
Lipidomic Analysis to Assess the Correlation between Ceramides, Stress Hyperglycemia, and HbA1c in Acute Myocardial Infarction

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Population Characteristics and Data Acquisition
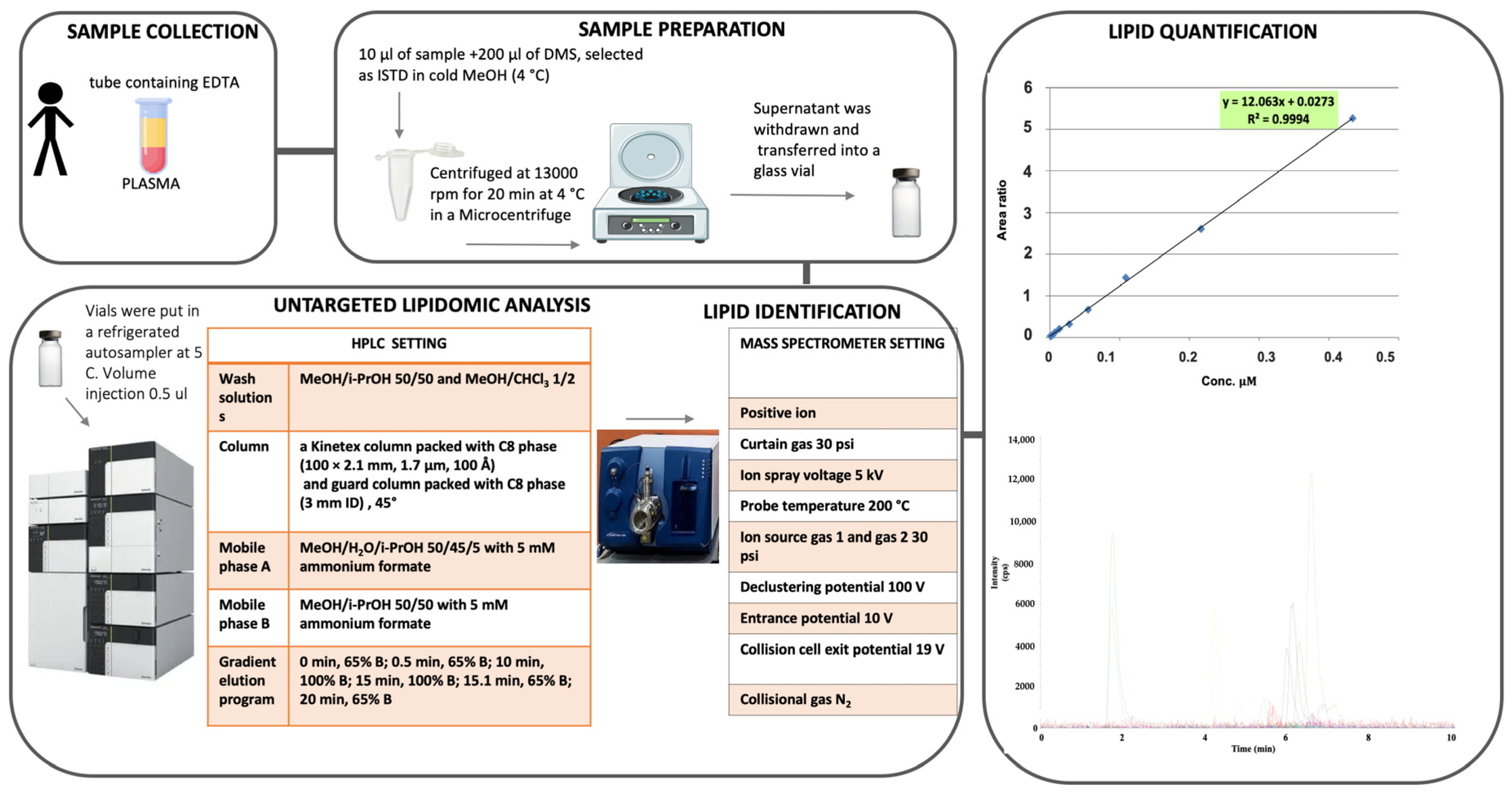
4.2. Plasma Processing and HPLC-MS/MS Analysis
4.3. Statistical Analysis
5. Limitations of the Study
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gaggini, M.; Sabatino, L.; Vassalle, C. Conventional and innovative methods to assess oxidativestressbiomarkersintheclinicalcardiovascular setting. Biotechniques 2020, 68, 223–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michelucci, E.; Di Giorgi, N.; Finamore, F.; Smit, J.M.; Scholte, A.J.H.A.; Signore, G.; Rocchiccioli, S. Lipid biomarkers in statin users with coronary artery disease annotated by coronary computed tomography angiography. Sci. Rep. 2021, 11, 12899. [Google Scholar] [CrossRef] [PubMed]
- Masoodi, M.; Gastaldelli, A.; Hyötyläinen, T.; Arretxe, E.; Alonso, C.; Gaggini, M.; Brosnan, J.; Anstee, Q.M.; Millet, O.; Ortiz, P.; et al. Metabolomics and lipidomics in NAFLD: Biomarkers and non-invasive diagnostic tests. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 835–856. [Google Scholar] [CrossRef] [PubMed]
- Hilvo, M.; Vasile, V.C.; Donato, L.J.; Hurme, R.; Laaksonen, R. Ceramides and Ceramide Scores: Clinical Applications for Cardiometabolic Risk Stratification. Front. Endocrinol. Lausanne 2020, 11, 570628. [Google Scholar] [CrossRef]
- Michelucci, E.; Rocchiccioli, S.; Gaggini, M.; Ndreu, R.; Berti, S.; Vassalle, C. Ceramides and Cardiovascular Risk Factors, Inflammatory Parameters and Left Ventricular Function in AMI Patients. Biomedicines 2022, 10, 429. [Google Scholar] [CrossRef]
- Capes, S.E.; Hunt, D.; Malmberg, K.; Gerstein, H.C. Stress hyperglycaemia and increased risk of death after myocardial infarction in patients with and without diabetes: A systematic overview. Lancet 2000, 355, 773–778. [Google Scholar] [CrossRef]
- Singh, K.; Hibbert, B.; Singh, B.; Carson, K.; Premaratne, M.; Le May, M.; Chong, A.Y.; Arstall, M.; So, D. Meta-Analysis of admission hyperglycaemia in acutemyocardial infarction patients treated with primary angioplasty: A cause or a marker of mortality? Eur. Hear. J.-Cardiovasc. Pharmacother. 2015, 1, 220–228. [Google Scholar] [CrossRef] [Green Version]
