
Comparison of Post-Tonsillectomy Hemorrhage Rate After Different Tonsillectomy Techniques: Systematic Review and Meta Analysis

 ,
,
Abstract
1. Introduction
1.1. Methodology
1.2. Search Strategy
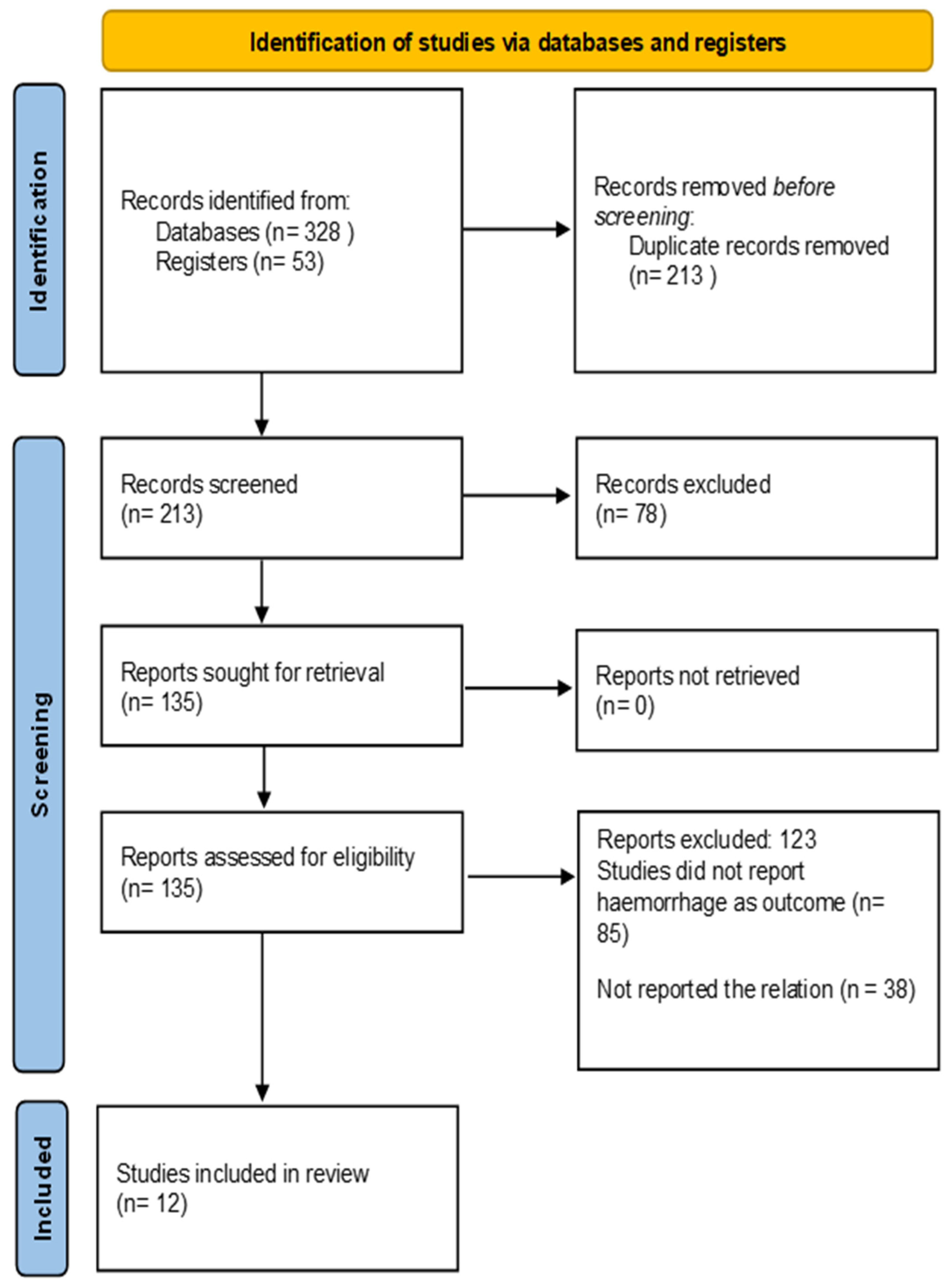
1.3. Study Selection
1.4. Data Extraction and Coding
1.5. Risk of Bias Assessment
1.6. Data Synthesis and Statistical Analysis
1.7. Subgroup Analyses
1.8. Dissemination of Results
2. Results
2.1. Results of the Meta-Analysis
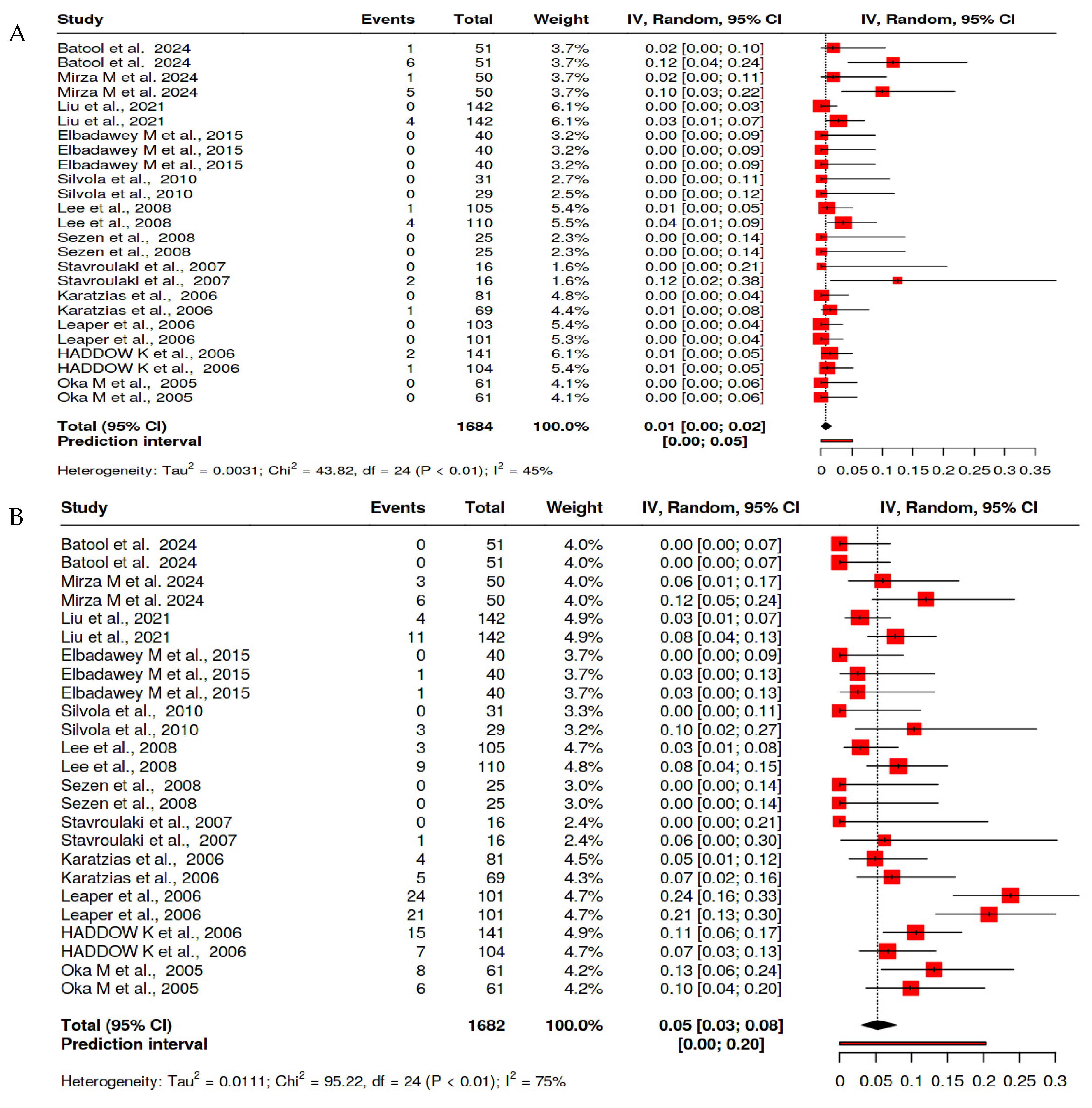
2.1.1. Rates of Primary and Secondary Hemorrhage After Tonsillectomy
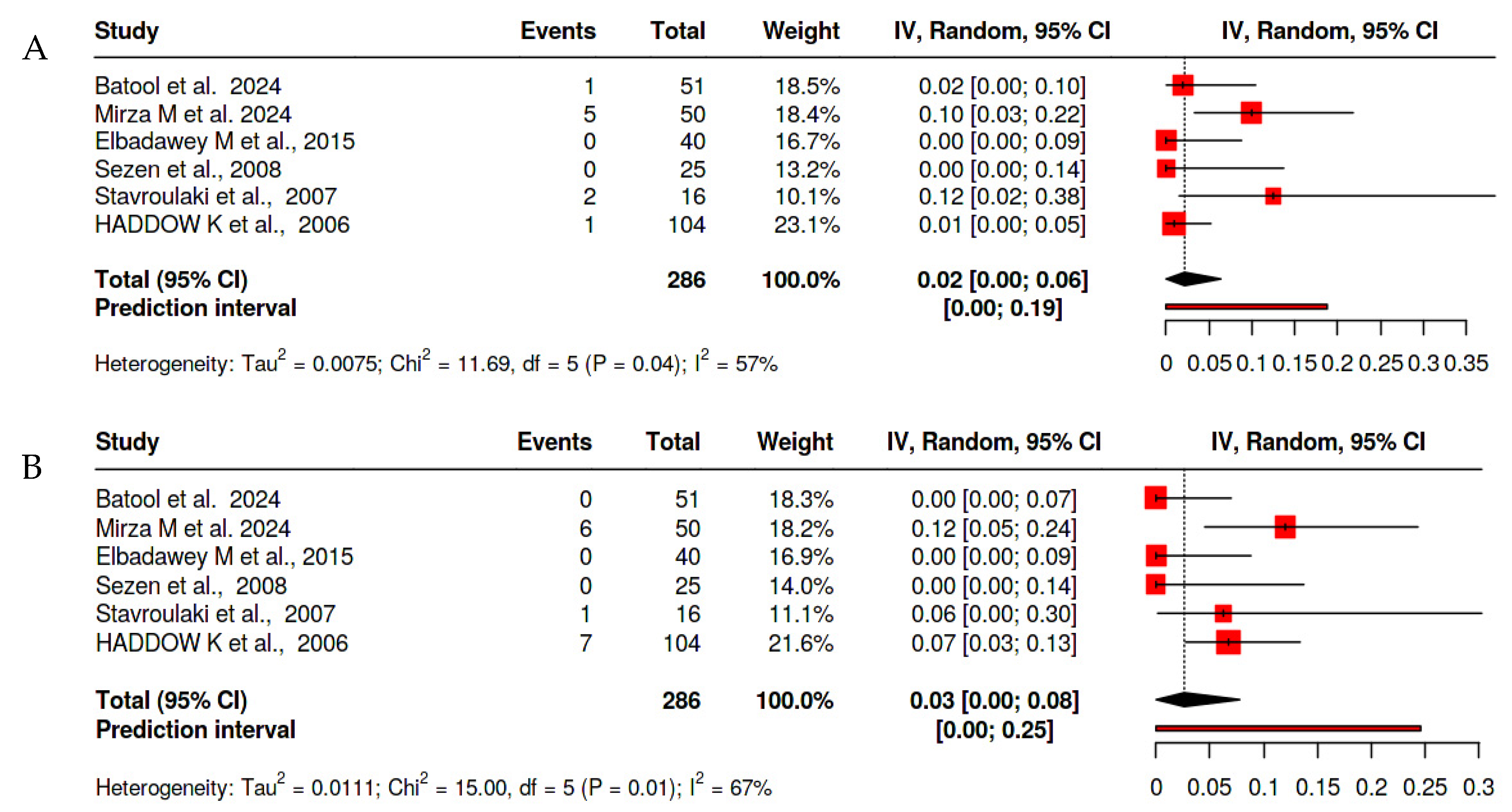
2.1.2. Cold Steel Tonsillectomy
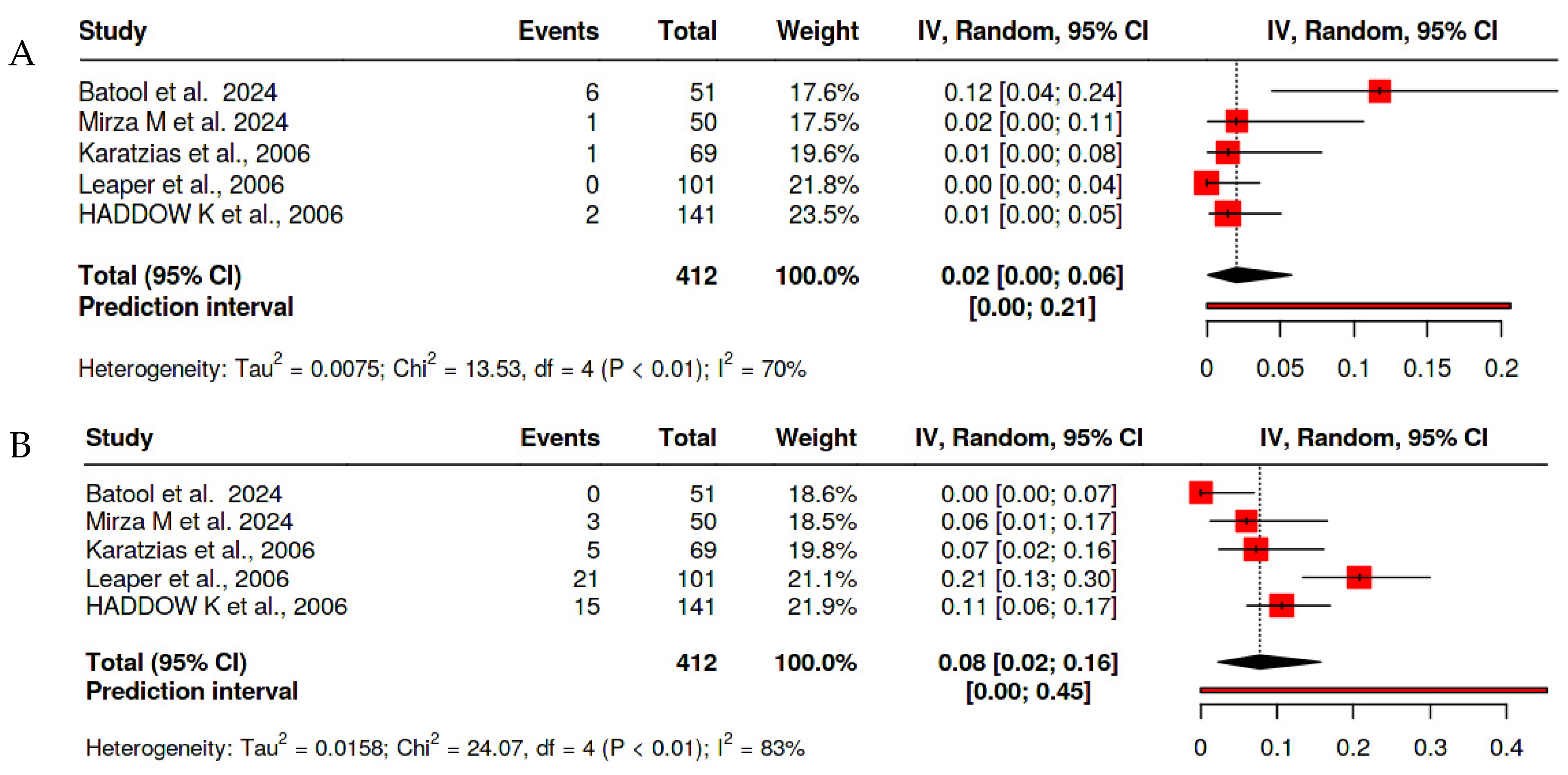
2.1.3. Bipolar Tonsillectomy
2.1.4. Risk of Bias Assessment
3. Discussion
3.1. Implications for Clinical Practice
3.2. Limitations and Recommendations for Future Research
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Di Mauro, P.; Cocuzza, S.; Maniaci, A.; Ferlito, S.; Rasà, D.; Anzivino, R.; Vicini, C.; Iannella, G.; La Mantia, I. The Effect of Adenotonsillectomy on Children’s Behavior and Cognitive Performance with Obstructive Sleep Apnea Syndrome: State of the Art. Children 2021, 8, 921. [Google Scholar] [CrossRef] [PubMed]
- Bagherihagh, A.; Najarzadeh, A.A.; Taheri, A.; Saeedi, M.; Hasanalifard, M. Comparative study of adult tonsillectomy in two methods: Harmonic scalpel and classical surgery. Egypt J. Otolaryngol. 2023, 39, 77. [Google Scholar] [CrossRef]
- Nguyen, B.K.; Quraishi, H.A. Tonsillectomy and Adenoidectomy-Pediatric Clinics of North America. Pediatr. Clin. N. Am. 2022, 69, 247–259. [Google Scholar] [CrossRef] [PubMed]
- Reckley, L.; Fernandez-Salvador, C.; Camacho, M. The effect of tonsillectomy on obstructive sleep apnea: An overview of systematic reviews. Nat. Sci. Sleep 2018, 10, 105–110. [Google Scholar] [CrossRef]
- Chinnadurai, S.; Jordan, A.K.; Sathe, N.A.; Fonnesbeck, C.; McPheeters, M.L.; Francis, D.O. Tonsillectomy for Obstructive Sleep-Disordered Breathing: A Meta-analysis. Pediatrics 2017, 139, e20163491. [Google Scholar] [CrossRef]
- Grasl, S.; Mekhail, P.; Janik, S.; Grasl, C.M.; Vyskocil, E.; Erovic, B.M.; Arnoldner, C.; Landegger, L.D. Temporal fluctuations of post-tonsillectomy haemorrhage. Eur. Arch. Oto-Rhino-Laryngol. 2022, 279, 1601–1607. [Google Scholar] [CrossRef]
- Windfuhr, J.P.; Schloendorff, G.; Baburi, D.; Kremer, B. Lethal outcome of post-tonsillectomy hemorrhage. Eur. Arch. Oto-Rhino-Laryngol. 2008, 265, 1527–1534. [Google Scholar] [CrossRef]
