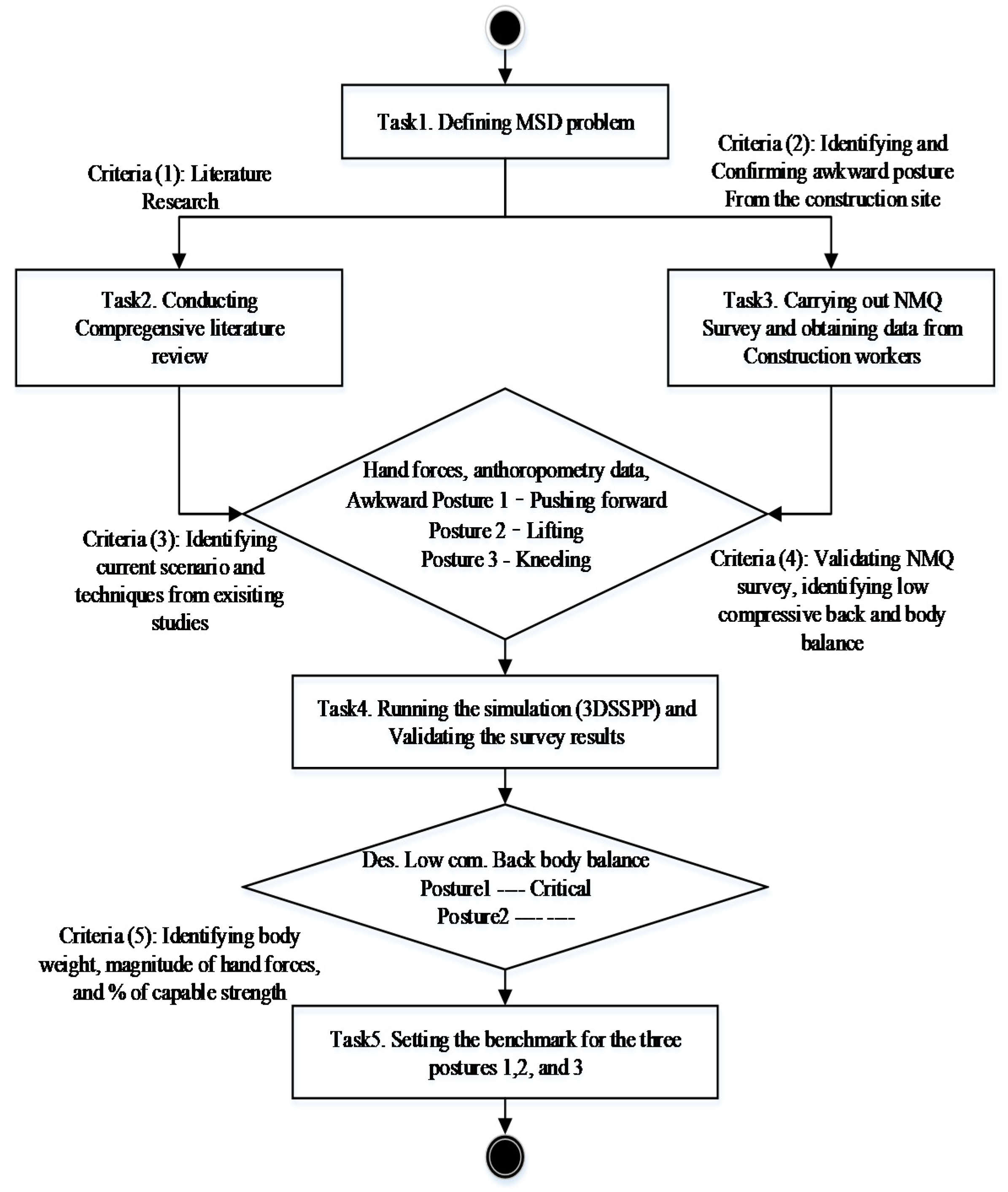
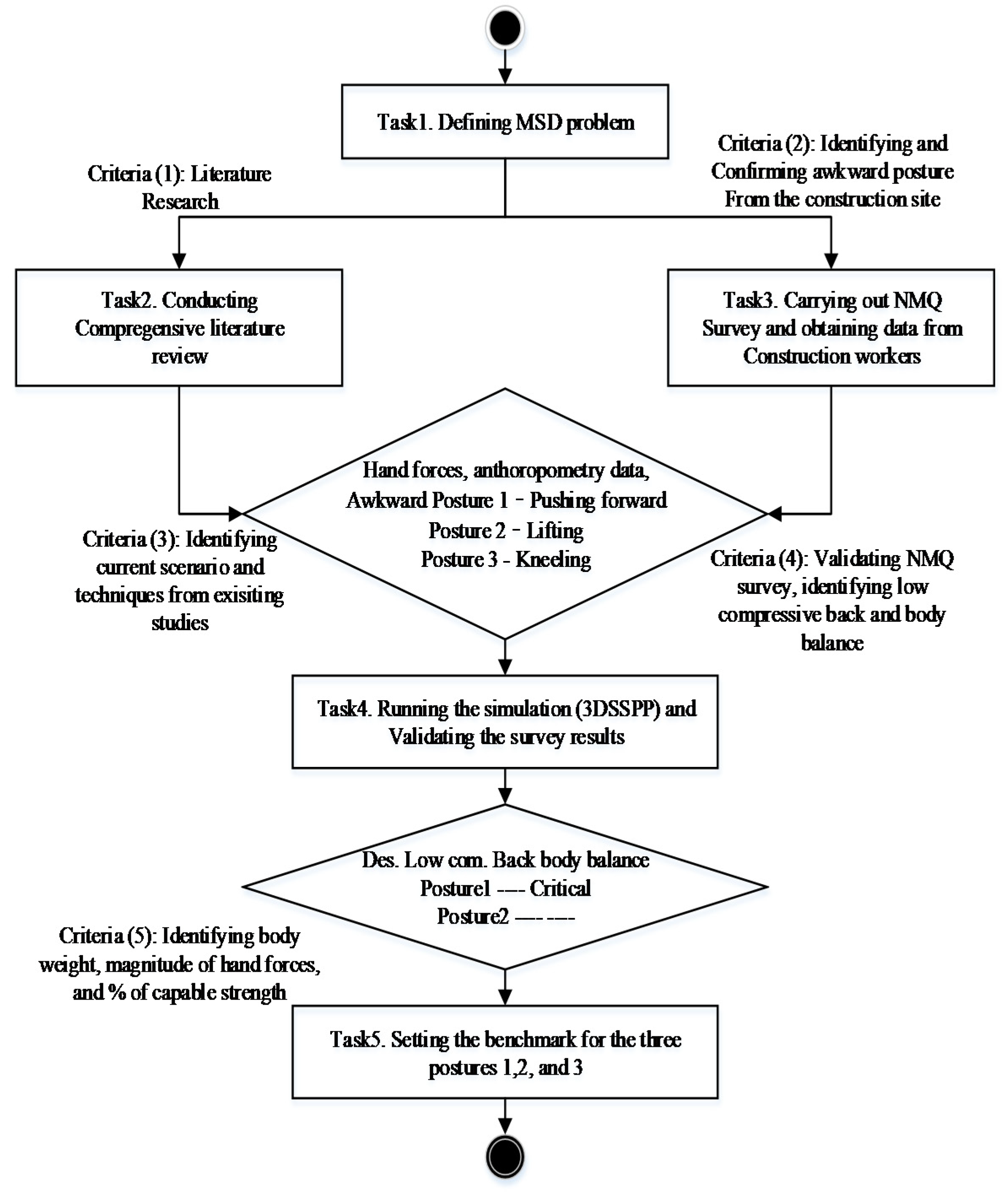
The research was conducted in five steps. First, the performance of existing ergonomic modeling and analysis methods for the construction industry was investigated through a literature review to identify new research contributions. Second, a set of Nordic Musculoskeletal Questionnaire surveys was administered to workers from various construction trades to identify the MSD issues of each trade. The ergonomic data, including the MSDs affecting various body parts of workers, were collected from workers engaged in bare-hand manual operations in four Korean construction sites. Third, the new ergonomic model that establishes a benchmark of the workload imposed on construction workers engaged in diverse working postures was implemented in an automated tool by mapping the survey findings into a three-dimensional static strength prediction program (3D SSPP) software. Fourth, the model performance was demonstrated using a set of working postures (i.e., pushing forward, lifting, stooping, and kneeling). The validity and effectiveness of the model were verified by performing a series of case studies, each of which the common awkward body postures were identified and the static strength and compressive forces attributed to each awkward posture were estimated using 3D SSPP. It was confirmed that the model established the benchmark using hand force and body mass index (BMI). Finally, the research contributions and limitations were examined. The material in this paper is organized in the same order. Indeed, the findings will be of help for construction administrators to understand MSD issues experienced by workers employed in a specific operation and will provide clues to identify those tasks that can be semi-automated or fully-automated for better benefits.
