Psychological Care of Health Workers during the COVID-19 Outbreak in Italy: Preliminary Report of an Occupational Health Department (AOUP) Responsible for Monitoring Hospital Staff Condition

 ,
,  , ,
, , 

Abstract
1. Introduction
2. Materials and Methods
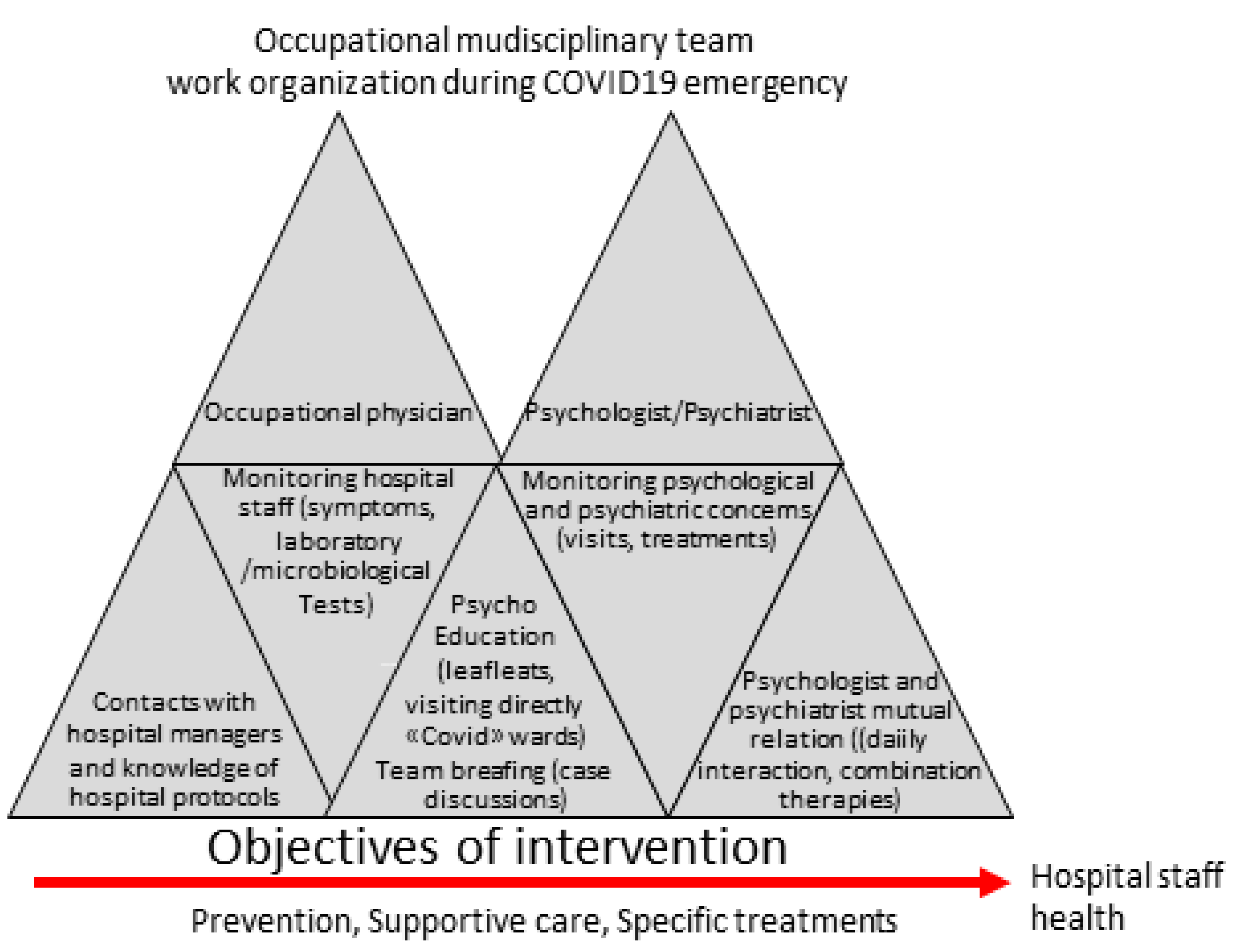
