
Atypically Displaced Meniscal Tears: An Educational Review with Focus on MRI and Arthroscopy

 ,
,  , , , , ,
, , , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Basic Interpretation of Meniscus Tear
2.1. Imaging of Menisci
2.2. MRI and Meniscal Tears
MRI Reporting Recommendations
- (1)
- Tear depth classifies tears as complete if they penetrate both the superior and inferior meniscal surfaces and partial if they penetrate only one of them.
- (2)
- The Cooper zone categorization of meniscal tears is used to assess the rim width, or circumferential location, based on the extent to which the tear spreads centrally into the meniscus. Cooper Zone 1 (rim width < 3 mm; outer third), Cooper Zone 2 (rim width 3 mm to <5 mm; middle third), and Cooper Zone 3 (rim width ≥ 5 mm; inner third) are the three areas into which tears are classified. Evidence of vascularity up to 3 mm from the meniscus’s perimeter led to the selection of the 3 mm threshold. A tear is graded based on the outermost zone involved (if multiple zones are involved), such as a radial tear. It is not recommended to use historical “red-red,” “red-white,” or “white-white” nomenclature.
- (3)
- The meniscus is divided into thirds by radial location topographic classification, which classifies tears according to their extension into the anterior, body, or posterior zones. Multiple zones can be torn at the same time; for example, a full bucket-handle tear would affect all three zones. Alternatively, unless a radial tear crosses the mid-body, the radial location can be classified as either anterior or posterior, splitting the meniscus in half.
- (4)
- If lateral meniscal tears reach entirely or partially in front of the popliteal hiatus, they are rated as central to the hiatus.
- (5)
- Tear patterns might be horizontal, radial, vertical flap, horizontal flap, longitudinal–vertical (which incorporates a bucket-handle tear as an extension), or complex. With the exception of complex tears, which include two or more tear patterns, the main tear pattern should be mentioned.
- (6)