- Heidemann, C.H.; Wallén, M.; Aakesson, M.; Skov, P.; Kjeldsen, A.D.; Godballe, C. Post-tonsillectomy hemorrhage: Assessment of risk factors with special attention to introduction of coblation technique. Eur. Arch. Oto-Rhino-Laryngol. 2009, 266, 1011–1015. [Google Scholar] [CrossRef]
- Ahmadieh, H.; Kreidieh, O.; A Akl, E.; Fuleihan, G.E.-H. Minimally invasive parathyroidectomy guided by intraoperative parathyroid hormone monitoring (IOPTH) and preoperative imaging versus bilateral neck exploration for primary hyperparathyroidism in adults. Cochrane Database Syst. Rev. 2020, 10, CD010787. [Google Scholar] [CrossRef]
- Haq, A.U.; Bansal, C.; Pandey, A.K.; Singh, V.P. Analysis of Different Techniques of Tonsillectomy: An Insight. Indian. J. Otolaryngol. Head Neck Surg. 2022, 74 (Suppl. S3), 5717–5730. [Google Scholar] [CrossRef]
- Liu, J.H.; Anderson, K.E.; Willging, J.P.; Iii, C.M.M.; Shott, S.R.; Bratcher, G.O.; Cotton, R.T. Posttonsillectomy Hemorrhage. Arch. Otolaryngol. Neck Surg. 2001, 127, 1271. [Google Scholar] [CrossRef] [PubMed]
- Silvola, J.; Salonen, A.; Nieminen, J.; Kokki, H. Tissue welding tonsillectomy provides an enhanced recovery compared to that after monopolar electrocautery technique in adults: A prospective randomized clinical trial. Eur. Arch. Oto-Rhino-Laryngol. 2011, 268, 255–260. [Google Scholar] [CrossRef]
- Lee, S.W.; Jeon, S.S.; Lee, J.D.; Lee, J.Y.; Kim, S.C.; Koh, Y.W. A comparison of postoperative pain and complications in tonsillectomy using BiClamp forceps and electrocautery tonsillectomy. Otolaryngol. Neck Surg. 2008, 139, 228–234. [Google Scholar] [CrossRef] [PubMed]
- Batool, F.; Ghani, S.; Asif, M.; Haroon, T.; Ibrahim, M.; Mohammad, N. Comparison of Post-Tonsillectomy Hemorrhage rate in patients undergoing two commonly used Tonsillectomy Methods. Prof. Med. J. 2024, 31, 1106–1112. [Google Scholar] [CrossRef]
- Liu, Q.; Zhang, Y.; Lyu, Y. Postoperative hemorrhage following coblation tonsillectomy with and without suture: A randomized study in Chinese adults. Am. J. Otolaryngol. 2021, 42, 102760. [Google Scholar] [CrossRef]
- Sezen, O.S.; Kaytanci, H.; Kubilay, U.; Coskuner, T.; ÜNver, Ş. Comparison between tonsillectomy with thermal welding and the conventional ‘cold’tonsillectomy technique. ANZ J. Surg. 2008, 78, 1014–1018. [Google Scholar] [CrossRef] [PubMed]
- Stavroulaki, P.; Skoulakis, C.; Theos, E.; Kokalis, N.; Valagianis, D. Thermal Welding versus Cold Dissection Tonsillectomy: A Prospective, Randomized, Single-Blind Study in Adult Patients. Ann. Otol. Rhinol. Laryngol. 2007, 116, 565–570. [Google Scholar] [CrossRef]
- Karatzias, G.T.; Lachanas, V.A.; Sandris, V.G. Thermal Welding versus Bipolar Tonsillectomy: A Comparative Study. Otolaryngol. Neck Surg. 2006, 134, 975–978. [Google Scholar] [CrossRef]