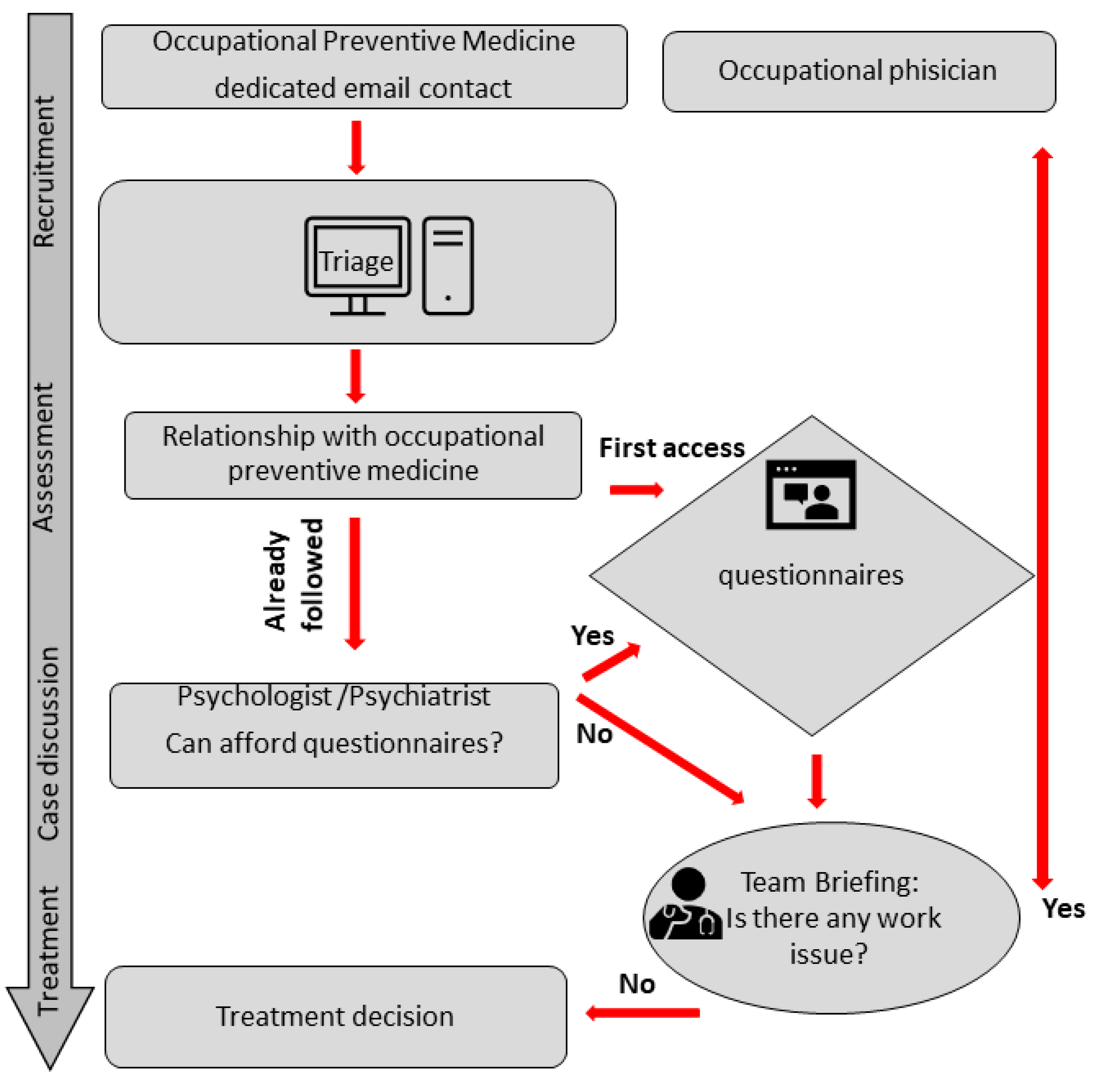
2.1. Procedures
2.1.1. Screening Questionnaires
2.1.2. Psychiatric Consulting
- working on a “COVID” or “non-COVID” ward;
- having contracted the Sars-Cov-2 infection;
- working exclusion due to temporary COVID19-related unfitness
- having a poor tolerance to personal protective equipment (PPE).