- Whether the meniscal tissue appears degenerative, nondegenerative, or unknown is referred to as tissue quality. Degenerative meniscal tissue is characterized by softening, fibrillations, cavitations, and/or numerous tear patterns.
- (7)
- The length of the meniscal tear that extends into its surface is called the tear length (in millimeters, as determined using an arthroscopy ruler or probe). The measured tear length does not account for confined tears or intermeniscal degeneration.
- (8)
- The percentage of meniscal tissue surface area that is removed arthroscopically is known as the “percentage of the meniscus excised.” This percentage can be calculated quantitatively and represented graphically by crosshatching the excised tissue on a diagram.
2.3. Diagnostic Arthroscopy
3. Exemplificative Cases: MRI and Arthroscopy
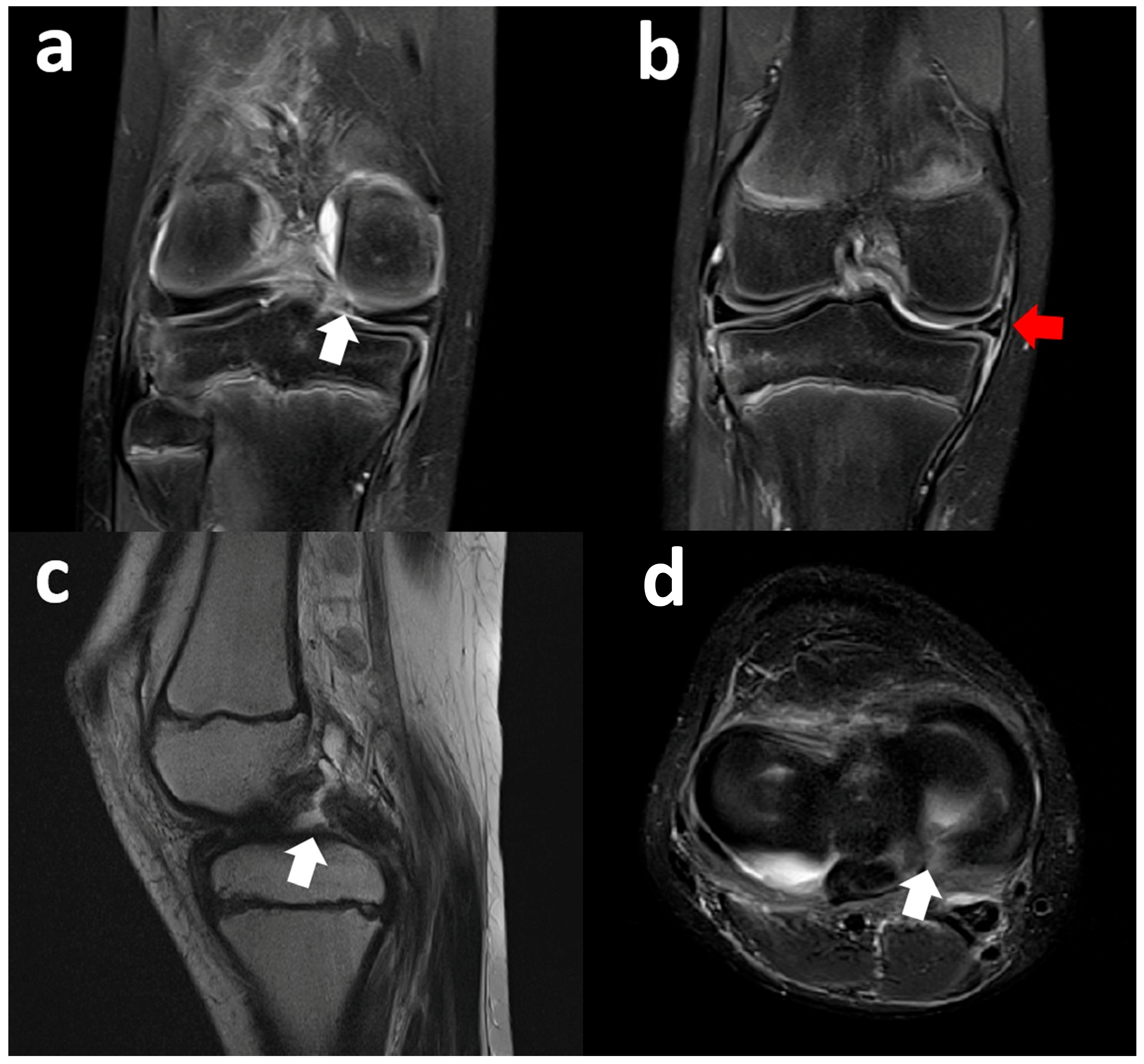
3.1. Medial Meniscus Flap Under the Medial Collateral Ligament
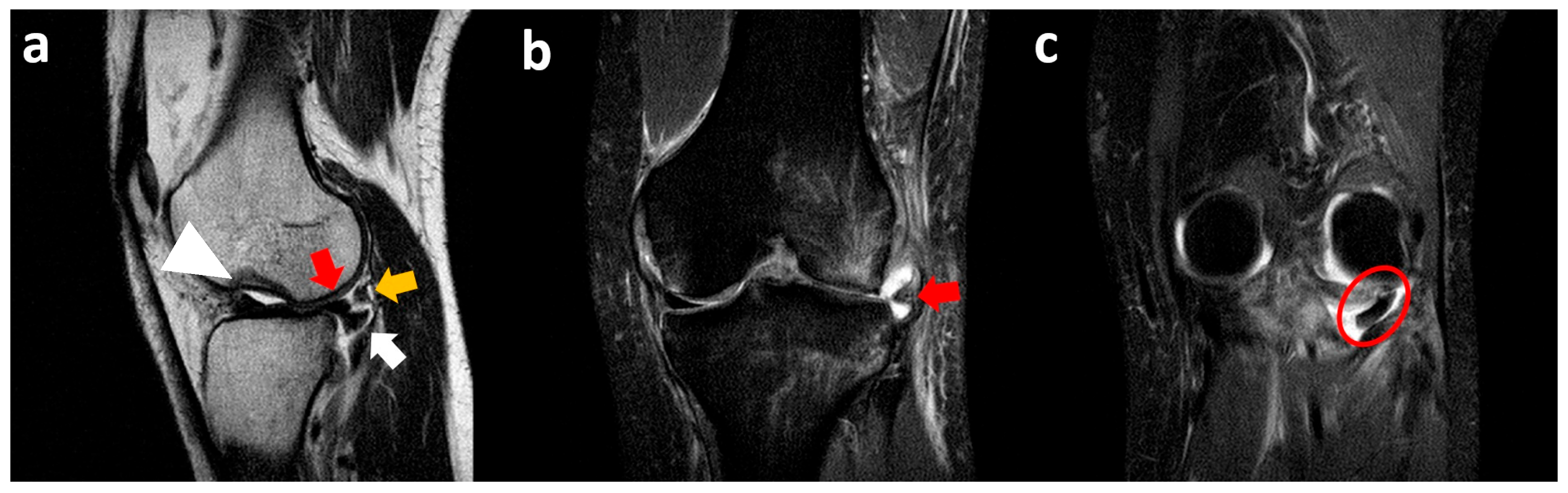
3.2. Medial Meniscus Radial Tear with Flipped Body
3.3. Medial Meniscus Posterior Root Tear with Extrusion
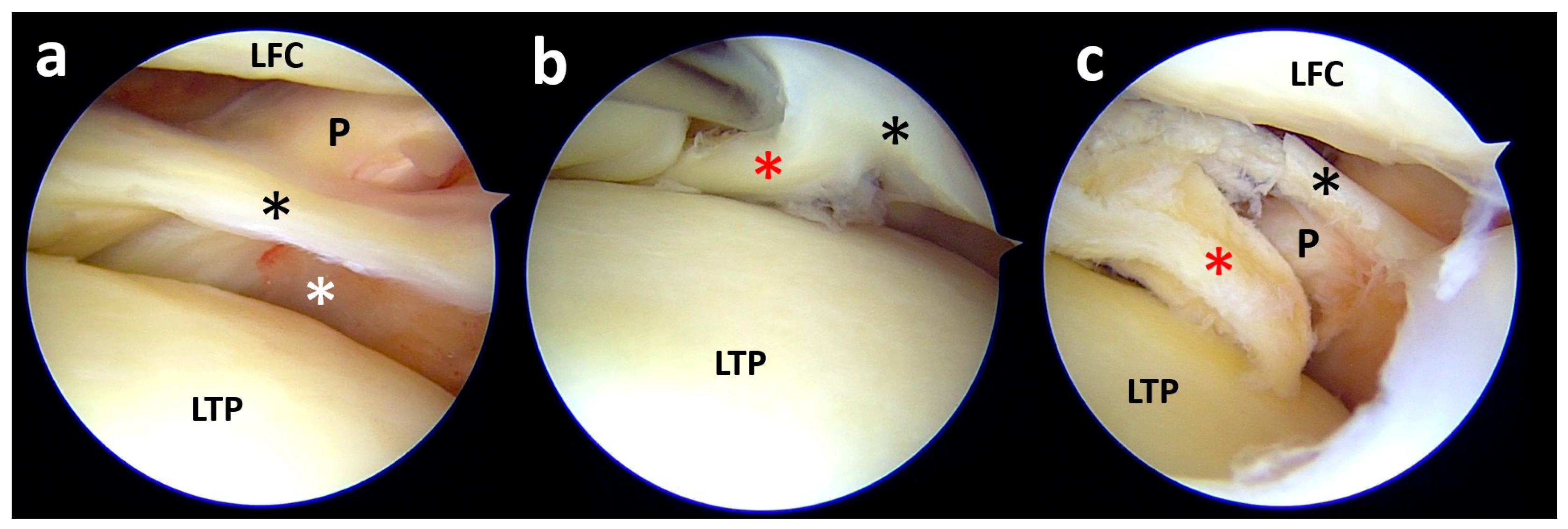
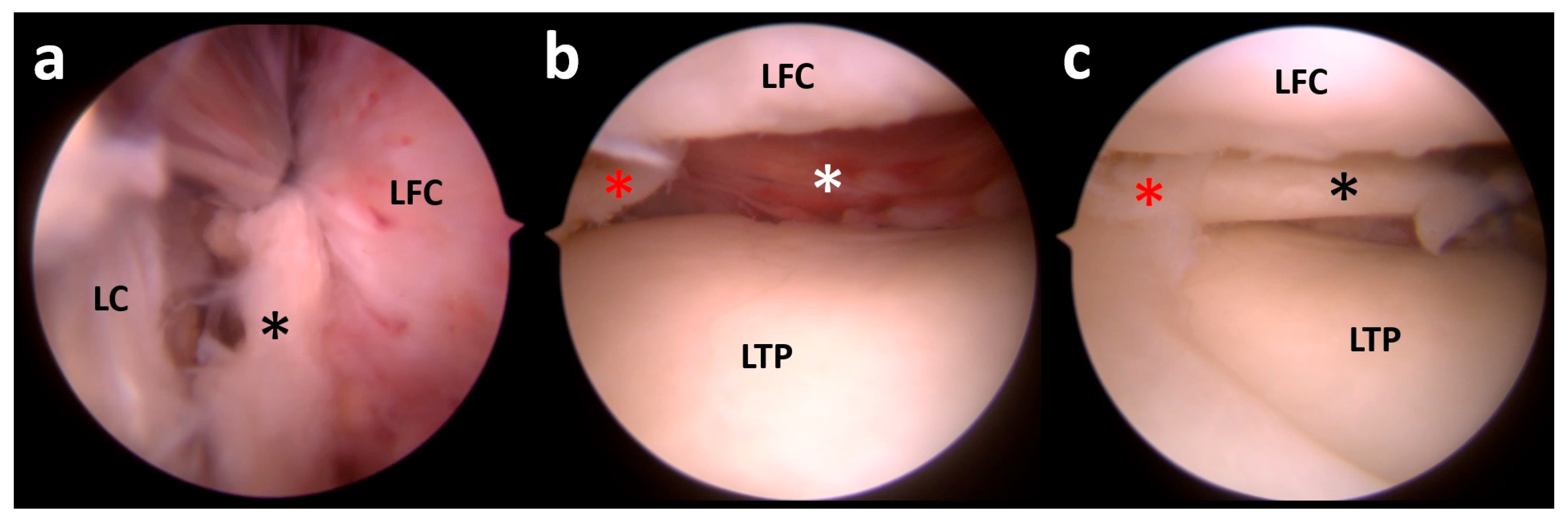
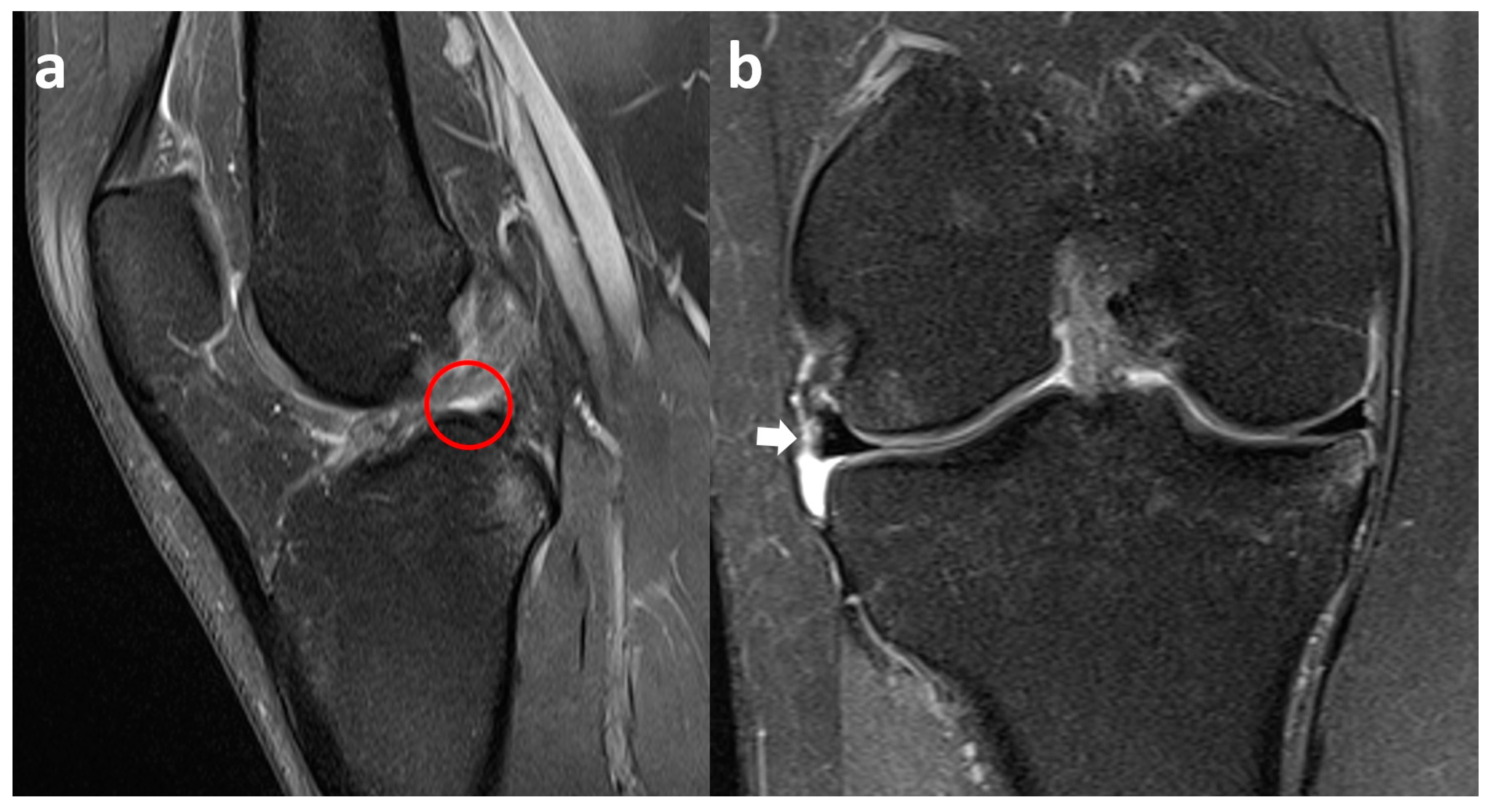
3.4. Lateral Meniscus Flap in Popliteus Recess
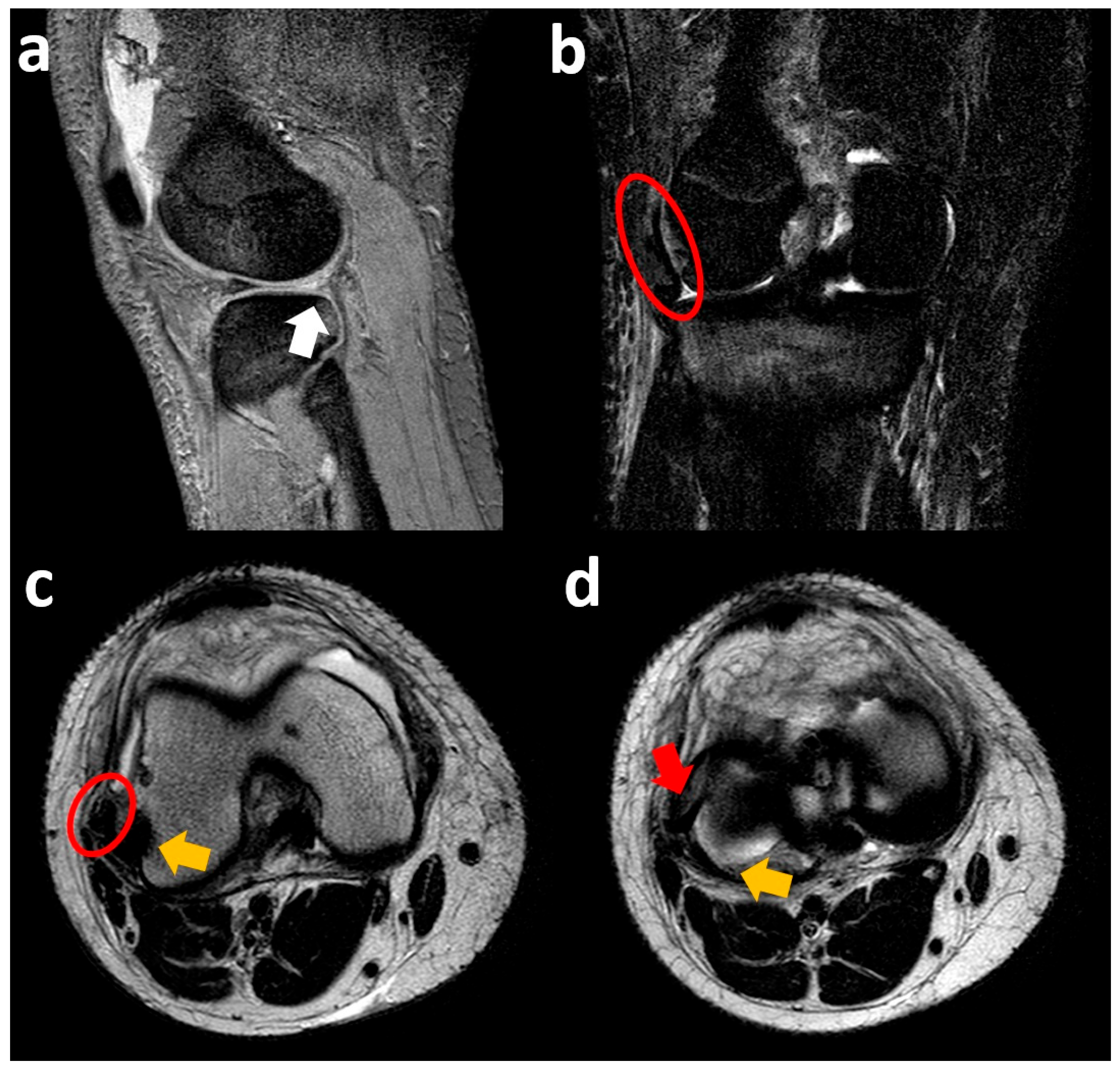
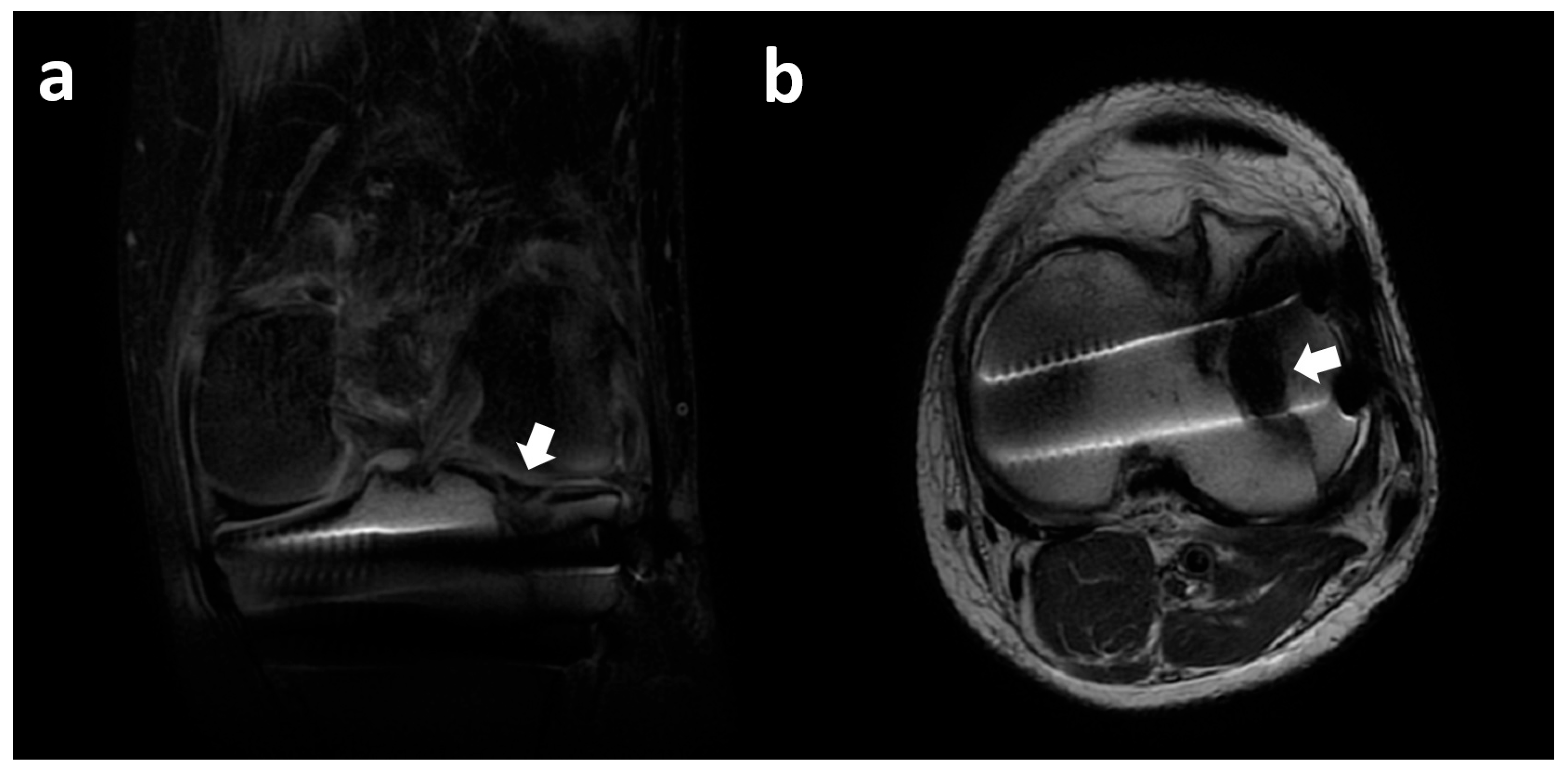
3.5. Lateral Meniscus Flipped in the Lateral Gutter
3.6. Lateral Meniscus Posterior Root Tear with Extrusion
3.7. Lateral Meniscus Body Within Tibial Plateau Fracture
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vande Berg, B.C.; Malghem, J.; Poilvache, P.; Maldague, B.; Lecouvet, F.E. Meniscal tears with fragments displaced in notch and recesses of knee: MR imaging with arthroscopic comparison. Radiology 2005, 234, 842–850. [Google Scholar] [CrossRef] [PubMed]
- Lecouvet, F.; Van Haver, T.; Acid, S.; Perlepe, V.; Kirchgesner, T.; Vande Berg, B.; Triqueneaux, P.; Denis, M.L.; Thienpont, E.; Malghem, J. Magnetic resonance imaging (MRI) of the knee: Identification of difficult-to-diagnose meniscal lesions. Diagn. Interv. Imaging 2018, 99, 55–64. [Google Scholar] [CrossRef]
- Nisar, O. Pattern of Meniscal Tears in Stable Knee. J. Med. Sci. Clin. Res. 2019, 7, 40. [Google Scholar] [CrossRef]