- Leaper, M.; Mahadevan, M.; Vokes, D.; Sandow, D.; Anderson, B.J.; West, T. A prospective randomised single blinded study comparing harmonic scalpel tonsillectomy with bipolar tonsillectomy. Int. J. Pediatr. Otorhinolaryngol. 2006, 70, 1389–1396. [Google Scholar] [CrossRef]
- Oko, M.O.; Ganly, I.; Loughran, S.; Clement, W.A.; Young, D.; Geddes, N.K. A Prospective Randomized Single-Blind Trial Comparing Ultrasonic Scalpel Tonsillectomy with Tonsillectomy by Blunt Dissection in a Pediatric Age Group. Otolaryngol. Neck Surg. 2005, 133, 579–584. [Google Scholar] [CrossRef]
- Elbadawey, M.R.; Hegazy, H.M.; Eltahan, A.E.; Powell, J. A randomised controlled trial of coblation, diode laser and cold dissection in paediatric tonsillectomy. J. Laryngol. Otol. 2015, 129, 1058–1063. [Google Scholar] [CrossRef] [PubMed]
- Haddow, K.; Montague, M.-L.; Hussain, S.S.M. Post-tonsillectomy haemorrhage: A prospective, randomized, controlled clinical trial of cold dissection versus bipolar diathermy dissection. J. Laryngol. Otol. 2006, 120, 450–454. [Google Scholar] [CrossRef] [PubMed]
- Elahi, M.M.K.; Mollik, K.H.; Kazi, M.; Reza, H.; Islam, A.; Sarkar, R.K.; Karim, R. Comparison of Surgical Complications between Cold Steel Dissection Method and Bipolar Electro Dissection Method in Tonsillectomy. Sch. J. Appl. Med. Sci. 2024, 12, 548–555. [Google Scholar] [CrossRef]
- Dharmawardana, N.; Chandran, D.; Elias, A.; Kao, S.S.-T. Management of post tonsillectomy secondary haemorrhage: Flinders experience. Aust. J. Otolaryngol. 2018, 1, 31. [Google Scholar] [CrossRef]
- Burton, K.; Hanke, S.; Gungor, A. Reduced post-tonsillectomy bleeding rates through a refined technique. Am. J. Otolaryngol. 2017, 38, 438–441. [Google Scholar] [CrossRef]
- Faramarzi, A.; Heydari, S.T. Prevalence of Post-tonsillectomy Bleeding as Day-case Surgery with Combination Method; Cold Dissection Tonsillectomy and Bipolar Diathermy Hemostasis. Iran. J. Pediatr. 2010, 20, 187–192. [Google Scholar]
- Abdel-Aziz, M.; Atef, A.; Sabry, O.A.; Yousef, A.I.; Ahmed, A.S.; Hussien, A.A.; Abdel-Haleem, M.; Samir, A. Different tonsillectomy techniques in Egypt: Advantages and disadvantages—Experience and review of literature. Egypt J. Otolaryngol. 2023, 39, 127. [Google Scholar] [CrossRef]
- Karam, M.; Abul, A.; Althuwaini, A.; Almuhanna, A.; Alenezi, T.; Aljadi, A.; Al-Naseem, A.; Alsaif, A.; Alwael, A. Coblation Versus Bipolar Diathermy Hemostasis in Pediatric Tonsillectomy Patients: Systematic Review and Meta-Analysis. Cureus 2022, 14, e23066. [Google Scholar] [CrossRef]