2.1.3. Psychological Consultation
- improvement of emotional and cognitive resource use to reinforce the sense of altruism, and to face anxiety and fear of contagion or death;
- improvement of awareness of factors within and beyond personal control to achieve a functional appraisal of what the epidemic actually represents;
- training emotion regulation skills and acceptance-based abilities; and
- restoration of personal resilience in the face of stress.
2.1.4. Team Briefing
3. Results
3.1. Overall Sample Characteristics
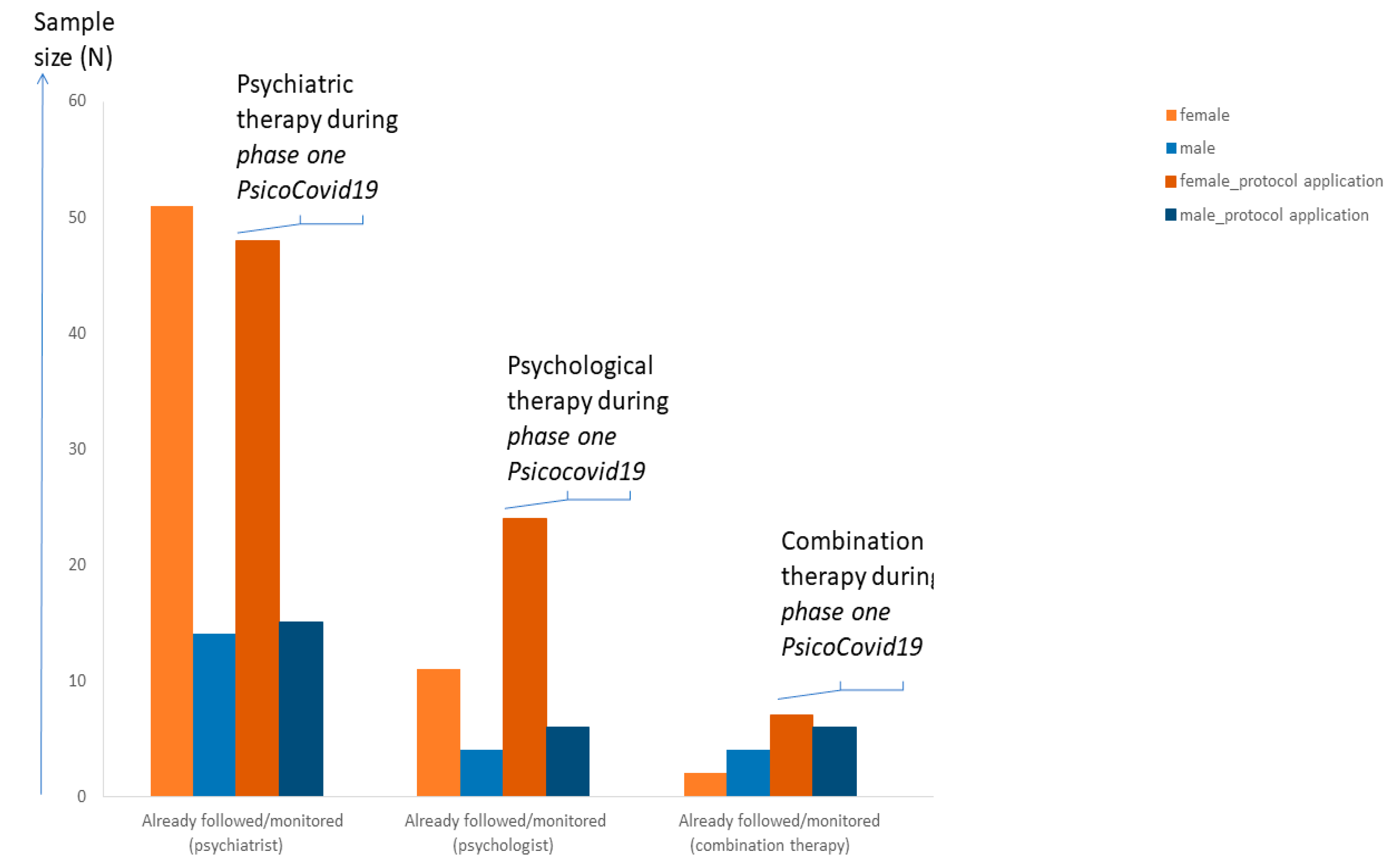
3.2. Workers’ Psychiatric Concerns
3.3. Workers Psychological Concerns
3.4. Satisfaction Rate
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ruotsalainen, J.; Serra, C.; Marine, A.; Verbeek, J. Systematic review of interventions for reducing occupational stress in health care workers. Scand. J. Work Environ. Health 2008, 34, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Ruotsalainen, J.H.; Verbeek, J.H.; Mariné, A.; Serra, C. Preventing occupational stress in healthcare workers. Cochrane Database Syst. Rev. 2014, 13, CD002892. [Google Scholar] [CrossRef]
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Cohen Silver, R.; Everall, I.; et al. Multidisciplinary research priorities for Covid-19 pandemic: A call for action for mental health science. Lancet Psichiatr. 2020. [Google Scholar] [CrossRef]
- Rajkumar, R.P. COVID-19 and mental health: A review of the existing literature. Asian J. Psychiatry 2020, 52, 102066. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Occupation Health. Health Worker Occupational Health. 2018. Available online: https://www.who.int/occupational_health/topics/hcworkers/en/ (accessed on 10 March 2019).
- Ramaci, T.; Barattucci, M.; Ledda, C.; Rapisarda, V. Social Stigma during COVID-19 and its Impact on HCWs Outcomes. Sustainability 2020, 12, 3834. [Google Scholar] [CrossRef]
- Cirrincione, L.; Plescia, F.; Ledda, C.; Rapisarda, V.; Martorana, D.; Moldovan, R.E.; Theodoridou, K.; Cannizzaro, E. COVID-19 Pandemic: Prevention and Protection Measures to Be Adopted at the Workplace. Sustainability 2020, 12, 3603. [Google Scholar] [CrossRef]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors Associated with Mental Health Outcomes Among Health Care Workers Exposed to Coronavirus Disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef]
- Zhang, J.; Wu, W.; Zhao, X.; Zhang, W. Recommended psychological crisis intervention response to the 2019 novel coronavirus pneumonia outbreak in China: A model of West China Hospital. Precis. Clin. Med. 2020, 3, 3–8. [Google Scholar] [CrossRef]
- Xiang, Y.T.; Yang, Y.; Li, W.; Zhang, L.; Zhang, Q.; Cheung, T.; Ng, C.H. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry 2020, 7, 228–229. [Google Scholar] [CrossRef]