- Jackson, T.; Fabricant, P.D.; Beck, N.; Storey, E.; Patel, N.M.; Ganley, T.J. Epidemiology, injury patterns, and treatment of meniscal tears in pediatric patients: A 16-year experience of a single center. Orthop. J. Sports Med. 2019, 7, 232596711989032. [Google Scholar] [CrossRef]
- Shiraev, T.; Anderson, S.; Hope, N. Meniscal tear-presentation, diagnosis and management. Aust. Fam. Physician 2012, 41, 182–187. [Google Scholar]
- Binfield, P.; Maffulli, N.; King, J. Patterns of meniscal tears associated with anterior cruciate ligament lesions in athletes. Injury 1993, 24, 557–561. [Google Scholar] [CrossRef] [PubMed]
- Am, T.; Mansour, A.; Fakih, R. Unusual presentation of a meniscal tear: A case report. Bull. Hosp. Jt. Dis. N. Y. 1995, 54, 103–105. [Google Scholar]
- Boya, H.; Pinar, H.; Gülay, Z.; Oktay, G.; Ozer, E. Clinical and arthroscopic features of meniscal tears and a search for the role of infection in histologically confirmed meniscal mucoid degeneration. Knee Surg. Sports Traumatol. Arthrosc. 2004, 12, 294–299. [Google Scholar] [CrossRef]
- MacFarlane, L.A.; Yang, H.; Collins, J.E.; Katz, J.; Xu, L.; Teeple, E.; Losina, E.; Guermazi, A.; Jones, M. Associations among meniscal damage, meniscal symptoms and knee pain severity. Osteoarthr. Cartil. 2017, 25, 850–857. [Google Scholar] [CrossRef]
- Parkar, A.P.; Adriaensen, M.E.A.P.M. ESR essentials: MRI of the knee—Practice recommendations by ESSR. Eur. Radiol. 2024, 34, 6590–6599. [Google Scholar] [CrossRef]
- D’Agostino, V.; Sorriento, A.; Cafarelli, A.; Donati, D.; Papalexis, N.; Russo, A.; Lisignoli, G.; Ricotti, L.; Spinnato, P. Ultrasound Imaging in Knee Osteoarthritis: Current Role, Recent Advancements, and Future Perspectives. J. Clin. Med. 2024, 13, 4930. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.E.; Kruse, R.C.; Boettcher, B.J. The Role of Ultrasound in the Diagnosis and Treatment of Meniscal Injuries. Curr. Rev. Musculoskelet. Med. 2024, 17, 171–184. [Google Scholar] [CrossRef] [PubMed]
- Dong, F.; Xu, J.; Wu, H.; Li, M.; Zhang, L.; Wang, S.; Dong, D.; Liu, Y. The diagnostic accuracy of B-mode ultrasound in detecting meniscal tears: A systematic review and pooled meta-analysis. Med. Ultrason. 2018, 20, 164–169. [Google Scholar] [CrossRef]