- Inuzuka, Y.; Mizutari, K.; Kamide, D.; Sato, M.; Shiotani, A. Risk factors of post-tonsillectomy hemorrhage in adults. Laryngoscope Investig. Otolaryngol. 2020, 5, 1056–1062. [Google Scholar] [CrossRef]
- El-Anwar, M.W.; Abdelhamid, H.I.; Ghanem, A.E.; El-Hussiny, A. Tonsillar healing membrane characteristic for tonsillectomy using combined cold dissection and bipolar electrocautery. Egypt J. Otolaryngol. 2024, 40, 73. [Google Scholar] [CrossRef]
- Mösges, R.; Hellmich, M.; Allekotte, S.; Albrecht, K.; Böhm, M. Hemorrhage rate after coblation tonsillectomy: A meta-analysis of published trials. Eur. Arch. Oto-Rhino-Laryngol. 2011, 268, 807–816. [Google Scholar] [CrossRef] [PubMed]
- Halme, A.L.E.; Roshanov, P.S.; Tornberg, S.V.; Lavikainen, L.I.; Devereaux, P.J.; Tikkinen, K.A.O.; VISION Investigators; DeBeer, J.; Kearon, C.; Mizera, R.; et al. Timing of Major Postoperative Bleeding Among Patients Undergoing Surgery. JAMA Netw. Open 2024, 7, e244581. [Google Scholar] [CrossRef] [PubMed]
- Lieberg, N.; Aunapuu, M.; Arend, A. Coblation tonsillectomy versus cold steel dissection tonsillectomy: A morphological study. J. Laryngol. Otol. 2019, 133, 770–774. [Google Scholar] [CrossRef] [PubMed]
- Walijee, H.; Al-Hussaini, A.; Harris, A.; Owens, D. What Are the Trends in Tonsillectomy Techniques in Wales? A Prospective Observational Study of 19,195 Tonsillectomies over a 10-Year Period. Int. J. Otolaryngol. 2015, 2015, 747403. [Google Scholar] [CrossRef]
- Verma, R.; Verma, R.R.; Verma, R.R. Tonsillectomy-Comparative Study of Various Techniques and Changing Trend. Indian J. Otolaryngol. Head Neck Surg. 2017, 69, 549–558. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Risk of Bias Domain | Description | Assessment |
|---|---|---|
| 1. Bias arising from the randomization process | Assesses whether the randomization was conducted properly and whether the allocation sequence was concealed. | Low Risk/Some Concerns/High Risk |
| 2. Bias due to deviations from intended interventions | Assesses whether the interventions were delivered as intended and if there were any deviations. | Low Risk/Some Concerns/High Risk |
| 3. Bias due to missing outcome data | Assesses whether there was sufficient and balanced handling of missing outcome data. | Low Risk/Some Concerns/High Risk |
| 4. Bias in measurement of the outcome | Assesses whether the outcome was measured appropriately and without bias (e.g., blinding). | Low Risk/Some Concerns/High Risk |
| 5. Bias in selection of the reported result | Assesses whether selective reporting of outcomes occurred, such as only reporting significant results. | Low Risk/Some Concerns/High Risk |