2. Current State of Musculoskeletal Disorder Studies
MSD is the highest contributor to global disability, accounting for 16% of all years lived with disability; lower back pain is the single leading cause (Global burden of disease, 2017). In South Korea, the percentage of workers aged 50 years or older was 25% in 2010 and this value is expected to exceed 33% in 2020 [
6]. Workers suffering from MSDs include aged construction craftsmen exposed to severe vibrations, construction and mining technicians, and construction finishing workers (61.3%, 47.8%, and 46%, respectively). The prevalence of chronic MSDs and degradation of body parts attributed to aging may lead to decreased physical labor capability. The frequency of back pain, upper extremities, and lower extremities and fatigue are chronically high in construction workers, about 30.7%, 61.3%, 49.2%, and 35.6%, respectively [
3]. Existing studies claim that, compared to young workers, aged workers are more likely to suffer from musculoskeletal symptoms.
Meanwhile, existing ergonomics analysis techniques may be classified into self-reporting, manual observation, direct sensing measurement, and vision-based analysis. Self-reporting is a data collection process that involves conducting interviews and web-based questionnaires [
7]. Manual observation tools facilitate measuring and/or evaluating MSD via hybridizing body position and movement-tracking tools (e.g., assessment of repetitive task, Ovako working posture analysis system, posture activity tools and handling, rapid upper limb assessment, and rapid entire body assessment (REBA)) [
8]. However, they lend themselves neither to a precise posture measurement nor to the recording of delicate movement patterns such as that possible in time-lapse video observation. In direct sensing measurement, various sensor(s) are attached to the body parts of workers; these approaches outperform the two approaches in terms of measurement accuracy. The accuracy may be augmented by hybridizing the measurement method with Microsoft Kinect Cameras for efficient real-time motion analysis [
9,
10]. Vision-based analysis allows for precise motion tracking along with biomechanical parameter measurements that use devices such as tapes and goniometers, microelectromechanical systems (MEMS), electrodes for electromyography (EMG), and magnetoresistive sensors. Although this method facilitates measuring joint angles, including the angle of the neck, it is cumbersome because construction workers must wear devices while working. Although it outperforms existing methods, methods based on such analysis are still far from the ideal [
11].
Existing studies have identified that construction workers suffer from physical fatigue and muscle pain when exposed to excessive energy consumption, resulting in human error, unsafe actions, and productivity loss, etc. In addition, a few studies claim that practical methods that assess MSD risks to all parts of the body are necessary in construction, proposing new technologies that facilitate the identification of preventive measures involved in appropriate body posture [
12]. However, they are not yet arrived in a maturity to proper implementation. MSD remains a substantial concern with considerable personal and societal burdens [
13]. Indeed, it would be beneficial to enlighten MSD issues to the construction practitioners hybridizing posture simulation and survey methods. It may contribute to identifying human MSD along with a benchmarking approach that supports making preventive MSD tools for construction personnel.