- Carrieri, D.; Briscoe, S.; Jackson, M.; Mattick, K.; Papoutsi, C.; Pearson, M.; Wong, G. ‘Care Under Pressure’: A realist review of interventions to tackle doctors’ mental ill-health and its impacts on the clinical workforce and patient care. BMJ Open 2018, 8, e021273. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Liang, M.; Li, Y.; Guo, J.; Fei, D.; Wang, L., III; He, L.; Sheng, C.; Cai, Y.; Li, X.; et al. Mental health care for medical staff in China during the COVID-19 outbreak. Lancet Psychiatry 2020, 7, e15–e16. [Google Scholar] [CrossRef]
- Zgueb, Y.; Bourgou, S.; Neffeti, A.; Amamou, B.; Masmoudi, J.; Chebbi, H.; Somrani, N.; Bouaskeri, A. Psychological crisis intervention response to the COVID 19 pandemic: A Tunisian centralised Protocol. Psychiatry Res. 2020, 289, 113042. [Google Scholar] [CrossRef] [PubMed]
- Kang, L.; Ma, S.; Chen, M.; Yang, J.; Wang, Y.; Li, R.; Yao, L.; Bai, H.; Cai, Z.; Yang, B.X.; et al. Impact on mental health and perceptions of psychological care among medical and nursing staff in Wuhan during the 2019 novel coronavirus disease outbreak: A cross-sectional study. Brain Behav. Immun. 2020, in press. [Google Scholar] [CrossRef] [PubMed]
- Buselli, R.; Veltri, A.; Baldanzi, S.; Marino, R.; Bonotti, A.; Chiumiento, M.; Girardi, M.; Pellegrini, L.; Guglielmi, G.; Dell’Osso, L.; et al. Plasma Brain-Derived Neurotrophic Factor (BDNF) and serum cortisol levels in a sample of workers exposed to occupational stress and suffering from Adjustment Disorders. Brain Behav. 2019, 9, e01298. [Google Scholar] [CrossRef] [PubMed]
- Buselli, R.; Pacciardi, B.; Gonnelli, C.; Novi, M.; Gattini, V.; Guglielmi, G.; Foddis, R.; Mignani, A.; Cristaudo, A. Psychiatric Support of Healthcare Workers Undergoing Periodic Health Assessment. G. Ital. Med. Lav. Ergon. 2009, 31, 149–153. [Google Scholar]
- Buselli, R.; Veltri, A.; Baldanzi, S.; Bozzi, S.; Marino, R.; Chiumiento, M.; Dell’Osso, L.; Cristaudo, A. Work-related Stress Disorders: Variability in Clinical Expression and Pitfalls in Psychiatric Diagnosis. Med. Lav. 2016, 107, 92–101. [Google Scholar] [PubMed]
- Buselli, R.; Del Guerra, P.; Caldi, F.; Veltri, A.; Battaglia, S.; Baldanzi, S.; Girardi, M.; Sallese, D.; Dell’Osso, L.; Cristaudo, A. Mental disability management within occupational health surveillance. Med. Lav. 2020, 111. in press. [Google Scholar]
- Buselli, R.; Carmassi, C.; Corsi, M.; Baldanzi, S.; Battistini, G.; Chiumiento, M.; Massimetti, G.; Dell’Osso, L.; Cristaudo, A. Post-traumatic stress symptoms in an Italian cohort of subjects complaining occupational stress. CNS Spectrum. 2020, in press. [Google Scholar]