- Demarchi, A.; Cornara, S.; Somaschini, A.; Fortuni, F.; Mandurino-Mirizzi, A.; Crimi, G.; Ferlini, M.; Gnecchi, M.; De Servi, S.; Visconti, L.O.; et al. Has hyperglycemia a different prognostic role in STEMI patients with or without diabetes? Nutr. Metab. Cardiovasc. Dis. 2021, 31, 528–531. [Google Scholar] [CrossRef]
- Chatzianagnostou, K.; Guiducci, L.; Paradossi, U.; De Caterina, A.R.; Mazzone, A.; Berti, S.; Vassalle, C. The role of prediabetes as a predictive factor for the outcomes in patients with stemi. Which is the right range of glycated hemoglobin to adopt in this setting? Appl. Sci. 2021, 11, 5518. [Google Scholar] [CrossRef]
- Gaggini, M.; Pingitore, A.; Vassalle, C. Plasma ceramides pathophysiology, measurements, challenges, and opportunities. Metabolites 2021, 11, 719. [Google Scholar] [CrossRef]
- Sigruener, A.; Kleber, M.E.; Heimerl, S.; Liebisch, G.; Schmitz, G.; Maerz, W. Glycerophospholipid and sphingolipid species and mortality: The Ludwigshafen risk and cardiovascular health (LURIC) study. PLoS ONE 2014, 9, e85724. [Google Scholar] [CrossRef] [Green Version]
- Laaksonen, R.; Ekroos, K.; Sysi-Aho, M.; Hilvo, M.; Vihervaara, T.; Kauhanen, D.; Suoniemi, M.; Hurme, R.; März, W.; Scharnagl, H.; et al. Plasma ceramides predict cardiovascular death in patients with stable coronary artery disease and acute coronary syndromes beyond LDL-cholesterol. Eur. Heart J. 2016, 37, 1967–1976. [Google Scholar] [CrossRef] [Green Version]
- Scherer, P.E.; Hill, J.A. Obesity, diabetes, and cardiovascular diseases. Circ. Res. 2016, 118, 1703–1705. [Google Scholar] [CrossRef] [Green Version]
- Boon, J.; Hoy, A.J.; Stark, R.; Brown, R.D.; Meex, R.C.; Henstridge, D.C.; Schenk, S.; Meikle, P.J.; Horowitz, J.F.; Kingwell, B.A.; et al. Ceramides contained in LDL are elevated in type 2 diabetes and promote inflammation and skeletal muscle insulin resistance. Diabetes 2013, 62, 401–410. [Google Scholar] [CrossRef] [Green Version]
- Cao, R.; Fang, Z.; Li, S.; Xu, M.; Zhang, J.; Han, D.; Hu, W.; Yan, L.; Wang, Y.; Fan, L.; et al. Circulating Ceramide: A New Cardiometabolic Biomarker in Patients With Comorbid Acute Coronary Syndrome and Type 2 Diabetes Mellitus. Front. Physiol. 2020, 11, 1104. [Google Scholar] [CrossRef]
- Fang, Z.; Pyne, S.; Pyne, N.J. Ceramide and sphingosine 1-phosphate in adipose dysfunction. Prog. Lipid Res. 2019, 74, 145–159. [Google Scholar] [CrossRef] [Green Version]
- Deedwania, P.; Kosiborod, M.; Barrett, E.; Ceriello, A.; Isley, W.; Mazzone, T.; Raskin, P. Hyperglycemia and acute coronary syndrome: A scientific statement from the american heart association diabetes committee of the council on nutrition, physical activity, and metabolism. Circulation 2008, 117, 1610–1619. [Google Scholar] [CrossRef]