- Ishii, Y.; Ishikawa, M.; Nakashima, Y.; Hashizume, T.; Okamoto, S.; Iwamoto, Y.; Okada, K.; Takagi, K.; Takahashi, M.; Adachi, N. Dynamic ultrasound reveals the specific behavior of the medial meniscus extrusion in patients with knee osteoarthritis. BMC Musculoskelet. Disord. 2023, 24, 272. [Google Scholar] [CrossRef]
- Farivar, D.; Pascual, T.A.; Hevesi, M.; Chahla, J. Measuring Technique for Meniscal Extrusion Using Ultrasound in the Setting of Posterior Medial Meniscal Root Tears. Arthrosc. Tech. 2024, 13, 102916. [Google Scholar] [CrossRef]
- Fox, M.G.; Graham, J.A.; Skelton, B.W.; Blount, K.J.; Alford, B.A.; Patrie, J.T.; Gaskin, C.M. Prospective Evaluation of Agreement and Accuracy in the Diagnosis of Meniscal Tears: MR Arthrography a Short Time After Injection Versus CT Arthrography After a Moderate Delay. Am. J. Roentgenol. 2016, 207, 142–149. [Google Scholar] [CrossRef]
- Nguyen, J.C.; De Smet, A.A.; Graf, B.K.; Rosas, H.G. MR Imaging–based diagnosis and classification of meniscal tears. RadioGraphics 2014, 34, 981–999. [Google Scholar] [CrossRef] [PubMed]
- Lance, V.; Heilmeier, U.R.; Joseph, G.B.; Steinbach, L.; Ma, B.; Link, T.M. MR imaging characteristics and clinical symptoms related to displaced meniscal flap tears. Skelet. Radiol. 2015, 44, 375–384. [Google Scholar] [CrossRef]
- Ruff, C.; Weingardt, J.P.; Russ, P.D.; Kilcoyne, R.F. MR imaging patterns of displaced meniscus injuries of the knee. Am. J. Roentgenol. 1998, 170, 63–67. [Google Scholar] [CrossRef]
- Dandy, D.J. The arthroscopic anatomy of symptomatic meniscal lesions. J. Bone Jt. Surg. Br. Vol. 1990, 72, 628–633. [Google Scholar] [CrossRef]
- Lecas, L.K.; Helms, C.A.; Kosarek, F.J.; Garret, W.E. Inferiorly displaced flap tears of the medial meniscus: MR appearance and clinical significance. Am. J. Roentgenol. 2000, 174, 161–164. [Google Scholar] [CrossRef] [PubMed]