- Liu, S.; Yang, L.; Zhang, C.; Xiang, Y.T.; Liu, Z.; Hu, S.; Zhang, B. Online mental health services in China during the COVID-19 outbreak. Lancet Psychiatry 2020, 7, e17–e18. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Ball, R.; Ranieri, W. Comparison of Beck Depression Inventories -IA and -II in psychiatric outpatients. J. Pers. Assess. 1996, 67, 588–597. [Google Scholar] [CrossRef] [PubMed]
- Kvaal, K.; Ulstein, I.; Nordhus, I.H.; Engedal, K. The Spielberger State-Trait Anxiety Inventory (STAI): The state scale in detecting mental disorders in geriatric patients. Int. J. Geriatr. Psychiatry 2005, 20, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, J.; Bond, F.W.; Flaxman, P. The value of psychological flexibility: Examining psychological mechanisms underpinning a cognitive behavioural therapy intervention for burnout. Work Stress 2013, 27, 181–199. [Google Scholar] [CrossRef]
- Howard, F. Managing stress or enhancing wellbeing? Positive psychology’s contributions to clinical supervision. Aust. Psychol. 2008, 43, 105–113. [Google Scholar] [CrossRef]
- Hobfoll, S.E.; Watson, P.; Bell, C.C.; Bryant, R.A.; Brymer, M.J.; Friedman, M.J.; Friedman, M.; Gersons, B.P.; de Jong, J.T.; Layne, C.M.; et al. Five essential elements of immediate and mid-term mass trauma intervention: Empirical evidence. Psychiatry 2007, 70, 283–315. [Google Scholar] [CrossRef] [PubMed]
- Bond, F.W.; Hayes, S.C.; Barnes-Holmes, D. Psychological Flexibility, ACT, and Organizational Behavior. J. Organ. Behav. Manag. 2006, 26, 25–54. [Google Scholar] [CrossRef]
- Duan, L.; Zhu, G. Psychological interventions for people affected by the COVID-19 epidemic. Lancet Psychiatry 2020, 7, 300–302. [Google Scholar] [CrossRef]
- Adalja, A.A.; Toner, E.; Inglesby, T.V. Priorities for the US Health Community Responding to COVID-19. JAMA 2020, 323, 1343–1344. [Google Scholar] [CrossRef]
- Park, J.S.; Lee, E.H.; Park, N.R.; Choi, Y.H. Mental Health of Nurses Working at a Government-designated Hospital during a MERS-CoV Outbreak: A Cross-sectional Study. Arch. Psychiatr. Nurs. 2018, 32, 2–6. [Google Scholar] [CrossRef]
- Xiang, Y.T.; Yu, X.; Ungvari, G.S.; Correll, C.U.; Chiu, H.F. Outcomes of SARS survivors in China: Not only physical and psychiatric co-morbidities. East Asian Arch. Psychiatry 2014, 24, 37–38. [Google Scholar]
- Li, W.; Yang, Y.; Liu, Z.H.; Zhao, Y.J.; Zhang, Q.; Zhang, L.; Cheung, T.; Xiang, Y.T. Progression of Mental Health Services during the COVID-19 Outbreak in China. Int. J. Biol. Sci. 2020, 16, 1732–1738. [Google Scholar] [CrossRef] [PubMed]
- Williams, P.G.; Tinajero, R.; Suchy, Y. Executive Functioning and Health. In Oxford Handbooks Online; Oxford University Press: Oxford, UK, November 2017; pp. 1–53, Online publication. [Google Scholar]