- Angeli, F.; Reboldi, G.; Poltronieri, C.; Lazzari, L.; Sordi, M.; Garofoli, M.; Bartolini, C.; Verdecchia, P. Hyperglycemia in acute coronary syndromes: From mechanisms to prognostic implications. Ther. Adv. Cardiovasc. Dis. 2015, 9, 412–424. [Google Scholar] [CrossRef]
- Liu, Y.; Yang, Y.M.; Zhu, J.; Tan, H.Q.; Liang, Y.; Li, J.D. Haemoglobin A1c, acute hyperglycaemia and short-term prognosis in patients without diabetes following acute ST-segment elevation myocardial infarction. Diabet. Med. 2012, 29, 1493–1500. [Google Scholar] [CrossRef]
- Marfella, R.; Di Filippo, C.; Portoghese, M.; Ferraraccio, F.; Rizzo, M.R.; Siniscalchi, M.; Musacchio, E.; D’Amico, M.; Rossi, F.; Paolisso, G. Tight Glycemic Control Reduces Heart Inflammation and Remodeling During Acute Myocardial Infarction in Hyperglycemic Patients. J. Am. Coll. Cardiol. 2009, 53, 1425–1436. [Google Scholar] [CrossRef]
- Knapp, K.M.; English, B.K. Ceramide-mediated stimulation of inducible nitric oxide synthase (iNOS) and tumor necrosis factor (TNF) accumulation in murine macrophages requires tyrosine kinase activity. J. Leukoc. Biol. 2000, 67, 735–741. [Google Scholar] [CrossRef] [PubMed]
- Choi, R.H.; Tatum, S.M.; Symons, J.D.; Summers, S.A.; Holland, W.L. Ceramides and other sphingolipids as drivers of cardiovascular disease. Nat. Rev. Cardiol. 2021, 18, 701–711. [Google Scholar] [CrossRef] [PubMed]
- Chaurasia, B.; Summers, S.A. Ceramides-Lipotoxic Inducers of Metabolic Disorders. Trends Endocrinol. Metab. 2015, 26. [Google Scholar] [CrossRef] [PubMed]
- Summers, S.A.; Chaurasia, B.; Holland, W.L. Metabolic Messengers: Ceramides. Nat. Metab. 2019, 1, 1051–1058. [Google Scholar] [CrossRef] [PubMed]
- Mazzone, A.; Clemente, A.; Chiappino, D.; Berti, S.; Vassalle, C. Double Face of Statins at the Crossroad of Coronary Atherosclerotic Plaque and Aortic Valve Calcification? JACC Cardiovasc. Imaging 2018, 11, 1930–1931. [Google Scholar] [CrossRef]
- Mazzone, A.; Clemente, A.; Sbrana, S.; Latta, D.D.; Chiappino, S.; Berti, S.; Chiappino, D.; Vassalle, C. Statins association with calcification in coronary plaque and heart valves: A possible different clinical significance: Montignoso HEart and Lung Project (MHELP) study preliminary data in primary cardiovascular prevention. Eur. J. Prev. Cardiol. 2021, 28, e15–e17. [Google Scholar] [CrossRef]