For construction workers, the anthropometric traits and hand forces to which different body parts (i.e., the neck, shoulder, fingers, knee, and wrist) are subjected depend on the task types (i.e., overhead work, ground-floor-level work, and manual material-handling work) [
14]. Several musculoskeletal injury prevention measures (e.g., site-specific ergonomics programs, engineering controls, mechanical devices, exercise programs) have been enforced to reduce the burden of manual-lifting hazards. The “best practices” do not cause pain and/or discomfort in the back and wrist, and were identified to increase the productivity [
2,
15]. These measures encourage the development of initiatives that analyze ergonomic hazards and implement site-specific mitigation strategies and practices. It will be beneficial to reengineer improvement techniques and to upgrade its dynamic condition against work-related MSDs. Existing studies provide methods to identify the body postures of workers and suggest their corresponding preventive measures. However, these studies did not deal with tracking transitory motion changes at an appropriate level of detail or modeling MSDs in a working environment. Therefore, construction safety still incurs considerable personal and socioeconomic burden. A new simulation modeling, analysis, and controlling tool that effectively handles the MSD issues faced by workers involved in a construction operation will be beneficial. A simulation model formulated based on worker survey results may contribute to the construction safety and health by establishing a benchmark for actioning MSD-prevention measures.
5. Discussion
The method combining the NMQ survey, biomechanical analysis, and benchmark approach facilitates quantitative MSD control over the muscle stress of construction workers. It encourages informed decision making on recruiting appropriate workers considering their physical merits (i.e., muscle strength) for a specific job function in a construction operation. It fills gaps the computational method handling different parts MSD that the existing methods had not adequately described to access the health risks of construction workers by doing simulation on construction worker postures. It may replicate specific task, finding construction workers’ MSD issues attributed to using semi-automatic or fully automatic tools. The biomechanical analysis outputs involved in the unacceptable and awkward postures (
Table 5,
Table 6 and
Table 7) that impose high risk provide a tool to field employment managers to identify the tradeoff between BMI and the magnitude of the hand forces to execute preventive measures (i.e., exercise programs and engineering controls) [
20]. Few studies provide an insight into reducing work-related musculoskeletal injuries given the existing preventive measures. This lack of research may be attributed to the fact that analysis of work tasks at a job site is a complex task because of various factors (e.g., organizational, human, task factors). The new hybrid method allows an elaborate analysis of work postures associated with construction tasks by considering job-specific risks attributed to process, motion, and posture. Note that the method identifies potential MSDs associated with the awkward postures of a worker performing a job function while controlling other job-site variables.
The limitations of the method are related to the biomechanical issues as follows: First, it is desirable that sophisticated postures are considered jointly by accommodating 3D motion analysis in a future version of the method. A worker’s muscle strength may not be determined by the biomechanical simulation model alone. However, the model may provide a control tool for MSD safety and health of workers by validating the physical demands (e.g., lower back compressive strength, percentage of strength capability, and body balance) obtained by expert group surveys of the construction community. Second, the momentary and transitory issues involved in motions have been intensified among the workers involved in construction. A controlled experiment on construction workers is not feasible because it is not easy to have many workers perform identical motions at a construction job site. In addition, their motions are momentary, transitory, and involve multiple tasks at a time. It will be commendable to perform controlled experiments in a simulated construction job site to generalize the outputs obtained by the method. Third, it will be beneficial to track each motion activated by a participant performing a specific task. It may encourage the elaborative evaluation of MSD. For instance, biomechanical human simulation may effectively predict the relation between muscle strength for a construction task and the workplace dimension by using identified awkward postures. Fourth, extensive controlled experiments with different exercise protocols (i.e., the type of working layouts, frequency of postures, intensity of motion, and duration of posture) may contribute to identifying unknown variables that influence the relationship between two variables and to secure the validity of the method and its corresponding data.







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}