| Study | Objective | Study Design | Population | Setting | Duration |
|---|---|---|---|---|---|
| Batool et al., 2024 [14] | To compare post-tonsillectomy hemorrhage rates in cold steel vs. bipolar diathermy methods. | RCT | 102 patients | Teaching hospital in Pakistan | October 2020 to June 2022 |
| Mirza M et al., 2024 [23] | To assess whether bipolar electro dissection tonsillectomy has better surgical outcomes compared to cold steel dissection. | RCT | 100 patients undergoing elective tonsillectomy | Dhaka Medical College Hospital | 1 January 2020–30 July 2021 |
| Liu et al., 2021 [15] | To compare post-tonsillectomy hemorrhage rates in coblation tonsillectomy with vs. without suture. | RCT | 284 adult patients | Single hospital in China | January 2017 to August 2019 |
| Elbadawey M et al., 2015 [21] | To compare the efficacy of diode laser, coblation, and cold dissection tonsillectomy in pediatric patients. | Prospective RCT | 120 patients aged 10–15 years with recurrent tonsillitis | Not specified | July 2010–May 2012 |
| Silvola et al., 2010 [12] | To evaluate recovery using TW vs. monopolar techniques | Single-blind RCT | 60 healthy adult day-surgery patients | Finland | 2 weeks post-op follow-up |
| Lee et al., 2008 [13] | To compare BiClamp forcep tonsillectomy with standard electrocautery tonsillectomy | Prospective RCT | Pediatric (92) and adult (123) patients | Not specified | 14 days post-op follow-up |
| Sezen et al., 2008 [16] | To evaluate length of procedure, anesthesia, fluid use, blood loss, and pain | Prospective RCT | 50 patients (3–28 years) | Turkey | Post-op daily assessments |
| Stavroulaki et al., 2007 [17] | To compare postoperative morbidity in adults undergoing TW vs. cold dissection | Single-blind RCT | 32 adults (mean age: 25–27 years) | Greece | 10 days post-op follow-up |
| Karatzias et al., 2006 [18] | To compare TWT with BET procedures | Prospective RCT | 150 adults (17–56 years) | Greece | Not specified |
| Leaper et al., 2006 [19] | To compare pain, analgesic use, and bleeding in children using harmonic scalpel vs. bipolar | RCT | 204 children (6–15 years) | Not specified | 13 days post-op follow-up |
| HADDOW K et al., 2006 [22] | To determine if bipolar dissection tonsillectomy is associated with a higher postoperative hemorrhage rate than cold dissection tonsillectomy. | Prospective RCT | 245 patients undergoing elective tonsillectomy | Teaching hospital | July 2002–November 2004 |