- Tarasov, K.; Ekroos, K.; Suoniemi, M.; Kauhanen, D.; Sylvänne, T.; Hurme, R.; Gouni-Berthold, I.; Berthold, H.K.; Kleber, M.E.; Laaksonen, R.; et al. Molecular lipids identify cardiovascular risk and are efficiently lowered by simvastatin and PCSK9 deficiency. J. Clin. Endocrinol. Metab. 2014, 99, E45–E52. [Google Scholar] [CrossRef] [Green Version]
- Ng, T.W.K.; Ooi, E.M.M.; Watts, G.F.; Chan, D.C.; Weir, J.M.; Meikle, P.J.; Barrett, P.H.R. Dose-dependent effects of rosuvastatin on the plasma sphingolipidome and phospholipidome in the metabolic syndrome. J. Clin. Endocrinol. Metab. 2014, 99, E2335–E2340. [Google Scholar] [CrossRef] [Green Version]
- Chaurasia, B.; Tippetts, T.S.; Monibas, R.M.; Liu, J.; Li, Y.; Wang, L.; Wilkerson, J.L.; Sweeney, C.R.; Pereira, R.F.; Sumida, D.H.; et al. Targeting a ceramide double bond improves insulin resistance and hepatic steatosis. Science 2019, 365, 386–392. [Google Scholar] [CrossRef]
- Dekker, M.J.; Baker, C.; Naples, M.; Samsoondar, J.; Zhang, R.; Qiu, W.; Sacco, J.; Adeli, K. Inhibition of sphingolipid synthesis improves dyslipidemia in the diet-induced hamster model of insulin resistance: Evidence for the role of sphingosine and sphinganine in hepatic VLDL-apoB100 overproduction. Atherosclerosis 2013, 228, 98–109. [Google Scholar] [CrossRef]
- Park, T.S.; Rosebury, W.; Kindt, E.K.; Kowala, M.C.; Panek, R.L. Serine palmitoyltransferase inhibitor myriocin induces the regression of atherosclerotic plaques in hyperlipidemic ApoE-deficient mice. Pharmacol. Res. 2008, 58, 45–51. [Google Scholar] [CrossRef]
- Glaros, E.N.; Kim, W.S.; Quinn, C.M.; Jessup, W.; Rye, K.A.; Garner, B. Myriocin slows the progression of established atherosclerotic lesions in apolipoprotein E gene knockout mice. J. Lipid Res. 2008, 49, 324–331. [Google Scholar] [CrossRef] [Green Version]
- Knapp, M.; Lisowska, A.; Knapp, P.; Baranowski, M. Dose-dependent effect of aspirin on the level of sphingolipids in human blood. Adv. Med. Sci. 2013, 58, 274–281. [Google Scholar] [CrossRef] [Green Version]
- Gaggini, M.; Ndreu, R.; Michelucci, E.; Rocchiccioli, S.; Vassalle, C. Ceramides as Mediators of Oxidative Stress and Inflammation in Cardiometabolic Disease. Int. J. Mol. Sci. 2022, 23, 2719. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D.; Corbett, S.; Chettibi, M.; Hayrapetyan, H.; et al. Fourth Universal Definition of Myocardial Infarction. Circulation 2018, 138, e618–e651. [Google Scholar] [CrossRef]