- Le Hir, P.; Charousset, C.; Duranthon, L.D.; Grimberg, J.; Schmider, L.; Elis, J.B.; Chassaing, V.; Laude, F. Diagnostic IRM des lambeaux méniscaux médiaux déplacés le long du ligament tibial collatéral [Magnetic resonance imaging of medial meniscus tears with displaced fragment in the meniscal recesses]. Rev. Chir. Orthop. Reparatrice Appar. Mot. 2007, 93, 357–363. (In French) [Google Scholar] [CrossRef]
- Dunoski, B.; Zbojniewicz, A.M.; Laor, T. MRI of displaced meniscal fragments. Pediatr. Radiol. 2012, 42, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, J.T.; Cannamela, P.C.; Cruz, A.I.; Mayo, M.; Styhl, A.C.; Richmond, C.G.; Ganley, T.J.; Shea, K.G. Incidence of Meniscal Entrapment and Associated Knee Injuries in Tibial Spine Avulsions. J. Pediatr. Orthop. 2018, 38, e38–e42. [Google Scholar] [CrossRef]
- Trunz, L.M.; Morrison, W.B. MRI of the Knee Meniscus. Magn. Reson. Imaging Clin. N. Am. 2022, 30, 307–324. [Google Scholar] [CrossRef]
- Mesgarzadeh, M.; Moyer, R.; Leder, D.S.; Revesz, G.; Russoniello, A.; Bonakdarpour, A.; Tehranzadeh, J.; Guttmann, D. MR imaging of the knee: Expanded classification and pitfalls to interpretation of meniscal tears. RadioGraphics 1993, 13, 489–500. [Google Scholar] [CrossRef] [PubMed]
- Sayegh, E.T.; Matzkin, E. Classifications in Brief: The International Society of Arthroscopy, Knee Surgery, and Orthopaedic Sports Medicine Classification of Meniscal Tears. Clin. Orthop. Relat. Res. 2022, 480, 39–44. [Google Scholar] [CrossRef]
- Chahwan, S.; Charbel, C.; Tannoury, E.; El Alam, A.; Otayek, J.; Ghanimeh, J.; Khoury, A.; Salameh, P.; Semaan, S. Risk factors for false positive and false negative MRI in diagnosing medial and lateral meniscal tears with concomitant ACL injury. Skelet. Radiol. 2025, 54, 303–315. [Google Scholar] [CrossRef]
- Nakasa, T.; Ishikawa, M.; Nekomoto, A.; Nakata, K.; Omoto, T.; Kamei, G.; Nakamae, A.; Adachi, N. Needle Arthroscopy as a Promising Alternative to MRI for the Diagnosis of Meniscus Injury. Cureus 2023, 15, e48671. [Google Scholar] [CrossRef]
- Griffith, J.F. Five Overlooked Injuries on Knee MRI. Am. J. Roentgenol. 2021, 217, 1165–1174. [Google Scholar] [CrossRef]
- Palisch, A.R.; Winters, R.R.; Willis, M.H.; Bray, C.D.; Shybut, T.B. Posterior Root Meniscal Tears: Preoperative, Intraoperative, and Postoperative Imaging for Transtibial Pullout Repair. RadioGraphics 2016, 36, 1792–1806. [Google Scholar] [CrossRef] [PubMed]