| Oko M et al., 2005 [20] | To determine if there was a difference in postoperative pain and dietary intake comparing ultrasonic scalpel (US) with blunt dissection (BD) tonsillectomy. | Prospective single-blind RCT | 122 children aged 5–13 years undergoing tonsillectomy for recurrent acute tonsillitis | Specialized pediatric hospital | 12 December 2002–14 February 2003 |
| Study | Techniques Compared | Sample Size | Age (Mean/Range) | Gender (% Male) | Other Characteristics |
|---|---|---|---|---|---|
| Batool et al., 2024 [14] | Cold steel vs. bipolar diathermy methods | Cold steel: 51 bipolar diathermy methods: 51 | 19.34 ± 13.44 years (range 3–59) | 61.76% | Stratified by age and gender |
| Mirza M et al., 2024 [23] | Bipolar electro dissection (BED) vs. cold steel dissection (CSD) | BED: 50 CSD: 50 | Not specified, presumed 18–50 years | Not specified | Elective tonsillectomy, randomized controlled trial |
| Liu et al., 2021 [15] | Coblation with vs. without suture | Coblation with suture: 142 without suture: 142 | 18–71 years | 53.80% | Comparable BMI and disease course |
| Elbadawey M et al., 2015 [21] | Diode laser vs. coblation vs. cold sissection | Diode laser: 40 Coblation: 40 Cold dissection: 40 | Diode laser: 10 (2.5) Coblation: 10 (2.8) Cold dissection: 10 (3.2) | Diode laser: 18 (45.0%) Coblation: 21 (52.5%) Cold dissection: 21 (47.5%) | Recurrent tonsillitis, randomized controlled trial |
| Silvola et al., 2010 [12] | TW vs. monopolar techniques | TW: 31 Monopolar: 29 | Monopolar: 28 (11) TW: 26 (8) | Monopolar: 41.4% TW: 45.2% | Indications: chronic-recurrent tonsillitis, hypertrophy, abscess |
| Lee et al., 2008 [13] | BiClamp vs. electrocautery | Pediatric BT: 45 Pediatric ET: 47 Adult BT: 60 Adult ET: 63 | Pediatric BT: 6.0 (2.5) Pediatric ET: 7.0 (2.5) Adult BT: 33 (13.6) Adult ET: 34.7 (11.8) | Pediatric BT: 60.0% Pediatric ET: 63.8% Adult BT: 70.0% Adult ET: 61.9% | Pediatric and adult groups evaluated separately |
| Sezen et al., 2008 [16] | TW vs. cold dissection | TW: 25 Cold: 25 | TW: 9.64 (6.24) Cold: 8.44 (5.47) | Similar across groups (p > 0.05) | Indications: recurrent tonsillitis, tonsil hypertrophy |
| Stavroulaki et al., 2007 [17] | TW vs. cold dissection | TW: 16 Cold: 16 | TW: 27.19 (8.28) Cold: 25.56 (5.10) | TW: 68.75% Cold: 81.25% | Exclusion: other procedures during tonsillectomy |
| Karatzias et al., 2006 [18] | TWT vs. BET | TWT: 81 BET: 69 | 26.8 years (range 17–56) | TWT: 55.6% BET: 52.2% | Exclusion: peritonsillar abscess, bleeding disorders |
| Leaper et al., 2006 [19] | Harmonic scalpel vs. bipolar | Harmonic: 103 Bipolar: 101 | Harmonic: 10 (2.8) Bipolar: 9 (2.6) | Harmonic: 39% Bipolar: 44% | Exclusion: none specified |