- Mansour, A.A.; Wanoose, H.L. Acute phase hyperglycemia among patients hospitalized with acute coronary syndrome: Prevalence and prognostic significance. Oman Med. J. 2011, 26, 85–90. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variable | Overall Population n = 140 | noT2D n = 102 | AH n = 12 | T2D n = 26 | p Value (χ2 Test) |
|---|---|---|---|---|---|
| Females | 37 (26) | 23 (22) | 4 (33) | 10 (38) | 0.52 |
| Age (>69 years 50th percentile) | 63 (45) | 40 (35) | 7 (58) | 16 (61) | 0.38 |
| Hypertension | 88 (63) | 59 (58) | 7 (58) | 22 (81) | 0.18 |
| Dyslipidemia | 69 (49) | 45 (44) | 7 (58) | 17 (65) | 0.53 |
| Smoking habit | 33 (24) | 28 (27) | 2 (17) | 3 (11) | 0.06 |
| Obesity | 23 (16) | 9 (9) | 4 (33) | 10 (38) | 0.048 |
| Ceramide | 18:1/18:0 | 18:1/20:0 | 18:1/22:0 | 18:1/23:0 | 18:1/24:0 | 18:1/24:1 | 18:1/25:0 | 18:2/22:0 |
|---|---|---|---|---|---|---|---|---|
| 18:1/16:0 | 0.8 <0.001 | 0.85 <0.001 | 0.71 <0.001 | 0.62 <0.001 | 0.54 <0.001 | 0.83 <0.001 | 0.51 <0.001 | 0.6 <0.001 |
| 18:1/18:0 | 0.91 <0.001 | 0.72 <0.001 | 0.62 <0.001 | 0.46 <0.001 | 0.8 <0.001 | 0.4 <0.001 | 0.57 <0.001 | |
| 18:1/20:0 | 0.86 <0.001 | 0.77 <0.001 | 0.64 <0.001 | 0.88 <0.001 | 0.6 <0.001 | 0.6 <0.001 | ||
| 18:1/22:0 | 0.9 <0.001 | 0.88 <0.001 | 0.82 <0.001 | 0.65 <0.001 | 0.91 <0.001 | |||
| 18:1/23:0 | 0.84 <0.001 | 0.77 <0.001 | 0.76 <0.001 | 0.88 <0.001 | ||||
| 18:1/24:0 | 0.63 <0.001 | 0.74 <0.001 | 0.77 <0.001 | |||||
| 18:1/24:1 | 0.63 <0.001 | 0.7 <0.001 | ||||||
| 18:1/25:0 | 0.53 <0.001 |
| Parameters | Ceramide Species | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 18:1/16:0 | 18:1/18:0 | 18:1/20:0 | 18:1/22:0 | 18:1/23:0 | 18:1/24:0 | 18:1/24:1 | 18:1/25:0 | 18:2/22:0 | 18:1/16:0 18:1/24:0 | 18:1/18:0 18:1/24:0 | 18:1/24:1 18:1/24:0 | |
| Females vs. males | 1.01 (0.38) vs. 0.89 (0.25) = 0.03 | 0.4 (0.26) vs. 0.3 (0.146) = 0.005 | 0.255 (0.146) vs. 0.21 (0.09) = 0.042 | 1.36 (0.6) vs. 1.29 (0.52) ns | 1 (0.44) vs. 1 (0.41) ns | 2.8 ( 1.1) vs. 3 (1.2) ns | 1.51 (0.7) vs. 1.34 (0.51) ns | 0.14 (0.09) vs. 0.13 (0.08) ns | 0.25 (0.13) vs. 0.22 (0.14) ns | 0.38 (0.127) vs. 0.323 (0.120) = 0.018 | 0.144 (0.066) vs. 0.105 (0.051) < 0.001 | 0.548 (0.174) vs. 0.475 (0.0165) = 0.027 |
| Age < 69 (50th percentile) vs. >69 | 0.86 (0.25) vs. 0.99 (0.33) = 0.016 | 0.31 (0.16) vs. 0.35 (0.22) ns | 0.22 (0.1) vs. 0.23 (0.13) ns | 1.34 (0.52) vs. 1.28 (0.56) ns | 1 (0.4) vs. 0.97 (0.43) ns | 3.14 (1.1) vs. 2.77 (1.1) ns | 1.30 (0.5) vs. 1.48 (0.63) ns | 0.136 (0.09) vs. 0.132 (0.08) ns | 0.22 (0.13) vs. 0.23 (0.14) ns | 0.288 (0.08) vs. 0.39 (0.14) < 0.001 | 0.1 (0.049) vs. 0.13 (0.063) = 0.004 | 0.428 (0.116) vs. 0.563 (0.188) < 0.001 |