- Guimarães, J.B.; Chemin, R.N.; Araujo, F.F.; Link, T.M.; Silva, F.D.; Bitar, A.; Nico, M.A.C.; Filho, A.G.O. Meniscal Root Tears: An Update Focused on Preoperative and Postoperative MRI Findings. Am. J. Roentgenol. 2022, 219, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Mundal, K.; Geeslin, A.G.; Solheim, E.; Inderhaug, E. Differences Between Traumatic and Degenerative Medial Meniscus Posterior Root Tears: A Systematic Review. Am. J. Sports Med. 2025, 53, 228–233. [Google Scholar] [CrossRef] [PubMed]
- Langhans, M.T.; Lamba, A.; Saris, D.B.F.; Smith, P.; Krych, A.J. Meniscal Extrusion: Diagnosis, Etiology, and Treatment Options. Curr. Rev. Musculoskelet. Med. 2023, 16, 316–327. [Google Scholar] [CrossRef]
- Patel, H.; Skalski, M.R.; Patel, D.B.; White, E.A.; Tomasian, A.; Gross, J.S.; Vangsness, C.T.; Matcuk, G.R., Jr. Illustrative review of knee meniscal tear patterns, repair and replacement options, and imaging evaluation. Clin. Imaging 2021, 69, 4–16. [Google Scholar] [CrossRef]
- Botnari, A.; Kadar, M.; Patrascu, J.M. A Comprehensive Evaluation of Deep Learning Models on Knee MRIs for the Diagnosis and Classification of Meniscal Tears: A Systematic Review and Meta-Analysis. Diagnostics 2024, 14, 1090. [Google Scholar] [CrossRef]
- Krych, A.J.; Wu, I.T.; Desai, V.S.; Murthy, N.S.; Collins, M.S.; Saris, D.B.F.; Levy, B.A.; Stuart, M.J. High Rate of Missed Lateral Meniscus Posterior Root Tears on Preoperative Magnetic Resonance Imaging. Orthop. J. Sports Med. 2018, 6, 2325967118765722. [Google Scholar] [CrossRef]
- Guimaraes, J.B.; Manatrakul, R.; Joseph, G.B.; Feeley, B.; Lansdown, D.A.; Chen, J.V.; Baal, J.D.; Link, T.M. Degenerative medial and lateral menisci root tears: Demographics, clinical presentation, imaging features, and associated findings. Skelet. Radiol. 2025, 54, 255–266. [Google Scholar] [CrossRef]
- LaPrade, R.F.; Floyd, E.R.; Carlson, G.B.; Moatshe, G.; Chahla, J.; Monson, J.K. Meniscal root tears: Solving the silent epidemic. J. Arthrosc. Surg. Sports Med. 2021, 2, 47–57. [Google Scholar] [CrossRef]