- Walton, M.; Murray, E.; Christian, M.D. Mental Health Care for Medical Staff and Affiliated Healthcare Workers during the COVID-19 Pandemic. Eur. Heart J. Acute Cardiovasc. Care 2020, 9, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.; Hu, T.; Hu, B.; Jin, C.; Wang, G.; Xie, C.; Chen, S. Prevalence and Correlates of PTSD and Depressive Symptoms One Month after the Outbreak of the COVID-19 Epidemic in a Sample of Home-Quarantined Chinese University Students. J. Affect. Disord. 2020, 274, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Chiu, W.T.; Demler, O.; Merikangas, K.R.; Walters, E.E. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 617–627. [Google Scholar] [CrossRef] [PubMed]
- Olff, M. Sex and gender differences in post-traumatic stress disorder: An update. Eur. J. Psychotraumatol. 2017, 8 (Suppl. S4), 1351204. [Google Scholar] [CrossRef]
- Carmassi, C.; Gesi, C.; Corsi, M.; Cremone, I.M.; Bertelloni, C.A.; Massimetti, E.; Olivieri, M.C.; Conversano, C.; Santini, M.; Dell’Osso, L. Exploring PTSD in emergency operators of a major University Hospital in Italy: A preliminary report on the role of gender, age, and education. Ann. Gen. Psychiatry 2018, 17, 17. [Google Scholar] [CrossRef] [PubMed]
- Remes, O.; Brayne, C.; Van der Linde, R.; Lafortune, L. A systematic reviews of reviews on the prevalence of anxiety disorders in adult populations. Brain Behav. 2016, 6, e00497. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total Mean ± SD; Range | Female Mean ± SD, Range | Male Mean ± SD, Range | ||
|---|---|---|---|---|
| Age (years) | 50 ± 9.9; 28–66 | 51 ± 9.8; 28–66 | 45.7 ± 10.1; 30–65 | |
| N; % | N; % | N; % | * p | |
| Hospital staff roles | ||||
| 58; 55 | 42; 53 | 16; 59 | 0.000 |
| 7; 7 | 6; 8 | 1; 1 | 0.061 |
| 12; 11 | 8; 10 | 4; 15 | 0.248 |
| 13; 12 | 12; 15 | 1; 4 | 0.002 |
| 1; 1 | 1; 1 | 0; 0 | 0.563 |
| 15; 14 | 10; 13 | 5; 19 | 0.196 |
| Questionnaires | (N = 44) Mean ± SD | Males (N = 12) Mean ± SD | Females (N = 32) Mean ± SD | Normative Data (Males, Mean ± SD) | Normative Data (Females, Mean ± SD) |
|---|---|---|---|---|---|
| BDI | 9.7 ± 2.1 | 8.6 ± 3.1 | 10.8 ± 4.3 | < 10 | < 14 |
| STAY-Y1 | 42.7 ± 11.4 | 38.5 ± 6.4 | 44.7 ± 7.4 * | 36 ± 9.7 | 39.9 ± 11 |
| STAY-Y2 | 42.1 ± 8.7 | 33.6 ± 7.6 | 40.1 ± 8.2 | 36.5 ± 9.6 | 41.3 ± 9.7 |
| Total | Female | Male | |
|---|---|---|---|
| N; % | N; % | N; % | |
| Health worker’s relationship with Occupational Preventive Medicine | |||
| 65; 61 | 51; 65 | 14; 52 |
| 15; 14 | 11; 14 | 4; 15 |
| 6; 6 | 2; 2 | 4; 15 |
| 20; 19 | 15; 19 | 5;18 |
| New treatment intervention following case discussion | |||
| 63; 60 | 48; 61 | 15; 56 |
| 30; 28 | 24; 30 | 6; 22 |