| HADDOW K et al., 2006 [22] | Bipolar dissection vs. cold dissection | Bipolar: 141 Cold: 104 | 3–70 years | 41.67% | Elective tonsillectomy, randomized controlled trial |
| Oko M et al., 2005 [20] | Ultrasonic scalpel (US) vs. blunt dissection (BD) | BD: 61 US: 61 | BD: 8 (2.51) US: 8.4 (2.55) | 76% | Recurrent acute tonsillitis, single-blind trial |
| Study | Postoperative Hemorrhage Rate | Severity of Hemorrhage | Re-Intervention | Length of Hospital Stay |
|---|---|---|---|---|
| Batool et al., 2024 [14] | Cold steel: 1.96% bipolar diathermy: 11.76% | Higher in bipolar diathermy group (p = 0.050) | None reported | Not specified |
| Mirza M et al., 2024 [23] | No significant difference in post-op hemorrhage between BED and CSD | Postoperative hemorrhage slightly more common in CSD (22% vs. 8%) | Conservative treatment for most hemorrhages | Not mentioned |
| Liu et al., 2021 [15] | Coblation with suture: 0.0% primary and 2.8% secondary; without suture: 2.8% primary and 7.7% secondary | Reduced in suture group (p = 0.02) | None in suture group, 15 cases in non-suture | Not specified |
| Elbadawey M et al., 2015 [21] | Coblation had lowest pain and blood loss, diode laser showed higher pain at day 7 | Secondary hemorrhage (1.7%) in each group | 2 secondary hemorrhages, conservative management | Not specified |
| Silvola et al., 2010 [12] | TW: 0% Monopolar: 10.3% | Secondary hemorrhage requiring electrocautery | TW: 0, monopolar: 3 cases | Not specified |
| Lee et al., 2008 [13] | Pediatric: BT: 0% ET: 6.4% Adult: BT: 6.7% ET: 14.3% | Primary and secondary hemorrhage rates higher in ET | BT: Lower ET: Higher | Not specified |
| Sezen et al., 2008 [16] | TW: 0 Cold: 0 | None observed | None | Not specified |
| Stavroulaki et al., 2007 [17] | TW: 0% Cold: 18.75% | 2 primary and 1 secondary bleed in cold group | TW: 0, cold: 2 surgeries | Not specified |
| Karatzias et al., 2006 [18] | TWT: 1.2% BET: 4.3% | Secondary hemorrhage | BET: 1 surgery | Not specified |
| Leaper et al., 2006 [19] | Harmonic: 23%, bipolar: 21% | Minor and major hemorrhages | 6 surgeries | Not specified |
| HADDOW K et al., 2006 [22] | Hemorrhage rate higher in bipolar dissection group (12.1% vs. 7.7%) | Secondary: 22 cases overall, 15 in bipolar dissection group | Conservative for most, 2 re-operations in bipolar dissection | No significant difference in length of stay |
| Oko M et al., 2005 [20] | US: significantly higher pain, BD: higher blood loss (33.1 mL vs. 3.0 mL) | Pain: US > BD, dietary intake: better in US group at days 1, 5, 7, 9 | No significant re-intervention | Not mentioned |