- Minami, T.; Muneta, T.; Sekiya, I.; Watanabe, T.; Mochizuki, T.; Horie, M.; Katagiri, H.; Otabe, K.; Ohara, T.; Katakura, M.; et al. Lateral meniscus posterior root tear contributes to anterolateral rotational instability and meniscus extrusion in anterior cruciate ligament-injured patients. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 1174–1181. [Google Scholar] [CrossRef]
- Alsaleh, N.S.; Alnasser, A.A.; Alqahtani, A.A. A case report of simultaneous tears of the medial and lateral posterior meniscal roots with an intact ACL graft. Int. J. Surg. Case Rep. 2024, 121, 109971. [Google Scholar] [CrossRef]
- Krych, A.J.; Hevesi, M.; Leland, D.P.; Stuart, M.J. Meniscal Root Injuries. J. Am. Acad. Orthop. Surg. 2019, 28, 491–499. [Google Scholar] [CrossRef]
- Koo, J.H.; Choi, S.H.; Lee, S.A.; Wang, J.H. Comparison of Medial and Lateral Meniscus Root Tears. PLoS ONE 2015, 10, e0141021. [Google Scholar] [CrossRef] [PubMed]
- De Smet, A.A.; Graf, B.K. Meniscal tears missed on MR imaging: Relationship to meniscal tear patterns and anterior cruciate ligament tears. Am. J. Roentgenol. 1994, 162, 905–911. [Google Scholar] [CrossRef] [PubMed]
- Jung, M.; Lee, D.H.; Kim, S.J.; Choi, C.H.; Kim, S.H.; Jin, S.; Park, K.B. Preoperative Diagnosis and Treatment Outcomes of Incarcerated Inferiorly Displaced Flap Tear of the Medial Meniscus: Comparison between Flap Tears with and without Incarcerated Fragment. BioMed. Res. Int. 2018, 2018, 5941057. [Google Scholar] [CrossRef] [PubMed]
- Eskander, M.S.; Drew, J.M.; Osuch, D.B.; Metzmaker, J. A lateral meniscus tear incarcerated behind the popliteus tendon: A case report. Knee 2010, 17, 359–361. [Google Scholar] [CrossRef]
- Yang, W.; Wang, H.; Shao, Z.; Huang, W. The Posteromedial-Transseptal Portal for Arthroscopic Suture Hook Repair of Posterior Horn Tears and Popliteomeniscal Fascicles Tears of the Lateral Meniscus. Arthrosc. Tech. 2023, 12, e1375–e1381. [Google Scholar] [CrossRef]
- Wang, Y.; Chen, J.; Li, D.; Yang, R.; Xiang, X. Single Needle All-Inside Technique for Lateral Meniscus Repair at Popliteal Hiatus Area: Safe, Effective, and Time-Saving. Arthrosc. Tech. 2023, 12, e371–e375. [Google Scholar] [CrossRef]