| 13; 12 | 7; 9 | 6; 22 |
| Number of PsicoCovid19 Psychiatric Visits During Phase 1 | Work Temporary Exclusion | Sars-Cov-2 Infection | Family Members Died for COVID-19 | Psychosocial Risk Factors Reported | First Access Characteristics |
|---|---|---|---|---|---|
| 3 workers: 6 access | 1 worker: decompensated diabetes | 1 worker: asynomatic/ still positive (3 months of self isolation) | 1 worker: husband | Excessive workloads | 1 worker: Agitation and insomnia during hospitalization |
| 5 workers: 4 access | 2 workers: severe lung disease | 2 workers: mild symptoms (now negative) | Conflicting demands | 2 workers: panic attacks, somatization, insomnia | |
| 10 workers: 3 access | 1 worker: severe oncological disease | 1worker: Hospitalized in ICU (still positive) | Lack of involvement in making decisions that affect the worker | 1 worker: O-C symptoms related to possible contagion (temperature and saturation measurement) | |
| 23 workers: 2 access | Poorly managed organisational change | ||||
| Difficulty managing patients anxiety and loneliness | |||||
| 24 workers: 1 access | Job insecurity | ||||
| Fear of contagion |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buselli, R.; Baldanzi, S.; Corsi, M.; Chiumiento, M.; Del Lupo, E.; Carmassi, C.; Dell’Osso, L.; Cristaudo, A. Psychological Care of Health Workers during the COVID-19 Outbreak in Italy: Preliminary Report of an Occupational Health Department (AOUP) Responsible for Monitoring Hospital Staff Condition. Sustainability 2020, 12, 5039. https://doi.org/10.3390/su12125039
Buselli R, Baldanzi S, Corsi M, Chiumiento M, Del Lupo E, Carmassi C, Dell’Osso L, Cristaudo A. Psychological Care of Health Workers during the COVID-19 Outbreak in Italy: Preliminary Report of an Occupational Health Department (AOUP) Responsible for Monitoring Hospital Staff Condition. Sustainability. 2020; 12(12):5039. https://doi.org/10.3390/su12125039
Chicago/Turabian StyleBuselli, Rodolfo, Sigrid Baldanzi, Martina Corsi, Martina Chiumiento, Elena Del Lupo, Claudia Carmassi, Liliana Dell’Osso, and Alfonso Cristaudo. 2020. "Psychological Care of Health Workers during the COVID-19 Outbreak in Italy: Preliminary Report of an Occupational Health Department (AOUP) Responsible for Monitoring Hospital Staff Condition" Sustainability 12, no. 12: 5039. https://doi.org/10.3390/su12125039
APA StyleBuselli, R., Baldanzi, S., Corsi, M., Chiumiento, M., Del Lupo, E., Carmassi, C., Dell’Osso, L., & Cristaudo, A. (2020). Psychological Care of Health Workers during the COVID-19 Outbreak in Italy: Preliminary Report of an Occupational Health Department (AOUP) Responsible for Monitoring Hospital Staff Condition. Sustainability, 12(12), 5039. https://doi.org/10.3390/su12125039