| Study | Bias Arising from Randomization Process | Bias Due to Deviations from Intended Interventions | Bias Due to Missing Outcome Data | Bias in Measurement of Outcome | Bias in Selection of Reported Results | Overall Risk of Bias |
|---|---|---|---|---|---|---|
| Batool et al., 2024 [14] | Low | Low | Low | Low | Low | Low |
| Mirza M et al., 2024 [23] | Low | Low | Low | Low | Low | Low |
| Liu et al., 2021 [15] | Low | Low | Low | Low | Low | Low |
| Elbadawey M et al., 2015 [21] | Low | Low | Low | Low | Low | Low |
| Silvola et al., 2010 [12] | Low | Low | Low | Low | Low | Low |
| Lee et al., 2008 [13] | Low | Low | Low | Low | Low | Low |
| Sezen et al., 2008 [16] | Low | Low | Low | Low | Low | Low |
| Stavroulaki et al., 2007 [17] | Low | Low | Low | Low | Low | Low |
| Karatzias et al., 2006 [18] | Low | Low | Low | Low | Low | Low |
| Leaper et al., 2006 [19] | Low | Low | Low | Low | Low | Low |
| HADDOW K et al., 2006 [22] | Low | Low | Low | Low | Low | Low |
| Oko M et al., 2005 [20] | Low | Low | Low | Low | Low | Low |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alenezi, M.M.; Al-Harbi, F.A.; Almoshigeh, A.N.M.; Alruqaie, S.S.; Alshahrani, N.M.; Alamro, A.M.; Aljulajil, A.A.; Alsaqri, R.A.; Alharbi, L.A. Comparison of Post-Tonsillectomy Hemorrhage Rate After Different Tonsillectomy Techniques: Systematic Review and Meta Analysis. Clin. Pract. 2025, 15, 85. https://doi.org/10.3390/clinpract15050085
Alenezi MM, Al-Harbi FA, Almoshigeh ANM, Alruqaie SS, Alshahrani NM, Alamro AM, Aljulajil AA, Alsaqri RA, Alharbi LA. Comparison of Post-Tonsillectomy Hemorrhage Rate After Different Tonsillectomy Techniques: Systematic Review and Meta Analysis. Clinics and Practice. 2025; 15(5):85. https://doi.org/10.3390/clinpract15050085
Chicago/Turabian StyleAlenezi, Mazyad M., Faisal A. Al-Harbi, Albaraa Nasser M. Almoshigeh, Sultan S. Alruqaie, Nada M. Alshahrani, Alwaleed Mohammed Alamro, Abdulmalik Abdulaziz Aljulajil, Rayan Abduallah Alsaqri, and Lama A. Alharbi. 2025. "Comparison of Post-Tonsillectomy Hemorrhage Rate After Different Tonsillectomy Techniques: Systematic Review and Meta Analysis" Clinics and Practice 15, no. 5: 85. https://doi.org/10.3390/clinpract15050085
APA StyleAlenezi, M. M., Al-Harbi, F. A., Almoshigeh, A. N. M., Alruqaie, S. S., Alshahrani, N. M., Alamro, A. M., Aljulajil, A. A., Alsaqri, R. A., & Alharbi, L. A. (2025). Comparison of Post-Tonsillectomy Hemorrhage Rate After Different Tonsillectomy Techniques: Systematic Review and Meta Analysis. Clinics and Practice, 15(5), 85. https://doi.org/10.3390/clinpract15050085