| No hypertension vs. hypertension | 0.9 (0.16) vs. 0.94 (0.34) ns | 0.3 (0.13) vs. 0.34 (0.22) ns | 0.21 (0.08) vs. 0.23 (0.12) ns | 1.22 (0.4) vs. 1.3 (0.6) ns | 0.9 (0.28) vs. 1.01 (0.46) ns | 2.8 (0.9) vs. 3.0 (1.2) ns | 1.28 (0.29) vs. 1.43 (0.65) ns | 0.12 (0.06) vs. 0.14 (0.09) ns | 0.21 (0.1) vs. 0.23 (0.15) ns | 0.356 (0.13) vs. 0.335 (0.12) ns | 0.121 (0.06) vs. 0.115 (0.06) ns | 0.51 (0.19) vs. 0.49 (0.16) ns |
| No dyslipidemia vs. dyslipidemia | 0.88 (0.27) vs. 0.96 (0.32) ns | 0.29 (0.16) vs. 0.36 (0.2) ns | 0.2 (0.1) vs. 0.24 (0.12) ns | 1.26 (0.5) vs. 1.34 (0.6) ns | 0.96 (0.4) vs. 1.0 (0.4) ns | 2.9 (1.1) vs. 3.0 (1.2) ns | 1.35 (0.6) vs. 1.42 (0.6) ns | 0.14 (0.09) vs. 0.13 (0.08) ns | 0.205 (0.11) vs. 0.239 (0.15) ns | 0.325 (0.121) vs. 0.353 (0.127) ns | 0.105 (0.049) vs. 0.126 (0.063) = 0.04 | 0.48 (0.18) vs. 0.51 (0.16) ns |
| No smoking habit vs. smoking habit | 0.93 (0.33) vs. 0.91 (0.21) ns | 0.33 (0.21) vs. 0.32 (0.14) ns | 0.22 (0.12) vs. 0.23 (0.08) ns | 1.29 (0.6) vs. 1.35 (0.4) ns | 1 (0.5) vs. 1 (0.3) ns | 2.9 (1.1) vs. 3.2 (1.2) ns | 1.41 (0.63) vs. 1.33 (0.38) ns | 0.13 (0.1) vs. 0.13 (0.07) ns | 0.23 (0.15) vs. 0.21 (0.1) ns | 0.353 (0.13) vs. 0.311 (0.1) ns | 0.12 (0.06) vs. 0.11 (0.05) ns | 0.52 (0.17) vs. 0.45 (0.15) ns |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gaggini, M.; Michelucci, E.; Ndreu, R.; Rocchiccioli, S.; Chatzianagnostou, K.; Berti, S.; Vassalle, C. Lipidomic Analysis to Assess the Correlation between Ceramides, Stress Hyperglycemia, and HbA1c in Acute Myocardial Infarction. Molecules 2023, 28, 716. https://doi.org/10.3390/molecules28020716
Gaggini M, Michelucci E, Ndreu R, Rocchiccioli S, Chatzianagnostou K, Berti S, Vassalle C. Lipidomic Analysis to Assess the Correlation between Ceramides, Stress Hyperglycemia, and HbA1c in Acute Myocardial Infarction. Molecules. 2023; 28(2):716. https://doi.org/10.3390/molecules28020716
Chicago/Turabian StyleGaggini, Melania, Elena Michelucci, Rudina Ndreu, Silvia Rocchiccioli, Kyriazoula Chatzianagnostou, Sergio Berti, and Cristina Vassalle. 2023. "Lipidomic Analysis to Assess the Correlation between Ceramides, Stress Hyperglycemia, and HbA1c in Acute Myocardial Infarction" Molecules 28, no. 2: 716. https://doi.org/10.3390/molecules28020716