- Zheng, J.P.; Xiao, Q.; Deng, H.Y.; Wu, Q.Q.; Zhai, W.L.; Lin, D.S. Arthroscopic classification and management for the popliteal hiatus of the lateral meniscus tears. Beijing Da Xue Xue Bao Yi Xue Ban 2021, 53, 891–895. (In Chinese) [Google Scholar] [CrossRef]
- Fraind-Maya, G.; Laniado, D.; Ilsar, I.; Chaimsky, G.; Mosheiff, R.; Weil, Y. Meniscal Entrapment After Tibial Plateau Fracture and Fixation: A Case Report. J. Bone Jt. Surg. 2021, 11, e20.01012. [Google Scholar] [CrossRef]
- Burstein, D.B.; Viola, A.; Fulkerson, J.P. Entrapment of the medial meniscus in a fracture of the tibial eminence. Arthroscopy 1988, 4, 47–50. [Google Scholar] [CrossRef] [PubMed]
- Chandler, J.T.; Miller, T.K. Tibial eminence fracture with meniscal entrapment. Arthrosc. J. Arthrosc. Relat. Surg. 1995, 11, 499–502. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spinnato, P.; Franceschi, P.; Martinese, G.; Parmeggiani, A.; D’Agostino, V.; Ferraro, S.; Matcuk, G.R.; Zaffagnini, S.; Grassi, A. Atypically Displaced Meniscal Tears: An Educational Review with Focus on MRI and Arthroscopy. Clin. Pract. 2025, 15, 109. https://doi.org/10.3390/clinpract15060109
Spinnato P, Franceschi P, Martinese G, Parmeggiani A, D’Agostino V, Ferraro S, Matcuk GR, Zaffagnini S, Grassi A. Atypically Displaced Meniscal Tears: An Educational Review with Focus on MRI and Arthroscopy. Clinics and Practice. 2025; 15(6):109. https://doi.org/10.3390/clinpract15060109
Chicago/Turabian StyleSpinnato, Paolo, Paola Franceschi, Giuseppe Martinese, Anna Parmeggiani, Valerio D’Agostino, Silvia Ferraro, George R. Matcuk, Stefano Zaffagnini, and Alberto Grassi. 2025. "Atypically Displaced Meniscal Tears: An Educational Review with Focus on MRI and Arthroscopy" Clinics and Practice 15, no. 6: 109. https://doi.org/10.3390/clinpract15060109
APA StyleSpinnato, P., Franceschi, P., Martinese, G., Parmeggiani, A., D’Agostino, V., Ferraro, S., Matcuk, G. R., Zaffagnini, S., & Grassi, A. (2025). Atypically Displaced Meniscal Tears: An Educational Review with Focus on MRI and Arthroscopy. Clinics and Practice, 15(6), 109. https://doi.org/10.3390/clinpract15060109